
Effects of Blood Flow Restriction Combined with Low-Intensity Resistance Training on Lower-Limb Muscle Strength and Mass in Post-Middle-Aged Adults: A Systematic Review and Meta-Analysis
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Statistical Analysis
3. Results
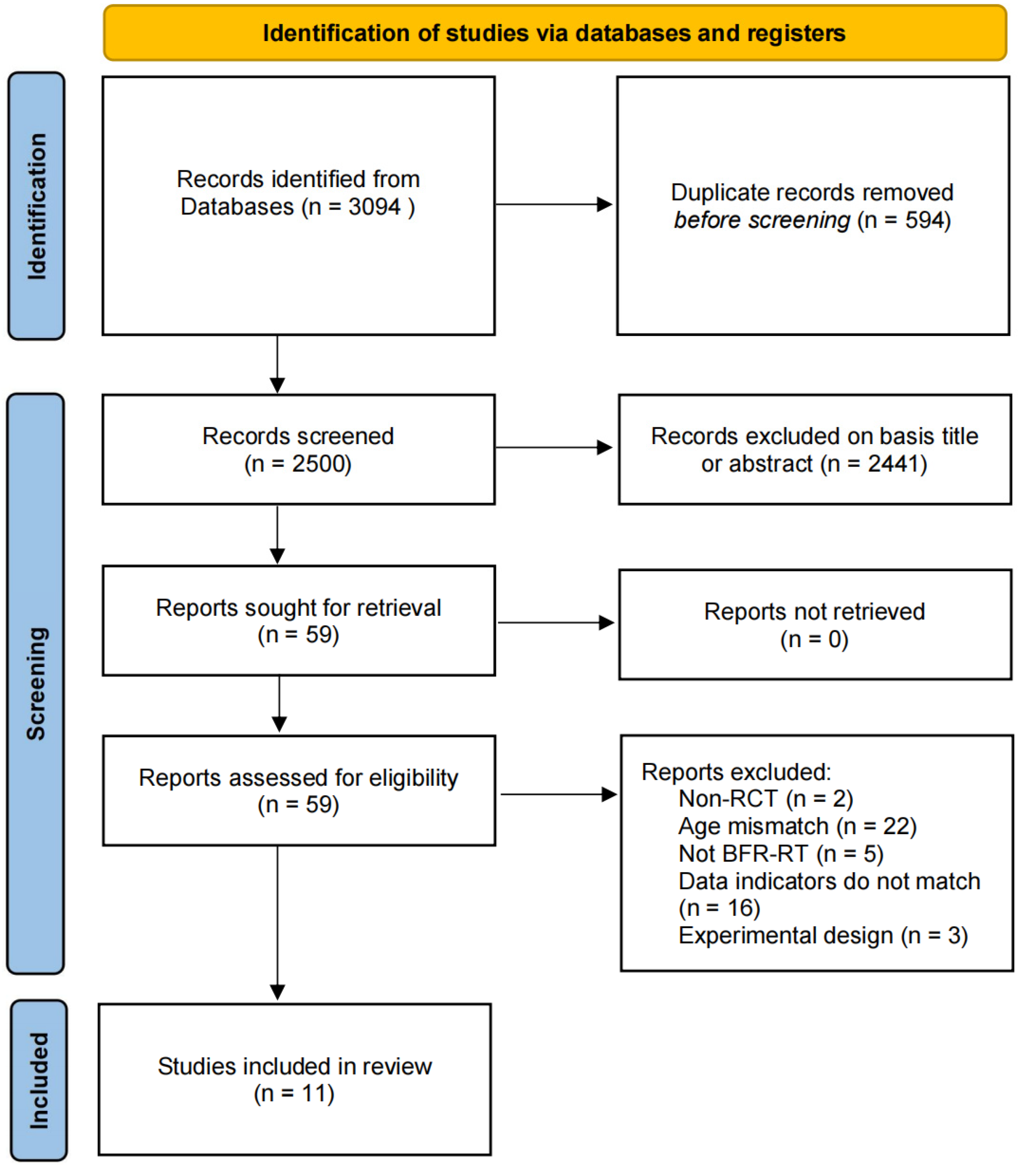
3.1. Search Results
3.2. Characteristics of the Studies
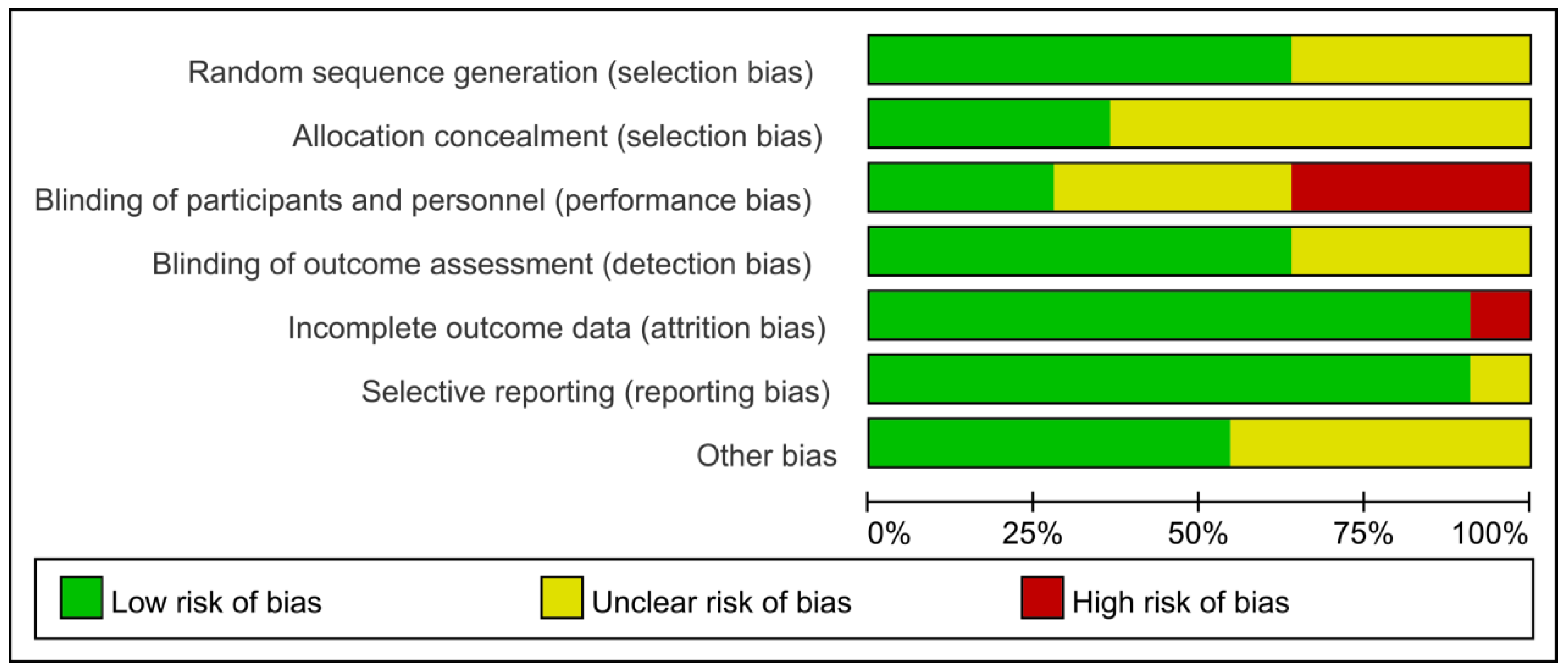
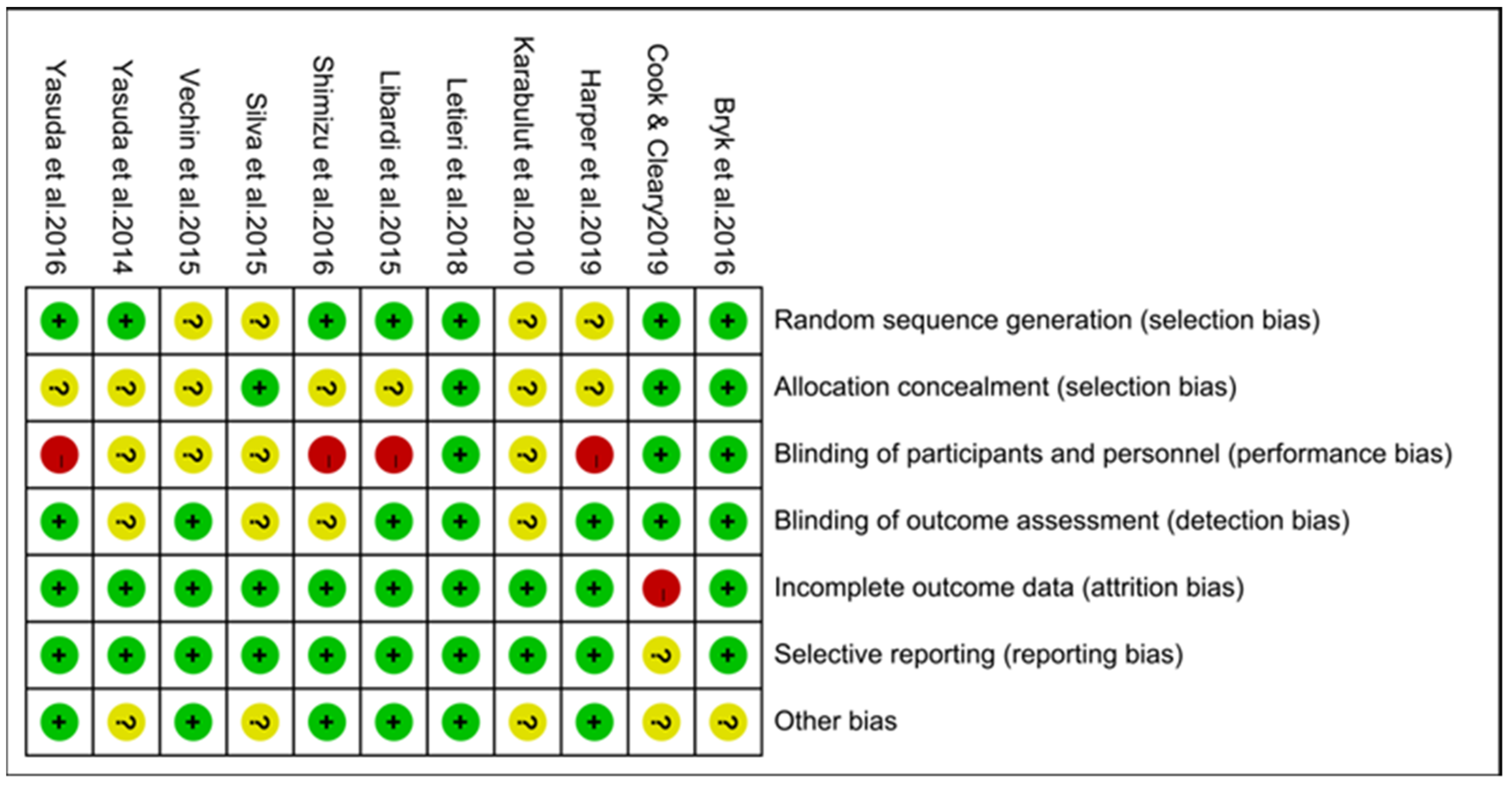
3.3. Methodological Quality Assessment of the Included Studies
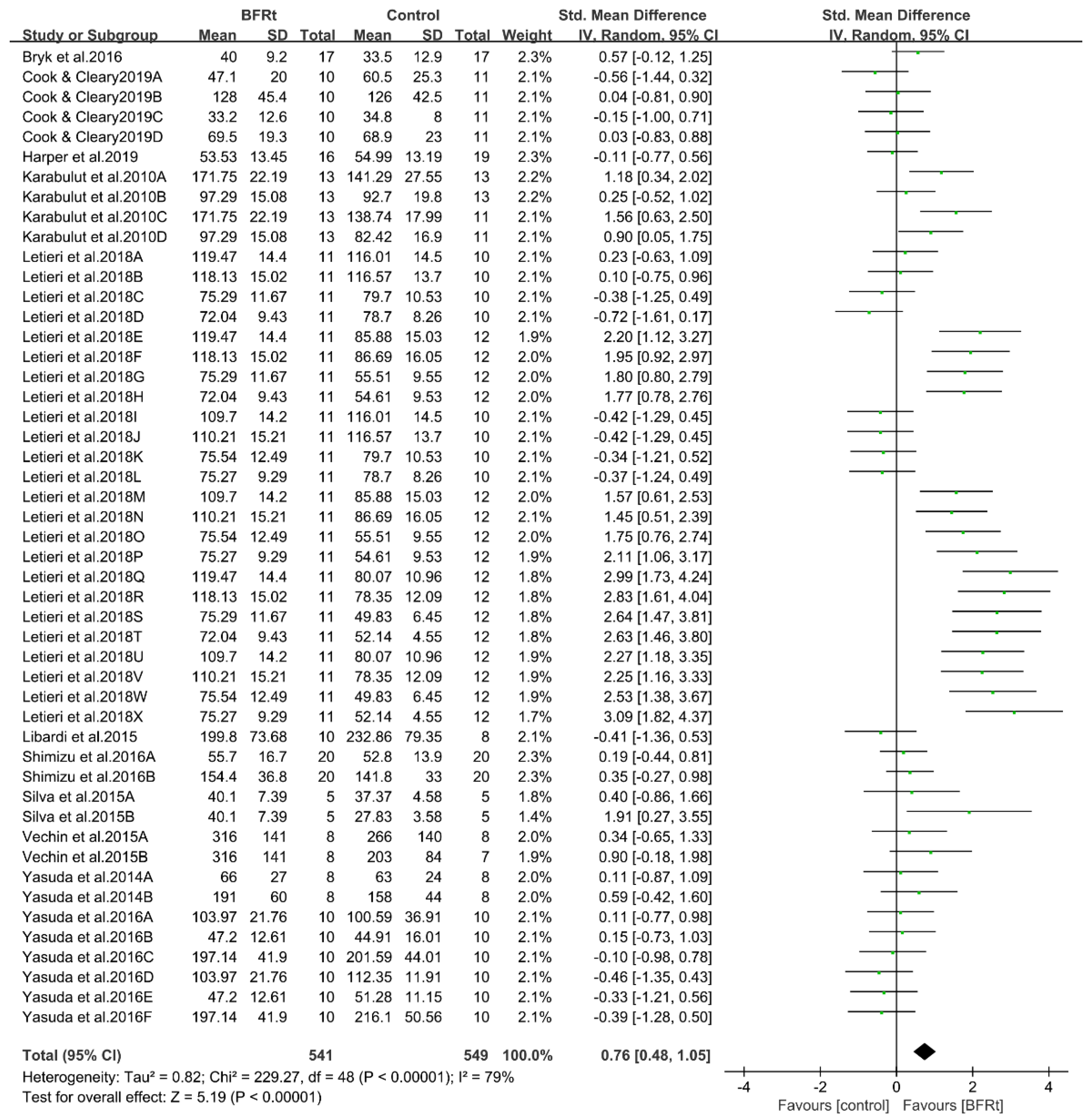
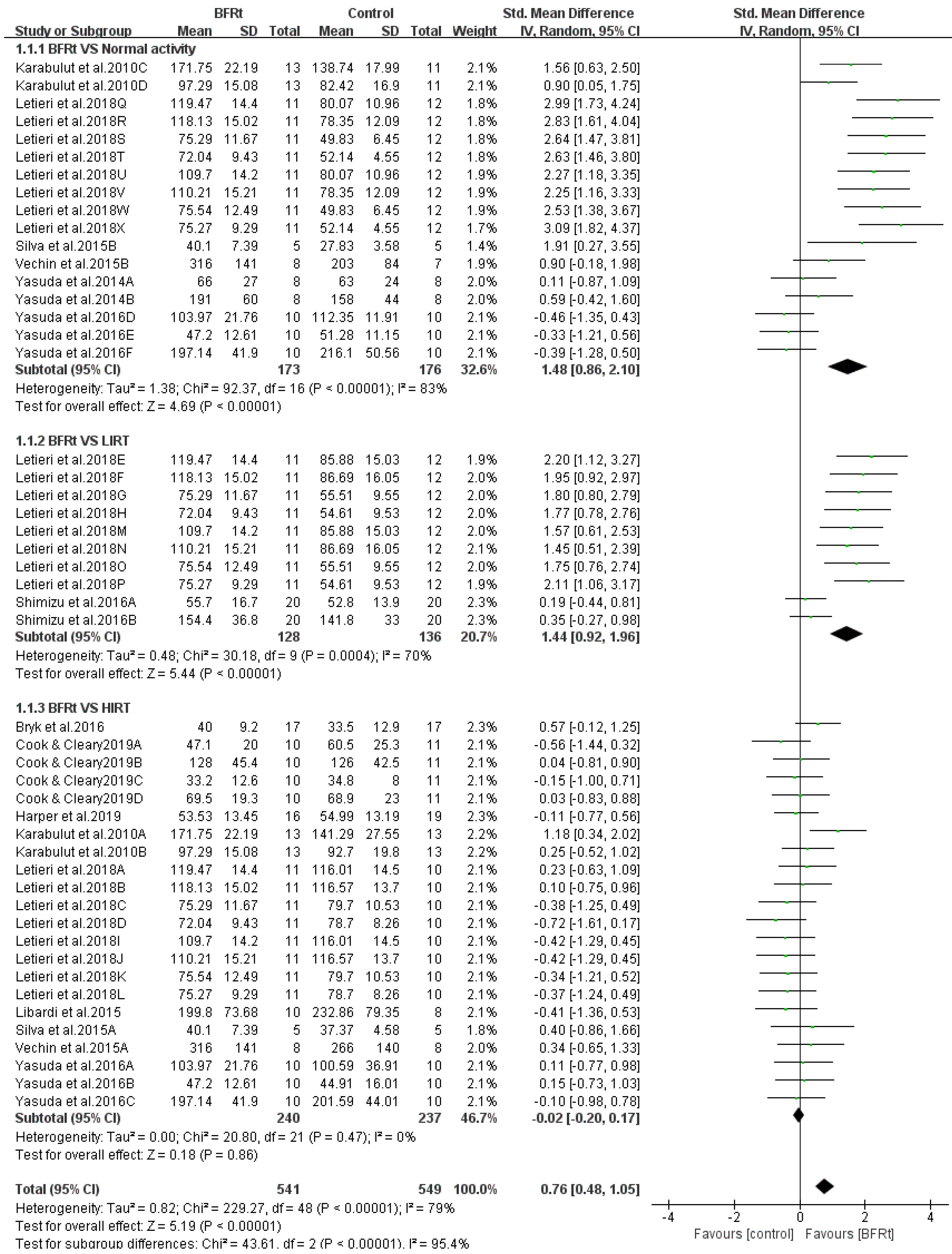
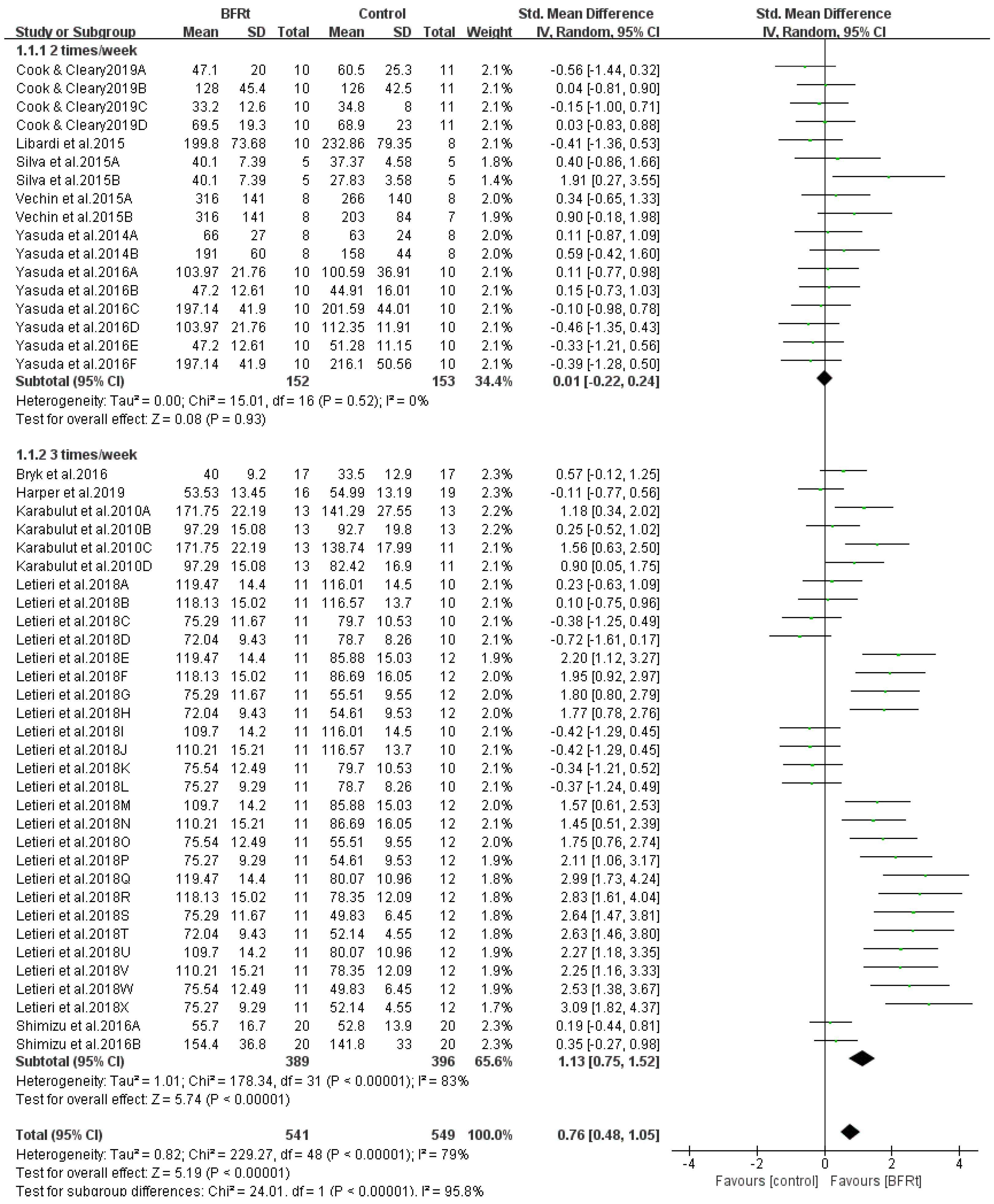
3.4. Effects of BFRt on Lower-Limb Muscle Strength in Post-Middle-Aged Adults
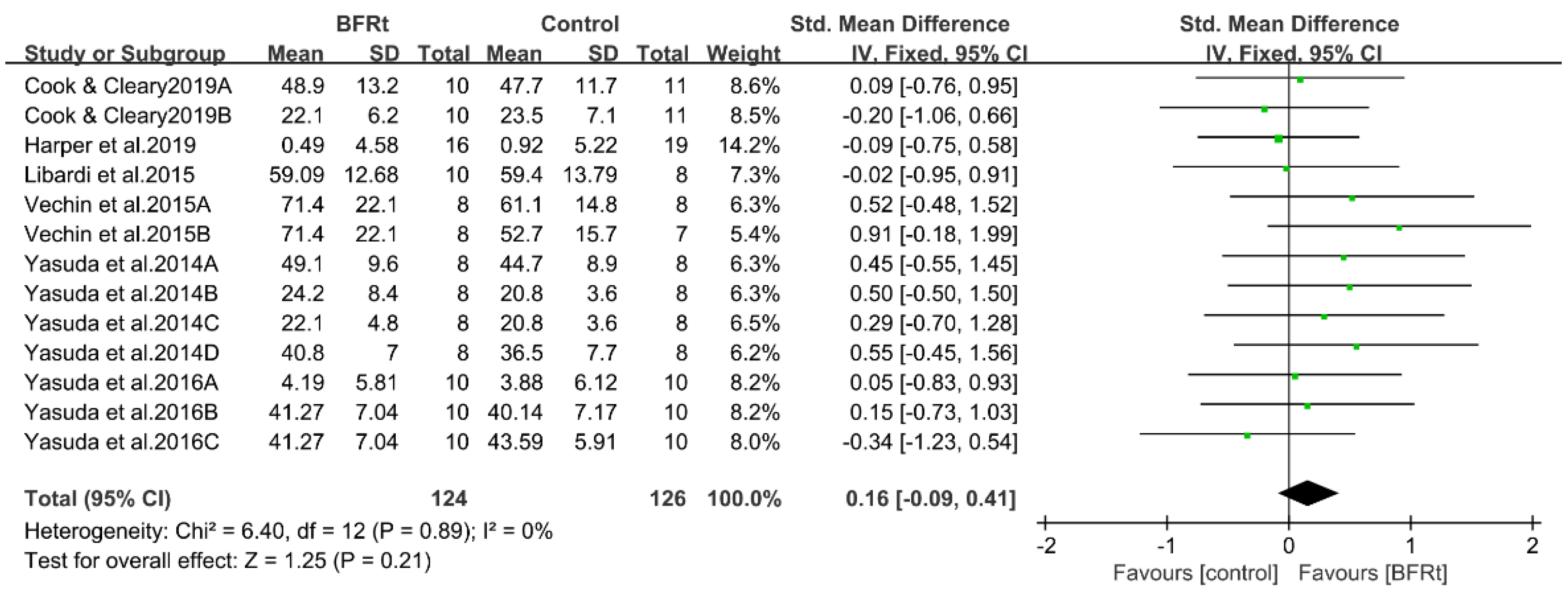
3.5. Effects of BFRt on Lower-Limb Muscle Mass in Post-Middle-Aged Adults
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations. World population prospects 2019: Highlights. In Statistical Papers-United Nations (Ser. A), Population and Vital Statistics Report; United Nations: New York, NY, USA, 2019. [Google Scholar]
- Naczk, M.; Marszalek, S.; Naczk, A. Inertial Training Improves Strength, Balance, and Gait Speed in Elderly Nursing Home Residents. Clin. Interv. Aging 2020, 15, 177–184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Trombetti, A.; Reid, K.F.; Hars, M.; Herrmann, F.R.; Pasha, E.; Phillips, E.M.; Fielding, R.A. Age-associated declines in muscle mass, strength, power, and physical performance: Impact on fear of falling and quality of life. Osteoporos. Int. 2016, 27, 463–471. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Allen, J.; Morelli, V. Aging and exercise. Clin. Geriatr. Med. 2011, 27, 661–671. [Google Scholar] [CrossRef] [PubMed]
- Partridge, L.; Deelen, J.; Slagboom, P.E. Facing up to the global challenges of ageing. Nature 2018, 561, 45–56. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Janssen, W.G.; Bussmann, H.B.; Stam, H.J. Determinants of the sit-to-stand movement: A review. Phys. Ther. 2002, 82, 866–879. [Google Scholar] [CrossRef]
- Krist, L.; Dimeo, F.; Keil, T. Can progressive resistance training twice a week improve mobility, muscle strength, and quality of life in very elderly nursing-home residents with impaired mobility? A pilot study. Clin. Interv. Aging 2013, 8, 443–448. [Google Scholar] [CrossRef] [Green Version]
- Tiggemann, C.L.; Dias, C.P.; Radaelli, R.; Massa, J.C.; Bortoluzzi, R.; Schoenell, M.C.; Noll, M.; Alberton, C.L.; Kruel, L.F. Effect of traditional resistance and power training using rated perceived exertion for enhancement of muscle strength, power, and functional performance. Age 2016, 38, 42. [Google Scholar] [CrossRef] [Green Version]
