
Specific Needs of Patients and Staff Reflected in the Design of an Orthopaedic and Rehabilitation Hospital—Design Recommendations Based on a Case Study (Poland)


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
1.1. Design of Healthcare Facilities and Its Social Impact
- Personal features of patients affect their satisfaction regarding hospital admission;
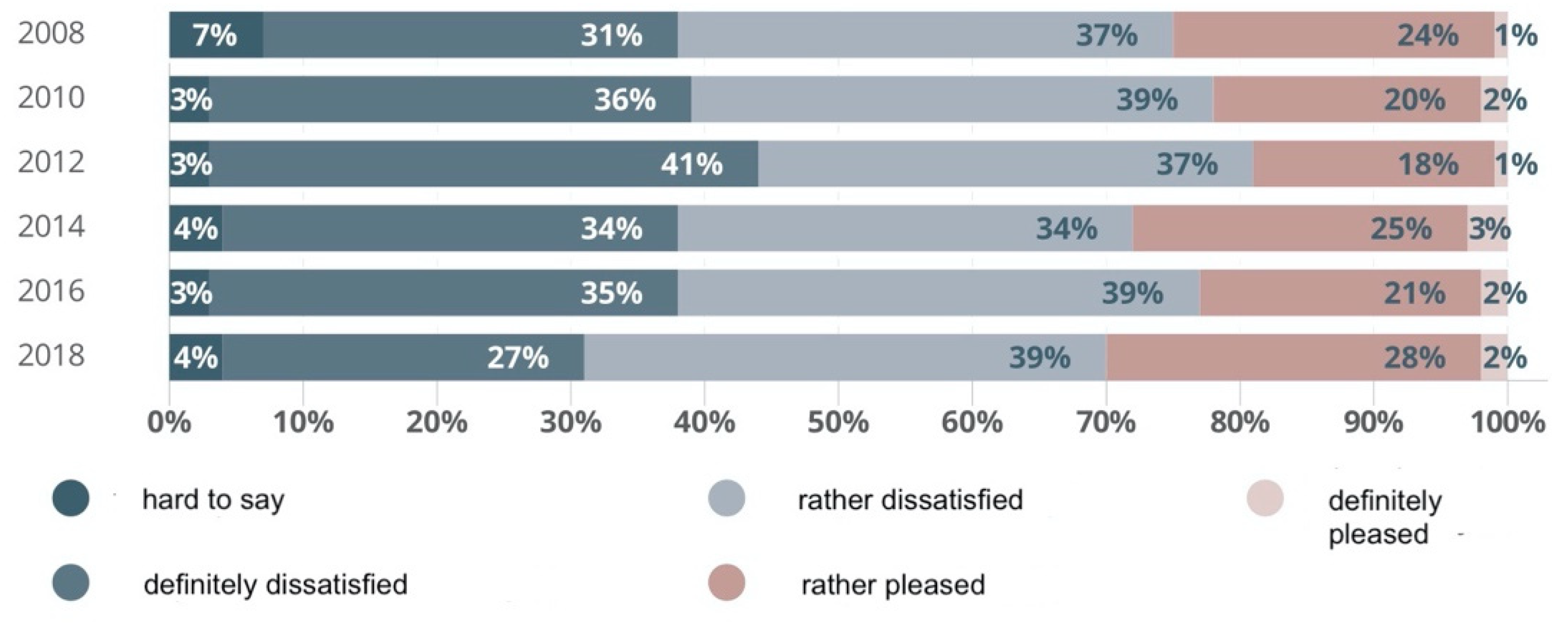
- ”Face to face” opinion polls are more reliable;
- If patients’ expectations are taken into account at the modernisation of space of admission rooms, patients’ satisfaction level increases.
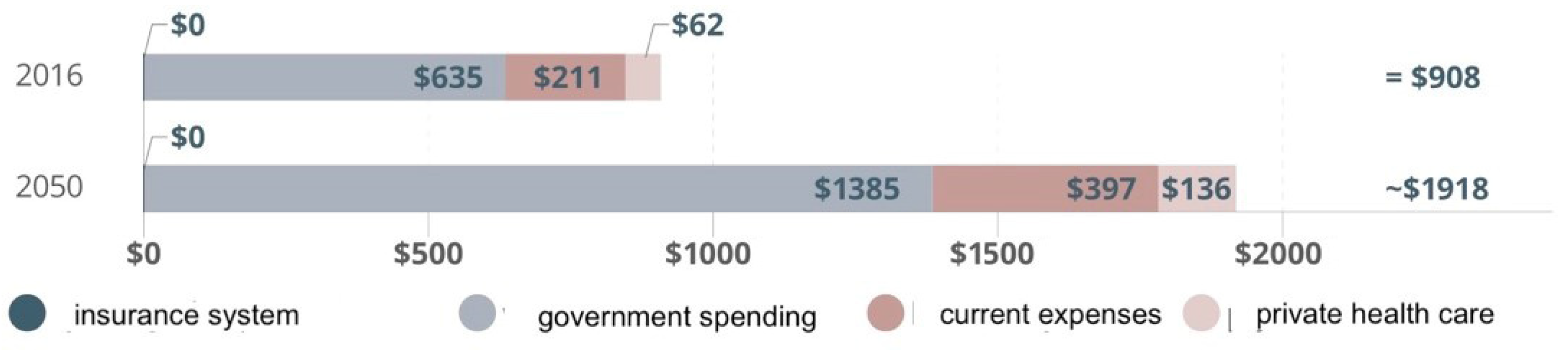
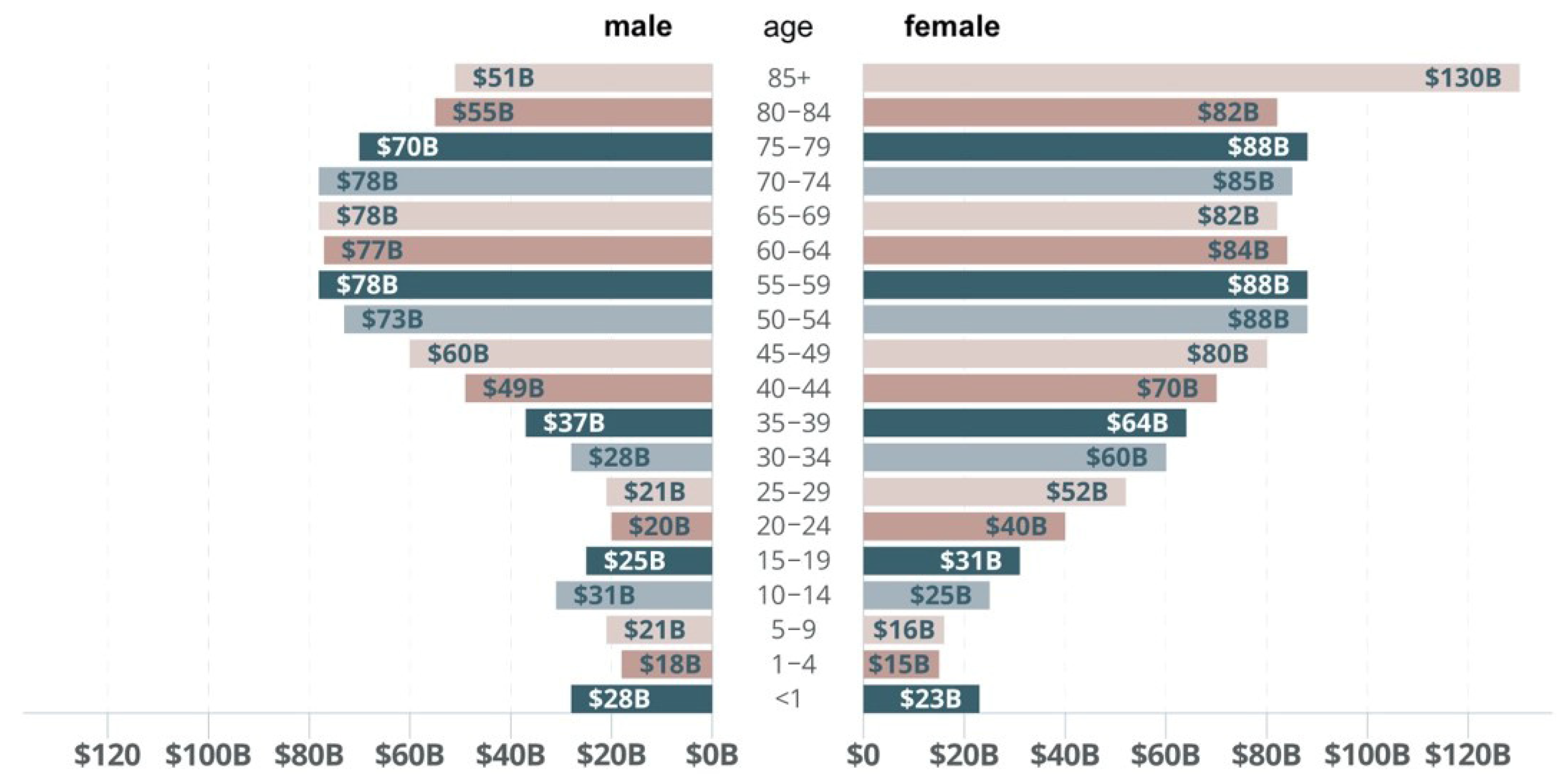
1.2. Situation of Healthcare Facilities in Poland in View of an Ageing Society
2. Material and Methods
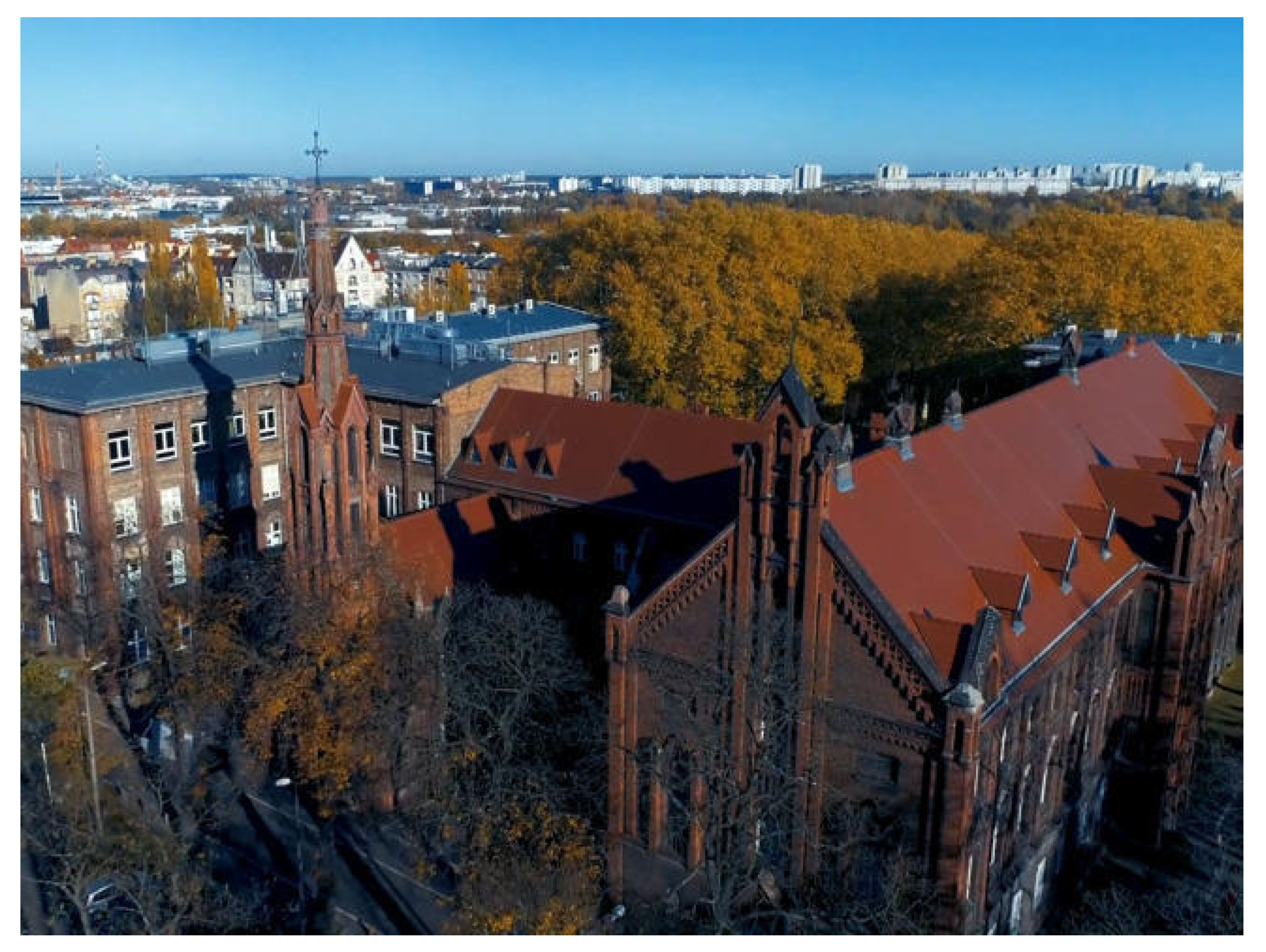
2.1. W. Dega Hospital in Poznan (Poland)
