
Influence of Chewing Ability on Elderly Adults’ Cognitive Functioning: The Mediating Effects of the Ability to Perform Daily Life Activities and Nutritional Status

 ,
, 

Abstract
:1. Introduction
- H1: Chewing ability will affect cognitive functioning;
- H2: The ability to chew will affect the ability to perform everyday activities;
- H3: Chewing ability will affect nutritional status;
- H4: The ability to perform ADLs will affect cognitive functioning;
- H5: Nutritional status will affect cognitive functioning;
- H6: Nutritional status will affect the ability to perform daily activities;
- H7: Chewing ability will indirectly affect cognitive functioning through the ADLs and nutritional status parameters;
- H8: Mastication ability will indirectly influence the ability to perform daily activities through nutritional status parameters;
- H9: Nutritional status will indirectly affect cognitive functioning through the parameters of ADLs;
2. Materials and Methods
2.1. Participants
2.2. Measurement Tools
2.2.1. Chewing Ability
Masticatory Performance Evaluating Gum
2.2.2. Cognitive Abilities
Korean Version of the Mini-Mental Status Examination for Dementia Screening (MMSE-DS)
2.2.3. ADLs
2.2.4. Nutritional Status
2.3. Data Collection Methods
2.4. Institutional Review Board (IRB)
2.5. Statistical Analysis
2.5.1. Descriptive Statistics and Analysis of Variance (ANOVA)
2.5.2. SEM Analysis
3. Results
3.1. Characteristics of the Study Population
3.2. ADLs, Nutritional Status, and Cognitive Functioning per Chewing Abilities and Their Respective Distribution
3.3. SEM Analysis
Validity Test
3.4. Study Hypotheses Testing
3.4.1. Model Fit for the Study Model
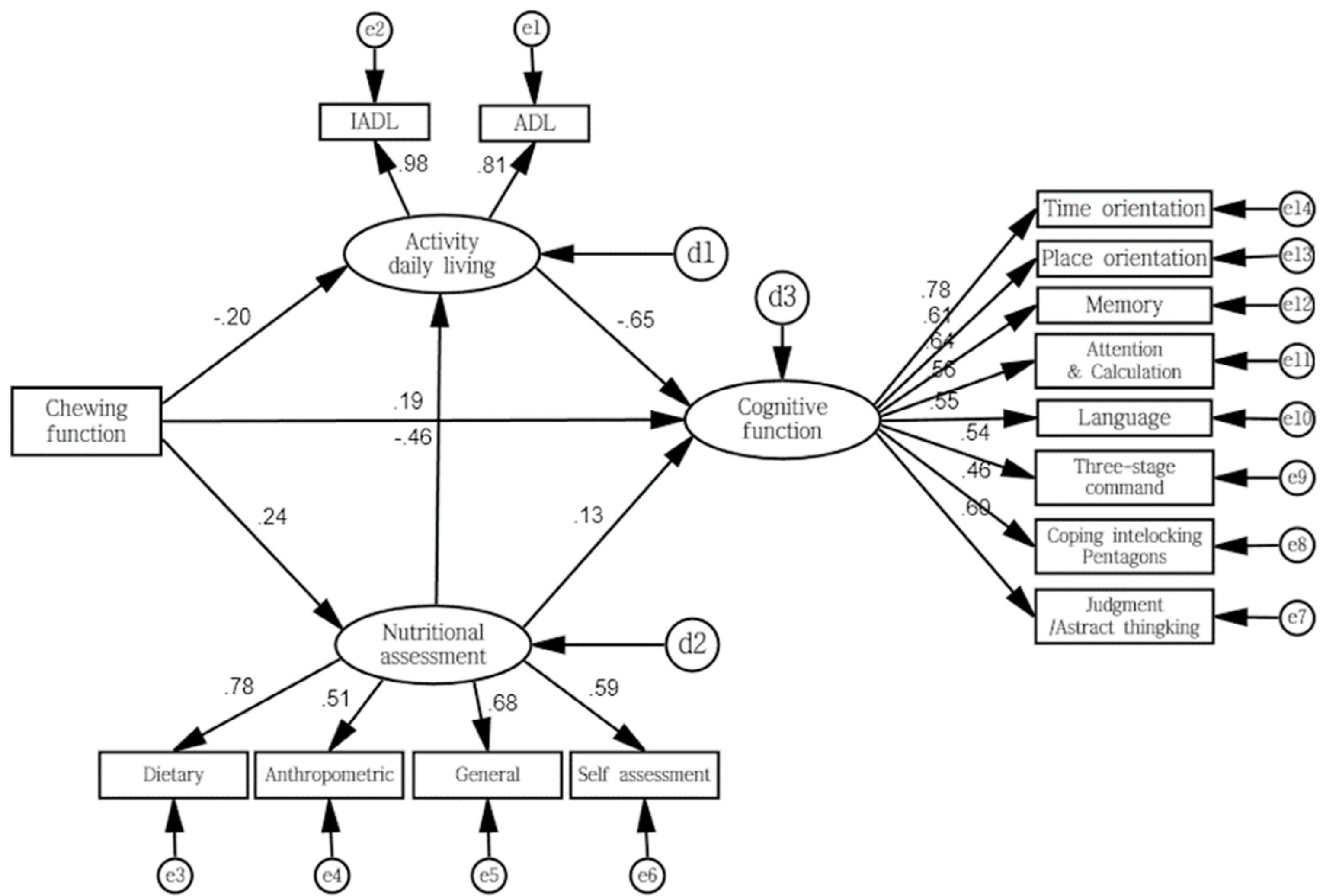
3.4.2. Path Coefficient for Study Model
3.4.3. Direct, Indirect, and Total Effects
4. Discussion
5. Conclusions
- When the participants were divided into groups with high, middle, and low chewing ability, the group with high chewing ability had significantly high ADL and IADL scores and were closer to dependency;
- The MNA and MMSE-DS scores for the groups with low chewing ability were significantly lower;
