

Study Protocol of “Sustainably Healthy—From Science 2 Highschool & University”—Prevalence of Mixed, Vegetarian, and Vegan Diets Linked to Sports & Exercise among Austrian Tertiary Students and Lecturers/Academic Staff
 ,
,  , , , , and
, , , , and
Abstract
:1. Introduction
2. Objectives and Hypotheses
- The first and major goal of this college/university study is to survey the prevalence of omnivorous, vegetarian, and vegan diets linked to levels of sports & exercise;
- The second goal is to investigate the health-related behaviors of adults but particularly those of emerging adulthood (students) at tertiary educational entities;
- The third goal is to validate the self-reported data regarding lifestyle habits with a special focus on diet type and engagement in sports & exercise.
3. Materials and Methods
3.1. Study Design
3.2. Sample
3.3. Inclusion Criteria
3.4. Questionnaire
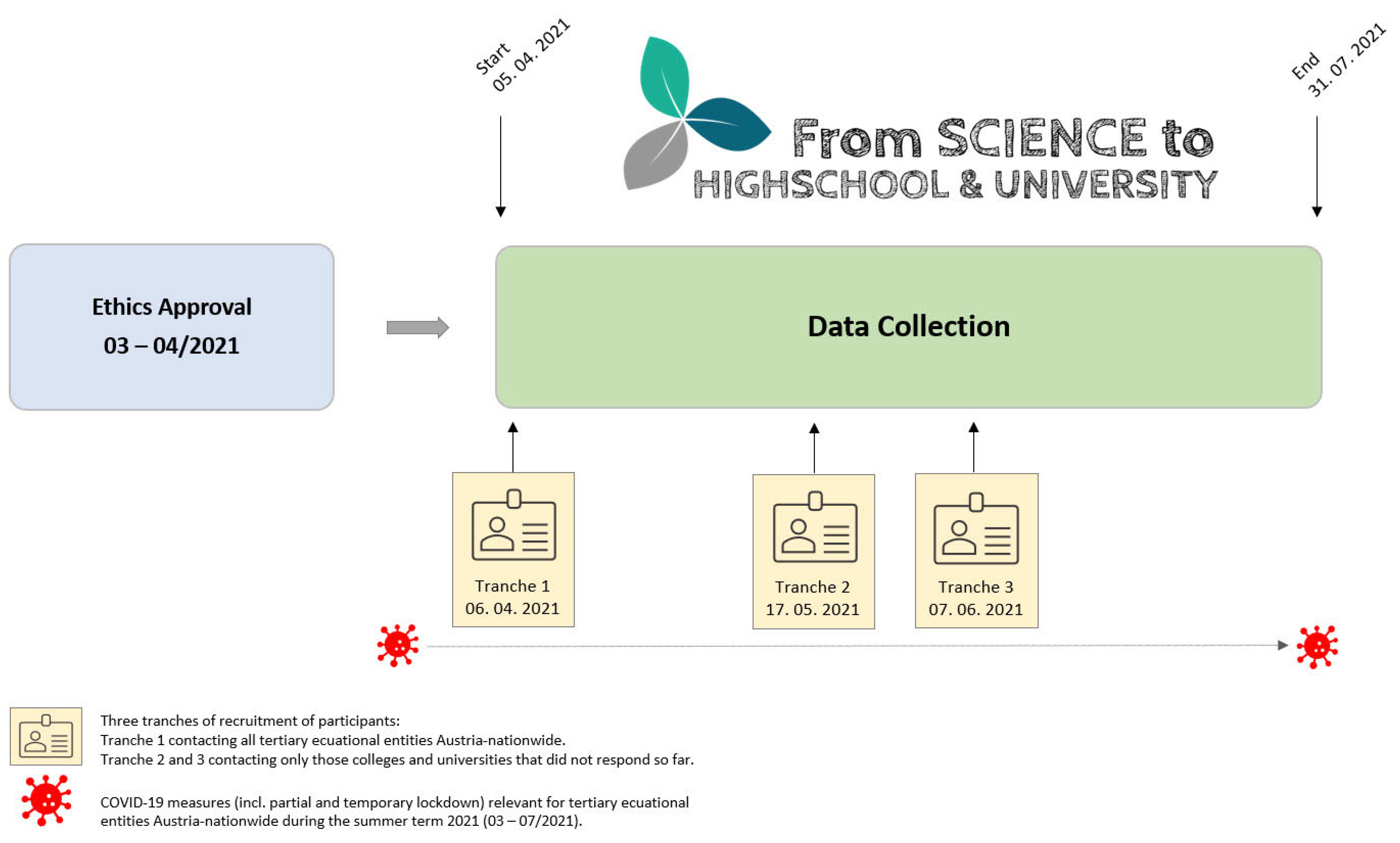
3.5. Procedure and Trial Status
3.6. Outcome Measures
3.6.1. Primary Outcome Measures
3.6.2. Further Outcome Measures
3.7. Ethical Principles
3.7.1. Written Informed Declaration of Consent and Publication
3.7.2. Vote of the Ethics Board of the main Tertiary Educational Entities
3.7.3. Duties on Part of the Investigators
3.7.4. Assessment of the Benefit–Risk Ratio
3.8. Data Security
3.9. Power Analysis, Calculation of Case Number Scenarios and Representativity
- (i)
- Students. For the estimation of a proportion of 15.1% (two sided 95%-CI) ± 2.5% accuracy, a sample size of n = 788 is required after data clearance;
- (ii)
- Lecturers/Academic Staff. For the estimation of a proportion of 9.45% (two sided 95%-CI) ± 2.5% accuracy, a sample size of n = 526 is required after data clearance.
3.10. Statistical Methods and Data Analysis
4. Discussion and Future Perspectives
4.1. Dual Approach of Health
4.2. Diet Type
4.3. The COVID-19 Pandemic and Health-Related Behaviors
4.4. Education and Health
4.5. Health at College/University Setting
4.6. Practical Implications
- The justification of the fundamental dual approach of “Healthy Eating, Active Living” [22,23] as a minimum recommendation for sustainable health, which—based on sound evidence—is considered a highly effective, safe, and low-cost strategy to promote the health of students and lecturers/academic staff in order to tackle individual and public health issues, and ultimately help improve health status and prevent NCDs;
- Encouraging policy and decision makers (e.g., federal authorities, stakeholders, board of deans, educational multipliers, and even families) to reflect, evaluate, and update the current health promotion offers, and to implement the dual approach to health in everyday scenarios and situations at tertiary educational settings and environments (e.g., curricula, sports & exercise opportunities, public catering of buffets, canteens, and cafeterias);
- Developing evidence-based and up-to-date health-related knowledge, skills, and competencies required for a sustainable health-orientated action readiness (regardless of socioeconomic background) through competence-oriented teaching to help achieve better individual health and develop professional health-related qualifications, particularly in emerging adulthood.
- Transfer the results to the public by first addressing the college/university settings, students (any discipline; not only limited to future teachers and doctors), and lecturers/academic staff as education professionals and health multipliers;
- Translate the findings into health-orientated actions and sustainable health-related action readiness (e.g., by recommending this safe, effective, and low-cost dual tool to policy and decision makers, multipliers, and experts in the health and education sector) by means of implementing this approach in tertiary teaching and training and everyday scenarios as a basic extension of the tertiary educational entity that is applicable for different populations (e.g., family, community, teachers, therapists, family/primary care and specialized physicians, dietitians, nutrition and sports experts, and educational supervisors/coaches);
- Apply the results most effectively in everyday college and university scenarios through creating and implementing further tertiary curricula-based competence-orientated education and training offers and raising awareness of state-of-the-art knowledge, skills, and competencies in order to (i) empower the peer group of tertiary students, and (ii) establish the basic dual approach for sustainable health as a minimum recommendation for health promotion in tertiary curricula as an educative, teaching, and research goal in line with the state mandate, thus seamlessly closing the gap between secondary and tertiary educational levels. By deliberately promoting the qualifications required to manage long-term individual health throughout (updated) tertiary level curricula, the evolution of programs and modules with regard to compulsory introductory and basic courses leading to advanced and in-depth courses and materials, especially for, but not limited to, future teachers and doctors, lecturers/academic staff, will ultimately aid to improve the future public health of nations.
