
Esthetic Assessment following Ridge Augmentation, Late Implant Placement and Immediate Esthetic Reconstruction of the Atrophic Anterior Maxilla


 , , , and
, , , and
Abstract
:1. Introduction
2. Methods and Materials
- Missing teeth in the anterior maxilla characterized by extensive bone loss of at least 3 mm horizontally and at least 3 mm vertically according to primary cone beam computerized tomography (CBCT).
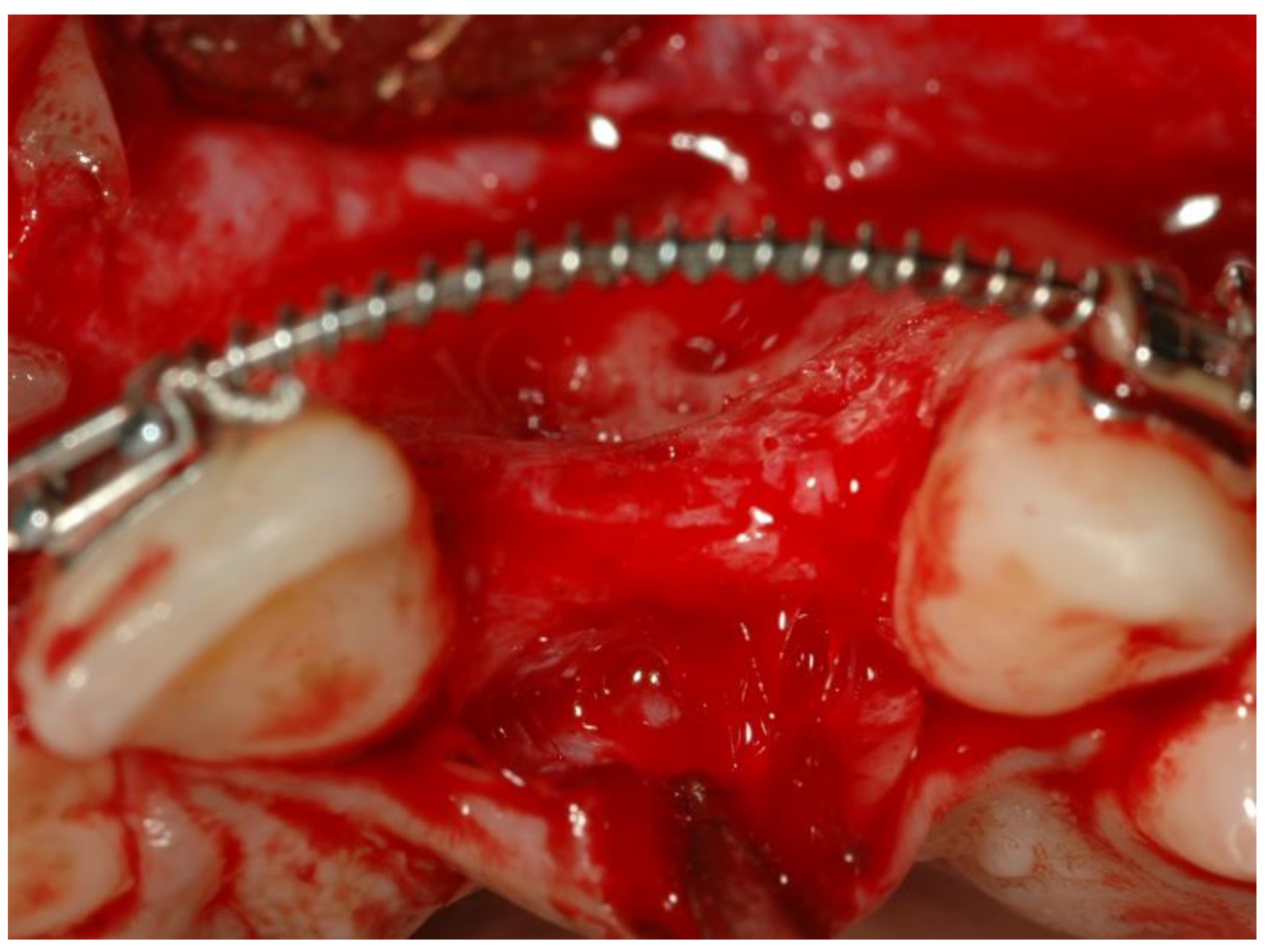
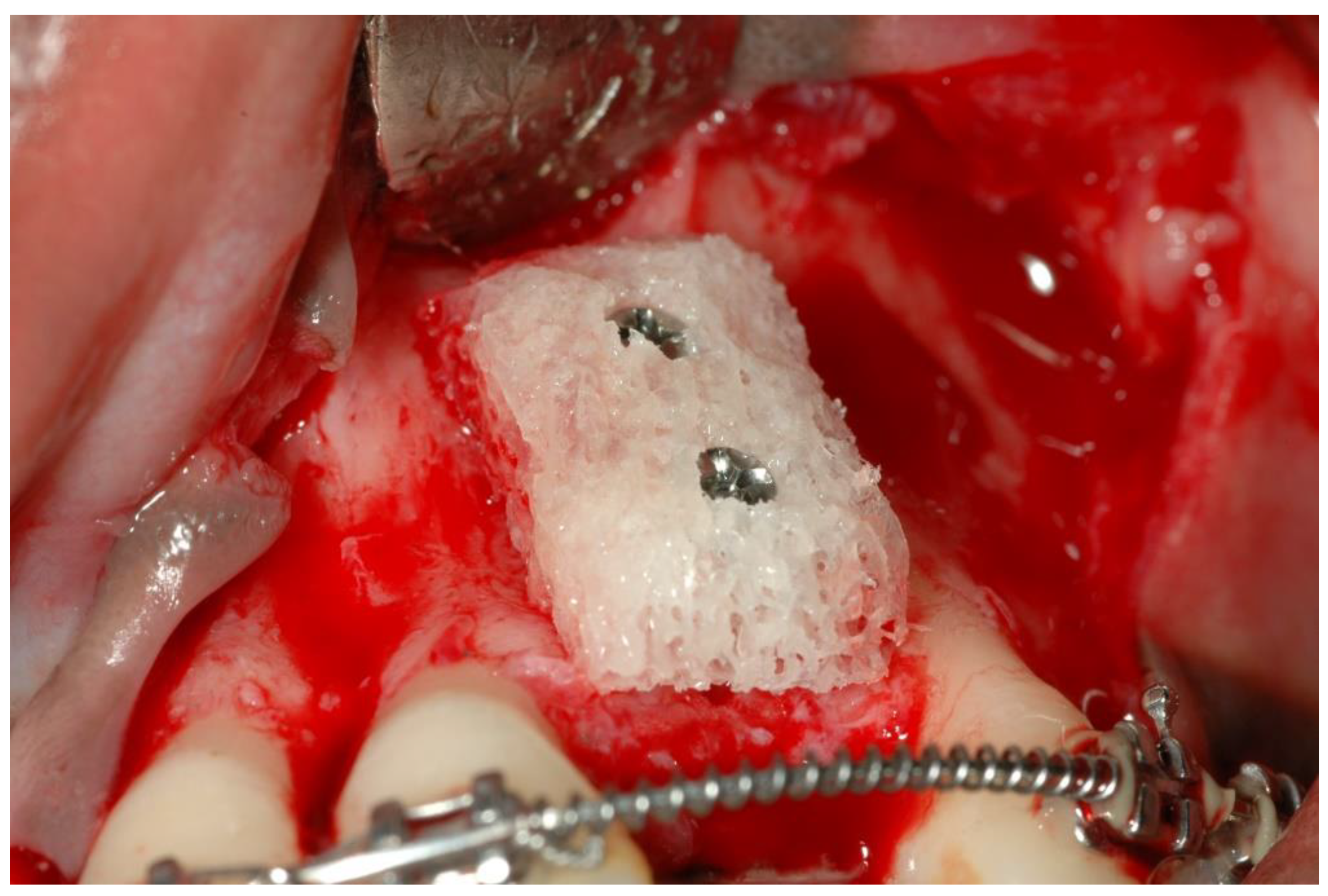
