
Olfactory Dysfunction in COVID-19 Patients Who Do Not Report Olfactory Symptoms: A Pilot Study with Some Suggestions for Dentists


 , ,
, ,
Abstract
:1. Introduction
2. Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Triggle, C.R.; Bansal, D.; Ding, H.; Islam, M.M.; Farag EA, B.A.; Hadi, H.A.; Sultan, A.A. A Comprehensive Review of Viral Characteristics, Transmission, Pathophysiology, Immune Response, and Management of SARS-CoV-2 and COVID-19 as a Basis for Controlling the Pandemic. Front. Immunol. 2021, 12, 338. [Google Scholar] [CrossRef] [PubMed]
- Peng, X.; Xu, X.; Li, Y.; Zheng, L.; Zhou, X.; Reb, B. Trasmission routes of 2019-nCoV and controls in dental practice. Int. J. Oral Sci. 2020, 12, 1–6. [Google Scholar] [CrossRef]
- Yesudhas, D.; Srivastava, A.; Gromiha, M.M. COVID-19 outbreak: History, mechanism, transmission, structural studies and therapeutics. Clin. Microbiol. Infect. 2020, 49, 199–213. [Google Scholar] [CrossRef] [PubMed]
- Cucinotta, D.; Vanelli, M. WHO declares COVID-19 a pandemic. Acta Biomed. 2020, 91, 157–160. [Google Scholar] [CrossRef]
- Berardi C, A.M. The COVID-19 pandemic in Italy: Policy and technology impact on health and non-health outcomes. Health Policy Technol. 2020, 9, 454–487. [Google Scholar] [CrossRef]
- Gostic, K.; Gomez, A.C.; Mummah, R.O.; Kucharski, A.J.; Lloyd-Smith, J.O. Estimated effectiveness of symptom and risk screening to prevent the spread of COVID-19. eLife 2020, 9, e55570. [Google Scholar] [CrossRef]
- Mansourian, M.; Ghandi, Y.; Habibi, D.; Mehrabi, S. COVID-19 infection in children: A systematic review and meta-analysis of clinical features and laboratory findings. Arch. Pediatr. 2021, 28, 242–248. [Google Scholar] [CrossRef] [PubMed]