2.2. Methodology
| Personnel perspective: |
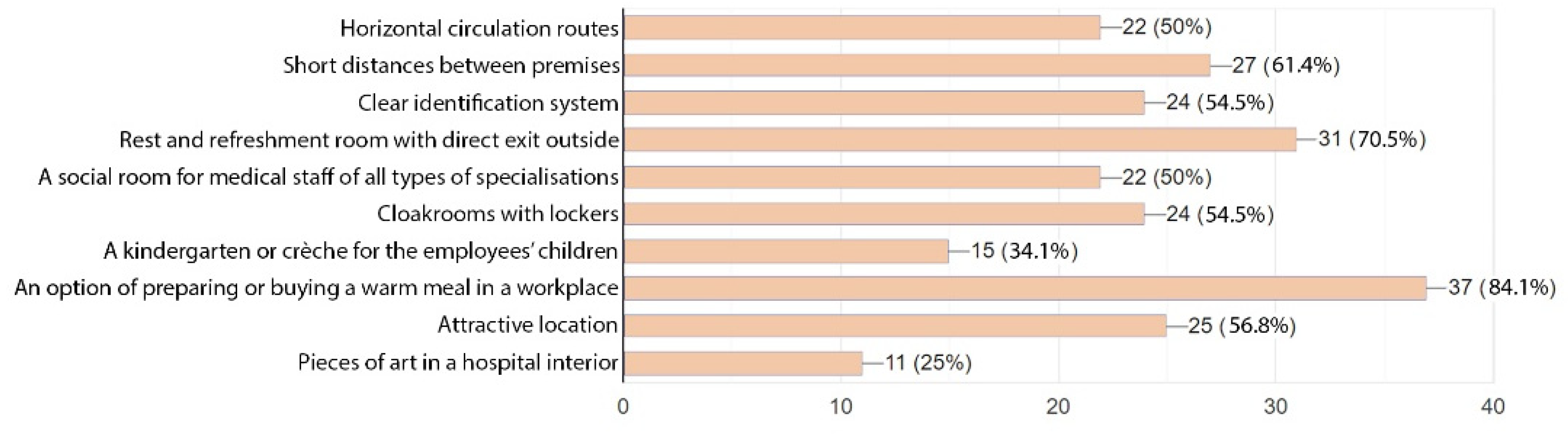
| 1. What emotions does work in the orthopaedic ward evoke in you? 2. What are your expectations for hospital space improvements? (Choose from those listed below or enter your own) - Horizontal circulation routes - Short distances between premises - Clear identification system - Rest and refreshment rooms with direct exit outside - A social room for a medical staff of all types of specialization - Cloakroom with lockers - A kindergarten or creche for the employees’ children - An option of preparing or buying a warm meal in the workplace - Attractive location - Pieces of art in hospital interiors - Other:…. |
| Patient perspective: |
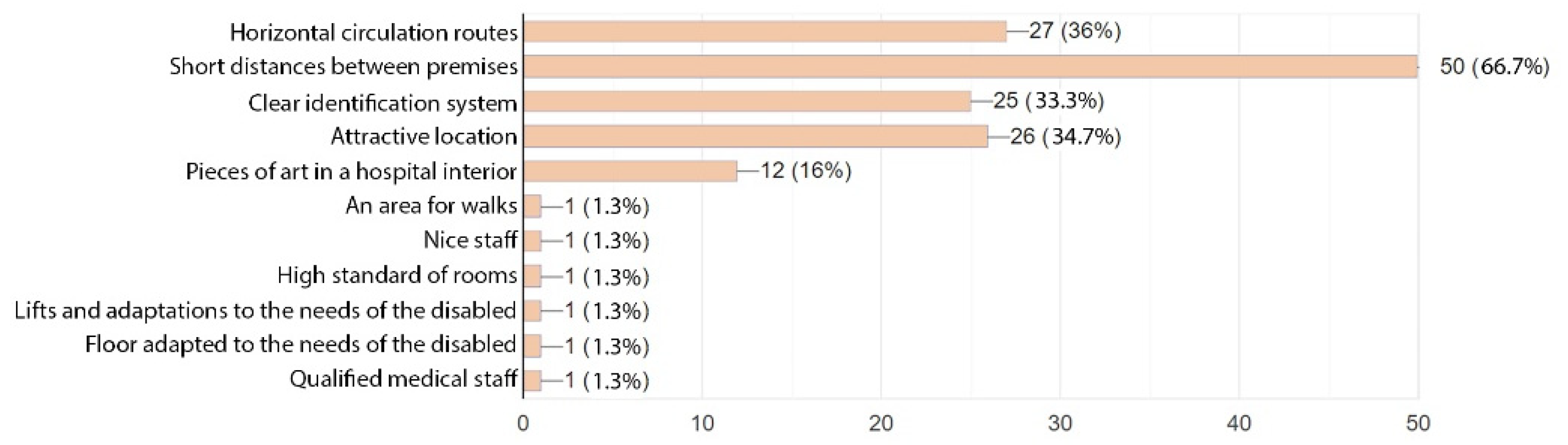