4.7. Limitations and Strengths
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American College of Lifestyle Medicine. JAMA Physician Competencies for Prescribing Lifestyle Medicine. Definition. Evidence Overwhelmingly Supports Efficacy of Lifestyle Medicine. Lifestyle Medicine Research. Available online: https://lifestylemedicine.org/overview/ (accessed on 20 October 2022).
- Beaglehole, R.; Bonita, R.; Alleyne, G.; Horton, R.; Li, L.; Lincoln, P.; Mbanya, J.C.; McKee, M.; Moodie, R.; Nishtar, S.; et al. UN High-Level Meeting on Non-Communicable Diseases: Addressing four questions. Lancet 2011, 378, 449–455. [Google Scholar] [CrossRef]
- The World Health Organization. Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 20 October 2022).
- Mikkelsen, B.; Williams, J.; Rakovac, I.; Wickramasinghe, K.; Hennis, A.; Shin, H.R.; Farmer, M.; Weber, M.; Berdzuli, N.; Borges, C.; et al. Life course approach to prevention and control of non-communicable diseases. BMJ 2019, 364, l257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in body-mass index, underweight, overweight, and obesity from 1975 to 2016: A pooled analysis of 2416 population-based measurement studies in 128.9 million children, adolescents, and adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [Green Version]
- Inoue, Y.; Qin, B.; Poti, J.; Sokol, R.; Gordon-Larsen, P. Epidemiology of obesity in adults: Latest trends. Curr. Obes. Rep. 2018, 7, 276–288. [Google Scholar] [CrossRef]
- Ruiz, L.D.; Zuelch, M.L.; Dimitratos, S.M.; Scherr, R.E. Adolescent obesity: Diet quality, psychosocial health, and cardiometabolic risk factors. Nutrients 2019, 12, 43. [Google Scholar] [CrossRef] [Green Version]
- Hruby, A.; Manson, J.E.; Qi, L.; Malik, V.S.; Rimm, E.B.; Sun, Q.; Willett, W.C.; Hu, F.B. Determinants and consequences of obesity. Am. J. Public Health 2016, 106, 1656–1662. [Google Scholar] [CrossRef]
- Budreviciute, A.; Damiati, S.; Sabir, D.K.; Onder, K.; Schuller-Goetzburg, P.; Plakys, G.; Katileviciute, A.; Khoja, S.; Kodzius, R. Management and prevention strategies for non-communicable diseases (NCDs) and their risk factors. Front. Public Health 2020, 8, 574111. [Google Scholar] [CrossRef]
- Lee, I.M.; Shiroma, E.J.; Lobelo, F.; Puska, P.; Blair, S.N.; Katzmarzyk, P.T.; Lancet Physical Activity Series Working Group. Effect of physical inactivity on major non-communicable diseases worldwide: An analysis of burden of disease and life expectancy. Lancet 2012, 380, 219–229. [Google Scholar] [CrossRef] [Green Version]
- Willett, W.C. Balancing life-style and genomics research for disease prevention. Science 2002, 296, 695–698. [Google Scholar] [CrossRef]
- American College of Lifestyle Medicine (ACLM). Physician Competencies for Prescribing Lifestyle Medicine. Available online: https://www.lifestylemedicine.org/ (accessed on 20 October 2022).
- Ornish Lifestyle Medicine. The Proven Lifestyle—Simple Choices Yet Powerful Results. Available online: https://www.ornish.com/ (accessed on 20 October 2022).
- Thompson, W.R.; Sallis, R.; Joy, E.; Jaworski, C.A.; Stuhr, R.M.; Trilk, J.L. Exercise is medicine. Am. J. Lifestyle Med. 2020, 14, 511–523. [Google Scholar] [CrossRef]
- Vina, J.; Sanchis-Gomar, F.; Martinez-Bello, V.; Gomez-Cabrera, M.C. Exercise acts as a drug; the pharmacological benefits of exercise. Br. J. Pharmacol. 2012, 167, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Wiklund, P. The role of physical activity and exercise in obesity and weight management: Time for critical appraisal. J. Sport Health Sci. 2016, 5, 151–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruedl, G.; Greier, N.; Niedermeier, M.; Posch, M.; Prünster, V.; Faulhaber, M.; Burtscher, M. Factors associated with physical fitness among overweight and non-overweight austrian secondary school students. Int. J. Environ. Res. Public Health. 2019, 16, 4117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leech, R.M.; McNaughton, S.A.; Timperio, A. The clustering of diet, physical activity and sedentary behavior in children and adolescents: A review. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 4. [Google Scholar] [CrossRef] [Green Version]
- Wirnitzer, K.; Drenowatz, C.; Kirschner, W.; Tanous, D.; Rosemann, T. International Research & Knowledge Exchange for Addressing Today’s Global Health Paradox. Front. Public Health 2020, 10. [Google Scholar] [CrossRef]
- Motevalli, M.; Drenowatz, C.; Tanous, D.R.; Khan, N.A.; Wirnitzer, K. Management of Childhood Obesity—Time to Shift from Generalized to Personalized Intervention Strategies. Nutrients 2021, 13, 1200. [Google Scholar] [CrossRef]
- Sénéchal, M.; Slaght, J.; Bharti, N.; Bouchard, D.R. Independent and combined effect of diet and exercise in adults with prediabetes. Diabetes Metab. Syndr. Obes. 2014, 7, 521–529. [Google Scholar]
- Kaiser Permanente (KP). Healthy Eating Active Living (HEAL) Program Health Promotion, and Synopses. Available online: http://gken.org/Synopses/HP_10003.pdf (accessed on 12 September 2017).
- Tuso, P. Physician update: Total health. Perm. J. 2014, 18, 58–63. [Google Scholar] [CrossRef] [Green Version]
- Johns, D.J.; Hartmann-Boyce, J.; Jebb, S.A.; Aveyard, P.; Behavioural Weight Management Review Group. Diet or exercise interventions vs. combined behavioral weight management programs: A systematic review and meta-analysis of direct comparisons. J. Acad. Nutr. Diet. 2014, 114, 1557–1568. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.S.; Lee, J. Effects of combined exercise and low carbohydrate ketogenic diet interventions on waist circumference and triglycerides in overweight and obese individuals: A systematic review and meta-analysis. Int. J. Environ. Res. Public Health 2021, 18, 828. [Google Scholar] [CrossRef]
- Beigrezaei, S.; Yazdanpanah, Z.; Soltani, S.; Rajaie, S.H.; Mohseni-Takalloo, S.; Zohrabi, T.; Kaviani, M.; Forbes, S.C.; Baker, J.S.; Salehi-Abargouei, A. The effects of exercise and low-calorie diets compared with low-calorie diets alone on health: A protocol for systematic reviews and meta-analyses of controlled clinical trials. Syst. Rev. 2021, 10, 120. [Google Scholar] [CrossRef] [PubMed]
- Clark, J.E. Diet, exercise or diet with exercise: Comparing the effectiveness of treatment options for weight-loss and changes in fitness for adults (18–65 years old) who are overfat, or obese; systematic review and meta-analysis. J. Diabetes Metab. Disord. 2015, 14, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoo, S. Dynamic energy balance and obesity prevention. J. Obes. Metab. Syndr. 2018, 27, 203–212. [Google Scholar] [CrossRef] [PubMed]
- Drenowatz, C.; Greier, K. The role of energy flux in weight management. Exerc. Med. 2017, 1, 4. [Google Scholar] [CrossRef] [Green Version]
- Koliaki, C.; Spinos, T.; Spinou, Μ.; Brinia, Μ.E.; Mitsopoulou, D.; Katsilambros, N. Defining the optimal dietary approach for safe, effective and sustainable weight loss in overweight and obese adults. Healthcare 2018, 6, 73. [Google Scholar] [CrossRef] [Green Version]
- Hever, J.; Cronise, R.J. Plant-based nutrition for healthcare professionals: Implementing diet as a primary modality in the prevention and treatment of chronic disease. J. Geriatr. Cardiol. 2017, 14, 355–368. [Google Scholar]
- Wirnitzer, K.C. Vegan diet in sports and exercise—Health benefits and advantages to athletes and physically active people: A narrative review. Int. J. Sports Exerc. Med. 2020, 6, 165. [Google Scholar]
- Physicians Committee for Responsible Medicine (PCRM)—Plant-Based Diets. Available online: https://www.pcrm.org/good-nutrition/plant-based-diets#RecommendVegDiet (accessed on 20 October 2022).