- Guerrero, J.I.; Barragán, L.A.; Martínez, J.D.; Montoya, J.P.; Peña, A.; Sobrino, F.E.; Tovar-Spinoza, Z.; Ghotme, K.A. Central and peripheral nervous system involvement by COVID-19: A systematic review of the pathophysiology, clinical manifestations, neuropathology, neuroimaging, electrophysiology, and cerebrospinal fluid findings. BMC Infect. Dis. 2021, 21, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Fotuhi, M.; Mian, A.; Rajji, C.A. Neurobiology of COVID-19. J. Alzheeimer’s Dis. 2020, 76, 3–19. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A.; Dequanter, D.; Blecic, S.; El Afia, F.; Distinguin, L.; et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef] [PubMed]
- Agyeman, A.A.; Chin, K.L.; Landersdorfer, C.B.; Liew, D.; Ofori-Asenso, R. Smell and Taste Dysfunction in Patients With COVID-19: A Systematic Review and Meta-analysis. Mayo Clin. Proc. 2020, 95, 1621–1631. [Google Scholar] [CrossRef]
- Ibekwe, T.S.; Fasunla, A.J.; Orimadegun, A. Systematic Review and Meta-analysis of Smell and Taste Disorders in COVID-19. OTO Open 2020, 4, 2473974X20957975. [Google Scholar] [CrossRef] [PubMed]
- Farronato, M.B.E. Scoping Review of Respirator Literature and a Survey among Dental Professionals. Int. J. Environ. Res. Public Health 2020, 17, 5968. [Google Scholar] [CrossRef]
- Hannum, M.E.; Ramirez, V.A.; Lipson, S.J.; Herriman, R.D.; Toskala, A.K.; Lin, C.; Joseph, P.V.; Reed, D.R. Objective Sensory Testing Methods Reveal a Higher Prevalence of Olfactory Loss in COVID-19-Positive Patients Compared to Subjective Methods: A Systematic Review and Meta-Analysis. Chem. Senses 2020, 45, 865–874. [Google Scholar] [CrossRef]