- The verification of the study model showed the presence of convergent, discriminant, and nomological validity; the model fit was in line with the standards of absolute and incremental indices of fit, which led to the conclusion that the study model and sample data were appropriate;
- When we tested the hypotheses for direct effects, chewing abilities influenced cognitive functioning, ADLs, and nutritional status, and nutritional status directly affected ADLs;
- When we tested the hypotheses for indirect effects, chewing ability indirectly affected cognitive functioning, with ADLs and nutritional status as mediators.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations. World Population Prospects: The 2008 Revision; Department for Economic and Social Affairs: New York, NY, USA, 2009. [Google Scholar]
- Lutz, W.; Sanderson, W.; Scherbov, S. The coming acceleration of global population ageing. Nature 2008, 451, 716–719. [Google Scholar] [CrossRef]
- Statistics Korea. 2015 Statistics on Elderly; Statistics Korea: Daejeon, Korea, 2015.
- Martínez, M.F.; Flores, J.C.; de las Heras, S.P.; Lekumberri, A.M.; Menocal, M.G.; Imirizaldu, J.J. Risk factors for dementia in the epidemiological study of Munguialde County (Basque Country-Spain). BMC Neurol. 2008, 8, 39. [Google Scholar]
- Kalaria, R.N.; Maestre, G.E.; Arizaga, R.; Friedland, R.P.; Galasko, D.; Hall, K.; Luchsinger, J.A.; Ogunniyi, A.; Perry, E.K.; Potocnik, F.; et al. Alzheimer’s disease and vascular dementia in developing countries: Prevalence, management, and risk factors. Lancet Neurol. 2008, 7, 812–826. [Google Scholar] [CrossRef] [Green Version]
- Fillit, H.; Nash, D.T.; Rundek, T.; Zuckerman, A. Cardiovascular risk factors and dementia. Am. J. Geriatr. Pharmacother. 2008, 6, 100–118. [Google Scholar] [CrossRef] [PubMed]
- Tsakos, G.; Watt, R.G.; Rouxel, P.L.; de Oliveira, C.; Demakakos, P. Tooth loss associated with physical and cognitive decline in older adults. J. Am. Geriatr. Soc. 2015, 63, 91–99. [Google Scholar] [CrossRef]
- Ministry of Health and Welfare. 2008 National Health and Nutrition Examination Survey; Ministry of Health and Welfare: Sejong City, Korea, 2008.