- Barnard, N. Your Body in Balance. The New Science of Food, Hormones, and Health; Grand Central Publishing: New York, NY, USA, 2020. [Google Scholar]
- Kadoch, M.A. The power of nutrition as medicine. Prev. Med. 2012, 55, 80. [Google Scholar] [CrossRef]
- William, A. Medical Food. Warum Obst und Gemüse als Heilmittel Potenter Sind als Jedes Medikament; Arkana: Munich, Germany, 2017. [Google Scholar]
- Wang, D.D.; Li, Y.; Bhupathiraju, S.N.; Rosner, B.A.; Sun, Q.; Giovannucci, E.L.; Rimm, E.B.; Manson, J.E.; Willett, W.C.; Stampfer, M.J.; et al. Fruit and vegetable intake and mortality: Results from 2 prospective cohort studies of US men and women and a meta-analysis of 26 cohort studies. Circulation 2021, 143, 1642–1654. [Google Scholar] [CrossRef]
- Popper, P. Food over Medicine; Benbella Books: Dallas, TX, USA, 2013. [Google Scholar]
- de Faria Coelho-Ravagnani, C.; Corgosinho, F.C.; Sanches, F.F.Z.; Prado, C.M.M.; Laviano, A.; Mota, J.F. Dietary recommendations during the COVID-19 pandemic. Nutr. Rev. 2021, 79, 382–393. [Google Scholar] [CrossRef]
- The Centre for Evidence-Based Medicine. Available online: https://www.cebm.net/covid-19/what-explains-the-high-rate-of-SARS-CoV-2-transmission-in-meat-and-poultry-facilities-2/ (accessed on 20 October 2022).
- Greger, M. Primary pandemic prevention. Am. J. Lifestyle Med. 2021, 15, 498–505. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.; Rebholz, C.M.; Hegde, S.; LaFiura, C.; Raghavan, M.; Lloyd, J.F.; Cheng, S.; Seidelmann, S.B. Plant-based diets, pescatarian diets and COVID-19 severity: A population-based case–control study in six countries. BMJ Nutr. Prev. Health. 2021, 4, 257–266. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Food Nutrition Tips during Self-Quarantine. Available online: http://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/novel-coronavirus-2019 (accessed on 20 October 2022).
- Wirnitzer, K. Vegan Nutrition: Latest Boom in Health and Exercise. In Therapeutic, Probiotic, and Unconventional Foods; Grumezescu, A., Holban, A.M., Eds.; Elsevier: London, UK, 2018; Chapter 21; p. 411. [Google Scholar]
- Kamiński, M.; Skonieczna-Żydecka, K.; Nowak, J.K.; Stachowska, E. Global and local diet popularity rankings, their secular trends, and seasonal variation in Google Trends data. Nutrition 2020, 79, 110759. [Google Scholar] [CrossRef]
- Heinrich Böll Stiftung. Meat Atlas. 2021. Available online: https://eu.boell.org/en/MeatAtlas (accessed on 20 October 2022).
- Mensink, G.; Barbosa, C.L.; Brettschneider, A.K. Prevalence of persons following a vegetarian diet in Germany. J. Health Monit. 2016, 1, 1–13. [Google Scholar] [CrossRef]
- Bundesministerium für Ernährung und Landwirtschaft BMEL. Deutschland, Wie Es Isst—Der BMEL-Ernährungsreport. 2021. Available online: https://www.bmel.de/DE/themen/ernaehrung/ernaehrungsreport2021.html (accessed on 20 October 2022).
- Vegan Magazine. The Year of the Vegan. Where Millennials Lead, Business Governments Will Follow. 2019. Available online: https://www.vegan-magazine.com/2018/12/20/2019-the-year-of-the-vegan/ (accessed on 20 October 2022).
- Forbes. Millenials Are Driving the Worldwide Shirt Away from Meat. Available online: https://www.forbes.com/sites/michaelpellmanrowland/2018/03/23/millennials-move-away-from-meat/#618a21aa4a49 (accessed on 20 October 2022).
- Plant Based News. 30% of British Shoppers Aged 18–24 Are Vegan or Considering It. Available online: https://www.plantbasednews.org/culture/30-british-shoppers-18-24-vegan-considering (accessed on 20 October 2022).
- Plant Based News. Young People in UK Are ‘Ditching Meat in Record Numbers’. Available online: https://plantbasednews.org/news/young-people-uk-ditching-meat-record-numbers/ (accessed on 20 October 2022).
- Allianz Österreich. Available online: https://www.ots.at/presseaussendung/OTS_20201216_OTS0048/oesterreichs-lebensstil-in-der-corona-krise-jeder-zweite-lebt-zurzeit-bewusst-gesund (accessed on 20 October 2022).
- Bundesministerium für Ernährung und Landwirtschaft (BMEL). Deutschland, Wie Es Isst: Der BMEL-Ernährungsreport. 2021. Available online: https://www.bmel.de/SharedDocs/Downloads/DE/Broschueren/ernaehrungsreport-2021.pdf?__blob=publicationFile&v=5 (accessed on 28 December 2021).
- Alcorta, A.; Porta, A.; Tárrega, A.; Alvarez, M.D.; Vaquero, M.P. Foods for plant-based diets: Challenges and innovations. Foods 2021, 10, 293. [Google Scholar] [CrossRef] [PubMed]
- Barker, D.J.; Osmond, C.; Kajantie, E.; Eriksson, J.G. Growth and chronic disease: Findings in the Helsinki Birth Cohort. Ann. Hum. Biol. 2009, 36, 445–458. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Report of the Commission on Ending Childhood Obesity. Implementation Plan: Executive Summary. Available online: https://apps.who.int/iris/bitstream/handle/10665/259349/WHO-NMH-PNDECHO-17.1-eng.pdf (accessed on 20 October 2022).
