
Sexual and Reproductive Health during the COVID-19 Pandemic: Results from a Cross-Sectional Online Survey in Germany


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants and Recruitment
2.3. Measures
2.4. Data Analysis
2.5. Quantitative Analysis
2.6. Qualitative Analysis
3. Results
3.1. Sociodemographic Characteristics
3.2. COVID-19 Impact on Daily Life
3.3. Sexual Behaviours and Experiences
3.4. Reasons for Changes in Sexual Behaviour
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Anaya, J.-M.; Rojas, M.; Salinas, M.L.; Rodríguez, Y.; Roa, G.; Lozano, M.; Rodríguez-Jiménez, M.; Montoya, N.; Zapata, E.; Monsalve, D.M.; et al. Post-COVID Syndrome. A Case Series and Comprehensive Review. Autoimmun. Rev. 2021, 20, 102947. [Google Scholar] [CrossRef]
- Ammar, A.; Trabelsi, K.; Brach, M.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of Home Confinement on Mental Health and Lifestyle Behaviours during the COVID-19 Outbreak: Insight from the ECLB-COVID19 Multicenter Study. Biol. Sport 2021, 38, 9. [Google Scholar] [CrossRef]
- Hussein, J. COVID-19: What Implications for Sexual and Reproductive Health and Rights Globally? Sex. Reprod. Health Matters 2020, 28, 1746065. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bolarinwa, O.A.; Ahinkorah, B.O.; Seidu, A.-A.; Ameyaw, E.K.; Saeed, B.Q.; Hagan, J.E.; Nwagbara, U.I. Mapping Evidence of Ompacts of COVID-19 Outbreak on Sexual and Reproductive Health: A Scoping Review. Healthcare 2021, 9, 436. [Google Scholar] [CrossRef] [PubMed]
- Kotlar, B.; Gerson, E.; Petrillo, S.; Langer, A.; Tiemeier, H. The Impact of the COVID-19 Pandemic on Maternal and Perinatal Health: A Scoping Review. Reprod. Health 2021, 18, 1–39. [Google Scholar] [CrossRef] [PubMed]
- Pennanen-Iire, C.; Prereira-Lourenço, M.; Padoa, A.; Ribeirinho, A.; Samico, A.; Gressler, M.; Jatoi, N.-A.; Mehrad, M.; Girard, A. Sexual Health Implications of COVID-19 Pandemic. Sex. Med. Rev. 2021, 9, 3. [Google Scholar] [CrossRef] [PubMed]
- Viero, A.; Barbara, G.; Montisci, M.; Kustermann, K.; Cattaneo, C. Violence against Women in the Covid-19 Pandemic: A Review of the Literature and a Call for Shared Strategies to Tackle Health and Social Emergencies. Forensic Sci. Int. 2021, 319, 110650. [Google Scholar] [CrossRef]
- Li, G.; Tang, D.; Song, B.; Wang, C.; Qunshan, S.; Xu, C.; Geng, H.; Wu, H.; He, X.; Cao, Y. Impact of the COVID-19 Pandemic on Partner Relationships and Sexual and Reproductive Health: Cross-Sectional, Online Survey Study. J. Med. Internet Res. 2020, 22, e20961. [Google Scholar] [CrossRef]
- Sanchez, T.H.; Zlotorzynska, M.; Rai, M.; Baral, S.D. Characterizing the Impact of COVID-19 on Men Who Have Sex with Men across the United States in April, 2020. AIDS Behav. 2020, 24, 2024–2032. [Google Scholar] [CrossRef]
- Saso, A.; Skirrow, H.; Kampmann, B. Impact of COVID-19 on Immunization Services for Maternal and Infant Vaccines: Results of a Survey Conducted by Imprint—The Immunising Pregnant Women and Infants Network. Vaccines 2020, 8, 556. [Google Scholar] [CrossRef]
- Caruso, S.; Rapisarda, A.M.C.; Minona, P. Sexual Activity and Contraceptive Use during Social Distancing and Self-Isolation in the COVID-19 Pandemic. Eur. J. Contracept. Reprod. Health Care 2020, 25, 445–448. [Google Scholar] [CrossRef]
- Yuksel, B.; Ozgor, F. Effect of the COVID-19 Pandemic on Female Sexual Behavior. Int. J. Gynecol. Obstet. 2020, 150, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Rothe, C.; Schunk, M.; Sothmann, P.; Bretzel, G.; Froeschl, G.; Wallrauch, C.; Zimmer, T.; Thiel, V.; Janke, C.; Guggemos, W.; et al. Transmission of 2019-NCoV Infection from an Asymptomatic Contact in Germany. N. Engl. J. Med. 2020, 382, 970–971. [Google Scholar] [CrossRef] [Green Version]
- Bundesministerium für Gesundheit Coronavirus-Pandemie (SARS-CoV-2): Chronik Bisheriger Maßnahmen Und Ereignisse. Available online: https://www.bundesgesundheitsministerium.de/coronavirus/chronik-coronavirus.html (accessed on 22 October 2021).
