
Occupational Exposure to Halogenated Anaesthetic Gases in Hospitals: A Systematic Review of Methods and Techniques to Assess Air Concentration Levels
 , , , , ,
, , , , ,  ,
,  ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
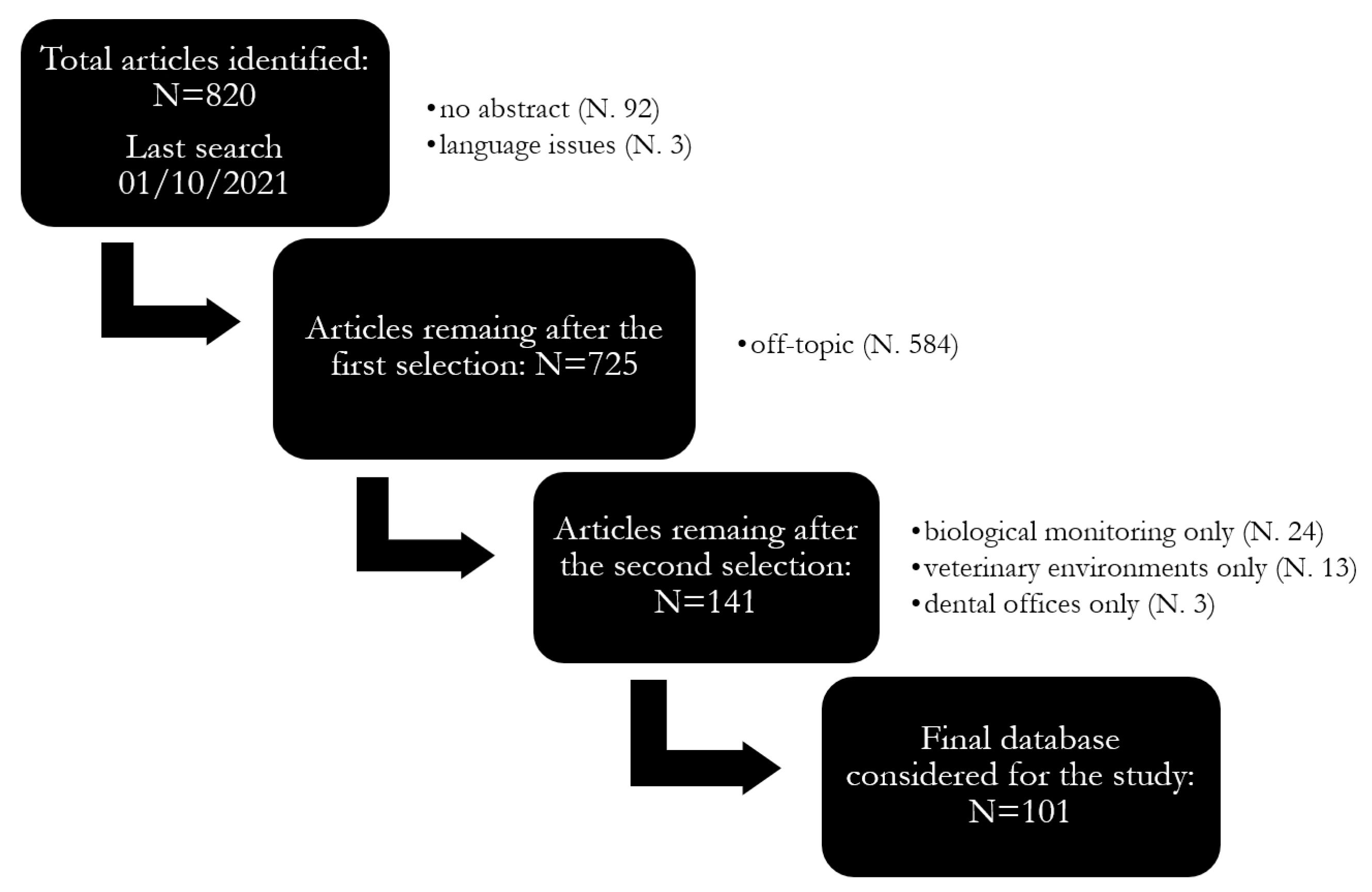
2.1. Systematic Review
2.2. Statistical Analysis
3. Results and Discussions
3.1. Halogenated WAGs and Concentrations Time Trends
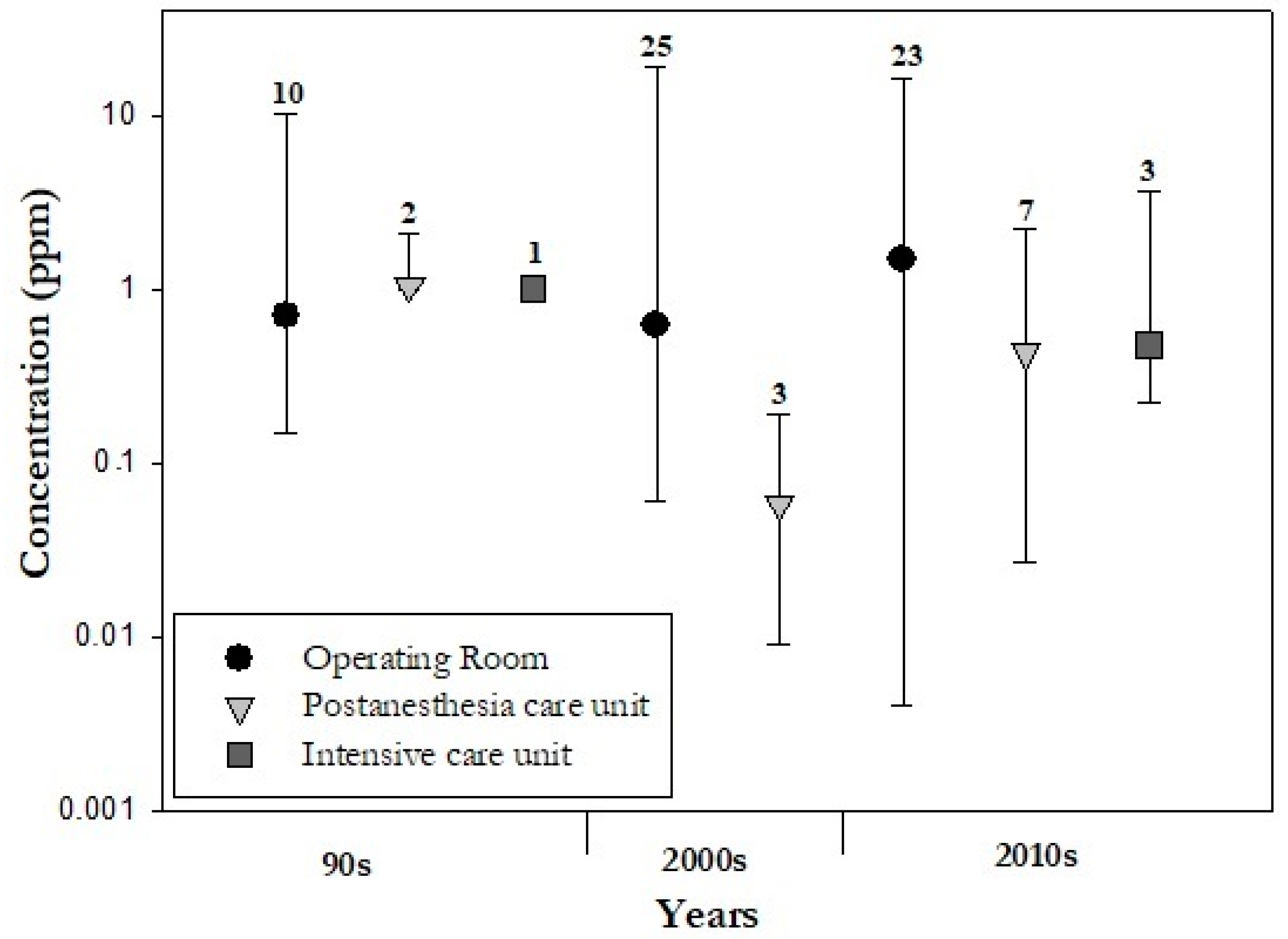
3.1.1. Concentrations of WAGs in Different Hospitals Areas
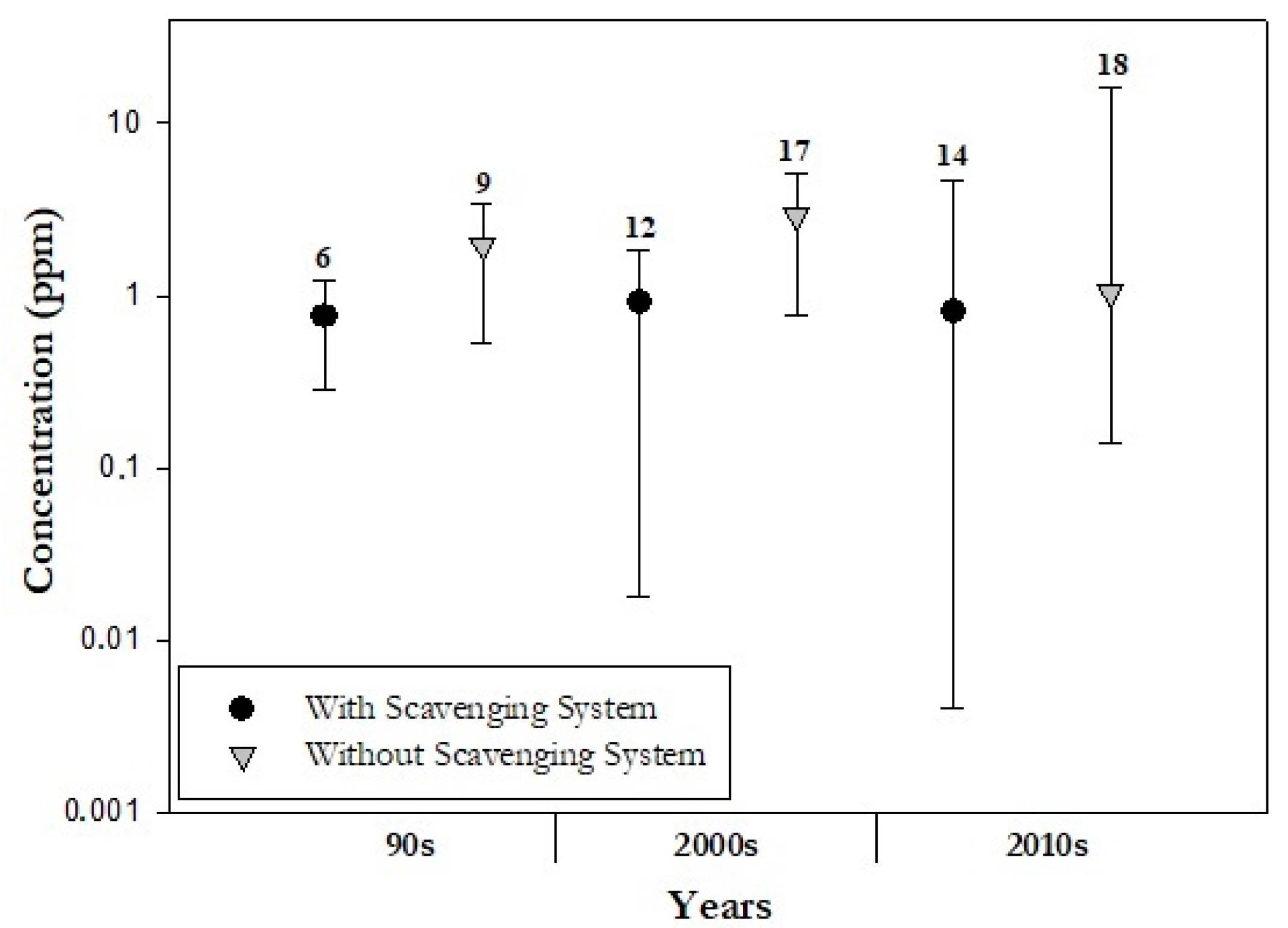
3.1.2. Mitigation Techniques of WAGs in Different Hospital Areas
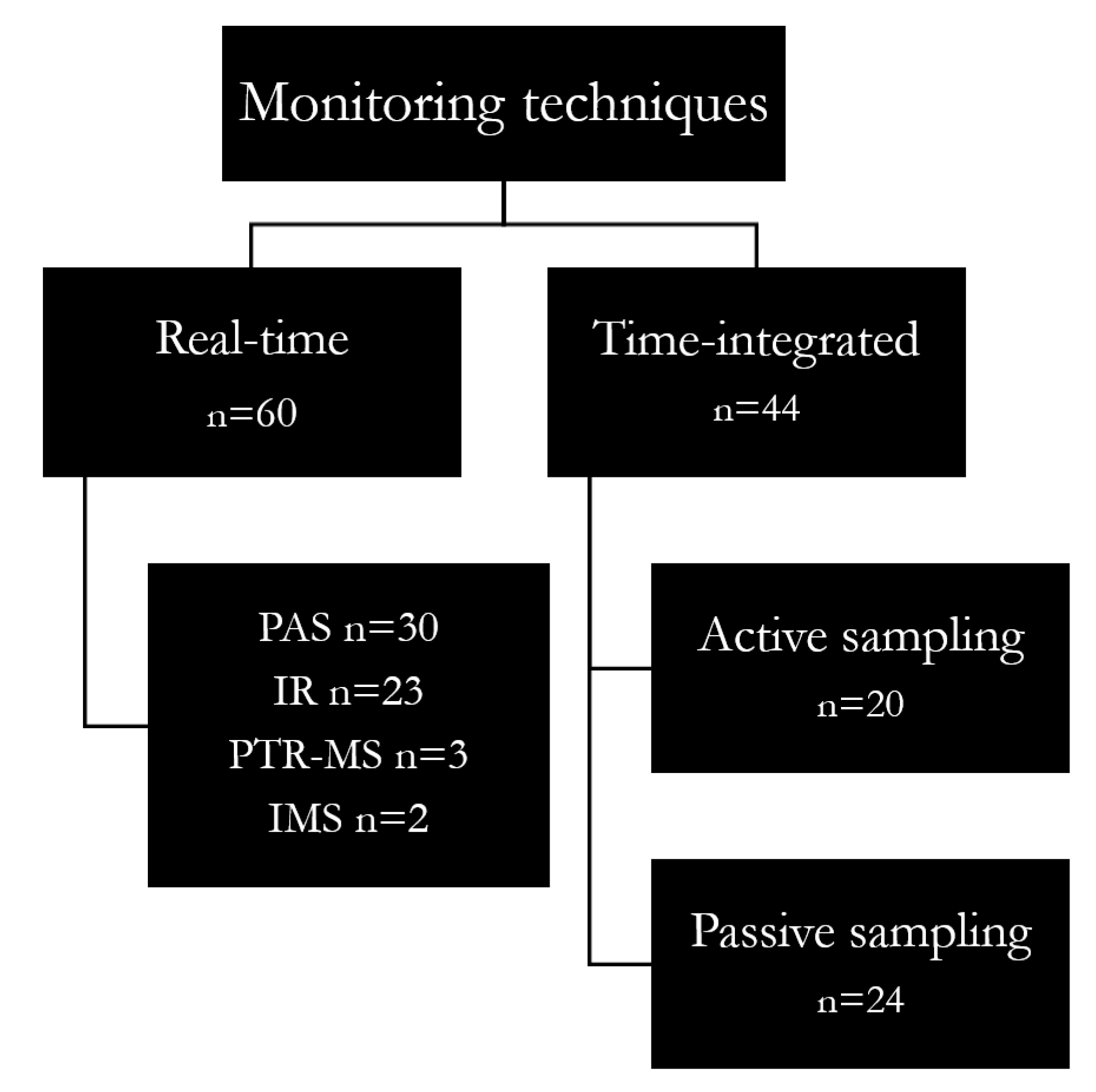
3.2. Types and Evolution in Monitoring Techniques
3.2.1. Real-Time Monitoring
3.2.2. Time-Integrated Sampling
3.2.3. Real-Time vs. Time-Integrated Monitoring
4. Overall Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vutskits, L.; Xie, Z. Lasting impact of general anaesthesia on the brain: Mechanisms and relevance. Nat. Rev. Neurosci. 