- Arnett, J.J. Emerging adulthood. A theory of development from the late teens through the twenties. Am. Psychol. 2000, 55, 469–480. [Google Scholar] [CrossRef]
- Kwan, M.Y.; Cairney, J.; Faulkner, G.E.; Pullenayegum, E.E. Physical activity and other health-risk behaviors during the transition into early adulthood: A longitudinal cohort study. Am. J. Prev. Med. 2012, 42, 14–20. [Google Scholar] [CrossRef]
- Pinquart, M. 2.4.3. Junges und mittleres Erwachsenenalter. In Online Lehrbuch der Medizinischen Psychologie und Medizinischen Soziologie; Deinzer, R., von dem Knesebeck, O., Eds.; German Medical Science GMS Publishing House: Berlin, Germany, 2018. [Google Scholar]
- Sogari, G.; Velez-Argumedo, C.; Gómez, M.I.; Mora, C. College students and eating habits: A study using an ecological model for healthy behavior. Nutrients 2018, 10, 1823. [Google Scholar] [CrossRef] [Green Version]
- Whatnall, M.C.; Patterson, A.J.; Brookman, S.; Convery, P.; Swan, C.; Pease, S.; Hutchesson, M.J. Lifestyle behaviors and related health risk factors in a sample of Australian university students. J. Am. Coll. Health 2020, 68, 734–741. [Google Scholar] [CrossRef]
- Aceijas, C.; Waldhäusl, S.; Lambert, N.; Cassar, S.; Bello-Corassa, R. Determinants of health-related lifestyles among university students. Perspect. Public Health 2017, 137, 227–236. [Google Scholar] [CrossRef] [PubMed]
- Almutairi, K.M.; Alonazi, W.B.; Vinluan, J.M.; Almigbal, T.H.; Batais, M.A.; Alodhayani, A.A.; Alsadhan, N.; Tumala, R.B.; Moussa, M.; Aboshaiqah, A.E.; et al. Health promoting lifestyle of university students in Saudi Arabia: A cross-sectional assessment. BMC Public Health 2018, 18, 1093. [Google Scholar] [CrossRef] [PubMed]
- Romero-Blanco, C.; Rodríguez-Almagro, J.; Onieva-Zafra, M.D.; Parra-Fernández, M.L.; Prado-Laguna, M.D.C.; Hernández-Martínez, A. Physical activity and sedentary lifestyle in university students: Changes during confinement due to the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 6567. [Google Scholar] [CrossRef]
- Argiropoulou, M.I.; Sofianopoulou, A.; Kalantzi-Azizi, A. The Relation between General Procrastination and Health Behaviors: What Can We Learn from Greek Students? In Perspectives on Procrastination, Health, and Well-Being; Sirois, F.M., Pychyl, T.A., Eds.; Academic Press: Cambridge, MA, USA, 2016; pp. 143–160. [Google Scholar]
- Arnett, J.J. Emerging adulthood: Understanding the new way of coming of age. In Emerging Adults in America: Coming of Age in the 21st Century; Arnett, J.J., Tanner, J.L., Eds.; American Psychological Association: Washington, DC, USA, 2006; pp. 3–19. [Google Scholar]
- Independent Accountability Panel. The Health of Women, Children and Adolescents Is at the Heart of Transforming Our World: Empowering Accountability. Available online: https://iapewec.org/reports/iap-2021-final-report/ (accessed on 20 October 2022).
- United Nations. Sustainable Development Goals. Transforming Our World. The 2030 Agenda for Sustainable Development. Available online: https://sustainabledevelopment.un.org/post2015/transformingourworld (accessed on 20 October 2022).
- World Health Organization (WHO). Global Action Plan for the Prevention and Control of Non-Communicable Diseases: 2013–2020. Available online: https://www.who.int/publications/i/item/ncd-surveillance-global-monitoring-framework (accessed on 20 October 2022).
- United Nations Educational, Scientific and Cultural Organization. Education for Sustainable Development Goals. Learning Objectives. Available online: https://www.unesco.de/sites/default/files/2018-08/unesco_education_for_sustainable_development_goals.pdf (accessed on 20 October 2022).
- Wirnitzer, K.; Drenowatz, C.; Kirschner, W.; Tanous, D.; Rosemann, T. An integrative approach in addressing today’s global health crisis. In International Research & Knowledge Exchange for Addressing Today’s Global Health Paradox; Frontiers Event Abstracts: Lausanne, Switzerland, 2020; pp. 14–22. [Google Scholar]
- Metcalf, B.; Henley, W.; Wilkin, T. Effectiveness of intervention on physical activity of children: Systematic review and meta-analysis of controlled trials with objectively measured outcomes (EarlyBird 54). BMJ 2012, 345, e5888. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raghupathi, V.; Raghupathi, W. The influence of education on health: An empirical assessment of OECD countries for the period 1995–2015. Arch. Public Health 2020, 78, 20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oshio, T. Widening disparities in health between educational levels and their determinants in later life: Evidence from a nine-year cohort study. BMC Public Health 2018, 18, 278. [Google Scholar] [CrossRef] [Green Version]
- Zajacova, A.; Lawrence, E.M. The relationship between education and health: Reducing disparities through a contextual approach. Annu. Rev. Public Health 2018, 39, 273–289. [Google Scholar] [CrossRef] [Green Version]
- De Bourdeaudhuij, I.; Van Cauwenberghe, E.; Spittaels, H.; Oppert, J.M.; Rostami, C.; Brug, J.; Van Lenthe, F.; Lobstein, T.; Maes, L. School-based interventions promoting both physical activity and healthy eating in Europe: A systematic review within the HOPE project. Obes. Rev. 2011, 12, 205–216. [Google Scholar] [CrossRef]
- García-Hermoso, A.; Alonso-Martínez, A.M.; Ramírez-Vélez, R.; Pérez-Sousa, M.Á.; Ramírez-Campillo, R.; Izquierdo, M. Association of physical education withimprovement of health-related physical fitness outcomes and fundamental motor skills among youths: A systematic review and meta-analysis. JAMA Pediatr. 2020, 174, e200223. [Google Scholar] [CrossRef]
- The Institute of Development Studies. The Impact of School Health Programmes. Available online: https://opendocs.ids.ac.uk/opendocs/handle/20.500.12413/13185 (accessed on 20 October 2022).
- Yuksel, H.S.; Sahin, F.N.; Maksimovic, N.; Drid, P.; Bianco, A. School-based intervention programs for preventing obesity and promoting physical activity and fitness: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 347. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization WHO-HBSC-Survey. Gesundheit und Gesundheitsverhalten von Österreichischen Schülerinnen und Schülern. Available online: https://images.derstandard.at/2019/07/11/HBSC-Studie.pdf (accessed on 20 October 2022).
- WHO Regional Office for Europe. Health Policy for Children and Adolescents (No. 6). Available online: https://www.euro.who.int/__data/assets/pdf_file/0007/167281/E96444_part1.pdf (accessed on 20 October 2022).
- WHO Regional Office for Europe. Nutrition, Physical Activity and Obesity in Austria. Available online: https://www.euro.who.int/__data/assets/pdf_file/0006/243285/Austria-WHO-Country-Profile.pdf?ua=1 (accessed on 20 October 2022).
- EXPORT.GOV. Healthcare Resource Guide: Austria. Available online: https://2016.export.gov/industry/health/healthcareresourceguide/eg_main_108562.asp (accessed on 20 October 2022).
- Bundesministerium für Gesundheit. Österreichischer Kinder—Und Jugendgesundheitsbericht. 2016. Available online: https://jasmin.goeg.at/94/1/%C3%96sterreichischer%20Kinder-%20und%20Jugendgesundheitsbericht.pdf (accessed on 20 October 2022).
- Großschädl, F.; Stronegger, W.J. Regional trends in obesity and overweight among Austrian adults between 1973 and 2007. Wien. Klin. Wochenschr. 2012, 124, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Österreichsicher Ernährungsbericht. 2017. Available online: https://broschuerenservice.sozialministerium.at/Home/Download?publicationId=528 (accessed on 20 October 2022).