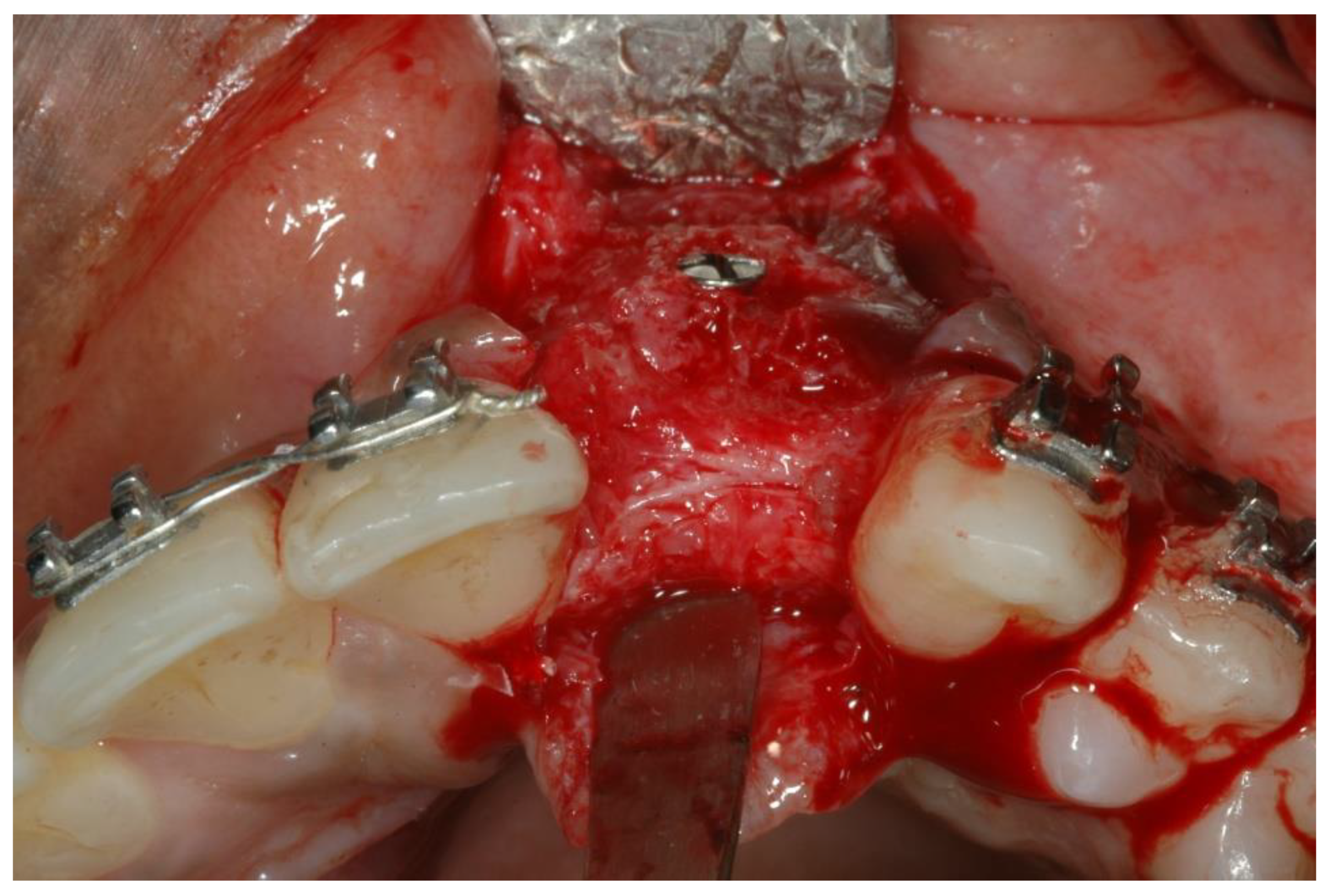
- Bone augmentations using cancellous allogeneic bone-blocks.
- Six months later, implant insertion followed immediately by a temporary restoration placement.
- Age > 18 years.
- No active periodontal disease (after initial preparation).
- Existing posterior occlusal support and antagonist natural dentition.
- Implant insertion at bone level.
- Similar permanent ISP metal-free porcelain crown type performed in the same laboratory.
- Periodic follow-up once a year.
- Unbalanced systemic diseases (e.g., diabetes).
- History of radiation to the head and neck area.
- Poor oral hygiene. (plaque index > 20%).
- Diseases of the mucous membranes (e.g., lichen planus).
- Parafunction (e.g., bruxism).
- Use of medications (e.g., bisphosphonates, calcium channels blockers as amlodipine, hydantoin, cyclosporine).
- Untreated and uncontrolled periodontal disease.
- Heavy smoking >10 cigarettes a day.