2016, 32, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Herzog-Niescery, J.; Seipp, H.M.; Weber, T.P.; Bellgardt, M. Inhaled anesthetic agent sedation in the ICU and trace gas concentrations: A review. J. Clin. Monit. Comput. 2018, 32, 667–675. [Google Scholar] [CrossRef] [PubMed]
- Özelsel, T.J.P.; Kim, S.; Buro, K.; Tsui, B. Elevated waste anaesthetic gas concentration in the paediatric postanaesthesia care unit. Turk Anesteziyoloji ve Reanimasyon Dern. Derg. 2018, 46, 362–366. [Google Scholar] [CrossRef]
- Gustorff, B.; Lorenzl, N.; Aram, L.; Krenn, C.G.; Jobst, B.P.; Hoerauf, K.H. Environmental monitoring of sevoflurane and nitrous oxide using the cuffed oropharyngeal airway. Anesth. Analg. 2002, 94, 1244–1248. [Google Scholar] [CrossRef] [PubMed]
- Li, S.-H.; Li, S.-N.; Shih, H.-Y.; Yi, H.-D.; Chiang, C.-Y. Personnel Exposure to Waste Sevoflurane and Nitrous Oxide during General Anesthesia with Cuffed Endotracheal Tube. Acta Anaesthesiol. Sin. 2002, 40, 185–190. [Google Scholar]