- Reitzle, L.; Schmidt, C.; Färber, F.; Huebl, L.; Wieler, L.H.; Ziese, T.; Heidemann, C. Perceived Access to Health Care Services and Relevance of Telemedicine during the COVID-19 Pandemic in Germany. Int. J. Environ. Res. Public Health 2021, 18, 7661. [Google Scholar] [CrossRef]
- Paffenholz, P.; Peine, A.; Hellmich, M.; Paffenholz, S.V.; Martin, L.; Luedde, M.; Haverkamp, M.; Roderburg, C.; Marx, G.; Heidenreich, A.; et al. Perception of the 2020 SARS-CoV-2 Pandemic among Medical Professionals in Germany: Results from a Nationwide Online Survey. Emerg. Microbes Infect. 2020, 9, 1590–1599. [Google Scholar] [CrossRef] [PubMed]
- Heidemann, C.; Paprott, R.; Huebl, L.; Scheidt-Nave, C.; Reitzle, L. Selbst Eingeschätzte Medizinische Versorgung Im Verlauf Der SARS-CoV-2-Pandemie in Deutschland: Ergebnisse Der COSMO-Studie. Epidemiol. Bull. 2020, 46, 3–10. [Google Scholar] [CrossRef]
- Barjenbruch, M.; Mangiapane, S.; Zhu, L.; Kretschmann, J.; Czihal, T.; von Stillfried, D. Veränderung in der Vertragsärztlichen Leistungsinanspruchnahme Während der COVID-Krise: Tabellarischer Trendreport für das Jahr 2020; Zentralinstitut für die kassenärztliche Versorgung in der Bundesrepublik Deutschland: Berlin, Germany, 2021. [Google Scholar]
- Peters, A.; Rospleszcz, S.; Greiser, K.H.; Dallavalle, M.; Berger, K. The Impact of the COVID-19 Pandemic on Self-Reported Health. Dtsch. Aerzteblatt Online 2020, 117, 861–867. [Google Scholar] [CrossRef]
- Schröder, J.; Bruns, E.; Schoon, W.; Briken, P.; Schöttle, D. Changes in Sexual Interests and Experiences during the COVID-19 Pandemic—A Qualitative Content Analysis. Psychotherapeut 2021, 66, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Panzeri, M.; Ferrucci, R.; Cozza, A.; Fontanesi, L. Changes in Sexuality and Quality of Couple Relationship during the COVID-19 Lockdown. Front. Psychol. 2020, 11, 565823. [Google Scholar] [CrossRef]
- Bodenmann, G.; Atkins, D.C.; Schär, M.; Poffet, V. The Association between Daily Stress and Sexual Activity. J. Fam. Psychol. 2010, 24, 271–279. [Google Scholar] [CrossRef]
- Hall, K.S.; Kusunoki, Y.; Gatny, H.; Barber, J. Stress Symptoms and Frequency of Sexual Intercourse among Young Women. J. Sex. Med. 2014, 11, 1982–1990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ballester-Arnal, R.; Nebot-Garcia, J.E.; Ruiz-Palomino, E.; Giménez-García, C.; Gil-Llario, M.D. “INSIDE” Project on Sexual Health in Spain: Sexual Life during the Lockdown Caused by COVID-19. Sex. Res. Soc. Policy 2020, 8, 1023–1041. [Google Scholar] [CrossRef]
- Torres, T.S.; Hoagland, B.; Bezerra, D.R.B.; Garner, A.; Jalil, E.M.; Coelho, L.E.; Benedetti, M.; Pimenta, C.; Grinsztejn, B.; Veloso, V.G. Impact of COVID-19 Pandemic on Sexual Minority Populations in Brazil: An Analysis of Social/Racial Disparities in Maintaining Social Distancing and a Description of Sexual Behavior. AIDS Behav. 2021, 25, 73–84. [Google Scholar] [CrossRef] [PubMed]