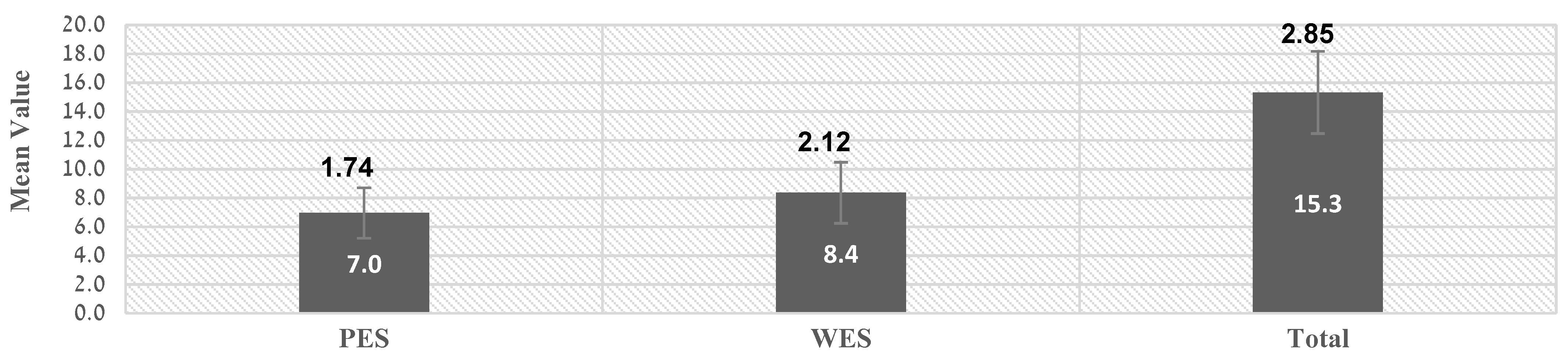
2.1. PES Index
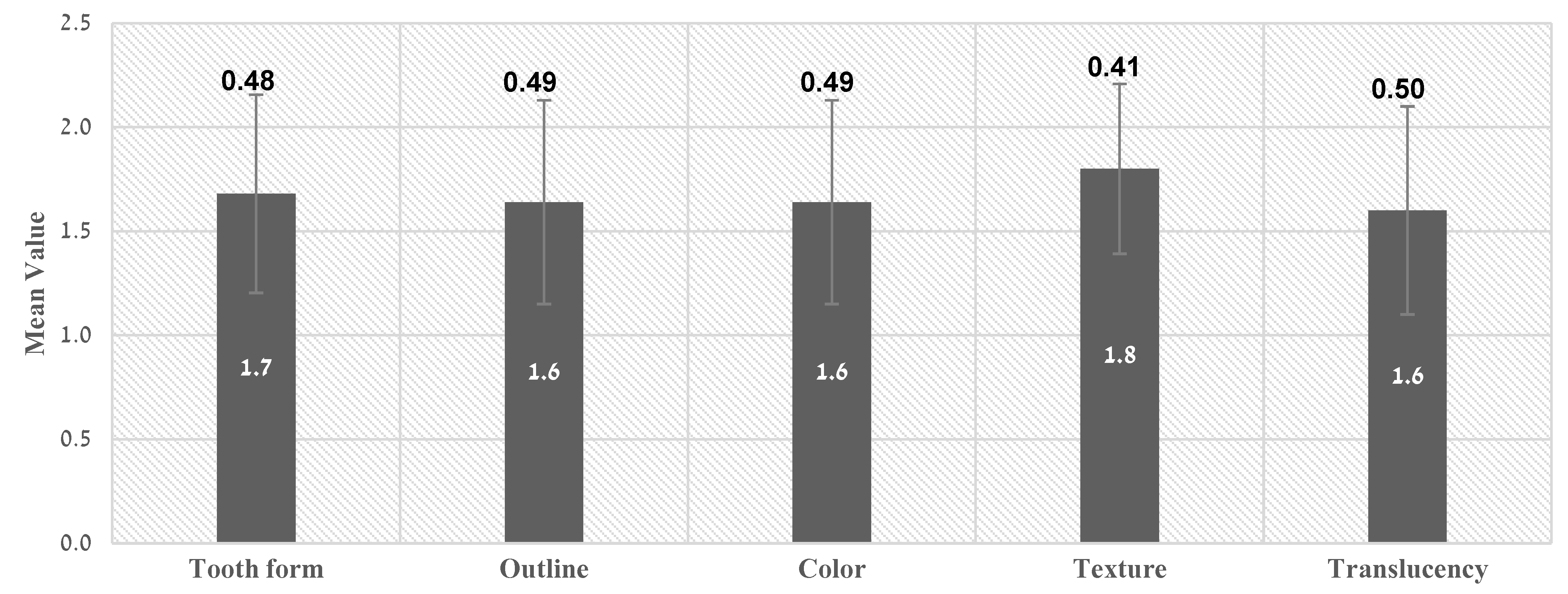
2.2. WES Index
2.3. Statistical Analysis
3. Results
3.1. Esthetic Evaluation of Treatment Results Using PES/WES Indices
3.2. Analysis of Esthetic Results According to PES Values
3.3. Analysis of Esthetic Results According to WES Values
3.4. Multivariate Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Boardman, N.; Darby, I.; Chen, S. A retrospective evaluation of aesthetic outcomes for single-tooth implants in the anterior maxilla. Clin. Oral Implant. Res. 2016, 27, 443–451. [Google Scholar] [CrossRef] [PubMed]
- Grunder, U.; Gracis, S.; Capelli, M. Influence of the 3-D bone-to-implant relationship on esthetics. Int. J. Periodontics Restor. Dent. 2005, 25, 113–119. [Google Scholar]
- Belser, U.C.; Grütter, L.; Vailati, F.; Bornstein, M.M.; Weber, H.P.; Buser, D. Outcome evaluation of early placed maxillary anterior single-tooth implants using objective esthetic criteria: A cross-sectional, retrospective study in 45 patients with a 2- to 4-year follow-up using pink and white esthetic scores. J. Periodontol. 2009, 80, 140–151. [Google Scholar] [CrossRef] [PubMed]
- Lanza, A.; Di Francesco, F.; De Marco, G.; Femiano, F.; Itro, A. Clinical application of the PES/WES index on natural teeth: Case report and literature review. Case Rep. Dent. 2017, 2017, 9659062. [Google Scholar] [CrossRef]
- Vidigal, G.; Groisman, M.; Clavijo, V.; Santos, I.; Fischer, R. Evaluation of pink and white esthetic scores for immediately placed and provisionally restored implants in the anterior maxilla. Int. J. Oral Maxillofac. Implant. 2017, 32, 625–632. [Google Scholar] [CrossRef]
- Geurs, N.C.; Korostoff, J.M.; Vassilopoulos, P.J.; Kang, T.H.; Jeffcoat, M.; Kellar, R.; Reddy, M.S. Clinical and histologic assessment of lateral alveolar ridge augmentation using a synthetic long-term bioabsorbable membrane and an allograft. J. Periodontol. 2008, 79, 1133–1140. [Google Scholar] [CrossRef]
- Bartee, B.K. Extraction site reconstruction for alveolar ridge preservation. Part 1: Rationale and materials selection. J. Oral Implantol. 2001, 27, 187–193. [Google Scholar] [CrossRef]
- Lekovic, V.; Camargo, P.M.; Klokkevold, P.R.; Weinlaender, M.; Kenney, E.B.; Dimitrijevic, B.; Nedic, M. Preservation of alveolar bone in extraction sockets using bioabsorbable membranes. J. Periodontol. 1998, 69, 1044–1049. [Google Scholar] [CrossRef]