- Bordin, A.; Mucignat-Caretta, C.; Gaudioso, P.; Pendolino, A.; Leoni, D.; Scarpa, B.; Andrews, P.J.; Cattelan, A.M.; Antonini, A.; Nicolai, P.; et al. Comparison of self-reported symptoms and psychophysical tests in coronavirus disease 2019 (COVID-19) subjects experiencing long-term olfactory dysfunction: A 6-month follow-up study. Int. Forum Allergy Rhinol. 2021. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Meini, S.; Suardi, R.; Busoni, M.; Roberts, A.; Fortini, A. Olfactory and gustatory dysfunctions in 100 patients hospitalized for COVID 19: Sex diferences and recovery time in real life. Eur. Arch. Oto-Rhino-Laryngol. 2020, 277, 3519–3523. [Google Scholar] [CrossRef] [PubMed]
- Vaira, L.A.; Deiana, G.; Fois, A.G.; Pirina, P.; Madeddu, G.; De Vito, A.; Babudieri, S.; Petrocelli, M.; Serra, A.; Bussu, F.; et al. Objective evaluation of anosmia and ageusia in COVID-19 patients: Single-center experience on 72 cases. Head Neck 2020, 42, 1252–1258. [Google Scholar] [CrossRef]
- Rumeau, C.; Nguyen, D.; Jankowski, R. How to assess olfactory performance with the Sniffin’ Sticks test. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2016, 133, 203–206. [Google Scholar] [CrossRef]
- Oleszkiewicz, A.; Schriever, V.A.; Croy, I.; Hähner, A.; Hummel, T. Updated Sniffin’ Sticks normative data based on an extended sample of 9139 subjects. Eur. Arch. Oto-Rhino-Laryngol. 2019, 276, 719–728. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rocke, J.; Hopkins, C.; Philpott, C.M.; Kumar, N. Is loss of sense of smell a diagnostic marker in COVID-19: A systematic review and meta-analysis. Clin. Otolaryngol. 2020, 45, 914–922. [Google Scholar] [CrossRef]