- Lopez, P.; Pinto, R.S.; Radaelli, R.; Rech, A.; Grazioli, R.; Izquierdo, M.; Cadore, E.L. Benefits of resistance training in physically frail elderly: A systematic review. Aging Clin. Exp. Res. 2018, 30, 889–899. [Google Scholar] [CrossRef]
- López-García, A.; Sánchez-Ruíz, M.E. Feasible Intervention through Simple Exercise for Risk of Falls in Dementia Patients: A Pilot Study. Int. J. Environ. Res. Public Health 2022, 19, 11854. [Google Scholar] [CrossRef]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.M.; Nieman, D.C.; Swain, D.P. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef]
- American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med. Sci. Sports Exerc. 2009, 41, 687–708. [CrossRef] [PubMed]
- Kerr, Z.Y.; Collins, C.L.; Comstock, R.D. Epidemiology of weight training-related injuries presenting to United States emergency departments, 1990 to 2007. Am. J. Sports Med. 2010, 38, 765–771. [Google Scholar] [CrossRef] [PubMed]
- Lim, Z.X.; Goh, J. Effects of blood flow restriction (BFR) with resistance exercise on musculoskeletal health in older adults: A narrative review. Eur. Rev. Aging Phys. Act. 2022, 19, 15. [Google Scholar] [CrossRef] [PubMed]
- Gheno, R.; Cepparo, J.M.; Rosca, C.E.; Cotten, A. Musculoskeletal disorders in the elderly. J. Clin. Imaging Sci. 2012, 2, 39. [Google Scholar] [CrossRef] [PubMed]
- Papa, E.V.; Dong, X.; Hassan, M. Skeletal Muscle Function Deficits in the Elderly: Current Perspectives on Resistance Training. J. Nat. Sci. 2017, 3, e272. [Google Scholar]
- Sato, Y. The history and future of KAATSU training. Int. J. KAATSU Train. Res. 2005, 1, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Heitkamp, H.C. Training with blood flow restriction. Mechanisms, gain in strength and safety. J. Sports Med. Phys. Fit. 2015, 55, 446–456. [Google Scholar]
- Libardi, C.A.; Chacon-Mikahil, M.P.; Cavaglieri, C.R.; Tricoli, V.; Roschel, H.; Vechin, F.C.; Conceição, M.S.; Ugrinowitsch, C. Effect of concurrent training with blood flow restriction in the elderly. Int. J. Sports Med. 2015, 36, 395–399. [Google Scholar] [CrossRef] [Green Version]
- Thiebaud, R.S.; Loenneke, J.P.; Fahs, C.A.; Rossow, L.M.; Kim, D.; Abe, T.; Anderson, M.A.; Young, K.C.; Bemben, D.A.; Bemben, M.G. The effects of elastic band resistance training combined with blood flow restriction on strength, total bone-free lean body mass and muscle thickness in postmenopausal women. Clin. Physiol. Funct. Imaging 2013, 33, 344–352. [Google Scholar] [CrossRef]