- Buser, D.; Wittneben, J.; Bornstein, M.M.; Grütter, L.; Chappuis, V.; Belser, U.C. Stability of contour augmentation and esthetic outcomes of implant-supported single crowns in the esthetic zone: 3-year results of a prospective study with early implant placement postextraction. J. Periodontol. 2011, 82, 342–349. [Google Scholar] [CrossRef]
- Nissan, J.; Marilena, V.; Gross, O.; Mardinger, O.; Chaushu, G. Histomorphometric analysis following augmentation of the anterior atrophic maxilla with cancellous bone block allograft. Int. J. Oral Maxillofac. Implant. 2012, 27, 84–89. [Google Scholar]
- Nissan, J.; Mardinger, O.; Strauss, M.; Peleg, M.; Sacco, R.; Chaushu, G. Implant-supported restoration of congenitally missing teeth using cancellous bone block-allografts. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 111, 286–291. [Google Scholar] [CrossRef] [PubMed]
- Schnettler, R.; Franke, J.; Rimashevskiy, D.; Zagorodniy, N.; Batpenov, N.; Unger, R.E.; Wenisch, S.; Barbeck, M. Allogeneic bone grafting materials–update of the current scientific status. Traumatol. Orthop. Russ. 2017, 23, 92–100. [Google Scholar] [CrossRef] [Green Version]
- Nissan, J.; Gross, O.; Mardinger, O.; Ghelfan, O.; Sacco, R.; Chaushu, G. Post-traumatic implant-supported restoration of the anterior maxillary teeth using cancellous bone block allografts. J. Oral Maxillofac. Surg. 2011, 69, e513–e518. [Google Scholar] [CrossRef] [PubMed]
- Tribst, J.P.; Dal Piva, A.M.; Lo Giudice, R.; Borges, A.L.; Bottino, M.A.; Epifania, E.; Ausiello, P. The influence of custom-milled framework design for an implant-supported full-arch fixed dental prosthesis: 3D-FEA study. Int. J. Environ. Res. Public Health 2020, 17, 4040. [Google Scholar] [CrossRef] [PubMed]
- Kolerman, R.; Nissan, J.; Mijiritsky, E.; Hamoudi, N.; Mangano, C.; Tal, H. Esthetic assessment of immediately restored implants combined with GBR and free connective tissue graft. Clin. Oral Implant. Res. 2016, 27, 1414–1422. [Google Scholar] [CrossRef]
- Nissan, J.; Mardinger, O.; Calderon, S.; Romanos, G.E.; Chaushu, G. Cancellous bone block allografts for the augmentation of the anterior atrophic maxilla. Clin. Implant. Dent. Relat. Res. 2011, 13, 104–111. [Google Scholar] [CrossRef]
- Nissan, J.; Romanos, G.E.; Mardinger, O.; Chaushu, G. Immediate nonfunctional loading of single-tooth implants in the anterior maxilla following augmentation with freeze-dried cancellous block allograft: A case series. Int. J. Oral Maxillofac. Implant. 2008, 23, 709–716. [Google Scholar]