- Lozada-Nur, F.; Chainani-Wu, N.; Fortuna, G.; Sroussi, H. Dysgeusia in COVID-19: Possible Mechanisms and Implications. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 130, 344–346. [Google Scholar] [CrossRef] [PubMed]
- Pendolino, A.L.; Ottaviano, G.; Scarpa, B.; Cattelan, A.; Andrews, J.A.; Andrews, P.J. Characteristics of taste dysfunction in COVID-19 subjects coming from two different countries. J. Neurovirol. 2021, 27, 482–485. [Google Scholar] [CrossRef] [PubMed]
- Kaye, R.; Chang, C.W.D.; Kazahaya, K.; Brereton, J.; Denneny, I.J.C. COVID-19 Anosmia Reporting Tool: Initial Findings. Otolaryngol.—Head Neck Surg. 2020, 163, 132–134. [Google Scholar] [CrossRef] [PubMed]
- Pang, K.W.; Chee, J.; Subramaniam, S.; Ng, C.L. Frequency and Clinical Utility of Olfactory Dysfunction in COVID-19: A Systematic Review and Meta-analysis. Curr. Allergy Asthma Rep. 2020, 20, 1–17. [Google Scholar] [CrossRef]
- Marchese-Ragona, R.; Restivo, D.A.; De Corso, E.; Vianello, A.; Nicolai, P.; Ottaviano, G. Loss of smell in COVID-19 patients: A critical review with emphasis on the use of olfactory tests. Acta Otorhinolaryngol. Ital. 2020, 40, 241–247. [Google Scholar] [CrossRef]
- Moein, S.; Hashemian, S.; Mansourafshar, B.; Khorram-Tousi, A.; Tabarsi, P.; Doty, R. Smell dysfunction: A biomarker for COVID-19. Int. Forum Allergy Rhinol. 2020, 10, 944–950. [Google Scholar] [CrossRef] [PubMed]
- Beltrán-Corbellini, Á.; Chico-García, J.L.; Martínez-Poles, J.; Rodríguez-Jorge, F.; Natera-Villalba, E.; Gómez-Corral, J.; Gómez-López, A.; Monreal, E.; Parra-Díaz, P.; Cortés-Cuevas, J.L.; et al. Acute-onset smell and taste disorders in the context of COVID-19: A pilot multicentre polymerase chain reaction based case–control study. Eur. J. Neurol. 2020, 27, 1738–1741. [Google Scholar] [CrossRef]