- Yasuda, T.; Fukumura, K.; Fukuda, T.; Uchida, Y.; Iida, H.; Meguro, M.; Sato, Y.; Yamasoba, T.; Nakajima, T. Muscle size and arterial stiffness after blood flow-restricted low-intensity resistance training in older adults. Scand. J. Med. Sci. Sports 2014, 24, 799–806. [Google Scholar] [CrossRef]
- Vechin, F.C.; Libardi, C.A.; Conceição, M.S.; Damas, F.R.; Lixandrão, M.E.; Berton, R.P.; Tricoli, V.A.; Roschel, H.A.; Cavaglieri, C.R.; Chacon-Mikahil, M.P.; et al. Comparisons between low-intensity resistance training with blood flow restriction and high-intensity resistance training on quadriceps muscle mass and strength in elderly. J. Strength Cond. Res. 2015, 29, 1071–1076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, T.; Wang, X.; Wang, J. Effect of blood flow restriction combined with low-intensity training on the lower limbs muscle strength and function in older adults: A meta-analysis. Exp. Gerontol. 2022, 164, 111827. [Google Scholar] [CrossRef] [PubMed]
- Centner, C.; Wiegel, P.; Gollhofer, A.; Konig, D. Correction to: Effects of Blood Flow Restriction Training on Muscular Strength and Hypertrophy in Older Individuals: A Systematic Review and Meta-Analysis. Sports Med. 2019, 49, 109–111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigo-Mallorca, D.; Loaiza-Betancur, A.F.; Monteagudo, P.; Blasco-Lafarga, C.; Chulvi-Medrano, I. Resistance Training with Blood Flow Restriction Compared to Traditional Resistance Training on Strength and Muscle Mass in Non-Active Older Adults: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2021, 18, 11441. [Google Scholar] [CrossRef]
- Labata-Lezaun, N.; Llurda-Almuzara, L.; González-Rueda, V.; López-de-Celis, C.; Cedeño-Bermúdez, S.; Bañuelos-Pago, J.; Perez-Bellmunt, A. Effectiveness of Blood Flow Restriction Training on Muscle Strength and Physical Performance in Older Adults: A Systematic Review and Meta-analysis. Arch. Phys. Med. Rehabil. 2022, 103, 1848–1857. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Letieri, R.V.; Teixeira, A.M.; Furtado, G.E.; Lamboglia, C.G.; Rees, J.L.; Gomes, B.B. Effect of 16 weeks of resistance exercise and detraining comparing two methods of blood flow restriction in muscle strength of healthy older women: A randomized controlled trial. Exp. Gerontol. 2018, 114, 78–86. [Google Scholar] [CrossRef]