- Chochlidakis, K.M.; Geminiani, A.; Papaspyridakos, P.; Singh, N.; Ercoli, C.; Chen, C.J. Buccal bone thickness around single dental implants in the maxillary esthetic zone. Quint. Int. 2017, 48, 295–308. [Google Scholar]
- Esposito, M.; Hirsch, J.M.; Lekholm, U.; Thomsen, P. Biological factors contributing to failures of osseointegrated oral implants. (I). Success criteria and epidemiology. Eur. J. Oral Sci. 1998, 106, 527–551. [Google Scholar] [CrossRef]
- Naishlos, S.; Zenziper, E.; Zelikman, H.; Nissan, J.; Mizrahi, S.; Chaushu, G.; Matalon, S.; Chaushu, L. Esthetic assessment succeeding anterior atrophic maxilla augmentation with cancellous bone-block allograft and late restoration loading. J. Clin. Med. 2021, 10, 4635. [Google Scholar] [CrossRef]
- Gjelvold, B.; Kisch, J.; Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Clinical and radiographic outcome following immediate loading and delayed loading of single-tooth implants: Randomized clinical trial. Clin. Implant. Dent. Relat. Res. 2017, 19, 549–558. [Google Scholar] [CrossRef]
- Belser, U.C.; Schmid, B.; Higginbottom, F.; Buser, D. Outcome analysis of implant restorations located in the anterior maxilla: A review of the recent literature. Int. J. Oral Maxillofac. Implant. 2004, 19, 30–42. [Google Scholar]
- Schropp, L. Bone healing and soft tissue contour changes following single-tooth extraction: A clinical and radiographic 12-month prospective study. J. Prosthet. Dent. 2003, 23, 303–323. [Google Scholar]
- Cardaropoli, G.; Lekholm, U.; Wennstro, J.L. Tissue alterations at implant-supported single-tooth replacements: A 1-year prospective clinical study. Clin. Oral Implant. Res. 2006, 17, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Spray, J.R.; Black, C.G.; Morris, H.F.; Ochi, S. The influence of bone thickness on facial marginal bone response: Stage 1 placement through stage 2 uncovering. Ann. Periodontol. 2005, 5, 119–128. [Google Scholar] [CrossRef] [PubMed]
- Jurczyk, K.; Belser, U.; Sculean, A. The management of peri-implant mucosa deficiencies in esthetic sites: Case report of a combined surgical-prosthetic approach. Int. J. Periodontics Restor. Dent. 2017, 37, 809–817. [Google Scholar] [CrossRef] [Green Version]
- Gross, M.D.; Nissan, J.; Samuel, R. Stress distribution around maxillary implants in anatomic photoelastic models of varying geometry. Part I. J. Prosthet. Dent. 2001, 85, 450–454. [Google Scholar] [CrossRef]