- Saber, A.T.; Hougaard, K.S. Isoflurane, Sevoflurane and Desflurane: The Nordic Expert Group for Criteria Documentation of Health Risks from Chemicals; University of Gothenburg: Gothenburg, Sweden, 2009; Volume 43, ISBN 9789185971169. [Google Scholar]
- Byhahn, C.; Heller, K.; Lischke, V.; Westphal, K. Surgeon’s Occupational Exposure to Nitrous Oxide and Sevoflurane during Pediatric Surgery. World J. Surg 2001, 25, 1109–1112. [Google Scholar] [CrossRef]
- Herzog-Niescery, J.; Vogelsang, H.; Bellgardt, M.; Botteck, N.M.; Seipp, H.-M.M.; Bartz, H.; Weber, T.P.; Gude, P. The child’s behavior during inhalational induction and its impact on the anesthesiologist’s sevoflurane exposure. Paediatr. Anaesth. 2017, 27, 1247–1252. [Google Scholar] [CrossRef] [PubMed]
- Hoerauf, K.H.; Wallner, T.; Akça, O.; Taslimi, R.; Sessler, D.I. Exposure to sevoflurane and nitrous oxide during four different methods of anesthetic induction. Anesth. Analg. 1999, 88, 925–929. [Google Scholar] [CrossRef]