- Walls, A.W.; Steele, J.G. The relationship between oral health and nutrition in older people. Mech. Ageing Dev. 2004, 125, 853–857. [Google Scholar] [CrossRef]
- González-Gross, M.; Marcos, A.; Pietrzik, K. Nutrition and cognitive impairment in the elderly. Br. J. Nutr. 2001, 86, 313–321. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pérès, K.; Helmer, C.; Amieva, H.; Orgogozo, J.M.; Rouch, I.; Dartigues, J.F.; Barberger-Gateau, P. Natural history of decline in instrumental activities of daily living performance over the 10 years preceding the clinical diagnosis of dementia: A prospective population-based study. J. Am. Geriatr. Soc. 2008, 56, 37–44. [Google Scholar]
- Weijenberg, R.A.; Scherder, E.J.; Lobbezoo, F. Mastication for the mind-the relationship between mastication and cognition in ageing and dementia. Neurosci. Biobehav. Rev. 2011, 35, 483–497. [Google Scholar] [CrossRef]
- Jo, M.J. The prevalence rate and risk factors of dementia for elderly in Korea. Health Welf. Forum 2009, 1, 43–48. [Google Scholar]
- Kamiyama, M.; Kanazawa, M.; Fujinami, Y.; Minakuchi, S. Validity and reliability of a Self-Implementable method to evaluate masticatory performance: Use of color-changeable chewing gum and a color scale. J. Prosthodont. Res. 2010, 54, 24–28. [Google Scholar] [CrossRef]
- Force USPST. Screening for dementia: Recommendations and rationale. Am. J. Nurs. 2003, 103, 87–89. [Google Scholar]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. “Mini-mental state”: A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Kim, T.H.; Jhoo, J.H.; Park, J.H.; Kim, J.L.; Ryu, S.H.; Moon, S.W.; Choo, I.H.; Lee, D.W.; Yoon, J.C.; Do, Y.J.; et al. Korean version of mini mental status examination for dementia screening and its’ short form. Psychiatr. Investig. 2010, 7, 102–108. [Google Scholar] [CrossRef]
- Kim, K.W. Standardization of Dementia Measuring Tools; Low Birth and Aging Society Strategy Team, Ministry of Health and Welfare Project for Seoul National University Bundang Hospital, Ministry of Health Welfare: Sejong City, Korea, 2012; Volume 47.
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of illness in the aged. The index of ADL: A standardized measure of biological and psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef] [PubMed]
- Won, C.W. Korea activities of daily living scale and Korea instrumental activities of daily living scale. Korean J. Geriatr. Soc. 2002, 6, 1–10. [Google Scholar]
- Lawton, M.P.; Brody, E.M. Assessment of older people: Self-maintaining and instrumental activities of daily living. Gerontologist 1969, 9, 179–186. [Google Scholar] [CrossRef]
- Vellas, B.J.; Guigoz, Y.; Garry, P.; Albarede, J. The Mini Nutritional Assessment (MNA) and its use in grading the nutritional state of elderly patients. Nutr. 1999, 15, 116–122. [Google Scholar] [CrossRef]
- Lee, K.S. Nutritional status at time of hospitalization for elderly surgical patients with stomach cancer using Mini Nutritional Assessment (MNA) and recovery-related factors after surgery. J. Korean Acad. Nurs. 2004, 5, 85–86. [Google Scholar]
- Wheaton, B.; Muthen, B.; Alwain, D.F.; Summers, G.F. Assessing reliability and stability in panel models. Sociol. Methodol. 1977, 8, 84–136. [Google Scholar] [CrossRef]