- Bryk, F.F.; Dos Reis, A.C.; Fingerhut, D.; Araujo, T.; Schutzer, M.; Cury Rde, P.; Duarte, A., Jr.; Fukuda, T.Y. Exercises with partial vascular occlusion in patients with knee osteoarthritis: A randomized clinical trial. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 1580–1586. [Google Scholar] [CrossRef]
- Silva, J.; Rodrigues Neto, G.; Freitas, E.; Neto, E.; Batista, G.; Torres, M.; do Socorro Sousa, M. Chronic Effect of Strength Training with Blood Flow Restriction on Muscular Strength among Women with Osteoporosis. J. Exerc. Physiol. Online 2015, 18, 33–41. [Google Scholar]
- Cook, S.B.; Cleary, C.J. Progression of Blood Flow Restricted Resistance Training in Older Adults at Risk of Mobility Limitations. Front. Physiol. 2019, 10, 738. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harper, S.A.; Roberts, L.M.; Layne, A.S.; Jaeger, B.C.; Gardner, A.K.; Sibille, K.T.; Wu, S.S.; Vincent, K.R.; Fillingim, R.B.; Manini, T.M.; et al. Blood-Flow Restriction Resistance Exercise for Older Adults with Knee Osteoarthritis: A Pilot Randomized Clinical Trial. J. Clin. Med. 2019, 8, 265. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karabulut, M.; Abe, T.; Sato, Y.; Bemben, M.G. The effects of low-intensity resistance training with vascular restriction on leg muscle strength in older men. Eur. J. Appl. Physiol. 2010, 108, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Yasuda, T.; Fukumura, K.; Tomaru, T.; Nakajima, T. Thigh muscle size and vascular function after blood flow-restricted elastic band training in older women. Oncotarget 2016, 7, 33595–33607. [Google Scholar] [CrossRef] [Green Version]
- Yasuda, T.; Fukumura, K.; Sato, Y.; Yamasoba, T.; Nakajima, T. Effects of detraining after blood flow-restricted low-intensity training on muscle size and strength in older adults. Aging Clin. Exp. Res. 2014, 26, 561–564. [Google Scholar] [CrossRef]
- Shimizu, R.; Hotta, K.; Yamamoto, S.; Matsumoto, T.; Kamiya, K.; Kato, M.; Hamazaki, N.; Kamekawa, D.; Akiyama, A.; Kamada, Y.; et al. Low-intensity resistance training with blood flow restriction improves vascular endothelial function and peripheral blood circulation in healthy elderly people. Eur. J. Appl. Physiol. 2016, 116, 749–757. [Google Scholar] [CrossRef]
- Cook, S.B.; LaRoche, D.P.; Villa, M.R.; Barile, H.; Manini, T.M. Blood flow restricted resistance training in older adults at risk of mobility limitations. Exp. Gerontol. 2017, 99, 138–145. [Google Scholar] [CrossRef]
- Krogh-Madsen, R.; Thyfault, J.P.; Broholm, C.; Mortensen, O.H.; Olsen, R.H.; Mounier, R.; Plomgaard, P.; van Hall, G.; Booth, F.W.; Pedersen, B.K. A 2-wk reduction of ambulatory activity attenuates peripheral insulin sensitivity. J. Appl. Physiol. 2010, 108, 1034–1040. [Google Scholar] [CrossRef] [Green Version]