- Vaira, L.A.; Hopkins, C.; Salzano, G.; Petrocelli, M.; Melis, A.; Cucurullo, M.; Ferrari, M.; Gagliardini, L.; Pipolo, C.; Deiana, G.; et al. Olfactory and gustatory function impairment in COVID-19 patients: Italian objective multicenter-study. Head Neck 2020, 42, 1560–1569. [Google Scholar] [CrossRef] [PubMed]
- Ottaviano, G.; Carecchio, M.; Scarpa, B.; Marchese-Ragona, R. Olfactory and rhinological evaluations in SARS-CoV-2 patients complaining of olfactory loss. Rhinology 2020, 58, 400–401. [Google Scholar] [CrossRef]
- Yan, C.H.; Faraji, F.; Prajapati, D.; Boone, C.E.; DeConde, A.S. Association of chemosensory dysfunction and COVID-19 in patients presenting with influenza-like symptoms. Int. Forum Allergy Rhinol. 2020, 10, 806–813. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Otte, M.S.; Eckel, H.N.C.; Poluschkin, L.; Klussmann, J.P.; Luers, J.C. Olfactory dysfunction in patients after recovering from COVID-19. Acta Otolaryngol. 2020, 140, 1032–1035. [Google Scholar] [CrossRef]
- Iannuzzi, L.; Salzo, A.E.; Angarano, G.; Palmieri, V.O.; Portincasa, P.; Saracino, A.; Gelardi, M.; Dibattista, M.; Quaranta, N. Gaining Back What Is Lost: Recovering the Sense of Smell in Mild to Moderate Patients After COVID-19. Chem. Senses 2020, 45, 875–881. [Google Scholar] [CrossRef]
- Landis, B.N.; Hummel, T. New Evidence for High Occurrence of Olfactory Dysfunctions within the Population. Am. J. Med. 2006, 119, 91–92. [Google Scholar] [CrossRef]
- Mutiawati, E.; Fahriani, M.; Mamada, S.; Fajar, J.; Frediansyah, A.; Anggun Maliga, H.; Ilmawan, M.; Emran, T.B.; Ophinni, Y.; Ichsan, I.; et al. Anosmia and dysgeusia in SARS-CoV-2 infection: Incidence and effects on COVID-19 severity and mortality, and the possible pathobiology mechanisms—A systematic review and meta-analysis. F1000Research 2021, 10, 40. [Google Scholar] [CrossRef] [PubMed]