- Coombe, J.; Kong, F.Y.S.; Bittleston, H.; Williams, H.; Tomnay, J.; Vaisey, A.; Malta, S.; Goller, J.L.; Temple-Smith, M.; Bourchier, L.; et al. Love during Lockdown: Findings from an Online Survey Examining the Impact of COVID-19 on the Sexual Health of People Living in Australia. Sex. Transm. Infect. 2020, 97, 357–362. [Google Scholar] [CrossRef]
- Pornhub Coronavirus Insights. Available online: https://www.pornhub.com/insights/corona-virus (accessed on 8 July 2021).
- Lehmiller, J.J.; Garcia, J.R.; Gesselman, A.N.; Mark, K.P. Less Sex, but More Sexual Diversity: Changes in Sexual Behavior during the COVID-19 Coronavirus Pandemic. Leis. Sci. 2021, 43, 295–304. [Google Scholar] [CrossRef]
- Enarson, E. Violence against Women in Disasters. Violence Against Women 1999, 5, 742–768. [Google Scholar] [CrossRef]
- Neil, J. Domestic Violence and COVID-19: Our Hidden Epidemic. Aust. J. Gen. Pract. 2020, 49. [Google Scholar] [CrossRef]
- Parkinson, D.; Zara, C. The Hidden Disaster: Domestic Violence in the Aftermath of Natural Disaster. Aust. J. Emerg. Manag. 2013, 28, 28–35. [Google Scholar] [CrossRef]
- Mahase, E. Covid-19: EU States Report 60% Rise in Emergency Calls about Domestic Violence. Br. Med. J. 2020, 369, m1872. [Google Scholar]
- Michielsen, K.; Larrson, E.C.; Kågesten, A.; Erausquin, J.T.; Griffin, S.; van de Velde, S.; Tucker, J.D. International Sexual Health and REproductive Health (I-SHARE) Survey during COVID-19: Study Protocol for Online National Surveys and Global Comparative Analyses. Sex. Transm. Infect. 2021, 97, 88–92. [Google Scholar] [CrossRef]
- World Medical Association WMA Declaration of Helsinki. Ethical Principles for Medical Reserach Involving Human Subjects. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 25 January 2022).
- Mayring, P. Qualitative Inhaltsanalyse. Grundlagen Und Techniken; Beltz: Weinheim, Germany, 2003. [Google Scholar]
- Cohen, J. Statistical Power Analysis for the Behavioural Sciences; Routledge: New York, NY, USA, 1988. [Google Scholar]
- Harwell, M.R.; Rubinstein, E.N.; Hayes, W.S.; Olds, C.C. Summarizing Monte Carlo Results in Methodological Research: The One- and Two-Factor Fixed Effects ANOVA Cases. J. Educ. Stat. 1992, 17, 315–339. [Google Scholar] [CrossRef]
- United Nations Population Fund. Impact of the COVID-19 Pandemic on Family Planning and Ending Gender-Based Violence, Female Genital Mutilation and Child Marriage: Interim Technical Note Information as of 27 April 2020; United Nations Population Fund: New York, NY, USA, 2020. [Google Scholar]
- World Health Organization. COVID-19 and Violence Against Women: What the Health Sector/System Can Do. Available online: https://www.who.int/docs/default-source/reproductive-health/covid-19-vaw-full-text.pdf (accessed on 25 January 2022).