- McAllister, B.S.; Haghighat, K. Bone augmentation techniques. J. Periodontol. 2007, 78, 377–396. [Google Scholar] [CrossRef] [Green Version]
- Fürhauser, R.; Florescu, D.; Benesch, T.; Haas, R.; Mailath, G.; Watzek, G. Evaluation of soft tissue around single-tooth implant crowns: The pink esthetic score. Clin. Oral Implant. Res. 2005, 16, 639–644. [Google Scholar] [CrossRef]
- Yildiz, P.; Zortuk, M.; Kilic, E.; Dincel, M.; Albayrak, H. Esthetic outcomes after immediate and late implant loading for a single missing tooth in the anterior maxilla. Niger. J. Clin. Pract. 2018, 21, 1164–1170. [Google Scholar]
- Raes, F.; Cosyn, J.; De Bruyn, H. Clinical, aesthetic, and patient-related outcome of immediately loaded single implants in the anterior maxilla: A prospective study in extraction sockets, healed ridges, and grafted sites. Clin. Implant. Dent. Relat. Res. 2013, 15, 819–835. [Google Scholar] [CrossRef] [PubMed]
- Gjelvold, B.; Kisch, J.; Mohammed, D.; Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Immediate loading of single implants, guided surgery, and intraoral scanning: A nonrandomized study. Int. J. Prosthod. 2020, 33, 513–522. [Google Scholar] [CrossRef] [PubMed]
- Wessels, R.; Vervaeke, S.; Seyssens, L.; Eghbali, A.; Cosyn, J. A 5-year cohort study on early implant placement with guided bone regeneration or alveolar ridge preservation with connective tissue graft. Clin. Implant. Dent. Relat. Res. 2020, 22, 697–705. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| WES | PES | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Patient | Implant
Site | Total
PES + WES | Total
WES | Trans-Lucency | Texture | Color | Outline | Tooth Form | Total
PES | Root
Convexity | Level of Facial
Mucosa | Curvature
of Facial Mucosa | Distal Papilla | Mesial Papilla |
| 1 | 11 | 12 | 6 | 1 | 2 | 1 | 1 | 1 | 6 | 1 | 1 | 1 | 2 | 1 |
| 2 | 12 | 12 | 7 | 1 | 2 | 1 | 1 | 2 | 5 | 1 | 1 | 1 | 1 | 1 |
| 3 | 12 | 15 | 10 | 2 | 2 | 2 | 2 | 2 | 5 | 1 | 1 | 1 | 1 | 1 |
| 4 | 22 | 19 | 10 | 2 | 2 | 2 | 2 | 2 | 9 | 2 | 2 | 2 | 2 | 1 |
| 5 | 11 | 19 | 10 | 2 | 2 | 2 | 2 | 2 | 9 | 2 | 2 | 2 | 2 | 1 |
| 6 | 22 | 19 | 10 | 2 | 2 | 2 | 2 | 2 | 9 | 2 | 2 | 2 | 2 | 1 |
| 7 | 21 | 19 | 10 | 2 | 2 | 2 | 2 | 2 | 9 | 2 | 2 | 2 | 2 | 1 |
| 8 | 21 | 15 | 10 | 2 | 2 | 2 | 2 | 2 | 5 | 1 | 1 | 1 | 1 | 1 |
| 9 | 22 | 13 | 5 | 1 | 1 | 1 | 1 | 1 | 8 | 1 | 2 | 2 | 2 | 1 |