- Kubota, A.; Sakuraba, K.; Koh, S.; Ogura, Y.; Tamura, Y. Blood flow restriction by low compressive force prevents disuse muscular weakness. J. Sci. Med. Sport 2011, 14, 95–99. [Google Scholar] [CrossRef]
- Suga, T.; Okita, K.; Morita, N.; Yokota, T.; Hirabayashi, K.; Horiuchi, M.; Takada, S.; Takahashi, T.; Omokawa, M.; Kinugawa, S.; et al. Intramuscular metabolism during low-intensity resistance exercise with blood flow restriction. J. Appl. Physiol. 2009, 106, 1119–1124. [Google Scholar] [CrossRef] [Green Version]
- Schoenfeld, B.J.; Ogborn, D.; Krieger, J.W. Effects of Resistance Training Frequency on Measures of Muscle Hypertrophy: A Systematic Review and Meta-Analysis. Sports Med. 2016, 46, 1689–1697. [Google Scholar] [CrossRef] [PubMed]
- Grgic, J.; Schoenfeld, B.J.; Davies, T.B.; Lazinica, B.; Krieger, J.W.; Pedisic, Z. Effect of Resistance Training Frequency on Gains in Muscular Strength: A Systematic Review and Meta-Analysis. Sports Med. 2018, 48, 1207–1220. [Google Scholar] [CrossRef] [PubMed]
- Ralston, G.W.; Kilgore, L.; Wyatt, F.B.; Buchan, D.; Baker, J.S. Weekly Training Frequency Effects on Strength Gain: A Meta-Analysis. Sports Med. Open 2018, 4, 36. [Google Scholar] [CrossRef] [PubMed]
- Burd, N.A.; West, D.W.; Moore, D.R.; Atherton, P.J.; Staples, A.W.; Prior, T.; Tang, J.E.; Rennie, M.J.; Baker, S.K.; Phillips, S.M. Enhanced amino acid sensitivity of myofibrillar protein synthesis persists for up to 24 h after resistance exercise in young men. J. Nutr. 2011, 141, 568–573. [Google Scholar] [CrossRef] [Green Version]
- Phillips, S.M.; Tipton, K.D.; Aarsland, A.; Wolf, S.E.; Wolfe, R.R. Mixed muscle protein synthesis and breakdown after resistance exercise in humans. Am. J. Physiol. 1997, 273, E99–E107. [Google Scholar] [CrossRef]
- Pareja-Blanco, F.; Rodríguez-Rosell, D.; Aagaard, P.; Sánchez-Medina, L.; Ribas-Serna, J.; Mora-Custodio, R.; Otero-Esquina, C.; Yáñez-García, J.M.; González-Badillo, J.J. Time Course of Recovery From Resistance Exercise With Different Set Configurations. J. Strength Cond. Res. 2020, 34, 2867–2876. [Google Scholar] [CrossRef]
- Dankel, S.J.; Mattocks, K.T.; Jessee, M.B.; Buckner, S.L.; Mouser, J.G.; Counts, B.R.; Laurentino, G.C.; Loenneke, J.P. Frequency: The Overlooked Resistance Training Variable for Inducing Muscle Hypertrophy? Sports Med. 2017, 47, 799–805. [Google Scholar] [CrossRef]