- Telles, L.E.; Valenca, A.M.; Barros, A.J.; da Silva, A.G. Domestic Violence in the COVID-19 Pandemic: A Forensic Psychiatric Perspective. Braz. J. Psychiatry 2021, 43, 233–234. [Google Scholar] [CrossRef] [PubMed]
- Briken, P. An Integrated Model to Assess and Treat Compulsive Sexual Behaviour Disorder. Nat. Rev. Urol. 2020, 17, 391–406. [Google Scholar] [CrossRef] [PubMed]
- Shih, J.H. Sex Differences in Stress Generation: An Examination of Sociotropy/Autonomy, Stress, and Depressive Symptoms. Personal. Soc. Psychol. Bull. 2006, 32, 434–446. [Google Scholar] [CrossRef]
- Bancroft, J.; Janssen, E.; Carnes, L.; Vukadinovic, Z.; Long, S.J. The Relation between Mood and Sexuality in Heterosexual Men. Arch. Sex. Behav. 2003, 32, 217–230. [Google Scholar] [CrossRef]
- Reid, R.C.; Carpenter, B.N.; Lloyd, T.Q. Assessing Psychological Symptom Patterns of Patients Seeking Help for Hypersexual Behavior. Sex. Relatsh. Ther. 2009, 24, 47–63. [Google Scholar] [CrossRef]
- Cocci, A.; Giunti, D.; Tonioni, C.; Cacciamani, G.; Tellini, R.; Polloni, G.; Cito, G.; Presicce, F.; di Mauro, M.; Minervini, A.; et al. Love at the Time of the Covid-19 Pandemic: Preliminary Results of an Online Survey Conducted during the Quarantine in Italy. Int. J. Impot. Res. 2020, 32, 556–557. [Google Scholar] [CrossRef]
- Jacob, L.; Smith, L.; Butler, L.; Barnett, Y.; Grabovac, I.; McDermott, D.; Armstrong, N.; Yakkundi, A.; Tully, M.A. Challenges in the Practice of Sexual Medicine in the Time of COVID-19 in the United Kingdom. J. Sex. Med. 2020, 17, 1229–1236. [Google Scholar] [CrossRef]
- Morgan, P.C.; Durtschi, J.A.; Kimmes, J.G. Sexual and Relationship Satisfaction Associated with Shifts in Dyadic Trajectories of Depressive Symptoms in German Couples across Four Years. J. Marital Fam. Ther. 2018, 44, 655–670. [Google Scholar] [CrossRef] [Green Version]
- Nicolosi, A.; Moreira, E.D.; Villa, M.; Glasser, D.B. A Population Study of the Association between Sexual Function, Sexual Satisfaction and Depressive Symptoms in Men. J. Affect. Disord. 2004, 82, 235–243. [Google Scholar] [CrossRef]
- Worsley, R.; Bell, R.J.; Gartoulla, P.; Davis, S.R. Prevalence and Predictors of Low Sexual Desire, Sexually Related Personal Distress, and Hypoactive Sexual Desire Dysfunction in a Community-Based Sample of Midlife Women. J. Sex. Med. 2017, 14, 675–686. [Google Scholar] [CrossRef] [PubMed]
