
Relationship between Drug Holidays of Antiresorptive Agents and Surgical Outcomes in Cancer Patients with Medication-Related Osteonecrosis of the Jaw

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patients
2.2. Variables
2.3. Statistical Analyses
2.4. Ethical Approval
3. Results
3.1. Patient Characteristics
3.2. Factors Related to Separation of Sequestrum
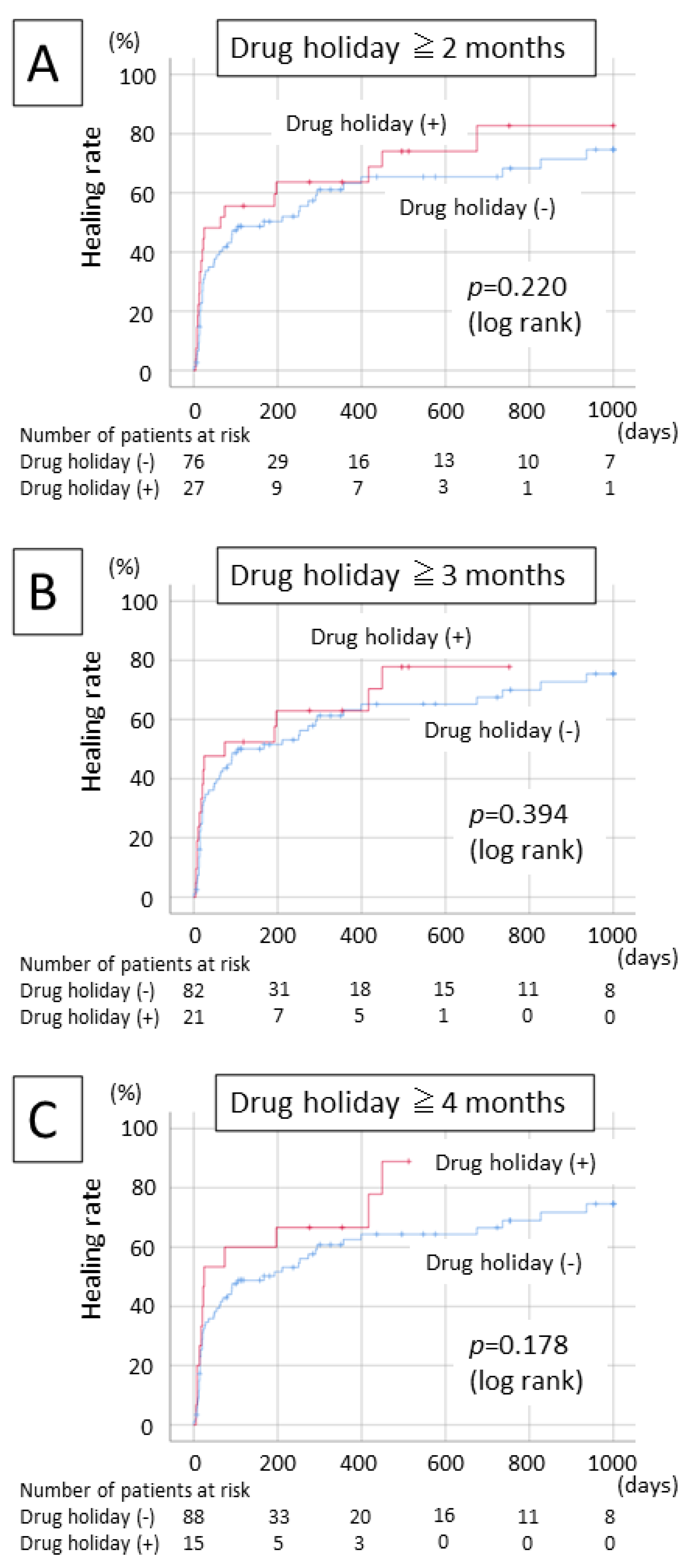
3.3. Relationship between a Drug Holiday before Surgery and Treatment Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yarom, N.; Shapiro, C.L.; Peterson, D.E.; Van Poznak, C.H.; Bohlke, K.; Ruggiero, S.L.; Migliorati, C.A.; Khan, A.; Morrison, A.; Anderson, H.; et al. Medication-Related Osteonecrosis of the Jaw: MASCC/ISOO/ASCO Clinical Practice Guideline. J. Clin. Oncol. 2019, 37, 2270–2290. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, S.L.; Dodson, T.B.; Fantasia, J.; Goodday, R.; Aghaloo, T.; Mehrotra, B.; O’Ryan, F.; American Association of Oral and Maxillofacial Surgeons. American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw—2014 update. J. Oral. Maxillofac. Surg. 2014, 72, 938–956. [Google Scholar] [CrossRef]
- Yoneda, T.; Hagino, H.; Sugimoto, T.; Ohta, H.; Takahashi, S.; Soen, S.; Taguchi, A.; Nagata, T.; Urade, M.; Shibahara, T.; et al. Antiresorptive agent-related osteonecrosis of the jaw: Position Paper 2017 of the Japanese Allied Committee on Osteonecrosis of the Jaw. J. Bone Miner. Metab. 2017, 35, 6–19. [Google Scholar] [CrossRef] [PubMed]
- Rupel, K.; Ottaviani, G.; Gobbo, M.; Contardo, L.; Tirelli, G.; Vescovi, P.; Di Lenarda, R.; Biasotto, M. A systematic review of therapeutical approaches in bisphosphonates-related osteonecrosis of the jaw (BRONJ). Oral Oncol. 2014, 50, 1049–1057. [Google Scholar] [CrossRef] [PubMed]
- Fliefel, R.; Tröltzsch, M.; Kühnisch, J.; Ehrenfeld, M.; Otto, S. Treatment strategies and outcome of bisphosphonate-related osteonecrosis of the jaw (BRONJ) with characterization of patients: A systematic review. Int. J. Oral Maxillofac. Surg. 2015, 44, 568–585. [Google Scholar] [CrossRef] [PubMed]
- Khan, A.A.; Morrison, A.; Hanley, D.A.; Felsenberg, D.; McCauley, L.K.; O’Ryan, F.; Reid, I.R.; Ruggiero, S.L.; Taguchi, A.; Tetradis, S.; et al. Diagnosis and management of osteonecrosis of the jaw: A systematic review and international consensus. J. Bone Miner. Res. 2015, 30, 3–23. [Google Scholar] [CrossRef] [PubMed]
- Hayashida, S.; Soutome, S.; Yanamoto, S.; Fujita, S.; Hasegawa, T.; Komori, T.; Kojima, Y.; Miyamoto, H.; Shibuya, Y.; Ueda, N.; et al. Evaluation of the treatment strategies for medication-related osteonecrosis of the jaws (MRONJ) and the factors affecting treatment outcome: A multicenter retrospective study with propensity score matching analysis. J. Bone Miner. Res. 2017, 32, 2022–2029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruggiero, S.L.; Dodson, T.B.; Assael, L.A.; Landesberg, R.; Marx, R.E.; Mehrotra, B.; American