- Hoerauf, K.H.; Funk, W.; Harth, M.; Hobbhahn, J. Occupational exposure to sevoflurane, halothane and nitrous oxide during paediatric anaesthesia. Waste gas exposure during paediatric anaesthesia. Anaesthesia 1997, 52, 215–219. [Google Scholar] [CrossRef]
- Lucio, L.M.C.; Braz, M.G.; Nascimento Junior, P.D.; Braz, J.R.C.; Braz, L.G. Occupational hazards, DNA damage, and oxidative stress on exposure to waste anesthetic gases. Braz. J. Anesthesiol. 2018, 68, 33–41. [Google Scholar] [CrossRef]
- Zaffina, S.; Camisa, V.; Poscia, A.; Tucci, M.G.; Montaldi, V.; Cerabona, V.; Wahocka, M.; Moscato, U. Esposizione professionale al Sevoflurano nelle sale operatorie di pertinenza pediatrica: Il contributo del monitoraggio ambientale con tecnica multi-punto nella valutazione del rischio. G. Ital. Med. Lav. 2012, 24, 266–268. [Google Scholar]
- Oliveira, C.R.D. Occupational exposure to anesthetic gases residue. Rev. Bras. Anestesiol. 2009, 59, 110–124. [Google Scholar] [CrossRef] [PubMed]
- CCOHS Waste Anesthetic Gases, Hazards of. Ccohs.Ca. 2007. Available online: http://www.ccohs.ca/oshanswers/chemicals/waste_anesthetic.html (accessed on 25 November 2022).