- Korkeila, K.; Suominen, S.; Ahvenainen, J.; Ojanlatva, A.; Rautava, P.; Helenius, H.; Koskenvuo, M. Non-Response and Related Factors in a Nation-Wide Health Survey. Eur. J. Epidemiol. 2001, 17, 991–999. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Section | Sample Items |
|---|---|
| Compliance with COVID-19 measures | How much have you complied with the contact restrictions so far? Have you been in domestic quarantine in the past, for example, because you had symptoms of COVID-19, or because you had contact with an infected person, or because you had returned from a severely affected country? |
| Couple and family relationships | Has your family situation changed during the contact restrictions? During the COVID-19 contact restrictions, how often did you experience tension in your relationship with your partner? |
| Sexual behaviour | During the COVID-19 contact restrictions, how satisfied were you with your sex life? During the COVID-19 contact restrictions, how often did you consume pornography? |
| Contraception | Are you or your partner currently doing anything to prevent or delay pregnancy, including condom use, contraceptive methods, etc.? Did the contact restrictions make it difficult for you to access contraceptives? |
| Pregnancy and maternal healthcare | If you are currently pregnant, was your pregnancy planned? Did you miss or postpone a prenatal care appointment during the contact restrictions? |
| Abortion | Did you need an abortion (termination of pregnancy) during the contact restrictions? Has the COVID-19 situation prevented you from seeking or having an abortion? |
| Sexual and intimate partner violence | During the COVID-19 contact restrictions, has your partner hit you, pushed you, kicked you, choked you, or thrown something at you that could have hurt you? During the COVID-19 contact restrictions, has your partner physically forced you to have sexual intercourse even though you did not want to? |
| Sociodemographic Characteristic | n (%) |
|---|---|
| Sex (N = 611) | |
| Female | 505 (82.7) |
| Male | 105 (17.2) |
| Other | 1 (0.2) |
| Gender (N = 611) | |
| Female | 486 (79.5) |
| Male | 98 (16.0) |
| Other | 27 (4.4) |
| Sexual orientation (N = 611) | |
| Heterosexual | 360 (59.0) |
| Homo-/bi-/pan-/asexual | 206 (33.8) |
| Other | 44 (7.2) |
| Relationship Status (N = 610) | |
| Single | 246 (40.3) |
| In relationship | 356 (58.3) |
| Other * | 9 (1.5) |
| Children (N = 611) | |
| No | 549 (89.9) |
| Yes (M = 1.82, SD = 1.2) | 62 (10.2) |
| Education (N = 611) | |