- World Health Organization (WHO). Austria—Physical Activity Factsheet. 2018. Available online: https://www.euro.who.int/__data/assets/pdf_file/0007/288052/AUSTRIA-Physical-Activity-Factsheet.pdf (accessed on 20 October 2022).
- Statistik Austria. Körperliche Aktivität in der Freizeit, Körperliche Aktivität. 2014. Available online: https://www.statistik.at/fileadmin/publications/OEsterreichische_Gesundheitsbefragung_2014.pdf (accessed on 20 October 2022).
- Berichtszeitraum. Gesundheitsbericht über Die Bevölkerung im Mittleren Alter. Wien: Bundesministerium für Arbeit, Soziales, Gesundheit und Konsumentenschutz, Wien. Available online: https://jasmin.goeg.at/1558/1/Gesundheitsbericht-mittleres-Alter.pdf (accessed on 20 October 2022).
- STATISTA. Statistiken zu Vegetarismus und Veganismus in Österreich. Available online: https://de.statista.com/themen/3804/vegetarismus-und-veganismus-in-oesterreich/ (accessed on 20 October 2022).
- Zachary, Z.; Brianna, F.; Brianna, L.; Garrett, P.; Jade, W.; Alyssa, D.; Mikayla, K. Self-quarantine and weight gain related risk factors during the COVID-19 pandemic. Obes. Res. Clin. Pract. 2020, 14, 210–216. [Google Scholar] [CrossRef] [PubMed]
- Keng, S.L.; Stanton, M.V.; Haskins, L.B.; Almenara, C.A.; Ickovics, J.; Jones, A.; Grigsby-Toussaint, D.; Agostini, M.; Bélanger, J.J.; Gützkow, B.; et al. COVID-19 stressors and health behaviors: A multilevel longitudinal study across 86 countries. Prev. Med. Rep. 2022, 27, 101764. [Google Scholar] [CrossRef] [PubMed]
- Wilke, J.; Mohr, L.; Tenforde, A.S.; Edouard, P.; Fossati, C.; González-Gross, M.; Sánchez Ramírez, C.; Laiño, F.; Tan, B.; Pillay, J.D.; et al. A Pandemic within the pandemic? physical activity levels substantially decreased in countries affected by COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 2235. [Google Scholar] [CrossRef]
- Vaillant, L.; La Ruche, G.; Tarantola, A.; Barboza, P. Epidemic intelligence team at in vs epidemiology of fatal cases associated with pandemic H1N1 influenza 2009. Eurosurveillance 2009, 14, 19309. [Google Scholar] [CrossRef] [Green Version]
- Khan, A.S.; Hichami, A.; Khan, N.A. Obesity and COVID-19: Oro-Naso-Sensory Perception. J. Clin. Med. 2020, 9, 2158. [Google Scholar] [CrossRef]
- Wirnitzer, K.C.; Tanous, D.R.; Motevalli, M.; Göbel, G.; Wirnitzer, G.; Drenowatz, C.; Ruedl, G.; Cocca, A.; Kirschner, W. Study protocol of “From Science 2 School”—Prevalence of sports and physical exercise linked to omnivorous, vegetarian and vegan, diets among Austrian secondary schools. Front. Sports Act. Living 2022, 4, 967915. [Google Scholar] [CrossRef]
- Wirnitzer, K.C.; Drenowatz, C.; Cocca, A.; Tanous, D.R.; Motevalli, M.; Wirnitzer, G.; Schätzer, M.; Ruedl, G.; Kirschner, W. Health Behaviors of Austrian Secondary Level Pupils at a Glance: First Results of the From Science 2 School Study Focusing on Sports Linked to Mixed, Vegetarian, and Vegan Diets. Int. J. Environ. Res. Public Health 2021, 18, 12782. [Google Scholar] [CrossRef]
- Wirnitzer, K.C.; Drenowatz, C.; Cocca, A.; Tanous, D.R.; Motevalli, M.; Wirnitzer, G.; Schätzer, M.; Ruedl, G.; Kirschner, W. Health Behaviors of Austrian Secondary School Teachers and Principals at a Glance: First Results of the From Science 2 School Study Focusing on Sports Linked to Mixed, Vegetarian, and Vegan Diets. Nutrients 2022, 14, 1065. [Google Scholar] [CrossRef]
- Jakše, B.; Jakše, B.; Godnov, U.; Pinter, S. Nutritional, cardiovascular health and lifestyle status of ‘health conscious’ adult vegans and non-vegans from Slovenia: A cross-sectional self-reported survey. Int. J. Environ. Res. Public Health 2021, 18, 5968. [Google Scholar] [CrossRef]
- Bedford, J.L.; Barr, S.I. Diets and selected lifestyle practices of self-defined adult vegetarians from a population-based sample suggest they are more ‘health conscious’. Int. J. Behav. Nutr. Phys. Act. 2005, 2, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leitzmann, C.; Keller, M. Vegetarische und Vegane Ernährung. 4. Vollständig Überarbeitete und Erweiterte Auflage; UTB: Stuttgart, Germany, 2020. [Google Scholar]
- World Health Organization. WHOQOL-BREF. Available online: https://www.who.int/toolkits/whoqol/whoqol-bref (accessed on 20 October 2022).
- WHO Regional Office for Europe. Body Mass Index—BMI. Available online: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 20 October 2022).
- Word Health Organization (WHO). Global Health Observatory (GHO) Data. Mean Body Mass Index (BMI). Situation and Trends. Available online: http://www.who.int/gho/ncd/risk_factors/bmi_text/en/ (accessed on 20 October 2022).
- Felder-Puig, R.; Ramelow, D.; Maier, G.; Teutsch, F. Ergebnisse der WieNGS Lehrer/innen-Befragung 2017; Institut für Gesundheitsförderung und Prävention, WIENGS-Forschungsbericht: Wien, Austria, 2017; pp. 15–16. [Google Scholar]
- Hofmann, F.; Griebler, R.; Ramelow, D.; Unterweger, K.; Griebler, U.; Felder-Puig, R.; Dür, W. Gesundheit und Gesundheitsverhalten von Österreichs Lehrer/Innen: Ergebnisse der Lehrer/Innen-Befragung 2010; LBIHPR Forschungsbericht: Wien, Austria, 2012; pp. 19–20. [Google Scholar]
- Xu, F.; Cohen, S.A.; Lofgren, I.E.; Greene, G.W.; Delmonico, M.J.; Greaney, M.L. Relationship between diet quality, physical activity and health-related quality of life in older adults: Findings from 2007–2014 National Health and Nutrition Examination Survey. J. Nutr. Health Aging 2018, 22, 1072–1079. [Google Scholar] [CrossRef] [Green Version]
- Markland, D.; Hardy, L. The exercise motivations inventory: Preliminary development and validity of a measure of individuals’ reasons for participation in regular physical exercise. Pers. Individ. Differ. 1993, 15, 289–296. [Google Scholar] [CrossRef]
- Schmid, J.; Molinari, V.; Lehnert, K.; Sudeck, G.; Conzelmann, A. BMZI-HEA. Adaption des Berner Motiv—Und Zielinventars im Freizeit—Und Gesundheitssport für Menschen im höheren Erwachsenenalter. Z. Für Gesundh. 2014, 22, 104–117. [Google Scholar] [CrossRef]
- Melina, V.; Craig, W.; Levin, S.; Academy of Nutrition and Dietetics (AND). Position of the Academy of Nutrition and Dietetics: Vegetarian Diets. J. Acad. Nutr. Diet 2016, 115, 1970–1980. [Google Scholar] [CrossRef] [PubMed]
- Cullum-Dugan, D.; Pawlak, R.; Academy of Nutrition and Dietetics (AND). Position of the academy of nutrition and dietetics: Vegetarian diets. J. Acad. Nutr. Diet 2015, 115, 801–810. [Google Scholar] [CrossRef]
- Hall, J.N.; Moore, S.; Harper, S.B.; Lynch, J.W. Global variability in fruit and vegetable consumption. Am. J. Prev. Med. 2009, 36, 402–409. [Google Scholar] [CrossRef]
- Österreichische Gesellschaft für Ernährung (ÖGE). Available online: https://www.oege.at/index.php/bildung-information/empfehlungen (accessed on 20 October 2022).