- Borm, P.J.A.; Kant, I.; Houben, G.; van Rijssen-Moll, M.; Henderson, P.T. Monitoring of Nitrous Oxide in Operating Rooms:Identification of Sources and Estimation of Occupational Exposure. J. Occup. Environ. Med. 1990, 32, 1112–1116. [Google Scholar] [CrossRef]
- Da Costa, M.G.; Kalmar, A.F.; Struys, M.M.R.F. Inhaled Anesthetics: Environmental Role, Occupational Risk, and Clinical Use. J. Clin. Med. 2021, 10, 1306. [Google Scholar] [CrossRef] [PubMed]
- Kanmura, Y. Causes of nitrous oxide contamination in operating rooms. Anesthesiology 1999, 90, 693–696. [Google Scholar] [CrossRef]
- Krajewski, W.; Kucharska, M.; Wesolowski, W.; Stetkiewicz, J.; Wronska-Nofer, T. Occupational exposure to nitrous oxide—The role of scavenging and ventilation systems in reducing the exposure level in operating rooms. Int. J. Hyg. Environ. Health 2007, 210, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Cheung, S.K.; Özelsel, T.; Rashiq, S.; Tsui, B.C. Postoperative environmental anesthetic vapour concentrations following removal of the airway device in the operating room versus the posthanesthesia care unit. Can. J. Anesth. 2016, 63, 1016–1021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sárkány, P.; Tankó, B.; Simon, É.; Gál, J.; Fülesdi, B.; Molnár, C. Does standing or sitting position of the anesthesiologist in the operating theatre influence sevoflurane exposure during craniotomies? BMC Anesthesiol. 2016, 16, 120. [Google Scholar] [CrossRef] [Green Version]
- Scapellato, M.L.; Carrieri, M.; Maccà, I.; Salamon, F.; Trevisan, A.; Manno, M.; Bartolucci, G.B. Biomonitoring occupational sevoflurane exposure at low levels by urinary sevoflurane and hexafluoroisopropanol. Toxicol. Lett. 2014, 231, 154–160. [Google Scholar] [CrossRef]
- Yılmaz, S.; Çalbayram, N.Ç. Exposure to anesthetic gases among operating room personnel and risk of genotoxicity: A systematic review of the human biomonitoring studies. J. Clin. Anesth. 2016, 35, 326–331. [Google Scholar] [CrossRef]
- Deng, H.-B.; Li, F.-X.; Cai, Y.-H.; Xu, S.-Y. Waste anesthetic gas exposure and strategies for solution. J. Anesth. 2018, 32, 269–282. [Google Scholar] [CrossRef]
- Blokker-Veldhuis, M.J.; Rutten, P.M.M.J.; De Hert, S.G. Occupational exposure to sevoflurane during cardiopulmonary bypass. Perfusion 2011, 26, 383–389. [Google Scholar] [CrossRef]
- Casale, T.; Caciari, T.; Rosati, M.V.; Gioffrè, P.A.; Schifano, M.P.; Capozzella, A.; Pimpinella, B.; Tomei, G.; Tomei, F. Anesthetic gases and occupationally exposed workers. Environ. Toxicol. Pharmacol. 2014, 37, 267–274. [Google Scholar] [CrossRef]
- Herzog-Niescery, J.; Botteck, N.M.; Vogelsang, H.; Gude, P.; Bartz, H.; Weber, T.P.; Seipp, H.M. Occupational chronic sevoflurane exposure in the everyday reality of the anesthesia workplace. Anesth. Analg. 2015, 121, 1519–1528. [Google Scholar] [CrossRef]
- Varughese, S.; Bacher, H.P. Validation of Waste Anaesthetic Gas Exposure Limits When Using a Closed Vaporizer Filling System: A Laboratory-Based Study. Adv. Ther. 2020, 37, 450–456. [Google Scholar] [CrossRef] [Green Version]
- Berry, A.J. Recommended Exposure Limits for Desflurane and Isoflurane. Anesth. Analg. 1999, 88, 1424. [Google Scholar] [CrossRef]
- ACGIH. Threshold Limit Values (TLVs®) and Biological Exposure Indices (BEIs®); ACGIH: Washington, DC, USA, 2022; pp. 1–298. [Google Scholar]
- IFA GESTIS International Limit Values GESTIS International Limit Values. 2015. Available online: https://www.dguv.de/ifa/gestis/gestis-internationale-grenzwerte-fuer-chemische-substanzen-limit-values-for-chemical-agents/index-2.jsp (accessed on 25 November 2022).
- Accorsi, A.; Morrone, B.; Domenichini, I.; Valenti, S.; Raffi, G.B.; Violante, F.S. Urinary sevoflurane and hexafluoro-isopropanol as biomarkers of low-level occupational exposure to sevoflurane. Int. Arch. Occup. Environ. Health 2005, 78, 369–378. [Google Scholar] [CrossRef]
- Alessio, A.; Zadra, P.; Negri, S.; Maestri, L.; Imberti, R.; Ghittori, S.; Imbriani, M.; Cavalleri, A. Monitoraggio biologico dell’esposizione occupazionale a Desflurane. G. Ital. Med. Lav. 2003, 25, 137–141. [Google Scholar]
- Imbriani, M.; Zadra, P.; Negri, S.; Alessio, A.; Maestri, L.; Ghittori, S. Monitoraggio biologico dell’esposizione professionale a sevoflurane. Med. Del Lav. 2001, 92, 173–180. [Google Scholar]
- Aun, A.G.; Souza, K.M.; Guedes, J.L.; Figueiredo, D.B.S.; Lara, J.R.; Silva, M.A.P.; Braz, L.G.; Braz, M.G. Hepatotoxic and neuroendocrine effects in physicians occupationally exposed to most modern halogenated anesthetics and nitrous oxide. Environ. Toxicol. Pharmacol. 2021, 81, 103515. [Google Scholar] [CrossRef]