- Loenneke, J.P.; Fahs, C.A.; Wilson, J.M.; Bemben, M.G. Blood flow restriction: The metabolite/volume threshold theory. Med. Hypotheses 2011, 77, 748–752. [Google Scholar] [CrossRef]
- Fujita, T.; WF, B.; Kurita, K.; Sato, Y.; Abe, T. Increased muscle volume and strength following six days of low-intensity resistance training with restricted muscle blood flow. Int. J. KAATSU Train. Res. 2008, 4, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Abe, T.; Yasuda, T.; Midorikawa, T.; Sato, Y.; CF, K.; Inoue, K.; Koizumi, K.; Ishii, N. Skeletal muscle size and circulating IGF-1 are increased after two weeks of twice daily “KAATSU” resistance training. Int. J. KAATSU Train. Res. 2005, 1, 6–12. [Google Scholar] [CrossRef] [Green Version]
- Hwang, P.S.; Willoughby, D.S. Mechanisms Behind Blood Flow-Restricted Training and its Effect Toward Muscle Growth. J. Strength Cond. Res. 2019, 33 (Suppl. S1), S167–S179. [Google Scholar] [CrossRef] [PubMed]
- Manini, T.M.; Yarrow, J.F.; Buford, T.W.; Clark, B.C.; Conover, C.F.; Borst, S.E. Growth hormone responses to acute resistance exercise with vascular restriction in young and old men. Growth Horm. IGF Res. 2012, 22, 167–172. [Google Scholar] [CrossRef] [Green Version]
- Pearson, S.J.; Hussain, S.R. A review on the mechanisms of blood-flow restriction resistance training-induced muscle hypertrophy. Sports Med. 2015, 45, 187–200. [Google Scholar] [CrossRef] [PubMed]
- Loenneke, J.P.; Abe, T.; Wilson, J.M.; Ugrinowitsch, C.; Bemben, M.G. Blood flow restriction: How does it work? Front. Physiol. 2012, 3, 392. [Google Scholar] [CrossRef] [Green Version]
- Laurentino, G.C.; Loenneke, J.P.; Ugrinowitsch, C.; Aoki, M.S.; Soares, A.G.; Roschel, H.; Tricoli, V. Blood-Flow-Restriction-Training-Induced Hormonal Response is not Associated with Gains in Muscle Size and Strength. J. Hum. Kinet. 2022, 83, 235–243. [Google Scholar] [CrossRef] [PubMed]
- Schoenfeld, B.J. The mechanisms of muscle hypertrophy and their application to resistance training. J. Strength Cond. Res. 2010, 24, 2857–2872. [Google Scholar] [CrossRef] [Green Version]
- Lang, F. Mechanisms and significance of cell volume regulation. J. Am. Coll. Nutr. 2007, 26, 613s–623s. [Google Scholar] [CrossRef]
- Meyer, R.A. Does blood flow restriction enhance hypertrophic signaling in skeletal muscle? J. Appl. Physiol. 2006, 100, 1443–1444. [Google Scholar] [CrossRef]