| Low or none | 15 (2.5) |
| Secondary | 579 (94.8) |
| Religion (N = 611) | |
| No religion | 397 (65.0) |
| Protestant/Catholic | 198 (32.4) |
| Other | 16 (2.6) |
| Area of living (N = 611) | |
| Urban area | 486 (79.6) |
| Rural area | 122 (20.0) |
| Other | 3 (0.5) |
| Items and Choices | Before COVID-19 (%) | During COVID-19 (%) | ||||
|---|---|---|---|---|---|---|
| How satisfied were you with your sex life? | Female | Male | Diverse | Female | Male | Diverse |
| (n = 481) | (n = 96) | (n = 25) | (n = 482) | (n = 95) | (n = 25) | |
| Not at all satisfied | 65.6 | 28.1 | 6.3 | 70.4 | 25.4 | 4.2 |
| Not very satisfied | 78.8 | 19.4 | 1.8 | 81.5 | 15.2 | 3.4 |
| Somewhat satisfied | 81.4 | 12.2.68 | 5.9 | 79.8 | 13.9 | 6.3 |
| Very satisfied | 81.7 | 15.7 | 2.6 | 84.3 | 14.8 | 0.9 |
| How often have you or your partner experienced sexual problems? | Female | Male | Diverse | Female | Male | Diverse |
| (n = 310) | (n = 56) | (n = 15) | (n = 258) | (n = 52) | (n = 12) | |
| Never | 33.9 | 37.5 | 26.7 | 30.6 | 42.3 | 33.3 |
| Sometimes | 56.8 | 50.0 | 73.3 | 54.7 | 40.4 | 58.3 |
| Often | 9.4 | 12.5 | - | 14.7 | 17.3 | 8.3 |
| Items and Choices | Before COVID-19 (%) | During COVID-19 (%) | ||
|---|---|---|---|---|
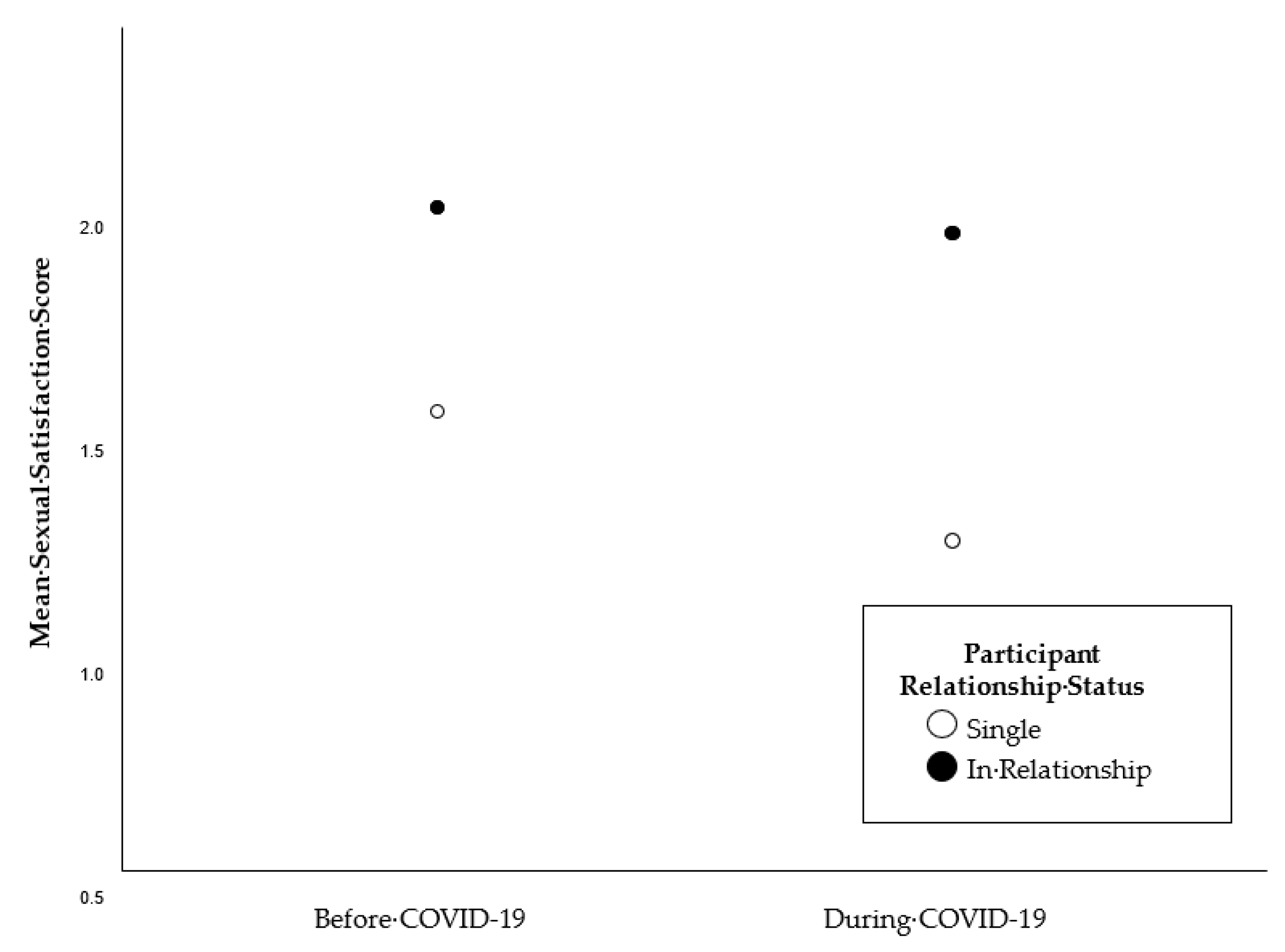
| How satisfied were you with your sex life? | Single | Rel. | Single | Rel. |
| (n = 238) | (n = 355) | (n = 238) | (n = 355) | |
| Not at all satisfied (0) | 81.3 | 18.6 | 80.3 | 19.7 |
| Not very satisfied (1) | 50.9 | 49.1 | 49.1 | 50.9 |
| Somewhat satisfied (2) | 36.6 | 63.4 | 32.2 | 67.8 |
| Very satisfied (3) | 21.4 | 78.6 | 17.1 | 82.9 |
| Mean Score (SD) | 1.53 (0.82) | 1.99 (0.74) | 1.24 (0.91) | 1.93 (0.82) |
| Sexual Behaviours | % | ||
|---|---|---|---|
| Female | Male | Diverse | |
| Sexual activities with steady partner | n = 258 | n = 52 | n = 12 |
| Decreased | 34.9 | 30.8 | 41.7 |
| Stayed the same | 46.5 | 53.8 | 58.3 |
| Increased | 18.6 | 15.4 | - |
| Hugging, kissing, holding hands with partner | n = 257 | n = 52 | n = 12 |
| Decreased | 15.2 | 15.4 | 25.0 |
| Stayed the same | 48.6 | 67.3 | 58.3 |
| Increased | 36.2 | 17.3 | 16.7 |
| Sexual activities with casual partner | n = 476 | n = 95 | n = 25 |
| Decreased | 17.2 | 26.3 | 36.0 |
| Stayed the same | 68.5 | 64.2 | 60.0 |
| Increased | 14.3 | 9.5 | 4.0 |
| Condom use with casual partner | n = 158 | n = 38 | n = 7 |
| Decreased | 4.4 | 2.6 | - |
| Stayed the same | 93.0 | 94.7 | 85.7 |