- Ikebe, K.; Matsuda, K.; Kagawa, R.; Enoki, K.; Yoshida, M.; Maeda, Y.; Nokubi, T. Association of masticatory performance with age, gender, number of teeth, occlusal force and salivary flow in Japanese older adults: Is ageing a risk factor for masticatory dysfunction? Arch. Oral. Biol. 2011, 56, 991–996. [Google Scholar] [CrossRef]
- Lee, H.K. The influence of teeth loss on chewing ability and nutrition intake. J. Korean Dent. Assoc. 1999, 37, 601. [Google Scholar]
- Miura, H.; Yamasaki, K.; Kariyasu, M.; Miura, K.; Sumi, Y. Relationship between cognitive function and mastication in elderly females. J. Oral Rehabil. 2003, 30, 808–811. [Google Scholar] [CrossRef]
- Teixeira, F.B.; Fernandes, L.P.; Noronha, P.T.; dos Santos, M.A.R.; Gomes-Leal, W.; Maia, C.D.S.F.; Lima, R.R. Masticatory deficiency as a risk factor for cognitive dysfunction. Int. J. Med. Sci. 2014, 11, 209–214. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cohen, U.; Weisman, G.D. Holding on to Home: Designing Environments for People with Dementia; Johns Hopkins University Press: Baltimore, MD, USA, 1991. [Google Scholar]
- Swanberg, M.M.; Tractenberg, R.E.; Mohs, R.; Thal, L.J.; Cummings, J.L. Executive dysfunction in Alzheimer disease. Arch. Neurol. 2004, 61, 556–560. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baudic, S.; Dalla Barba, G.; Thibaudet, M.C.; Smagghe, A.; Remy, P.; Traykov, L. Executive function deficits in early Alzheimer’s disease and their relations with episodic memory. Arch. Clin. Neuropsychol. 2006, 26, 15–21. [Google Scholar] [CrossRef] [Green Version]
- Galasko, D.; Klauber, M.R.; Hofstetter, C.R.; Salmon, D.P.; Lasker, B.; Thal, L.J. The Mini-Mental State Examination in the early diagnosis of Alzheimer’s disease. Arch. Neurol. 1990, 47, 49–52. [Google Scholar] [CrossRef]
- Kang, Y.; Na, D.L.; Hahn, S. A validity study on the Korean Mini-Mental State Examination (K-MMSE) in dementia patients. J. Korea Neurol. Assoc. 1997, 15, 300–308. [Google Scholar]
- Royall, D.R.; Lauterbach, E.C.; Kaufer, D.; Malloy, P.; Coburn, K.L.; Black, K.J. The cognitive correlates of functional status: A review from the Committee on Research of the American Neuropsychiatric Association. J. Neuropsychiatry Clin. Neurosci. 2007, 19, 249–265. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.K.; Yoo, Y.W.; Jo, Y.J.; Oh, J.E.; Hong, S.H.; Jo, J.Y. Factors Relating to the Activities of Daily Living of Elderly Patients; Collection of Papers; Soonchunhyang University, Medical School: Asan-si, Korea, 2008; Volume 14, pp. 97–108. [Google Scholar]
- Elsig, F.; Schimmel, M.; Duvernay, E.; Giannelli, S.V.; Graf, C.E.; Carlier, S.; Herrmann, F.R.; Michel, J.P.; Gold, G.; Zekry, D.; et al. Tooth loss, chewing efficiency and cognitive impairment in geriatric patients. Gerodontology 2015, 32, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Onozuka, M.; Hirano, Y.; Tachibana, A.; Kim, W.; Ono, Y.; Sasaguri, K.; Kubo, K.; Niwa, M.; Kanematsu, K.; Watanabe, K. Interactions between chewing and brain activity in humans. In Novel Trends in Brain Science; Springer: Tokyo, Japan, 2008; pp. 99–113. [Google Scholar]