- Sundberg, C.J. Exercise and training during graded leg ischaemia in healthy man with special reference to effects on skeletal muscle. Acta Physiol. Scand. Suppl. 1994, 615, 1–50. [Google Scholar]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Age | Gender, M/F | Groups/Sessions | Exercise Mode | Duration (wk) | Frequency (t/wk) | Sets × Repetitions | Cuff Pressure (mm Hg) | Cuff Width (cm) | Muscle Strength/Mass |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Bryk et al., 2016 [30] | Brazil | 30% 1RM-BFR, 62.3 ± 7; 70% 1RM, 60.4 ± 6.7 | 34/0 | 30% 1RM-BFR, N = 17; 70% 1RM, N = 17 | quadriceps exercise | 6 | 3 | 30% 1RM-BFR 3 × 10; 70% 1RM 3 × 10 | 200 | NR | Quadriceps strength |
| Cook & Cleary 2019 [32] | USA | 67–90 | 9/12 | 30% 1RM-BFR, N = 10; 70% 1RM, N = 11 | Knee flexion, leg press, knee extension | 12 | 2 | 30% 1RM-BFR 3 × 10; 70% 1RM 3 × 10 | 184 ± 25 | 6 | Knee extension (10RM, MVC), Knee flexion (10RM, MVC); Quadriceps CSA, Hamstrings CSA |
| Harper et al., 2019 [33] | USA | ≥60 | NR | 20% 1RM-BFR, N = 16; 60% 1RM, N = 19 | leg press, leg extension, calf flexion, leg curl, | 12 | 3 | NR | 0.5 (SBP) + 2 (thighcircumference) + 5 | NR | knee extensor Strength torque; Lower body lean mass |
| Karabulut et al., 2010 [34] | USA | 56.8 ± 0.6 | 37/0 | 20% 1RM-BFR, N = 13; 80% 1RM, N = 13; normal activity, N = 11 | leg press, leg extension | 6 | 3 | 20% 1RM-BFR 30,15,15; 80% 1RM 3 × 8; | 205.4 ± 4.3 | NR | Leg press strength, Leg extension strength |
| Libardi et al., 2015 [19] | Brazil | 64.7 ± 4.1 | NR | 20–30% 1RM-BFR, N = 10; 70–80% 1RM, N = 8 | leg press | 12 | 2 | 20–30% 1RM-BFR 30,15,15,15; 70–80% 1RM 4 × 10 | 67 ± 8.0 | 17.5 | Leg press 1RM; Quadriceps CSA |
| Shimizu et al., 2016 [37] | Japan | 71 ± 4 | 33/7 | 20% 1RM-BFR, N = 20; 20% 1RM, N = 20 | leg extension, leg press | 4 | 3 | 20% 1RM-BFR 3 × 20; 20% 1RM 3 × 20 | 100% femoral SBP | 10 | Leg extension 1RM, Leg press 1RM, |
| Silva et al., 2015 [31] | Brazil | 62.2 ± 4.53 | 0/15 | 30% 1RM- BFR, N = 5; 80% 1RM, N = 5; normal activity, N = 5 | knee extension (right, leg) | 12 | 2 | 30% 1RM-BFR 4 × (7.0 ± 3.38); 80% 1RM 4 × 8.0 ± 2.0 | 104.20 ± 7.88 | 18 | Leg extension-R 1RM |
| Vechin et al., 2015 [22] | Brazil | 64.04 ± 3.81 | 14/9 | 20–30% 1RM-BFR, N = 8; 70–80% 1RM, N = 8; normal activity, N = 7 | leg press | 12 | 2 | 20–30% 1RM-BFR 30,15,15,15; 70–80% 1RM, 4 × 10 | 71 ± 9 | 18 | Leg press 1RM; Quadriceps CSA |
| Yasuda et al., 2016 [35] | Japan | 61–86 | 0/30 | 35–45% 1RM-BFR, N = 10; 70–90% 1RM, N = 10; normal activity, N = 10 | bilateral squat, knee extension | 12 | 2 | 35–45% 1RM-BFR 30,15,15,15; 70–90% 1RM 13, 13 (at 1st–12th training session) or 12 (at 13th–24th training session | 161 ± 12 | 5 | Knee extension, (1RM, MVC), Leg press 1RM; Quadriceps CSA, Muscle thickness of mid-thigh |