- Haftenberger, M.; Heuer, T.; Heidemann, C.; Kube, F.; Krems, C.; Mensink, G.B. Relative validation of a food frequency questionnaire for national health and nutrition monitoring. Nutr. J. 2010, 9, 36. [Google Scholar] [CrossRef] [Green Version]
- Schüpbach, R.; Wegmüller, R.; Berguerand, C.; Bui, M.; Herter-Aeberli, I. Micronutrient status and intake in omnivores, vegetarians and vegans in Switzerland. Eur. J. Nutr. 2017, 56, 283–293. [Google Scholar] [CrossRef]
- Leitzmann, C. Veganismus. Grundlagen, Vorteile, Risiken; Verlag C H Beck: Munich, Germany, 2018. [Google Scholar]
- Wirnitzer, K.; Seyfart, T.; Leitzmann, C.; Keller, M.; Wirnitzer, G.; Lechleitner, C.; Rüst, C.A.; Rosemann, T.; Knechtle, B. Prevalence in running events and running performance of endurance runners following a vegetarian or vegan diet compared to non-vegetarian endurance runners: The NURMI Study. Springer Plus 2016, 5, 458. [Google Scholar] [CrossRef] [Green Version]
- Neuhauser, H.; Schienkiewitz, A.; Schaffrath-Rosario, A.; Dortschy, R.; Kurth, B.M. Beiträge zur Gesundheitsberichterstattung des Bundes. Referenzperzentile für Anthropometrische Maßzahlen und Blutdruck aus der Studie zur Gesundheit von Kindern und Jugendlichen in Deutschland (KiGGS); Robert-Koch Institut: Berlin, Germany, 2013. [Google Scholar]
- Ramelow, D.; Teutsch, F.; Hofmann, F.; Felder-Puig, R. Ludwig Boltzmann Institut Health Promotion Research. Gesundheit und Gesundheitsverhalten von Österreichischen Schülern und Schülerinnen. Ergebnisse des WHO-HBSC-Survey (2014); Bundesministerium für Gesundheit: Wien, Austria, 2015. [Google Scholar]
- Dijkstra, T.K. On statistical inference with parameter estimates on the boundary of the parameter space. Br. J. Math. Stat. Psychol. 1992, 45, 289–309. [Google Scholar] [CrossRef]
- Kim, S.H.; Cho, D. Validation of exercise motivations inventory—2 (EMI-2) scale for college students. J. Am. Coll. Health 2022, 70, 114–121. [Google Scholar] [CrossRef] [PubMed]
- Markland, D.; Ingledew, D.K. The measurement of exercise motives: Factorial validity and invariance across gender of a revised exercise motivations inventory. Br. J. Health Psychol. 1997, 2, 361–376. [Google Scholar] [CrossRef]
- Gesundheit Österreich Forschungs. Kinder—Und Jugendgesundheit in Niederösterreich. Available online: https://www.noe.gv.at/noe/Gesundheitsvorsorge-Forschung/Kinder-_und_Jugendgesundheit_in_NOE.pdf (accessed on 20 October 2022).
- Leitzmann, C.; Keller, M. Vegetarische Ernährung. 3 Aktualisierte Auflage Edn; UTB: Stuttgart, Germany, 2013. [Google Scholar]
- Prifysgol Bangor University. EMI-2 in German. Available online: http://exercise-motivation.bangor.ac.uk/emi/german.php (accessed on 20 October 2022).
- Hu, L.T.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Struct. Equ. Model. 1999, 6, 1–55. [Google Scholar] [CrossRef]
- Smith, J.D.; Fu, E.; Kobayashi, M.A. Prevention and management of childhood obesity and its psychological and health comorbidities. Annu. Rev. Clin. Psychol. 2020, 16, 351–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Euractiv Special Report. Physical Inactivity Costs Estimated at €80 bn per Year. Available online: https://www.euractiv.com/section/sports/news/physical-inactivity-costs-estimated-at-80bn-per-year/ (accessed on 20 October 2022).
- Tuso, P.; Huynh, D.N.; Garofalo, L.; Lindsay, G.; Watson, H.L.; Lenaburg, D.L.; Lau, H.; Florence, B.; Jones, J.; Harvey, P.; et al. The readmission reduction program of Kaiser Permanente Southern California-knowledge transfer and performance improvement. Perm. J. 2013, 17, 58–63. [Google Scholar] [CrossRef] [Green Version]
- Tuso, P. Behavior medicine specialist. Perm. J. 2014, 18, 52–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlson, A.; Frazão, E. Food costs, diet quality and energy balance in the United States. Physiol. Behav. 2014, 134, 20–31. [Google Scholar] [CrossRef]
- Flynn, M.; Schiff, A. Economical healthy diets: Including lean animal protein costs more than using extra virgin olive oil. J. Hunger. Und Environ. Nutr. 2012, 10, 467–482. [Google Scholar] [CrossRef]
- Tuso, P.; Ismail, M.; Ha, B.; Bartolotto, C. Nutritional update for physicians: Plant-based diets. Perm. J. 2013, 17, 61–66. [Google Scholar] [CrossRef] [Green Version]
- Barnard, N.D.; Goldman, D.M.; Loomis, J.F.; Kahleova, H.; Levin, S.M.; Neabore, S.; Batts, T.C. Plant-Based diets for cardiovascular safety and performance in endurance sports. Nutrients 2019, 11, 130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim. H.; Caulfield, L.E.; Garcia-Larsen, V.; Steffen, L.M.; Coresh, J.; Rebholz, C.M. Plant-Based diets are associated with a lower risk of incident cardiovascular disease, cardiovascular disease mortality, and all-cause mortality in a general population of middle-aged adults. J. Am. Heart Assoc. 2019, 8, e012865. [Google Scholar]
- Nutrition Facts. How Not to Die: Discover the Foods Scientifically Proven to Prevent and Reverse Disease. Available online: https://nutritionfacts.org/book/how-not-to-die/ (accessed on 20 October 2022).