| 10 | 21 | 14 | 7 | 1 | 1 | 1 | 2 | 2 | 7 | 1 | 2 | 2 | 1 | 1 |
| 11 | 12 | 15 | 10 | 2 | 2 | 2 | 2 | 2 | 5 | 1 | 1 | 1 | 1 | 1 |
| 12 | 22 | 15 | 10 | 2 | 2 | 2 | 2 | 2 | 5 | 1 | 1 | 1 | 1 | 1 |
| 13 | 21 | 17 | 10 | 2 | 2 | 2 | 2 | 2 | 7 | 0 | 2 | 2 | 2 | 1 |
| 14 | 22 | 12 | 5 | 1 | 1 | 1 | 1 | 1 | 7 | 0 | 2 | 2 | 2 | 1 |
| 15 | 21 | 13 | 5 | 1 | 1 | 1 | 1 | 1 | 8 | 1 | 2 | 2 | 2 | 1 |
| 16 | 22 | 13 | 5 | 1 | 1 | 1 | 1 | 1 | 8 | 1 | 2 | 2 | 2 | 1 |
| 17 | 21 | 18 | 10 | 2 | 2 | 2 | 2 | 2 | 8 | 1 | 2 | 2 | 2 | 1 |
| 18 | 11 | 20 | 10 | 2 | 2 | 2 | 2 | 2 | 10 | 2 | 2 | 2 | 2 | 2 |
| 19 | 21 | 20 | 10 | 2 | 2 | 2 | 2 | 2 | 10 | 2 | 2 | 2 | 2 | 2 |
| 20 | 12 | 15 | 10 | 2 | 2 | 2 | 2 | 2 | 5 | 1 | 1 | 1 | 1 | 1 |
| 21 | 11 | 17 | 10 | 2 | 2 | 2 | 2 | 2 | 7 | 1 | 1 | 2 | 2 | 1 |
| 22 | 12 | 15 | 10 | 2 | 2 | 2 | 2 | 2 | 5 | 1 | 1 | 1 | 1 | 1 |
| 23 | 12 | 12 | 7 | 1 | 2 | 2 | 1 | 1 | 5 | 1 | 1 | 1 | 1 | 1 |
| 24 | 22 | 12 | 6 | 1 | 2 | 1 | 1 | 1 | 6 | 1 | 1 | 1 | 1 | 2 |
| 25 | 23 | 12 | 6 | 1 | 2 | 1 | 1 | 1 | 6 | 1 | 1 | 2 | 1 | 1 |
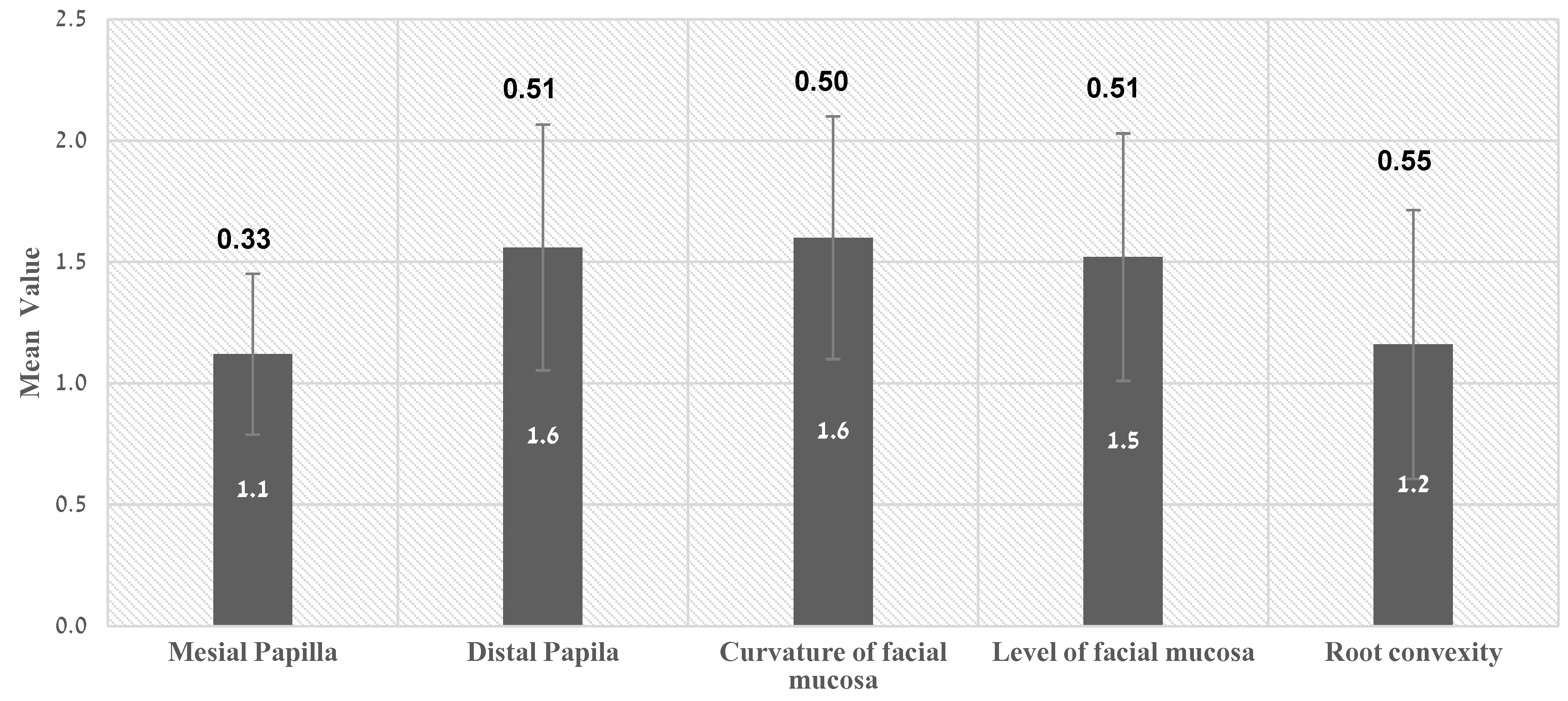
| Average | 15.3 | 8.4 | 1.6 | 1.8 | 1.6 | 1.6 | 1.7 | 7 | 1.2 | 1.5 | 1.6 | 1.6 | 1.1 | |
| SD | 2.85 | 2.12 | 0.50 | 0.41 | 0.49 | 0.49 | 0.48 | 1.74 | 0.55 | 0.51 | 0.50 | 0.51 | 0.33 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naishlos, S.; Reiser, V.; Zelikman, H.; Nissan, J.; Masri, D.; Nassra, H.; Chaushu, G.; Blumer, S.; Chaushu, L. Esthetic Assessment following Ridge Augmentation, Late Implant Placement and Immediate Esthetic Reconstruction of the Atrophic Anterior Maxilla. Int. J. Environ. Res. Public Health 2022, 19, 3689. https://doi.org/10.3390/ijerph19063689
Naishlos S, Reiser V, Zelikman H, Nissan J, Masri D, Nassra H, Chaushu G, Blumer S, Chaushu L. Esthetic Assessment following Ridge Augmentation, Late Implant Placement and Immediate Esthetic Reconstruction of the Atrophic Anterior Maxilla. International Journal of Environmental Research and Public Health. 2022; 19(6):3689. https://doi.org/10.3390/ijerph19063689
Chicago/Turabian StyleNaishlos, Sarit, Vadim Reiser, Helena Zelikman, Joseph Nissan, Daya Masri, Hiba Nassra, Gavriel Chaushu, Sigalit Blumer, and Liat Chaushu. 2022. "Esthetic Assessment following Ridge Augmentation, Late Implant Placement and Immediate Esthetic Reconstruction of the Atrophic Anterior Maxilla" International Journal of Environmental Research and Public Health 19, no. 6: 3689. https://doi.org/10.3390/ijerph19063689