Association of Oral and Maxillofacial Surgeons. American Association of Oral and Maxillofacial Surgeons position paper on bisphosphonate-related osteonecrosis of the jaws—2009 Update. J. Oral Maxillofac. Surg. 2009, 67, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Hellstein, J.W.; Adler, R.A.; Edwards, B.; Jacobsen, P.L.; Kalmar, J.R.; Koka, S.; Migliorati, C.A.; Ristic, H.; American Dental Association Council on Scientific Affairs Expert Panel on Antiresorptive Agents. Managing the care of patients receiving antiresorptive therapy for prevention and treatment of osteoporosis: Executive summary of recommendations from the American Dental Association Council on Scientific Affairs. J. Am. Dent. Assoc. 2011, 142, 1243–1251. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damm, D.D.; Jones, D.M. Bisphosphonate-related osteonecrosis of the jaws: A potential alternative to drug holidays. Gen. Dent. 2013, 61, 33–38. [Google Scholar] [PubMed]
- Kim, J.W.; Kwak, M.K.; Han, J.J.; Lee, S.T.; Kim, H.Y.; Kim, S.H.; Jung, J.; Lee, J.K.; Lee, Y.K.; Kwon, Y.D.; et al. Medication related osteonecrosis of the jaw: 2021 Position Statement of the Korean Society for Bone and Mineral Research and the Korean Association of Oral and Maxillofacial Surgeons. J. Bone Metab. 2021, 28, 279–296. [Google Scholar] [CrossRef] [PubMed]
- Hayashida, S.; Yanamoto, S.; Fujita, S.; Hasegawa, T.; Komori, T.; Kojima, Y.; Miyamoto, H.; Shibuya, Y.; Ueda, N.; Kirita, T.; et al. Drug holiday clinical relevance verification for antiresorptive agent in medication-related osteonecrosis cases of the jaw. J. Bone Miner. Metab. 2020, 38, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Baron, R.; Ferrari, S.; Graham, R.; Russell, G. Denosumab and bisphosphonates: Different mechanisms of action and effects. Bone 2011, 48, 677–692. [Google Scholar] [CrossRef] [PubMed]
- Hanley, D.A.; Adachi, J.D.; Bell, A.; Brown, V. Denosumab: Mechanism of action and clinical outcomes. Int. J. Clin. Pract. 2012, 66, 1139–1146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasegawa, T.; Kawakita, A.; Ueda, N.; Funahara, R.; Tachibana, A.; Kobayashi, M.; Kondou, E.; Takeda, D.; Kojima, Y.; Sato, S.; et al. A multicenter retrospective study of the risk factors associated with medication-related osteonecrosis of the jaw after tooth extraction in patients receiving oral bisphosphonate therapy: Can primary wound closure and a drug holiday really prevent MRONJ? Osteoporos. Int. 2017, 28, 2465–2473. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, T.; Hayashida, S.; Kondo, E.; Takeda, Y.; Miyamoto, H.; Kawaoka, Y.; Ueda, N.; Iwata, E.; Nakahara, H.; Kobayashi, M.; et al. Medication-related osteonecrosis of the jaw after tooth extraction in cancer patients: A multicenter retrospective study. Osteoporos. Int. 2019, 30, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, T.; Ueda, N.; Yamada, S.I.; Kato, S.; Iwata, E.; Hayashida, S.; Kojima, Y.; Shinohara, M.; Tojo, I.; Nakahara, H.; et al. Denosumab-related osteonecrosis of the jaw after tooth extraction and the effects of a short drug holiday in cancer patients: A multicenter retrospective study. Osteoporos. Int. 2021, 32, 2323–2333. [Google Scholar] [CrossRef] [PubMed]