- Li, D. Effect of the vegetarian diet on non-communicable diseases. J. Sci. Food Agric. 2014, 94, 169–173. [Google Scholar] [CrossRef]
- Barnard, N.; Kahleova, H.; Levin, S.M. The use of plant-based diets for obesity treatment. Int. J. Dis. Reversal. Prev. 2019, 1, 12. [Google Scholar] [CrossRef]
- Mishra, S.; Xu, J.; Agarwal, U.; Gonzales, J.; Levin, S.; Barnard, N.D. A multicenter randomized controlled trial of a plant-based nutrition program to reduce body weight and cardiovascular risk in the corporate setting: The GEICO study. Eur. J. Clin. Nutr. 2013, 67, 718–724. [Google Scholar] [CrossRef] [Green Version]
- Benatar, J.R.; Stewart, R. Cardiometabolic risk factors in vegans: A meta-analysis of observational studies. PLoS ONE 2018, 13, e0209086. [Google Scholar] [CrossRef] [Green Version]
- Keaver, L.; Ruan, M.; Chen, F.; Du, M.; Ding, C.; Wang, J.; Shan, Z.; Liu, J.; Zhang, F.F. Plant- and animal-based diet quality and mortality among US adults: A cohort study. Br. J. Nutr. 2021, 125, 1405–1415. [Google Scholar] [CrossRef]
- Neufingerl, N.; Eilander, A. nutrient intake and status in adults consuming plant-based diets compared to meat-eaters: A systematic review. Nutrients 2021, 14, 29. [Google Scholar] [CrossRef]
- Peretti, N.; Darmaun, D.; Chouraqui, J.P.; Bocquet, A.; Briend, A.; Feillet, F.; Frelut, M.L.; Guimber, D.; Hankard, R.; Lapillonne, A.; et al. Vegetarian diet in children and adolescents: A health benefit? Arch. Pediatr. 2020, 27, 173–175. [Google Scholar] [CrossRef]
- Waldmann, A.; Koschizke, J.W.; Leitzmann, C.; Hahn, A. Dietary intakes and lifestyle factors of a vegan population in Germany: Results from the German Vegan Study. Eur. J. Clin. Nutr. 2003, 57, 947–955. [Google Scholar] [CrossRef] [Green Version]
- Deckers, J. Animal (De) Liberation: Should the Consumption of Animal Products Be Banned? Might a Vegan Diet Be Healthy, or Even Healthier? Available online: https://www.ncbi.nlm.nih.gov/books/NBK396513/ (accessed on 20 October 2022).
- Shenkin, A. Micronutrients in health and disease. Postgrad. Med. J. 2006, 82, 559–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cena, H.; Calder, P.C. Defining a healthy diet: Evidence for the role of contemporary dietary patterns in health and disease. Nutrients 2020, 12, 334. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neuhouser, M.L. The importance of healthy dietary patterns in chronic disease prevention. Nutr. Res. 2019, 70, 3–6. [Google Scholar] [CrossRef] [PubMed]
- Kenney, E.L.; Long, M.W.; Cradock, A.L.; Gortmaker, S.L. Prevalence of inadequate hydration among US children and disparities by gender and race/ethnicity: National health and nutrition examination survey, 2009–2012. Am. J. Public Health 2015, 105, 113–118. [Google Scholar] [CrossRef]
- Albert Schweitzer Stiftung. Portugal: Vegane Speisen Sind in Kantinen Pflicht. Available online: https://albert-schweitzer-stiftung.de/aktuell/portugal-vegane-speisen-inkantinen-pflicht (accessed on 20 October 2022).
- American Medical Association (AMA). House of Delegates Healthful Hospitals. Reference Committee D. Resolution 406 (A-17). pp. 5–37. District of Columbia. Annual Conference, Chicago. Available online: https://www.ama-assn.org/sites/default/files/mediabrowser/public/yps/a17-yps-d-final-grid.pdf (accessed on 20 October 2022).
- American Medical Association (AMA). House of Delegates Healthful Hospitals. Reference Committee D. Resolution 406 (A-17). pp. 5–37. District of Columbia. Annual Conference, Chicago. Available online: https://www.amaassn.org/sites/default/files/media-browser/public/hod/a17-refcomm-d.pdf (accessed on 20 October 2022).
- Azzouzi, S.; Stratton, C.; Muñoz-Velasco, L.P.; Wang, K.; Fourtassi, M.; Hong, B.Y.; Cooper, R.; Balikuddembe, J.K.; Palomba, A.; Peterson, M.; et al. The impact of the COVID-19 pandemic on healthy lifestyle behaviors and perceived mental and physical health of people living with non-communicable diseases: An international cross-sectional survey. Int. J. Environ. Res. Public Health 2022, 19, 8023. [Google Scholar] [CrossRef]
- Tan, M.; He, F.J.; MacGregor, G.A. Obesity and COVID-19: The role of the food industry. BMJ 2020, 369, m2237. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Food and Nutrition Tips during Self-Quarantine. Available online: http://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/novel-coronavirus-2019-ncov-technical-guidance-OLD/food-and-nutrition-tips-during-self-quarantine (accessed on 20 October 2022).
- World Health Organization (WHO). Stay Physically Active during Self-Quarantine. Available online: http://www.euro.who.int/en/health-topics/health-emergencies/coronavirus-covid-19/novel-coronavirus-2019-ncov-technical-guidance-OLD/stay-physically-active-during-self-quarantine (accessed on 20 October 2022).
- Laaksonen, M.; Talala, K.; Martelin, T.; Rahkonen, O.; Roos, E.; Helakorpi, S.; Laatikainen, T.; Prättälä, R. Health behaviours as explanations for educational level differences in cardiovascular and all-cause mortality: A follow-up of 60,000 men and women over 23 years. Eur. J. Public Health 2008, 18, 38–43. [Google Scholar] [CrossRef] [Green Version]
- Hofer-Fischanger, K.; Fuchs-Neuhold, B.; Müller, A.; Grasser, G.; van Poppel, M.N.M. Health literacy and active transport in Austria: Results from a rural setting. Int. J. Environ. Res. Public Health 2020, 17, 1404. [Google Scholar] [CrossRef] [Green Version]
- Global Health Data Exchange (GHDx). Global Burden of Disease Study 2019 (GBD 2019) Data Resources. Available online: https://ghdx.healthdata.org/gbd-2019 (accessed on 20 October 2022).
- Besnier, E.; Thomson, K.; Stonkute, D.; Mohammad, T.; Akhter, N.; Todd, A.; Jensen, M.R.; Klivik, A.; Bambra, C. Which public health interventions are effective in reducing morbidity, mortality and health inequalities from infectious diseases amongst children in low- and middle-income countries (LMICs): An umbrella review. PLoS ONE 2021, 16, e0251905. [Google Scholar] [CrossRef]
- Telama, R. Tracking of physical activity from childhood to adulthood: A review. Obes. Facts. 2009, 2, 187–195. [Google Scholar] [CrossRef]
- Gries, K.J.; Raue, U.; Perkins, R.K.; Lavin, K.M.; Overstreet, B.S.; D’Acquisto, L.J.; Graham, B.; Finch, W.H.; Kaminsky, L.A.; Trappe, T.A.; et al. Cardiovascular and skeletal muscle health with lifelong exercise. J. Appl. Physiol. 2018, 125, 1636–1645. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arnett, J.J. Emerging Adulthood: The Winding Road from the Late Teens through the Twenties, 2nd ed.; Oxford University Press: New York, NY, USA, 2015. [Google Scholar]
- Cheung, P. Teachers as role models for physical activity: Are preschool children more active when their teachers are active? Eur. Phys. Educ. Rev. 2020, 26, 101–110. [Google Scholar] [CrossRef]
- Wong, L.S.; Gibson, A.M.; Farooq, A.; Reilly, J.J. Interventions to increase moderate-to-vigorous physical activity in elementary school physical education lessons: Systematic review. J. Sch. Health 2021, 91, 836–845. [Google Scholar] [CrossRef] [PubMed]
- Scheuch, K.; Haufe, E.; Seibt, R. Teachers’ health. Dtsch. Arztebl. Int. 2015, 112, 347–356. [Google Scholar] [CrossRef]
- Ulich, K. Beruf Lehrer/in. Arbeitsbelastungen, Beziehungskonflikte, Zufriedenheit; Weinheim und Basel: Beltz, Australia, 1996. [Google Scholar]
- Nieskens, B.; Rupprecht, S.; Erbring, S. Was Hält Lehrkräfte Gesund? Ergebnisse der Gesundheitsforschung für Lehrkräfte und Schulen. In Handbuch Lehrergesundheit Impulse für Die Entwicklung Guter Gesunder Schulen; Eine Veröffentlichung der DAK-Gesundheit und der Unfallkasse Nordrhein-Westfalen; Carl Link (Wolters Kuiwer): Köln, Germany, 2012; pp. 31–96. [Google Scholar]
- Stafford, F.; Chiteji. N. Shaping health behavior across generations: Evidence from time use data in the panel study of income dynamics and its supplements. Ann. Econ. Stat. 2012, 105, 185–208. [Google Scholar] [CrossRef] [Green Version]
- Lehrplan AHS. Unterstufe (Sekundarstufe I). 2021. Available online: https://www.bmbwf.gv.at/Themen/schule/schulpraxis/lp/lp_ahs.html (accessed on 20 October 2022).