- Jakobsson, J. Desflurane: A clinical update of a third-generation inhaled anaesthetic. Acta Anaesthesiol. Scand. 2012, 56, 420–432. [Google Scholar] [CrossRef]
- Gentili, A.; Accorsi, A.; Pigna, A.; Bachiocco, V.; Domenichini, I.; Baroncini, S.; Violante, F.S. Exposure of personnel to sevoflurane during paediatric anaesthesia: Influence of professional role and anesthetic procedure. Eur. J. Anaesthesiol. 2004, 21, 638–645. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Moher, D. Updating guidance for reporting systematic reviews: Development of the PRISMA 2020 statement. J. Clin. Epidemiol. 2021, 134, 103–112. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Cattaneo, A.; Taronna, M.; Garramone, G.; Peruzzo, C.; Schlitt, C.; Consonni, D.; Cavallo, D.M. Comparison between personal and individual exposure to Urban air pollutants. Aerosol Sci. Technol. 2010, 44, 370–379. [Google Scholar] [CrossRef]
- Sloan, M.H.; Conard, P.F.; Karsunky, P.K.; Gross, J.B. Sevoflurane Versus Isoflurane: Induction and Recovery Characeristics with Single-Breath Inhaled Inductions of Anesthesia. Anesth. Analg. 1996, 82, 528–532. [Google Scholar]
- Behne, M.; Wilke, H.-J.; Harder, S. Clinical Pharmacokinetics of Sevoflurane; Adis International: Auckland, New Zealand, 1999. [Google Scholar]
- Patel, S.S.; Goa, K.L. Desflurane: A review of its pharmacodynamic and pharmacokinetic properties and its efficacy in general anaesthesia. Drugs 1995, 50, 742–767. [Google Scholar] [CrossRef]
- Hall, J.E.; Henderson, K.A.; Oldham, T.A.; Pugh, S.; Harmer, M. Environmental Monitoring during Gaseous Induction with Sevoflurane. Br. J. Anaesth. 1997, 79, 342–345. [Google Scholar] [CrossRef] [Green Version]
- Henderson, K.A.; Matthews, I.P. An environmental survey of compliance with occupational exposure standards (OES) for anaesthetic gases. Anaesthesia 1999, 54, 941–947. [Google Scholar] [CrossRef]
- Tanser, S.J.; Johnson, A. Evaluation of a new paediatric scavenging valve. Paediatr. Anaesth. 2002, 12, 448–450. [Google Scholar] [CrossRef]
- Velzen, J.; Atkinson, S.; Rowley, E.; Martin, J.L. The Tradition of Anaesthetic Rooms: Best Practice or Patient Risk? Procedia Manuf. 2015, 3, 59–66. [Google Scholar] [CrossRef] [Green Version]
- Hoerauf, K.H.; Harth, M.; Wild, K.; Hobbhahn, J. Occupational exposure to desflurane and isoflurane during cardiopulmonary bypass: Is the gas outlet of the membrane oxygenator an operating theatre pollution hazard? Br. J. Anaesth. 1997, 78, 378–380. [Google Scholar] [CrossRef]
- Braz, M.G.; Carvalho, L.I.M.; Chen, C.Y.O.; Blumberg, J.B.; Souza, K.M.; Arruda, N.M.; Filho, D.A.A.; Resende, L.O.; Faria, R.T.B.G.; Canário, C.d.A.; et al. High concentrations of waste anesthetic gases induce genetic damage and inflammation in physicians exposed for three years: A cross-sectional study. Indoor Air 2020, 30, 512–520. [Google Scholar] [CrossRef]
- Cakmak, G.; Eraydın, D.; Berkkan, A.; Yagar, S.; Burgaz, S. Genetic damage of operating and recovery room personnel occupationally exposed to waste anaesthetic gases. Hum. Exp. Toxicol. 2019, 38, 3–10. [Google Scholar] [CrossRef]
- Eroglu, A.; Celep, F.; Erciyes, N. A comparison of sister chromatid exchanges in lymphocytes of anesthesiologists to nonanesthesiologist in the same hospital. Anesth. Analg. 2006, 102, 1573–1577. [Google Scholar] [CrossRef]
- Gobbo Braz, L.; Reinaldo, J.; Braz, C.; Aparecido, G.; Cavalcante, S.; Souza, K.M.; Mendes De Carvalho Lucio, L.; Gobbo Braz, M. Comparison of waste anesthetic gases in operating rooms with or without an scavenging system in a Brazilian University Hospital. Braz. J. Anesthesiol. 2017, 67, 516–520. [Google Scholar] [CrossRef]
- Imberti, R.; Preseglio, I.; Imbriani, M.; Ghittori, S.; Cimino, F.; Mapelli, A. Low flow anaesthesia reduces occupational exposure to inhalation anaesthetics Environmental and biological measurements in operating room personnel. Acta Anaesthesiol. Scand. 1995, 39, 586–591. [Google Scholar] [CrossRef]
- Wiesner, G.; Harth, M.; Hoerauf, K.; Szulc, R.; Jurczyk, W.; Sobczynski, P.; Hobbhahn, J.; Taeger, K. Occupational exposure to inhaled anaesthetics: A follow-up study on anaesthetists of an eastern European university hospital. Int. Arch. Occup. Environ. Health 2000, 74, 16–20. [Google Scholar] [CrossRef]
- Elmer, J. An Analytical Comparison of Isoflurane Levels in Veterinary Operating Theaters. 2010. Available online: http://idea.library.drexel.edu/handle/1860/3581 (accessed on 25 November 2022).