- Morishita, K.; Otsuru, M.; Soutome, S.; Hayashida, S.; Murata, M.; Umeda, M. Duration of drug holiday of oral bisphosphonate and osteoclast morphology in osteoporosis patients with medication-related osteonecrosis of the jaw. J. Oral Maxillofac. Surg. Med. Pathol. 2022, 10, 1140. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Number of Patients/Mean ± SD | |
|---|---|---|
| Sex | man | 45 |
| woman | 58 | |
| Age | (years) | 70.3 ± 10.7 |
| Primary disease | solid cancer | 88 |
| myeloma | 15 | |
| MRONJ site | upper jaw | 39 |
| lower jaw | 64 | |
| MRONJ stage | stage 1 | 11 |
| stage 2 | 70 | |
| stage 3 | 22 | |
| Antiresorptive agent | BP | 37 |
| Dmab | 42 | |
| BP→Dmab | 24 | |
| Use of steroid | (−) | 81 |
| (+) | 22 | |
| Diabetes | (−) | 79 |
| (+) | 24 | |
| Duration of administration | <4 years | 67 |
| ≧4 years | 34 | |
| unknown | 2 | |
| Duration of drug holiday before CT examination | (days) | 34.1 ± 78.0 |
| ≧60 days | 22 | |
| ≧90 days | 17 | |
| ≧120 days | 11 | |
| Duration of drug holiday before surgery | (days) | 69.2 ± 171.9 |
| ≧60 days | 27 | |
| ≧90 days | 21 | |
| ≧120 days | 15 | |
| Leukocytes | (/µL) | 6387 ± 1813 |
| Albumin | (g/dL) | 3.69 ± 0.522 |
| Creatinine | (mg/dL) | 0.889 ± 0.396 |
| Extent of osteolytic area | localized | 75 |
| extended | 28 | |
| Periosteal reaction | (−) | 75 |
| (+) | 28 | |
| Separation of sequestrum | (−) | 94 |
| (+) | 9 | |
| Surgical procedure | marginal resection | 94 |
| segmental resection | 9 | |
| Total | 103 |
| Variable | Separation of Sequestrum (−) | Separation of Sequestrum (+) | p-Value | |
|---|---|---|---|---|
| Sex | man | 42 | 3 | 0.728 |
| woman | 52 | 6 | ||
| Age | 70.3 ± 10.7 | 70.2 ± 9.30 | 0.993 | |
| Primary disease | solid cancer | 81 | 7 | 0.616 |
| myeloma | 13 | 2 | ||
| MRONJ site | upper jaw | 35 | 4 | 0.727 |
| lower jaw | 59 | 5 | ||
| MRONJ stage | stage 1 | 9 | 2 | 0.424 |
| stage 2 | 64 | 6 | ||
| stage 3 | 21 | 1 | ||
| Antiresorptive agent | BP | 33 | 4 | 0.482 |
| Dmab | 40 | 2 | ||
| BP→Dmab | 21 | 3 | ||
| use of steroid | (−) | 72 | 9 | 0.199 |
| (+) | 22 | 0 | ||
| Diabetes | (−) | 72 | 7 | 1.000 |
| (+) | 22 | 2 | ||
| Duration of administration | <4 years | 64 | 5 | 0.473 |
| ≧4 years | 30 | 4 | ||
| Drug holiday before CT ≧ 60 days | (−) | 76 | 5 | 0.095 |
| (+) | 18 | 4 | ||
| Drug holiday before CT ≧ 90 days | (−) | 79 | 7 | 0.641 |
| (+) | 15 | 2 | ||
| Drug holiday before CT ≧ 120 days | (−) | 85 | 7 | 0.246 |
| (+) | 9 | 2 | ||
| Leukocytes | (/µL) | 6192 ± 1854 | 6120 ± 1150 | 0.932 |
| Albumin | (g/dL) | 3.67 ± 0.529 | 3.84 ± 0.441 | 0.392 |