- Wu, B.; Fillenbaum, G.G.; Plassman, B.L.; Gue, L. Association between oral health and cognitive status: A systematic review. J Am. Geriatr. Soc. 2016, 64, 739–751. [Google Scholar] [CrossRef] [Green Version]
- Tada, A.; Miura, H. Association between mastication and cognitive status: A systematic review. Arch. Gerontol. Geriatr. 2017, 70, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Kimura, Y.; Ogawa, H.; Yoshihara, A.; Yamaga, T.; Takiguchi, T.; Wada, T.; Sakamoto, R.; Ishimoto, Y.; Fukutomi, E.; Chen, W.; et al. Evaluation of chewing ability and its relationship with activities of daily living, depression, cognitive status and food intake in the community-dwelling elderly. Geriatr. Gerontol. Int. 2013, 13, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Nordenram, G.; Ryd-Kjellen, E.; Johansson, G.; Nordstrom, G.; Winblad, B. Alzheimer’s disease, oral function and nutritional status. Gerodontology 1996, 13, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Bergdahl, M.; Habib, R.; Bergdahl, J.; Nyberg, L.; Nilsson, L.G. Natural teeth and cognitive function in humans. Scand. J. Psychol. 2007, 48, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Kondo, K.; Nimo, M.; Shido, K. A case-control study of Alzheimer’s disease in Japan–significance of life-styles. Dementia 1994, 5, 314–326. [Google Scholar] [CrossRef]
- Stein, P.S.; Desrosiers, M.; Donegan, S.J.; Yepes, J.F.; Kryscio, R.J. Tooth loss, dementia and neuropathology in the nun study. J. Am. Dent. Assoc. 2007, 138, 1314–1322. [Google Scholar] [CrossRef]
- Budtz-Jorgensen, E.; Chung, J.P.; Rapin, C.H. Nutrition and oral health. Best Pract. Res. Clin. Gastroenterol. 2001, 15, 885–896. [Google Scholar] [CrossRef]
- Won, Y.S.; Jin, K.N. The relationship of oral state and health condition among elderly people. J. Korea Acad. Dent. Hyg. Edu. 2003, 3, 157–168. [Google Scholar]
- Joshipura, K.J.; Willett, W.C.; Douglass, C.W. The impact of edentulousness on food and nutrient intake. J. Am. Dent. Assoc. 1996, 127, 459–467. [Google Scholar] [CrossRef] [PubMed]
- Morris, M.C. Nutritional determinants of cognitive aging and dementia. Proc. Nutr. Soc. 2012, 71, 1–13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perez, L.; Helm, L.; Sherzai, A.D.; Jaceldo-Siegl, K.; Sherzai, A. Nutrition and vascular dementia. J. Nutr. 2012, 16, 319–324. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| n | % | ||
|---|---|---|---|
| Sex | |||
| Male | 95 | 32.2 | |
| Female | 200 | 67.8 | |
| Age (y) (range: 70–102 y, Mean ± SD: 81.35 ± 6.70) | |||
| 70–74 | 54 | 18.3 | |
| 75–79 | 70 | 23.7 | |
| 80–84 | 73 | 24.7 | |
| 85–89 | 53 | 18.0 | |
| ≥90 | 45 | 15.3 | |
| Education | |||
| No formal education | 162 | 54.9 | |
| Primary school | 105 | 35.6 | |
| Middle school | 16 | 5.4 | |
| More than high school | 12 | 4.1 | |
| Cohabitant | |||
| Yes | 183 | 62.0 | |
| No | 112 | 38.0 | |
| Range | Chewing Function | p-Value * | ||||
|---|---|---|---|---|---|---|
| Total | Low (Score 1–2) | Middle (Score 3) | High (Score 4–5) | |||
| Chewing function n (%) | ||||||
| (1–5) | 3.02 ± 0.02 | 100 (33.9) | 86 (29.2) | 109 (36.9) | ||
| Activities of daily living | ||||||
| ADL | (7–16) | 7.45 ± 0.456 | 7.85 ± 0.856 a | 7.43 ± 0.436 a,b | 7.09 ± 0.096 b | 0.001 |
| IADL | (10–33) | 12.33 ± 2.33 | 13.73 ± 3.73 a | 12.69 ± 2.69 a | 10.77 ± 0.77 b | <0.001 |