- Haisch, C. Photoacoustic spectroscopy for analytical measurements. Meas. Sci. Technol. 2011, 23, 12001. [Google Scholar] [CrossRef]
- Christensen, J. Technical Review—Optical filters and their Use with the Type 1302 & Type 1306 Photoacoustic Gas Monitors. Tech. Rev. 1990, 2, 1–20. [Google Scholar]
- Herzog-Niescery, J.; Gude, P.; Gahlen, F.; Seipp, H.-M.; Bartz, H.; Botteck, N.M.; Bellgardt, M.; Dazert, S.; Weber, T.P.; Vogelsang, H. Surgeons’ exposure to sevoflurane during paediatric adenoidectomy: A comparison of three airway devices. Anaesthesia 2016, 71, 915–920. [Google Scholar] [CrossRef] [Green Version]
- Palzer, S. Photoacoustic-Based Gas Sensing: A Review. Sensors 2020, 20, 2745. [Google Scholar] [CrossRef]
- Hsu, C.-P.S. Infrared Spectroscopy. Handb. Instrum. Tech. Anal. Chem. 1997, 50, 466–476. [Google Scholar] [CrossRef]
- Gianella, M.; Hahnloser, D.; Rey, J.M.; Sigrist, M.W. Quantitative chemical analysis of surgical smoke generated during laparoscopic surgery with a vessel-sealing device. Surg. Innov. 2014, 21, 170–179. [Google Scholar] [CrossRef]
- Li, S.-H.; Li, S.-N.; Shih, H.-Y.; Chiou, S.-F.; Yi, H.-D. A local scavenging system to remove waste anesthetic gases during general anesthesia. Acta Anaesthesiol. Taiwan 2004, 42, 61–67. Available online: http://www.ncbi.nlm.nih.gov/pubmed/15346700 (accessed on 25 November 2022).
- Hansen, J.; Schaal, N.; Juarez, T.; Woodlee, C. Nitrous Oxide Exposure Among Dental Personnel and Comparison of Active and Passive Sampling Techniques. Ann. Work Expo. Health 2019, 63, 337–348. [Google Scholar] [CrossRef]
- Rieder, J.; Prazeller, P.; Boehler, M.; Lirk, P.; Lindinger, W.; Amann, A. Online monitoring of air quality at the postanesthetic care unit by proton-transfer-reaction mass spectrometry. Anesth. Analg. 2001, 92, 389–392. [Google Scholar] [CrossRef]
- Rieder, J.; Keller, C.; Brimacombe, J.; Gruber, G.; Lirk, P.; Summer, G.; Amann, A. Monitoring pollution by proton-transfer-reaction mass spectrometry during paediatric anaesthesia with positive pressure ventilation via the laryngeal mask airway or uncuffed tracheal tube. Anaesthesia 2002, 57, 663–666. [Google Scholar] [CrossRef]
- Summer, G.; Lirk, P.; Hoerauf, K.; Riccabona, U.; Bodrogi, F.; Raifer, H.; Deibl, M.; Rieder, J.; Schobersberger, W. Sevoflurane in exhaled air of operating room personnel. Anesth. Analg. 2003, 97, 1070–1073. [Google Scholar] [CrossRef]
- De Gouw, J.; Warneke, C.; Karl, T.; Eerdekens, G.; Van der Veen, C.; Fall, R. Sensitivity and specificity of atmospheric trace gas detection by proton-transfer-reaction mass spectrometry. Int. J. Mass Spectrom. 2003, 223, 365–382. [Google Scholar] [CrossRef]
- Heiderich, S.; Thoben, C.; Dennhardt, N.; Koppert, W.; Krauß, T.; Sümpelmann, R.; Zimmermann, S.; Klingler, W. Low anaesthetic waste gas concentrations in postanaesthesia care unit. Eur. J. Anaesthesiol. 2018, 35, 534–538. [Google Scholar] [CrossRef]
- Kunze, N.; Weigel, C.; Vautz, W.; Schwerdtfeger, K.; Jünger, M.; Quintel, M.; Perl, T. Multi-capillary column-ion mobility spectrometry (MCC-IMS) as a new method for the quantification of occupational exposure to sevoflurane in anaesthesia workplaces: An observational feasibility study. J. Occup. Med. Toxicol. 2015, 10, 12. [Google Scholar] [CrossRef] [Green Version]
- Hill, H.H.; Simpson, G. Capabilities and limitations of ion mobility spectrometry for field screening applications. F. Anal. Chem. Technol. 1997, 1, 119–134. [Google Scholar] [CrossRef]
- Zabiegała, B.; Kot-Wasik, A.; Urbanowicz, M.; Namieśnik, J. Passive sampling as a tool for obtaining reliable analytical information in environmental quality monitoring. Anal. Bioanal. Chem. 2010, 396, 273–296. [Google Scholar] [CrossRef]
- Jafari, A.; Bargeshadi, R.; Jafari, F.; Mohebbi, I.; Hajaghazadeh, M. Environmental and biological measurements of isoflurane and sevoflurane in operating room personnel. Int. Arch. Occup. Environ. Health 2018, 91, 349–359. [Google Scholar] [CrossRef]
- Imbriani, M.; Ghittori, S.; Pezzagno, G. The Biological Monitoring of Inhalation Anaesthetics. G. Ital. Med. Lav. Ergon. 1998, 20, 44–49. [Google Scholar]
- Cope, K.A.; Merritt, W.T.; Krenzischek, D.A.; Schaefer, J.; Bukowski, J.; Foster, W.M.; Bernacki, E.; Dorman, T.; Risby, T.H. Phase II collaborative pilot study: Preliminary analysis of central neural effects from exposure to volatile anesthetics in the PACU. J. Perianesthesia Nurs. 2002, 17, 240–250. [Google Scholar] [CrossRef]
- Prado, C.; Periago, F.; Ibarra, I.; Tortosa, J. Evaluation of isoflurane in air by thermal desorption-gas chromatography. J. Chromatogr. A 1993, 657, 131–137. [Google Scholar] [CrossRef]