| Creatinine | (mg/dL) | 0.912 ± 0.396 | 0.908 ± 0.413 | 0.975 |
| Extent of osteolytic area | localized | 70 | 5 | 0.250 |
| extended | 24 | 4 | ||
| Periosteal reaction | (−) | 70 | 5 | 0.250 |
| (+) | 24 | 4 | ||
| Surgical procedure | marginal resection | 90 | 8 | 0.373 |
| segmental resection | 4 | 1 |
| Variable | Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|---|
| p-Value | HR | 95% CI | p-Value | HR | 95% CI | ||
| Sex | woman/man | 0.765 | 0.93 | 0.579–1.492 | |||
| Age | (years) | 0.062 | 0.997 | 0.975–1.019 | |||
| Primary disease | multiple myeloma/solid cancer | 0.769 | 0.911 | 0.486–1.704 | |||
| MRONJ site | lower jaw/upper jaw | 0.083 | 0.653 | 0.403–1.058 | |||
| MRONJ stage | stage 3/2/1 | 0.59 | 0.892 | 0.590–1.350 | |||
| Antiresorptive agent | BP→Dmab/Dmab/BP | 0.22 | 0.821 | 0.600–1.125 | |||
| use of steroid | (+)/(−) | 0.408 | 0.788 | 0.449–1.385 | 0.043 | 0.494 | 0.250–0.977 |
| Diabetes | (+)/(−) | 0.208 | 1.398 | 0.830–2.354 | |||
| Duration of administration | ≧4 years/<4 years | 0.918 | 0.974 | 0.590–1.608 | |||
| Drug holiday before surgery ≧90 days | (+)/(−) | 0.398 | 1.281 | 0.720–2.283 | |||
| Leukocytes | (/µL) | 0.124 | 1 | 0.999–1.000 | |||
| Albumin | (g/dL) | 0.068 | 0.659 | 0.421–1.032 | |||
| Creatinine | (mg/dL) | 0.074 | 1.789 | 0.946–3.383 | 0.003 | 2.787 | 1.410–5.509 |
| Extent of osteolytic area | Extended/localized | 0.22 | 1.387 | 0.822–2.341 | 0.014 | 2.233 | 1.176–4.238 |
| Periosteal reaction | (+)/(−) | 0.266 | 0.727 | 0.415–1.274 | |||
| Separation of sequestrum | (+)/(−) | 0.532 | 1.308 | 0.564–3.032 | |||
| Surgical procedure | segmental resection/margical resection | 0.605 | 1.307 | 0.474–3.601 | |||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otsuru, M.; Soutome, S.; Omori, K.; Suyama, K.; Morishita, K.; Hayashida, S.; Murata, M.; Takagi, Y.; Sasaki, M.; Sumi, M.; et al. Relationship between Drug Holidays of Antiresorptive Agents and Surgical Outcomes in Cancer Patients with Medication-Related Osteonecrosis of the Jaw. Int. J. Environ. Res. Public Health 2022, 19, 4624. https://doi.org/10.3390/ijerph19084624
Otsuru M, Soutome S, Omori K, Suyama K, Morishita K, Hayashida S, Murata M, Takagi Y, Sasaki M, Sumi M, et al. Relationship between Drug Holidays of Antiresorptive Agents and Surgical Outcomes in Cancer Patients with Medication-Related Osteonecrosis of the Jaw. International Journal of Environmental Research and Public Health. 2022; 19(8):4624. https://doi.org/10.3390/ijerph19084624
Chicago/Turabian StyleOtsuru, Mitsunobu, Sakiko Soutome, Keisuke Omori, Koki Suyama, Kota Morishita, Saki Hayashida, Maho Murata, Yukinori Takagi, Miho Sasaki, Misa Sumi, and et al. 2022. "Relationship between Drug Holidays of Antiresorptive Agents and Surgical Outcomes in Cancer Patients with Medication-Related Osteonecrosis of the Jaw" International Journal of Environmental Research and Public Health 19, no. 8: 4624. https://doi.org/10.3390/ijerph19084624