| Nutritional assessment | ||||||
| MNA | (9.5–30) | 23.60 ± 3.60 | 22.73 ± 2.73 a | 23.01 ± 3.01 a | 24.86 ± 4.86 b | <0.001 |
| Cognitive functioning | ||||||
| MMSE | (5–30) | 23.14 ± 3.14 | 21.11 ± 1.11 a | 22.63 ± 2.63 a | 25.40 ± 5.40 b | <0.001 |
| χ2 | χ2/df | GFI | AGFI | CFI | RMR | RMSEA | TLI | NFI | |
|---|---|---|---|---|---|---|---|---|---|
| Standard | p > 0.05 | <3 | >0.9 | >0.9 | >0.9 | <0.05 | 0.1–0.08 normally 0.08–0.05 fine 0.05 > excellent | >0.9 | >0.9 |
| Study model | 169.040 (p = 0.001) | 2.037 | 0.933 | 0.903 | 0.954 | 0.102 | 0.049 | 0.942 | 0.915 |
| Path | Regression Weight | Standardized Regression Weight | SE | CR | p | |||
|---|---|---|---|---|---|---|---|---|
| H1 | Chewing ability | → | Cognitive functioning | 0.111 | 0.142 | 0.038 | 2.926 | 0.003 |
| H2 | Chewing ability | → | Activities of daily living | −0.218 | −0.256 | 0.049 | −4.490 | <0.001 |
| H3 | Chewing ability | → | Nutritional assessment | 0.156 | 0.173 | 0.053 | 2.925 | 0.003 |
| H4 | Activity daily living | → | Cognitive functioning | −0.645 | −0.698 | 0.061 | −10.590 | <0.001 |
| H5 | Nutritional assessment | → | Cognitive functioning | 0.103 | 0.118 | 0.044 | 2.359 | 0.018 |
| H6 | Nutritional assessment | → | Activities of daily living | −0.258 | −0.272 | 0.056 | −4.625 | <0.001 |
| Path | Direct Effect | p | Indirect Effect | p | Total Effect | p | |||
|---|---|---|---|---|---|---|---|---|---|
| H7 | Chewing ability | → | Cognitive functioning | 0.142 | 0.004 | 0.232 | 0.004 | 0.374 | 0.004 |
| H8 | Chewing ability | → | Activities of daily living | −0.256 | 0.004 | −0.047 | 0.007 | −0.303 | 0.004 |
| Chewing ability | → | Nutritional assessment | 0.173 | 0.006 | - | - | 0.173 | 0.006 | |
| Activity daily living | → | Cognitive functioning | −0.698 | 0.004 | - | - | −0.698 | 0.004 | |
| H9 | Nutritional assessment | → | Cognitive functioning | 0.118 | 0.085 | 0.190 | 0.004 | 0.308 | 0.004 |
| Nutritional assessment | → | Activities of daily living | −0.272 | 0.004 | - | - | −272 | 0.004 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jung, Y.-S.; Park, T.; Kim, E.-K.; Jeong, S.-H.; Lee, Y.-E.; Cho, M.-J.; Song, K.-B.; Choi, Y.-H. Influence of Chewing Ability on Elderly Adults’ Cognitive Functioning: The Mediating Effects of the Ability to Perform Daily Life Activities and Nutritional Status. Int. J. Environ. Res. Public Health 2022, 19, 1236. https://doi.org/10.3390/ijerph19031236
Jung Y-S, Park T, Kim E-K, Jeong S-H, Lee Y-E, Cho M-J, Song K-B, Choi Y-H. Influence of Chewing Ability on Elderly Adults’ Cognitive Functioning: The Mediating Effects of the Ability to Perform Daily Life Activities and Nutritional Status. International Journal of Environmental Research and Public Health. 2022; 19(3):1236. https://doi.org/10.3390/ijerph19031236
Chicago/Turabian StyleJung, Yun-Sook, Taejun Park, Eun-Kyong Kim, Seong-Hwa Jeong, Young-Eun Lee, Min-Jeong Cho, Keun-Bae Song, and Youn-Hee Choi. 2022. "Influence of Chewing Ability on Elderly Adults’ Cognitive Functioning: The Mediating Effects of the Ability to Perform Daily Life Activities and Nutritional Status" International Journal of Environmental Research and Public Health 19, no. 3: 1236. https://doi.org/10.3390/ijerph19031236