| 1. What emotions does work in the orthopaedic ward evoke in you? 2. What are your expectations for hospital space improvements? (Choose from those listed below or enter your own) - Horizontal circulation routes - Short distances between premises - Clear identification system - Rest and refreshment rooms with direct exit outside - A social room for a medical staff of all types of specialization - Cloakroom with lockers - A kindergarten or creche for the employees’ children - An option of preparing or buying a warm meal in workplace - Attractive location - Pieces of art in hospital interiors - Other:…. |
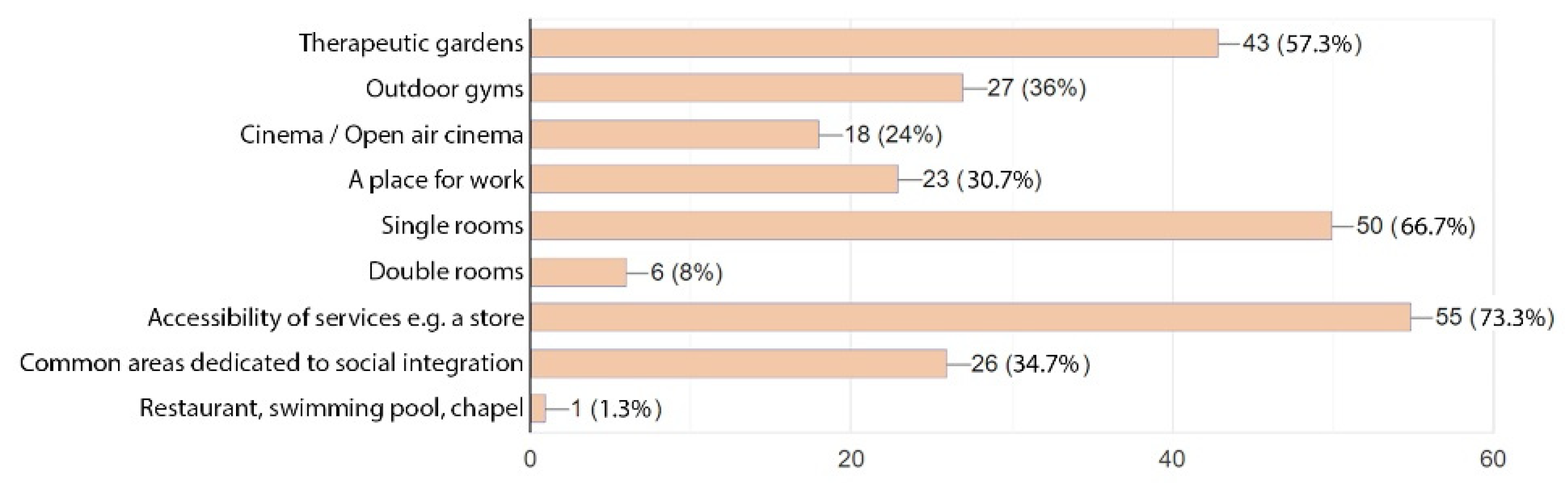
| 3. What are additional functions missing in the hospital that are concerned or well-proven in other similar facilities? - Therapeutic garden - Outdoor gyms - Cinema/open air cinema - A place for work - Single rooms - Double rooms - Accessibility of services, e.g., a store - Common areas dedicated to social integration - Restaurant, swimming pool, chapel |