- Las Casas Lima, M.H.; Cavalcante, A.L.B.; Leão, S.C. Pathophysiological relationship between COVID-19 and olfactory dysfunction: A systematic review. Braz. J. Otorhinolaryngol. 2021, 25, S1808-8694(21)00073-2. [Google Scholar] [CrossRef]
- Mahmoud, M.M.; Abuohashish, H.M.; A Khairy, D.; Bugshan, A.S.; Khan, A.M.; Moothedath, M.M. Pathogenesis of dysgeusia in COVID-19 patients: A scoping review. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 1114–1134. [Google Scholar] [PubMed]
- Luchiari, H.R.; Giordano, R.J.; Sidman, R.L.; Pasqualini, R.; Arap, W. Does the RAAS play a role in loss of taste and smell during COVID-19 infections? Pharmacogenomics J. 2021, 21, 109–115. [Google Scholar] [CrossRef] [PubMed]
- Bilinska, K.; Butowt, R. Anosmia in COVID-19: A Bumpy Road to Establishing a Cellular Mechanism. ACS Chem. Neurosci. 2020, 11, 2152–2155. [Google Scholar] [CrossRef] [PubMed]
- Soler, Z.M.; Patel, Z.M.; Turner, J.H.; Holbrook, E.H. A primer on viral-associated olfactory loss in the era of COVID-19. Int. Forum Allergy Rhinol. 2020, 10, 814–820. [Google Scholar] [CrossRef]
- Ottaviano, G.; Zuccarello, D.; Frasson, G.; Scarpa, B.; Nardello, E.; Foresta, C.; Marioni, G.; Staffieri, A. Olfactory Sensitivity and Sexual Desire in Young Adult and Elderly Men: An Introductory Investigation. Am. J. Rhinol. Allergy 2013, 27, 157–161. [Google Scholar] [CrossRef]
- Abdelalim, A.; Mohamady, A.; Elsayed, R.; Elawady, M.; Ghallab, A. Corticosteroid nasal spray for recovery of smell sensation in COVID-19 patients: A randomized controlled trial. Am. J. Otolaryngol. 2021, 42, 102884. [Google Scholar] [CrossRef]