- Sessler, D.I.; Badgwell, J.M. Exposure of postoperative nurses to exhaled anesthetic gases. Anesth. Analg. 1998, 87, 1083–1088. [Google Scholar] [CrossRef]
- Herzog-Niescery, J.; Steffens, T.; Bellgardt, M.; Breuer-Kaiser, A.; Gude, P.; Vogelsang, H.; Weber, T.P.; Seipp, H.M. Photoacoustic gas monitoring for anesthetic gas pollution measurements and its cross-sensitivity to alcoholic disinfectants. BMC Anesthesiol. 2019, 19, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaljurand, M.; Gorbatšova, J.; Mazina-Šinkar, J. A gas chromatograph for citizen science. Microchem. J. 2021, 165, 106195. [Google Scholar] [CrossRef]
- Ritzu, S.; Boccalon, P.; Sanchez, M.A.; Arcangeli, G.; Capelli, V. Esposizione a gas anestetici: Risultati di 13 anni di monitoraggio ambientale e biologico in un’ azienda ospedaliera. G. Ital. Med. Lav. 2007, 29, 411. [Google Scholar]
- Virgili, A.; Scapellato, M.L.; Maccà, I.; Perini, M.; Carrieri, M.; Gori, G.; Saia, B.; Bartolucci, G.B. Esposizione professionale a gas anestetici in alcuni ospedali del Veneto. G. Ital. Med. Lav. 2002, 24, 447–450. [Google Scholar]
- Sackey, P.V.; Martling, C.R.; Nise, G.; Radell, P.J. Ambient isoflurane pollution and isoflurane consumption during intensive care unit sedation with the Anesthetic Conserving Device. Crit. Care Med. 2005, 33, 585–590. [Google Scholar] [CrossRef]
- Fanti, G.; Borghi, F.; Spinazzè, A.; Rovelli, S.; Campagnolo, D.; Keller, M.; Cattaneo, A.; Cauda, E.; Cavallo, D.M. Features and practicability of the next-generation sensors and monitors for exposure assessment to airborne pollutants: A systematic review. Sensors 2021, 21, 4513. [Google Scholar] [CrossRef]
- EN 482:2021; Workplace Exposure—Procedures for the Determination of the Concentration of Chemical Agents—Basic Performance Requirements. CEN-European Committee for Standardization: Brussels, Belgium, 2021; pp. 20–21.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Isoflurane | Sevoflurane | Desflurane | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Limit Value 8 h | Limit Value Short Term | Limit Value 8 h | Limit Value Short Term | Limit Value 8 h | Limit Value Short Term | |||||||
| ppm | mg/m3 | ppm | mg/m3 | ppm | mg/m3 | ppm | mg/m3 | ppm | mg/m3 | ppm | mg/m3 | |
| Austria | 10 | 80 | 20 | 160 | ||||||||
| Canada-Ontario | 2 | 15 | ||||||||||
| Denmark | 5 | 38 | 10 (1) | 76 (1) | 5 | 35 | 10 (1) | 70 (1) | ||||
| Finland | 10 | 77 | 20 (1) | 150 (1) | 10 | 83 | 20 (1) | 170(1) | 10 | 70 | 20 (1) | 140 (1) |
| Ireland | 50 | 380 | ||||||||||
| Israel | 2 | 15 | 6 (1) | 45 (1) | 2 (1) | 16 (1) | ||||||
| Norway | 2 | 15 | 5 | 35 | 5 | 35 | ||||||
| Poland | 32 | 55 | 125 | |||||||||
| Spain | 50 | 383 | ||||||||||
| Sweden | 10 | 80 | 20 (1) | 150 (1) | 10 | 80 | 20 (1) | 170 (1) | 10 | 70 | 20 (1) | 140 (1) |
| Switzerland | 10 | 77 | 80 | 616 | ||||||||
| UK | 50 | 383 | ||||||||||
| Database | Search Query |
|---|---|
| Scopus | (TITLE-ABS-KEY ((((occupational OR workplace OR work) AND (exposure OR monitoring) AND (sevoflurane OR isoflurane OR desflurane) OR (“anaesthetic gases”)))) AND LANGUAGE (english OR italian)) |
| PubMed | ((((occupational OR workplace OR work) AND (exposure OR monitoring) AND (sevoflurane OR isoflurane OR desflurane) OR (“anaesthetic gases”)))) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Keller, M.; Cattaneo, A.; Spinazzè, A.; Carrozzo, L.; Campagnolo, D.; Rovelli, S.; Borghi, F.; Fanti, G.; Fustinoni, S.; Carrieri, M.; et al. Occupational Exposure to Halogenated Anaesthetic Gases in Hospitals: A Systematic Review of Methods and Techniques to Assess Air Concentration Levels. Int. J. Environ. Res. Public Health 2023, 20, 514. https://doi.org/10.3390/ijerph20010514
Keller M, Cattaneo A, Spinazzè A, Carrozzo L, Campagnolo D, Rovelli S, Borghi F, Fanti G, Fustinoni S, Carrieri M, et al. Occupational Exposure to Halogenated Anaesthetic Gases in Hospitals: A Systematic Review of Methods and Techniques to Assess Air Concentration Levels. International Journal of Environmental Research and Public Health. 2023; 20(1):514. https://doi.org/10.3390/ijerph20010514
Chicago/Turabian StyleKeller, Marta, Andrea Cattaneo, Andrea Spinazzè, Letizia Carrozzo, Davide Campagnolo, Sabrina Rovelli, Francesca Borghi, Giacomo Fanti, Silvia Fustinoni, Mariella Carrieri, and et al. 2023. "Occupational Exposure to Halogenated Anaesthetic Gases in Hospitals: A Systematic Review of Methods and Techniques to Assess Air Concentration Levels" International Journal of Environmental Research and Public Health 20, no. 1: 514. https://doi.org/10.3390/ijerph20010514