| Yasuda et al., 2014 [36] | Japan | 61–78 | 5/11 | 20–30% 1RM-BFR, N = 8; normal activity, N = 8 | NR | 12 | 2 | NR | 120–270 | NR | Knee extension 1RM, Leg press 1RM; Quadriceps CSA, Adductors CSA, Hamstrings CSA, Gluteus maximus CSA |
| Letieri et al., 2018 [29] | Brazil | 68.8 ± 5.09 | 0/56 | 20–30% 1RM- BFR- high occlusion pressure, N = 11; 20–30% 1RM-BFR-low occlusion pressure, N = 11; 70–80% 1RM, N = 10; 20–30% 1RM, N = 12; normal activity, N = 12 | Squat, Leg Press, Knee Extension, Leg Curl | 16 | 3 | 20–30% 1RM- BFR-high occlusion pressure 3–4 × 15; 20–30% 1RM- BFR- low occlusion pressure 3–4 × 15; 70–80% 1RM 3–4 × 6–8; 20–30% 1RM 3–4 × 15 | 20–30% 1RM-BFR-H 185.75 ± 5.45 20–30% 1RM-BFR-L 105.45 ± 6.5 | NR | Peak Torque Extension (right, left), Peak Right Flexion (right, left) |
| Experimental Intervention | Coefficient | Standard Error | T-Value | p-Value | [95% Conf. Interval] | |
|---|---|---|---|---|---|---|
| Comparator intervention group | 0.820633 | 0.1485629 | 5.52 | 0.000 | 0.5198832 | 1.121383 |
| Exercise mode | 0.0279026 | 0.136192 | 0.20 | 0.839 | −0.2478037 | 0.3036089 |
| Cuff pressure | 0.0008191 | 0.00321 | 0.26 | 0.800 | −0.0056792 | 0.0073174 |
| Duration (wk) | 0.0348827 | 0.0448527 | 0.78 | 0.442 | −0.0559168 | 0.1256822 |
| Frequency (t/wk) | 0.8428523 | 0.3637526 | 2.32 | 0.026 | 0.1064737 | 1.579231 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chang, H.; Yao, M.; Chen, B.; Qi, Y.; Zhang, J. Effects of Blood Flow Restriction Combined with Low-Intensity Resistance Training on Lower-Limb Muscle Strength and Mass in Post-Middle-Aged Adults: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 15691. https://doi.org/10.3390/ijerph192315691
Chang H, Yao M, Chen B, Qi Y, Zhang J. Effects of Blood Flow Restriction Combined with Low-Intensity Resistance Training on Lower-Limb Muscle Strength and Mass in Post-Middle-Aged Adults: A Systematic Review and Meta-Analysis. International Journal of Environmental Research and Public Health. 2022; 19(23):15691. https://doi.org/10.3390/ijerph192315691
Chicago/Turabian StyleChang, Hualong, Mengxing Yao, Biao Chen, Yongle Qi, and Jianli Zhang. 2022. "Effects of Blood Flow Restriction Combined with Low-Intensity Resistance Training on Lower-Limb Muscle Strength and Mass in Post-Middle-Aged Adults: A Systematic Review and Meta-Analysis" International Journal of Environmental Research and Public Health 19, no. 23: 15691. https://doi.org/10.3390/ijerph192315691