- Vandersteen, C.; Payne, M.; Dumas, L.É.; Plonka, A.; D’Andréa, G.; Chirio, D.; Demonchy, É.; Risso, K.; Robert, P.; Fernandez, X.; et al. What about using sniffin’ sticks 12 items test to screen post-COVID-19 olfactory disorders? Eur. Arch. Oto-Rhino-Laryngol. 2021, 1–8, (Epub ahead of print). [Google Scholar] [CrossRef]
- Remington, W.D.; Ott, B.C.; Hartka, T.R. Effectiveness of barrier devices, high-volume evacuators, and extraoral suction devices on reducing dental aerosols for the dental operator: A pilot study. J. Am. Dent. Assoc. 2021, S0002-8177(21)00546-8. [Google Scholar] [CrossRef]
- Shirazi, S.; Stanford, C.; Cooper, L. Testing for COVID-19 in dental offices: Mechanism of action, application, and interpretation of laboratory and point-of-care screening tests. J. Am. Dent. Assoc. 2021, 152, 514–525. [Google Scholar] [CrossRef] [PubMed]
- Winkel, B.; Schram, E.; Gremmels, H.; Debast, S.; Schuurman, R.; Wensing, A.; Bonten, M.; Goedhart, E.; Hofstra, M. Antigen Rapid Test Validation Group. Screening for SARS-CoV-2 infection in asymptomatic individuals using the Panbio COVID-19 antigen rapid test (Abbott) compared with RT-PCR: A prospective cohort study. BMJ Open 2021, 11, e048206. [Google Scholar] [CrossRef]
- Bidra, A.S.; Pelletier, J.S.; Westover, J.B.; Frank, S.; Brown, S.M.; Tessema, B. Rapid In-Vitro Inactivation of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) Using Povidone-Iodine Oral Antiseptic Rinse. J. Prosthodont. 2020, 29, 529–533. [Google Scholar] [CrossRef] [PubMed]