2.3. Qualitative Studies—Results



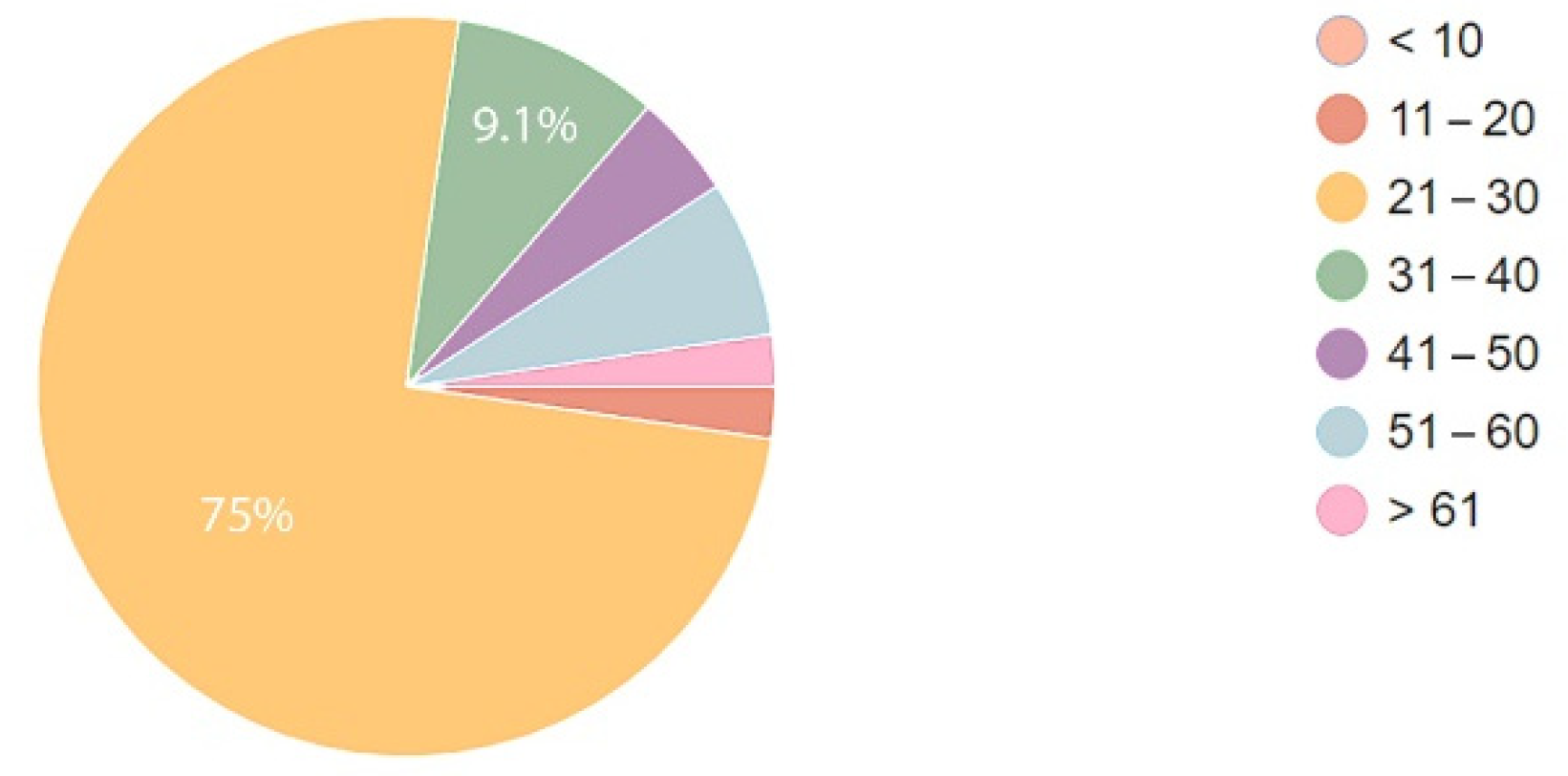
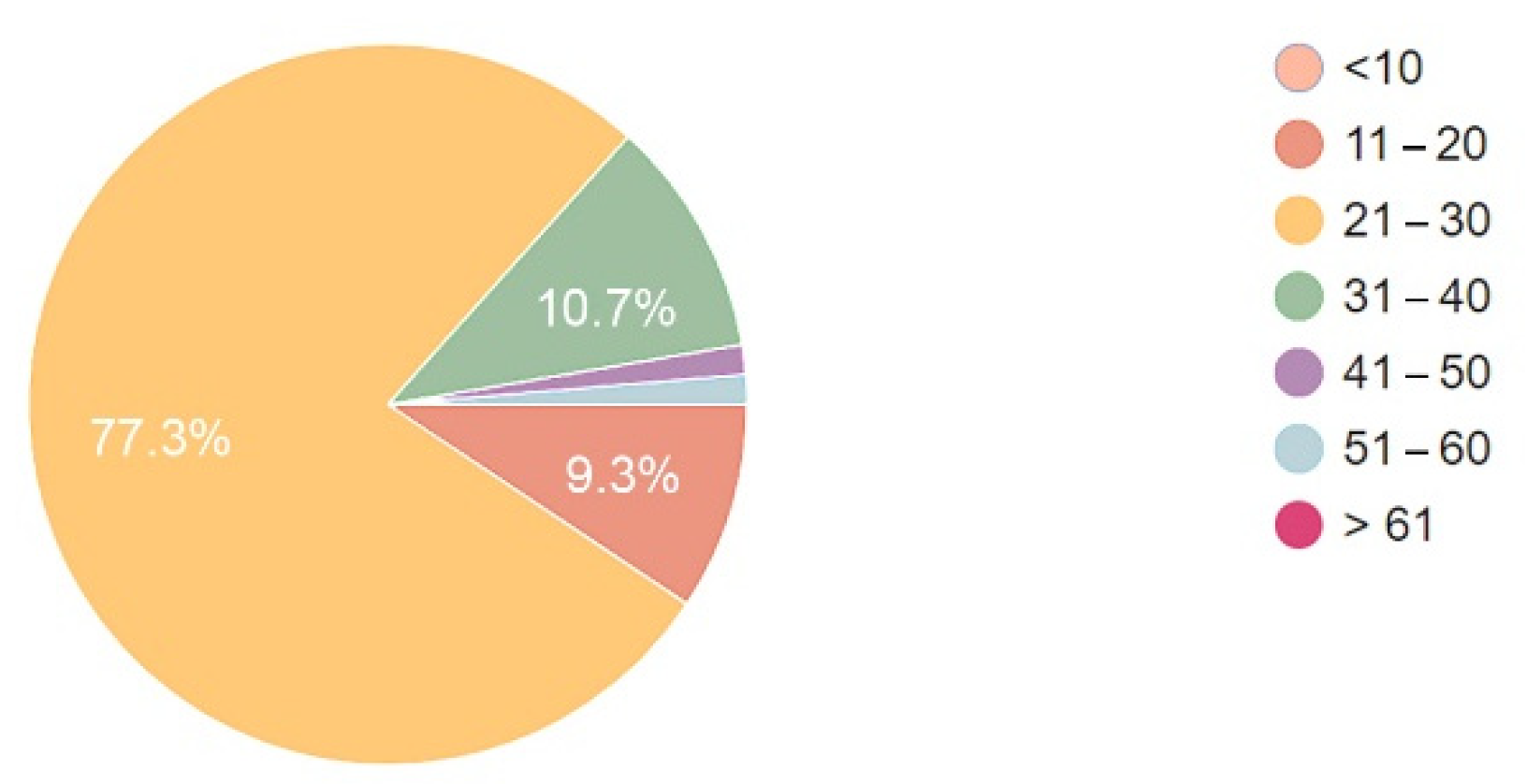
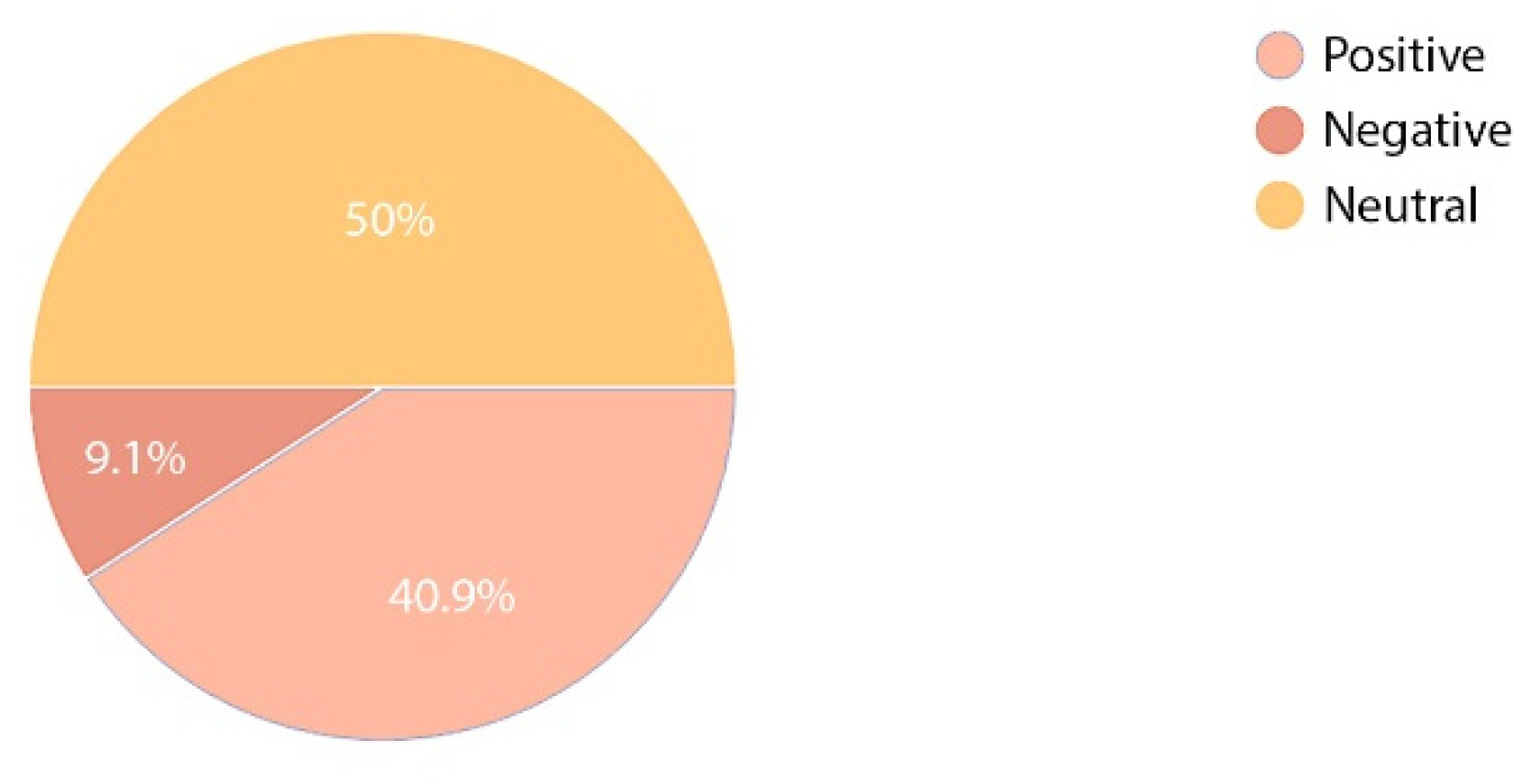
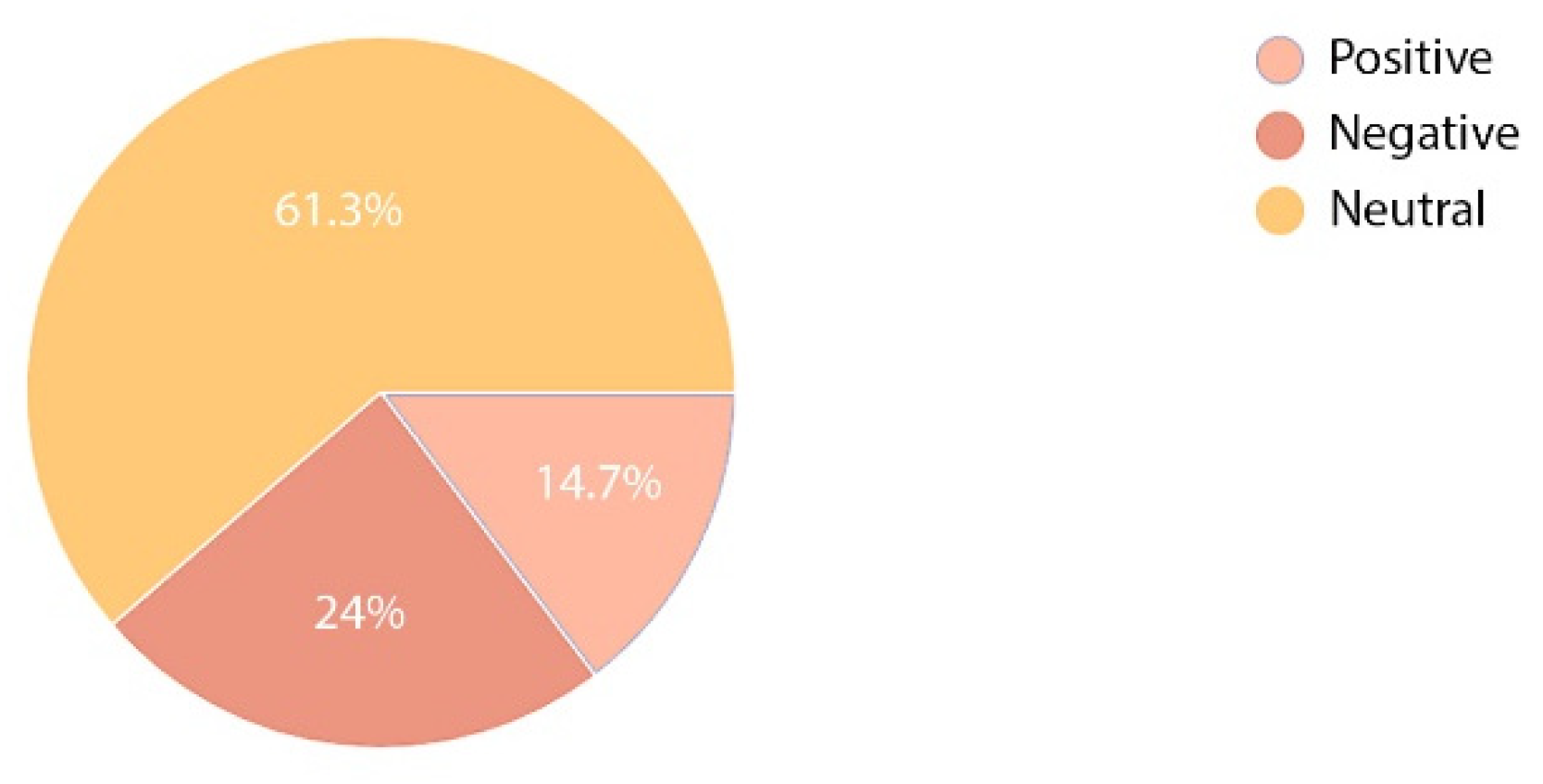
2.4. Quantitative Research—Results
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Price, A.D.F.; Lu, J. Impact of hospital space standardization on patient health and safety. Archit. Eng. Des. Manag. 2013, 9, 49–61. [Google Scholar] [CrossRef]
- Lang, J. Creating Architectural Theory: The Role of the Behavioral Science in Environmental Design; Van Nostrand Reinhold: New York, NY, USA, 1997. [Google Scholar]
- Springer, P. rticipatory design of healthcare facilities using virtual reality. Teka Kom. Archit. Urban. I Stud. Kraj. 2020, 16, 128–136. [Google Scholar] [CrossRef]