- Lehrplan AHS Unterstufe (Sekundarstufe I). 2021. Available online: https://www.ris.bka.gv.at/GeltendeFassung.wxe?Abfrage=Bundesnormen&Gesetzesnummer=10008568 (accessed on 20 October 2022).
- Lehrplan AHS Oberstufe (Sekundarstufe II). 2018. Available online: https://www.bmbwf.gv.at/Themen/schule/schulpraxis/lp/lp_ahs.html (accessed on 20 October 2022).
- Lehrplan AHS Oberstufe (Sekundarstufe II). 2021. Available online: https://www.ris.bka.gv.at/GeltendeFassung.wxe?Abfrage=Bundesnormen&Gesetzesnummer=10008568 (accessed on 20 October 2022).
- Lehrplan der Neuen Mittelschule. 2018. Available online: https://www.ris.bka.gv.at/Dokumente/Bundesnormen/NOR40199276/NOR40199276.pdf (accessed on 20 October 2022).
- European Commission—State of Health in the EU. Available online: https://ec.europa.eu/commission/presscorner/detail/en/IP_19_6336 (accessed on 20 October 2022).
- BMUK—Grundsatzerlass Gesundheitserziehung. Available online: https://schularzt.at/fileadmin/user_upload/Grundsatzerlass_Gesundheitserziehung_1997.pdf (accessed on 20 October 2022).
- Morton, K.F.; Pantalos, D.C.; Ziegler, C.; Patel, P.D. A place for plant-based nutrition in us medical school curriculum: A survey-based study. Am. J. Lifestyle Med. 2021, 16, 271–283. [Google Scholar] [CrossRef]
- Havermans, R.C.; Rutten, G.; Bartelet, D. Adolescent’s willingness to adopt a more plant-based diet: A theory-based interview study. Front. Nutr. 2021, 8, 688131. [Google Scholar] [CrossRef]
- Kudelka, P.; Hnat, F.; Müller-Amenitsch, R. Vegan im Recht. Das Handbuch für Juristische Fragen des Veganen Lebensstils. Österreich Edition. Kapitel 3.1—Veganes Essen in der Schule; Vegane Gesellschaft Österreich: Wien, Austria, 2017. [Google Scholar]
- World Health Organization (WHO). School Policy Framework: Implementation of the WHO Global Strategy on Diet, Physical Activity and Health. Available online: https://apps.who.int/iris/handle/10665/43923 (accessed on 20 October 2022).
- McIver, J.P.; Carmines, E.G. Unidimensional Scaling. Quantitative Applications in the Social Sciences; Sage Publications: Beverly Hills, Australia, 1981. [Google Scholar] [CrossRef]
- Hoeppner, B.B.; Kelly, J.F.; Urbanoski, K.A.; Slaymaker, V. Comparative utility of a single-item versus multiple-item measure of self-efficacy in predicting relapse among young adults. J. Subst. Abuse. Treat. 2011, 41, 305–312. [Google Scholar] [CrossRef] [Green Version]
- Cocca, A.; Niedermeier, M.; Prünster, V.; Wirnitzer, K.; Drenowatz, C.; Greier, K.; Labek, K.; Ruedl, G. Self-Rated health status of upper secondary school pupils and its associations with multiple health-related factors. Int. J. Environ. Res. Public Health 2022, 19, 6947. [Google Scholar] [CrossRef]
- Carreras, M.; Puig, G.; Sánchez-Pérez, I.; Inoriza, J.M.; Coderch, J.; Gispert, R. Morbidity and self-perception of health, two different approaches to health status. Gac. Sanit. 2020, 34, 601–607. [Google Scholar] [CrossRef]
- Rolstad, S.; Adler, J.; Ryden, A. Response burden and questionnaire length: Is shorter better? A review and meta-analysis. Value Health 2011, 14, 1101–1108. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Mensink et al. (2016) [47] German Norm Population (18–69 Years) | Wirnitzer et al. (2021) [98] Austrian Secondary Level Pupils (10–19 Years) | Wirnitzer et al. (2022) [99] Austrian Secondary Teachers/Principals (20–65 Years) | |
|---|---|---|---|
| Confidence level | 95% | 95% | 95% |
| Alternative Hypothesis | 2-sided interval | 2-sided interval | 2-sided interval |
| Expected proportion (%) | 6.5% | 15.1% | 9.45% |
| Margin of Error (ME; distance from proportion to limit) | 2.5% | 2.5% | 2.5% |
| Power (accepted min. 80%) | 96% (0.96) | 91% (0.91) | 100% (0.1) |
| Number per cell per stratum | 374 | 788 | 526 |
| df (n) | Effect Size (w) | Level of Significance | Power | N (Total) | |
|---|---|---|---|---|---|
| Students [diet] | 2 | 0.12 | 0.05 | 0.8 | 694 |
| [diet] * [age * sex] | 6 | 0.10 | 0.05 | 0.8 | 1363 |
| [diet] * [age * sex * field of study] | 14 | 0.10 | 0.05 | 0.8 | 1834 |
| Lecturers/Academic Staff [diet] | 2 | 0.13 | 0.05 | 0.8 | 573 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wirnitzer, K.C.; Motevalli, M.; Tanous, D.R.; Wirnitzer, G.; Wagner, K.-H.; Cocca, A.; Schätzer, M.; Kirschner, W.; Drenowatz, C.; Ruedl, G. Study Protocol of “Sustainably Healthy—From Science 2 Highschool & University”—Prevalence of Mixed, Vegetarian, and Vegan Diets Linked to Sports & Exercise among Austrian Tertiary Students and Lecturers/Academic Staff. Int. J. Environ. Res. Public Health 2022, 19, 15313. https://doi.org/10.3390/ijerph192215313
Wirnitzer KC, Motevalli M, Tanous DR, Wirnitzer G, Wagner K-H, Cocca A, Schätzer M, Kirschner W, Drenowatz C, Ruedl G. Study Protocol of “Sustainably Healthy—From Science 2 Highschool & University”—Prevalence of Mixed, Vegetarian, and Vegan Diets Linked to Sports & Exercise among Austrian Tertiary Students and Lecturers/Academic Staff. International Journal of Environmental Research and Public Health. 2022; 19(22):15313. https://doi.org/10.3390/ijerph192215313
Chicago/Turabian StyleWirnitzer, Katharina C., Mohamad Motevalli, Derrick R. Tanous, Gerold Wirnitzer, Karl-Heinz Wagner, Armando Cocca, Manuel Schätzer, Werner Kirschner, Clemens Drenowatz, and Gerhard Ruedl. 2022. "Study Protocol of “Sustainably Healthy—From Science 2 Highschool & University”—Prevalence of Mixed, Vegetarian, and Vegan Diets Linked to Sports & Exercise among Austrian Tertiary Students and Lecturers/Academic Staff" International Journal of Environmental Research and Public Health 19, no. 22: 15313. https://doi.org/10.3390/ijerph192215313