| Increased | 2.5 | 2.6 | 14.3 |
| Masturbation | n = 481 | n = 95 | n = 24 |
| Decreased | 24.9 | 10.5 | 8.3 |
| Stayed the same | 43.9 | 55.8 | 62.5 |
| Increased | 31.2 | 33.7 | 29.2 |
| Sending/receiving (semi-) naked pictures/videos | n = 476 | n = 95 | n = 24 |
| Decreased | 11.3 | 6.3 | 8.3 |
| Stayed the same | 76.5 | 86.3 | 79.2 |
| Increased | 12.2 | 7.4 | 12.5 |
| Pornography consumption | n = 477 | n = 96 | n = 24 |
| Decreased | 15.7 | 9.4 | 12.5 |
| Stayed the same | 67.3 | 58.3 | 70.8 |
| Increased | 17.0 | 32.3 | 16.7 |
| Online sex | n = 473 | n = 95 | n = 25 |
| Decreased | 2.1 | 2.1 | 4.0 |
| Stayed the same | 94.7 | 93.7 | 92.0 |
| Increased | 3.2 | 4.2 | 4.0 |
| Categories | f (%) | ||
|---|---|---|---|
| Female (n = 266) | Male (n = 43) | Diverse (n = 16) | |
| Psychological stress | 61 (83.6) | 11 (15.1) | |
| Fewer options for social contact | 49 (77.8) | 9 (14.3) | 5 (7.9) |
| More time | 42 (85.7) | 7 (14.3) | - |
| Tension in partnership | 32 (94.1) | 1 (2.9) | 1 (2.9) |
| Separation from (casual) partner(s) | 26 (86.7) | 3 (10.0) | 1 (3.3) |
| Shift to domestic life | 22 (81.5) | 4 (14.8) | 1 (3.7) |
| Caution and fear of infection | 8 (61.5) | 4 (30.8) | 1 (7.7) |
| Increased need for closeness | 10 (83.3) | - | 2 (16.7) |
| Reflecting sexual behaviour and mental health | 7 (70.0) | 1 (10.0) | 2 (20.0) |
| Change in sexual desire | 7 (70.0) | 1 (10.0) | 2 (20.0) |
| Change in motives for sexual activity | 1 (50.0) | 1 (50.0) | - |
| Change in partner’s sexual desire | 1 (50.0) | 1 (50.0) | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Räuchle, J.; Briken, P.; Schröder, J.; Ivanova, O. Sexual and Reproductive Health during the COVID-19 Pandemic: Results from a Cross-Sectional Online Survey in Germany. Int. J. Environ. Res. Public Health 2022, 19, 1428. https://doi.org/10.3390/ijerph19031428
Räuchle J, Briken P, Schröder J, Ivanova O. Sexual and Reproductive Health during the COVID-19 Pandemic: Results from a Cross-Sectional Online Survey in Germany. International Journal of Environmental Research and Public Health. 2022; 19(3):1428. https://doi.org/10.3390/ijerph19031428
Chicago/Turabian StyleRäuchle, Jule, Peer Briken, Johanna Schröder, and Olena Ivanova. 2022. "Sexual and Reproductive Health during the COVID-19 Pandemic: Results from a Cross-Sectional Online Survey in Germany" International Journal of Environmental Research and Public Health 19, no. 3: 1428. https://doi.org/10.3390/ijerph19031428