- Ulrich, R.; Quan, X.; Zimring, C.; Joseph, A.; Choudhary, R. The role of the physical environment in the hospital of the 21st century: A once-in-a-lifetime opportunity [Electronic version]. J. Manag. Policy Pract. 2013, 14. Available online: http://www.healthdesign.org/sites/default/files/Role%20Physical%20Environ%20in%20the%2021st%20Century%20Hospital_0.pdf,stanna10.04.2014r (accessed on 1 January 2020).
- Mourshed, M.; Zhao, Y. Healthcare providers’ perception of design factors related to physical environments—Ronments in hospitals. J. Environ. Psychol. 2012, 32, 362–370. [Google Scholar] [CrossRef] [Green Version]
- Agata, G. Architektura Szpitala—Izba Przyjęć, Wyd; Politechniki Poznańskiej: Poznań, Poland, 2019. [Google Scholar]
- Bahari, M.B.; Ling, Y.W. Factors Contributing to Customer Satisfaction with Community Pharmacies in Malaysia. J. Public Health 2010, 18, 35–41. [Google Scholar] [CrossRef]
- Monjur, M.; Yisong, Z. Building Energy Research Group, School of Civil and Building Engineering; Loughborough University: Loughborough, UK, 2014. [Google Scholar]
- McKee, M.; Healy, J. Hospitals in a Changing Europe; WHO, Open University Press: Buckingham, UK, 2002. [Google Scholar]
- Tsai, C.Y.; Wang, M.C.; Liao, W.T.; Lu, J.H.; Sun, P.H.; Lin, B.Y.J.; Breen, G.M. Hospital outpatient perceptions of the physical environment of waiting areas: The role of patient characteristics on atmospherics in one academic medical center. MC Health Serv. Res. 2007, 7, 198. [Google Scholar] [CrossRef] [Green Version]
- Cadirci, T.O.; Akmaz, A.E. The Impact of Healthscape on Customer Satisfaction and Loyalty in Public and Private Healthcare Institutions. Yildiz Soc. Sci. Rev. 2017, 3, 81–962. [Google Scholar]
- Caixeta, M.C.B.F.; Fabricio, M.M. Physical-digital model for co-design in healthcare buildings. J. Build. Eng. 2021, 34, 101900. [Google Scholar] [CrossRef]
- Weinstein, M.C.; Stason, W.B. Foundations of cost-effectiveness analysis for health and medical practices. N. Engl. J. Med. 1977, 296, 716–721. [Google Scholar] [CrossRef]
- Institute for Health Metrics and Evaluation (IHME). Financing Global Health 2019: Tracking Health Spending in a Time of Crisis; IHME: Seattle, WA, USA, 2020. [Google Scholar]
- Gholami, R.; Higon, A.D.; Emrouznejad, A. Hospital Performance: Efficiency or quality? Can we have both with IT? Expert Syst. Appl. 2015, 42, 5390–5400. [Google Scholar] [CrossRef] [Green Version]
- GUS, Central Statistical Office Poland, Source. Available online: https://stat.gov.pl/en/topics/health/health/methodological-report-health-and-health-care-statistics-statistics-polands-reports,16,2.html (accessed on 20 August 2022).