- Arefin, M.K. Povidone Iodine (PVP-I) Oro-Nasal Spray: An Effective Shield for COVID-19 Protection for Health Care Worker (HCW), for all. Indian J. Otolaryngol. Head Neck Surg. 2021, 1–6, (Epub ahead of print). [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indicator | All Patients | ||
|---|---|---|---|
| n | Prob | p-Value Prob ≥ 0.9 | |
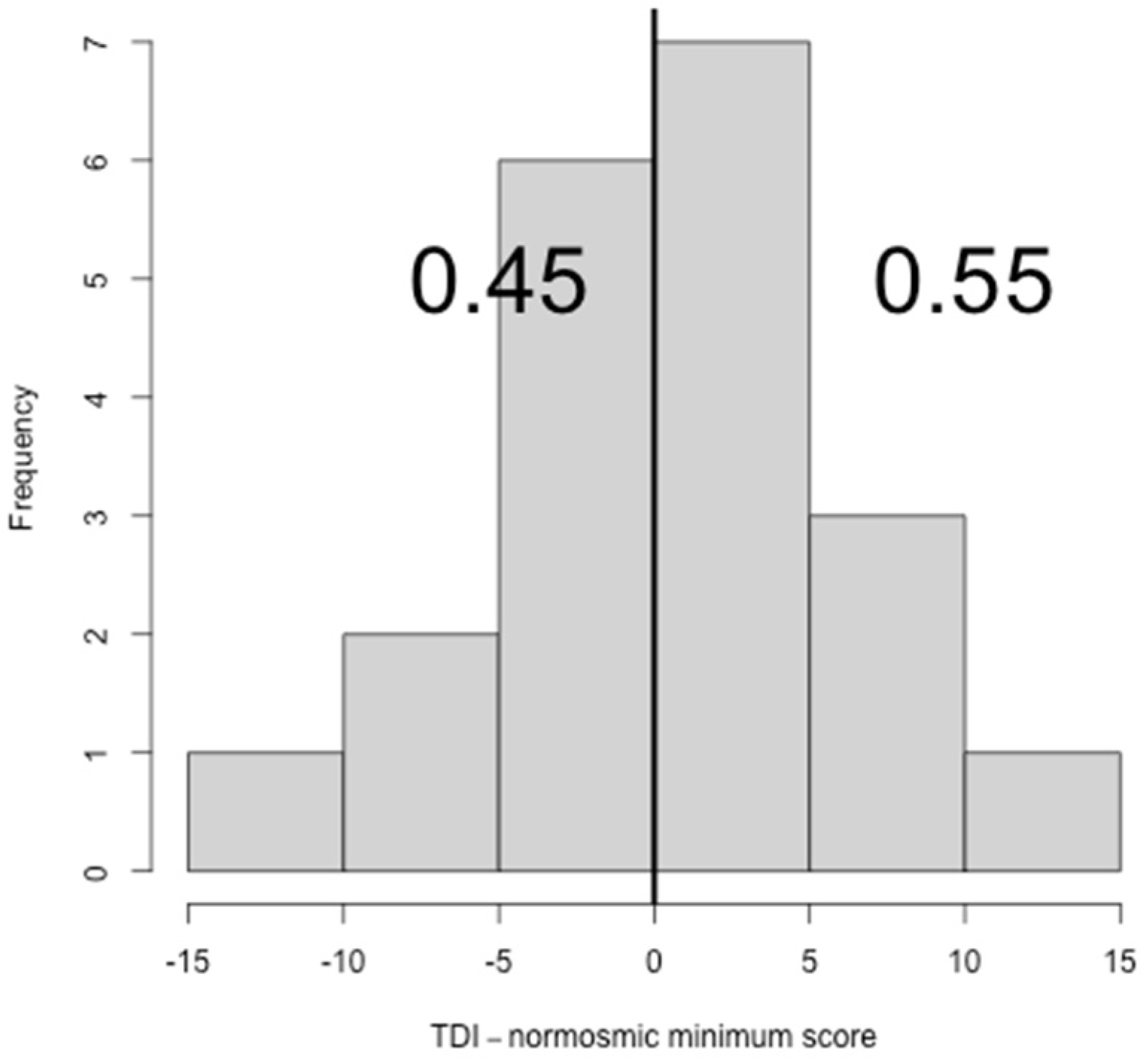
| TDI > cutoff | 11 | 0.55 | <0.001 |
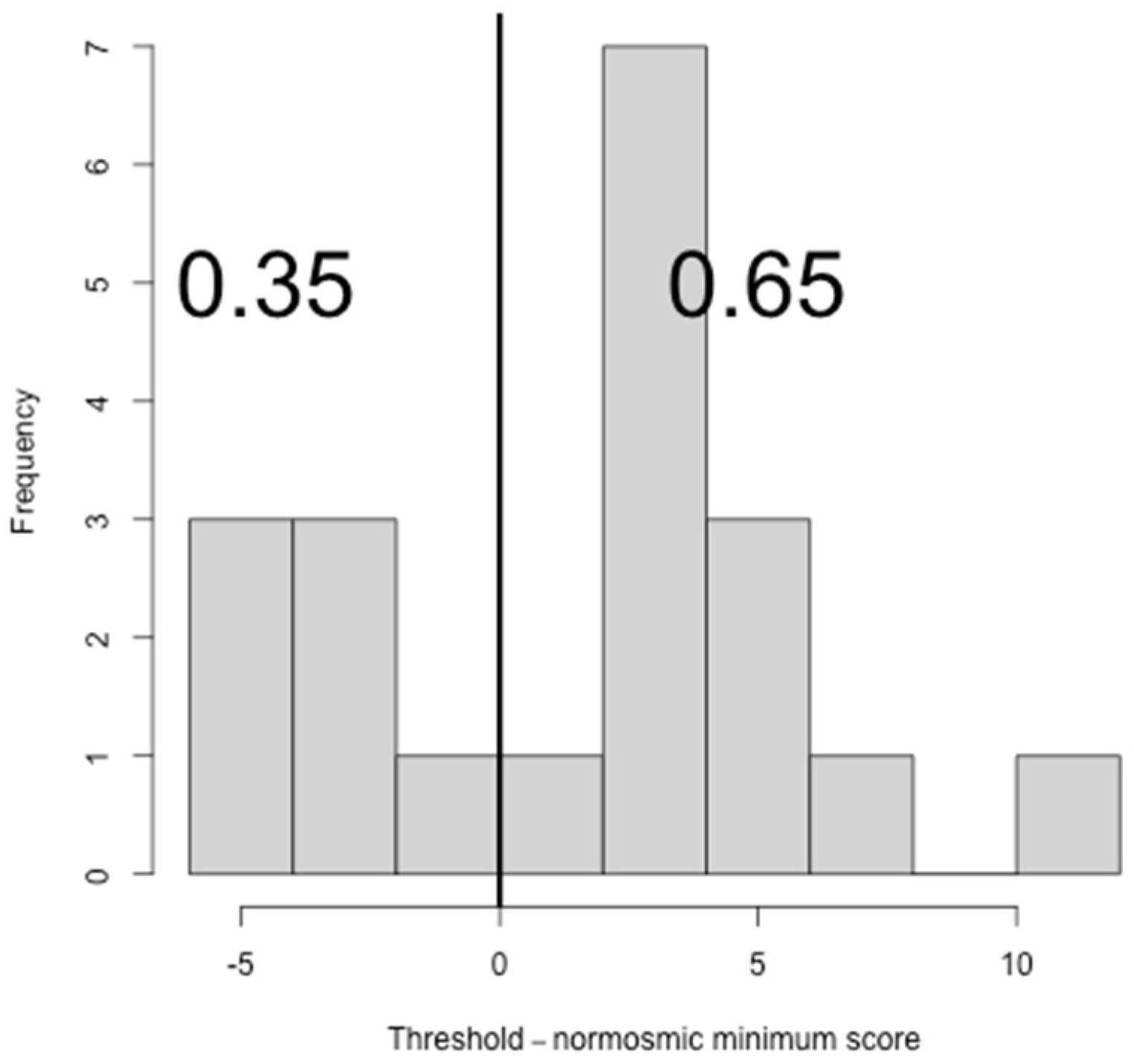
| Threshold | 13 | 0.65 | 0.002 |
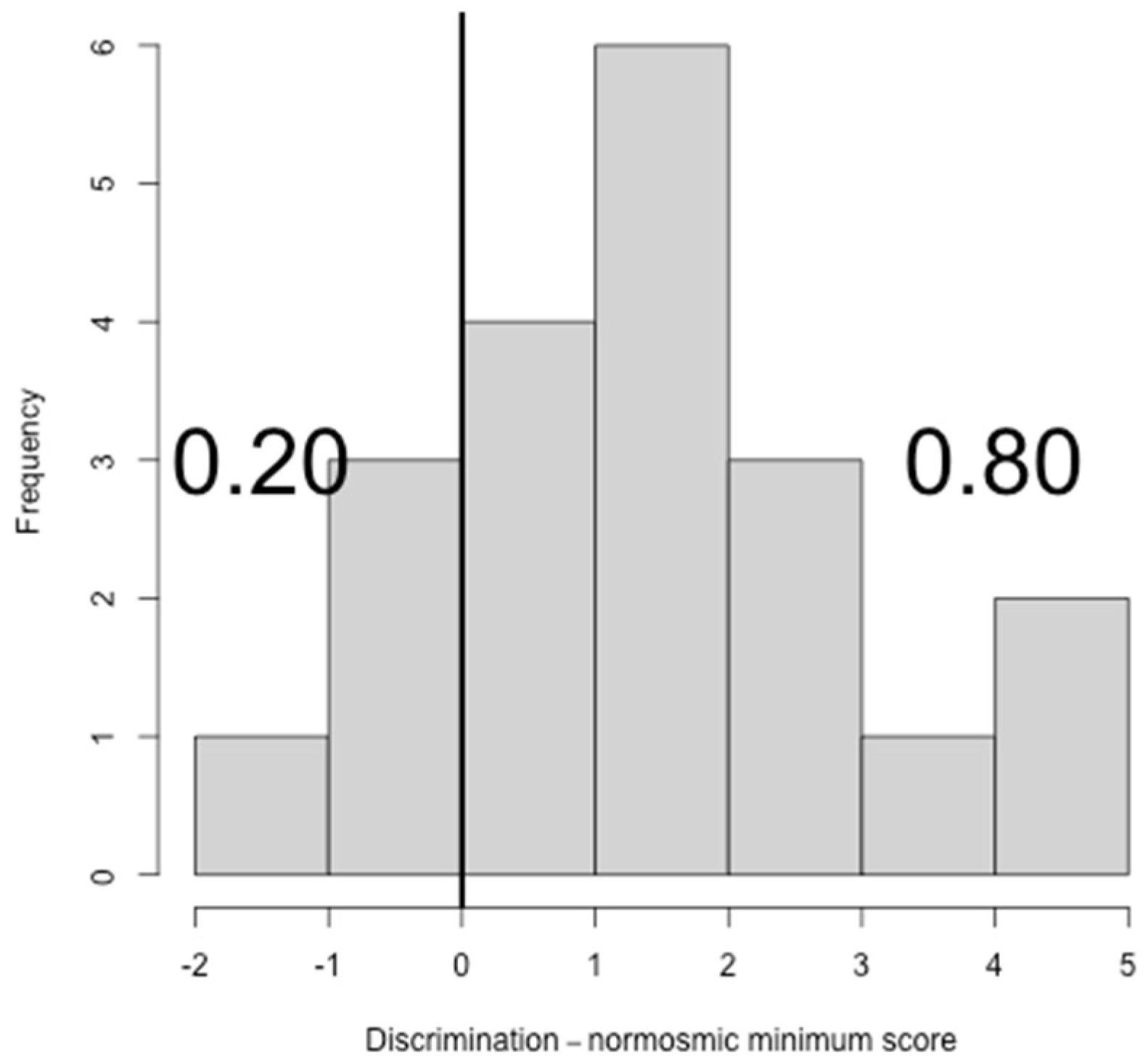
| Discrimination | 16 | 0.8 | 0.133 |
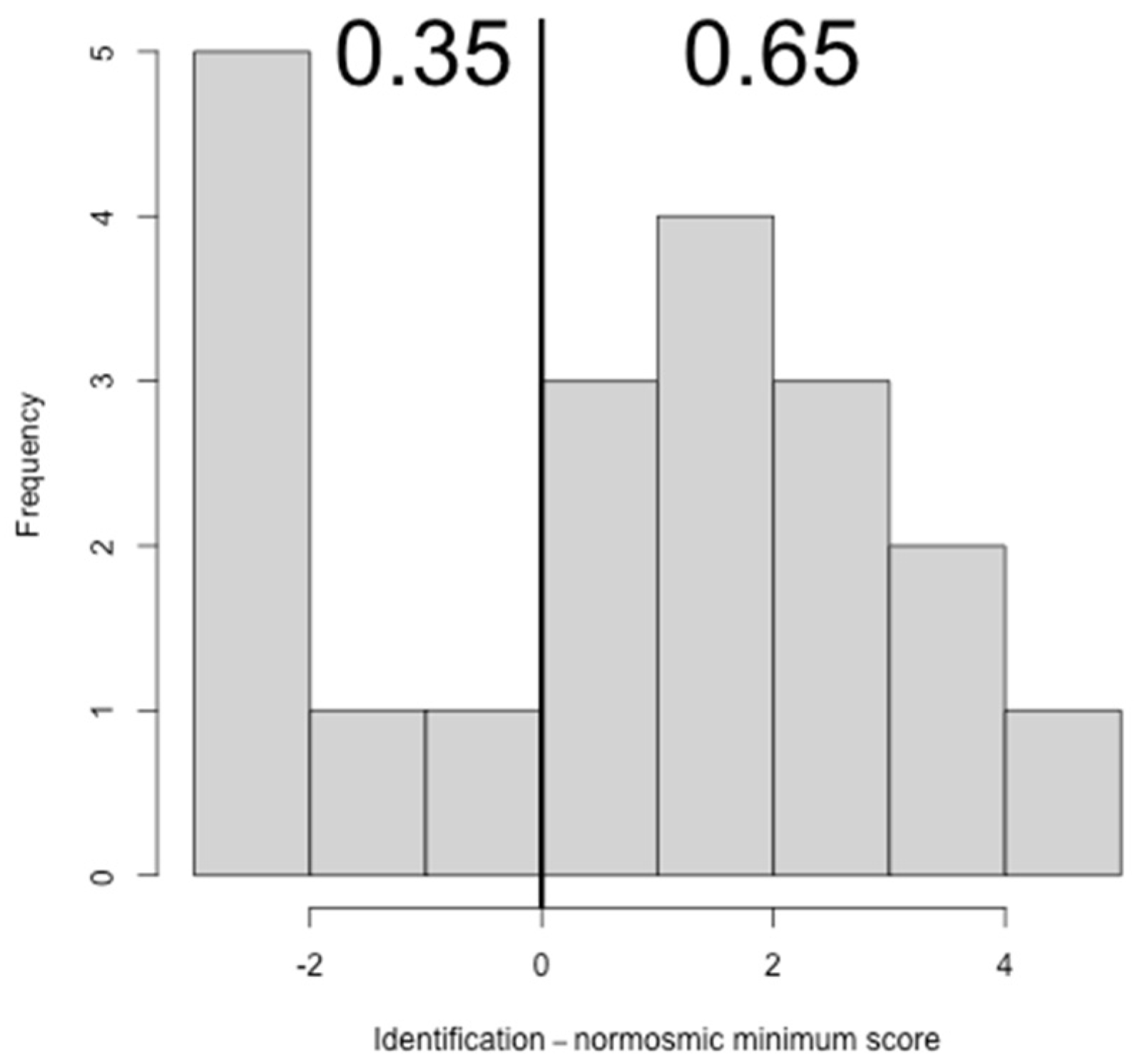
| Identification | 13 | 0.65 | 0.002 |
| Total | 20 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Favero, R.; Hajrulla, S.; Bordin, A.; Mucignat-Caretta, C.; Gaudioso, P.; Scarpa, B.; Favero, L.; Ottaviano, G. Olfactory Dysfunction in COVID-19 Patients Who Do Not Report Olfactory Symptoms: A Pilot Study with Some Suggestions for Dentists. Int. J. Environ. Res. Public Health 2022, 19, 1036. https://doi.org/10.3390/ijerph19031036
Favero R, Hajrulla S, Bordin A, Mucignat-Caretta C, Gaudioso P, Scarpa B, Favero L, Ottaviano G. Olfactory Dysfunction in COVID-19 Patients Who Do Not Report Olfactory Symptoms: A Pilot Study with Some Suggestions for Dentists. International Journal of Environmental Research and Public Health. 2022; 19(3):1036. https://doi.org/10.3390/ijerph19031036
Chicago/Turabian StyleFavero, Riccardo, Silva Hajrulla, Anna Bordin, Carla Mucignat-Caretta, Piergiorgio Gaudioso, Bruno Scarpa, Lorenzo Favero, and Giancarlo Ottaviano. 2022. "Olfactory Dysfunction in COVID-19 Patients Who Do Not Report Olfactory Symptoms: A Pilot Study with Some Suggestions for Dentists" International Journal of Environmental Research and Public Health 19, no. 3: 1036. https://doi.org/10.3390/ijerph19031036