- Lurka, K. Dużo Łóżek Szpitalnych, za Dużo, Termedia. 2019. Available online: https://www.termedia.pl/mz/Duzo-lozek-szpitalnych-za-duzo,33181.html (accessed on 20 August 2022).
- Nikou, S.; Agahari, W.; Keijzer-Broers, W.; de Reuver, M. Digital healthcare technology adoption by elderly people: A capability approach model. Telemat. Inform. 2020, 53, 101315. [Google Scholar] [CrossRef]
- Kasali, A.; Nersessian, J.N. Architects in interdyscyplinary contexts: Representational practices in healthcare design. Des. Stud. 2015, 41, 205–223. [Google Scholar] [CrossRef]
- Dega, W. Hospital in Poznan (Poland) Website. Available online: https://orsk.pl (accessed on 20 August 2022).
- Reay, S.; Collier, G.; Kennedy-Good, J.; Old, A.; Reid, D.; Bill, A. Designing the future of healthcare together: Prototyping a hospital co-design space. CoDesign 2017, 13, 227–244. [Google Scholar] [CrossRef]
- Lawson, B.; Phiri, M. The Architectural Healthcare Environment and its Effects on Patients. 2003. Available online: http://www.wales.nhs.uk/sites3/documents/254/archhealthenv.pdf (accessed on 18 July 2022).
- Health Outcomes; University of Sheffield, NHS Estates: Sheffield, UK, 2021.
- Hsieh, Y.S. Taking Patients’ Voices Into Account Within Quality Systems: A Comparative Study. Int. J. Health Care Qual. Assur. 2009, 22, 289–299. [Google Scholar] [CrossRef] [PubMed]
- Benek, I.; Szewczenko, A. Realizacja potrzeb społecznych pacjentów w obrębie szpitala geriatrycznego. Acta Univ. Lodz. Folia Oeconomica 2015, 4, 315. [Google Scholar] [CrossRef]
- Bielak-Zasadzka, M.; Bryśkiewicz, K. Evidence-based design i jakość behawioralna w przestrzeni medycznej. Projekt koncepcyjny obiektu szpitalnego. Builder 2021, 25, 44–47. [Google Scholar] [CrossRef]
- Dentzer, S. Healthcare without Walls. A Roadmap for Reinventing U.S. Health Care, Wyd; NEHI: Cambridge, UK, 29 October 2018; ISBN 728915414. [Google Scholar]
- Pereno, A.; Eriksson, D. A multi-stakeholder perspective on sustainable healthcare: From 2030 onwards. Futures 2020, 122, 1026052. [Google Scholar] [CrossRef]
- Groat, L.; Wang, D. Architectural Research Methods; John Wiley & Sons: Hoboken, NJ, USA, 2013. [Google Scholar]
- Poplatek, J.; Marczak, E.; Czabański, W.; Pokrzywnicka, K. Architektura Ochrony Zdrowia. Teoria i Praktyka; Wydawnictwo Politechniki Gdańskiej: Gdańsk, Poland, 2018. [Google Scholar]
- Wagenar, C.; Mens, N.; Manja, G.; Niemeijer, C.; Guthknecht, T. A Design Manual Hospitals; Birkhauser: Basel, Switzerland, 2020. [Google Scholar]
- Harty, C.; Jacobsen, P.H.; Tryggestad, K. Constructing healthcare spaces—The complex role of visualizations in negotiating hospital designs and practices. Procedia Econ. Financ. 2015, 21, 578–585. [Google Scholar] [CrossRef] [Green Version]
- Ferris, T.K. Evidence-Based Design and the Fields of Human Factors and Ergonomics: Complementary Systems-Oriented Approaches to Healthcare Design. Health Environ. Res. Des. J. 2013, 6, 3–5. [Google Scholar] [CrossRef]
- Becker, F.; Parsons, K.S. Hospital facilities and the role of evidence-based design. J. Facil. Manag. 2007, 5, 263–274. [Google Scholar] [CrossRef] [Green Version]
- Ridge, A.; Peterson, G.M.; Seidel, B.M.; Anderson, V.; Nash, R. Healthcare Providers’ Perceptions of Potentially Preventable Rural Hospitalisations: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 12767. [Google Scholar] [CrossRef] [PubMed]















Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gawlak, A.; Stankiewicz, M. Specific Needs of Patients and Staff Reflected in the Design of an Orthopaedic and Rehabilitation Hospital—Design Recommendations Based on a Case Study (Poland). Int. J. Environ. Res. Public Health 2022, 19, 15388. https://doi.org/10.3390/ijerph192215388
Gawlak A, Stankiewicz M. Specific Needs of Patients and Staff Reflected in the Design of an Orthopaedic and Rehabilitation Hospital—Design Recommendations Based on a Case Study (Poland). International Journal of Environmental Research and Public Health. 2022; 19(22):15388. https://doi.org/10.3390/ijerph192215388
Chicago/Turabian StyleGawlak, Agata, and Marta Stankiewicz. 2022. "Specific Needs of Patients and Staff Reflected in the Design of an Orthopaedic and Rehabilitation Hospital—Design Recommendations Based on a Case Study (Poland)" International Journal of Environmental Research and Public Health 19, no. 22: 15388. https://doi.org/10.3390/ijerph192215388