
Returning to Leisure Activity Post-Stroke: Barriers and Facilitators to Engagement
 , , and
, , and
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Questionnaires
2.3. Data Analysis
3. Results
3.1. Participant Characteristics at 6-Month Follow-Up
3.2. Barriers and Facilitators at 6 Month Follow-Up: Conceptual Themes
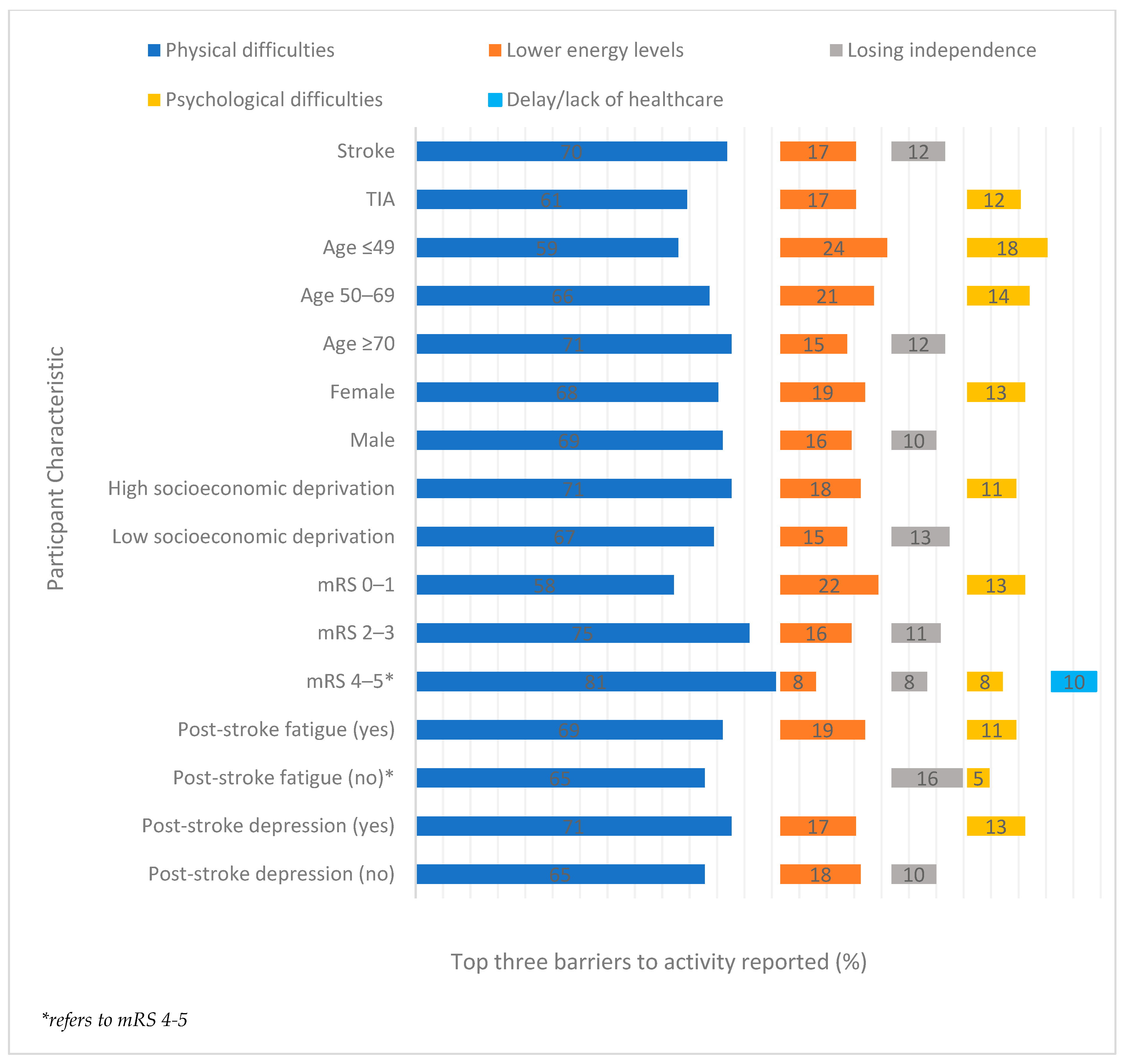
3.2.1. Barriers: Distribution of Participant Characteristics
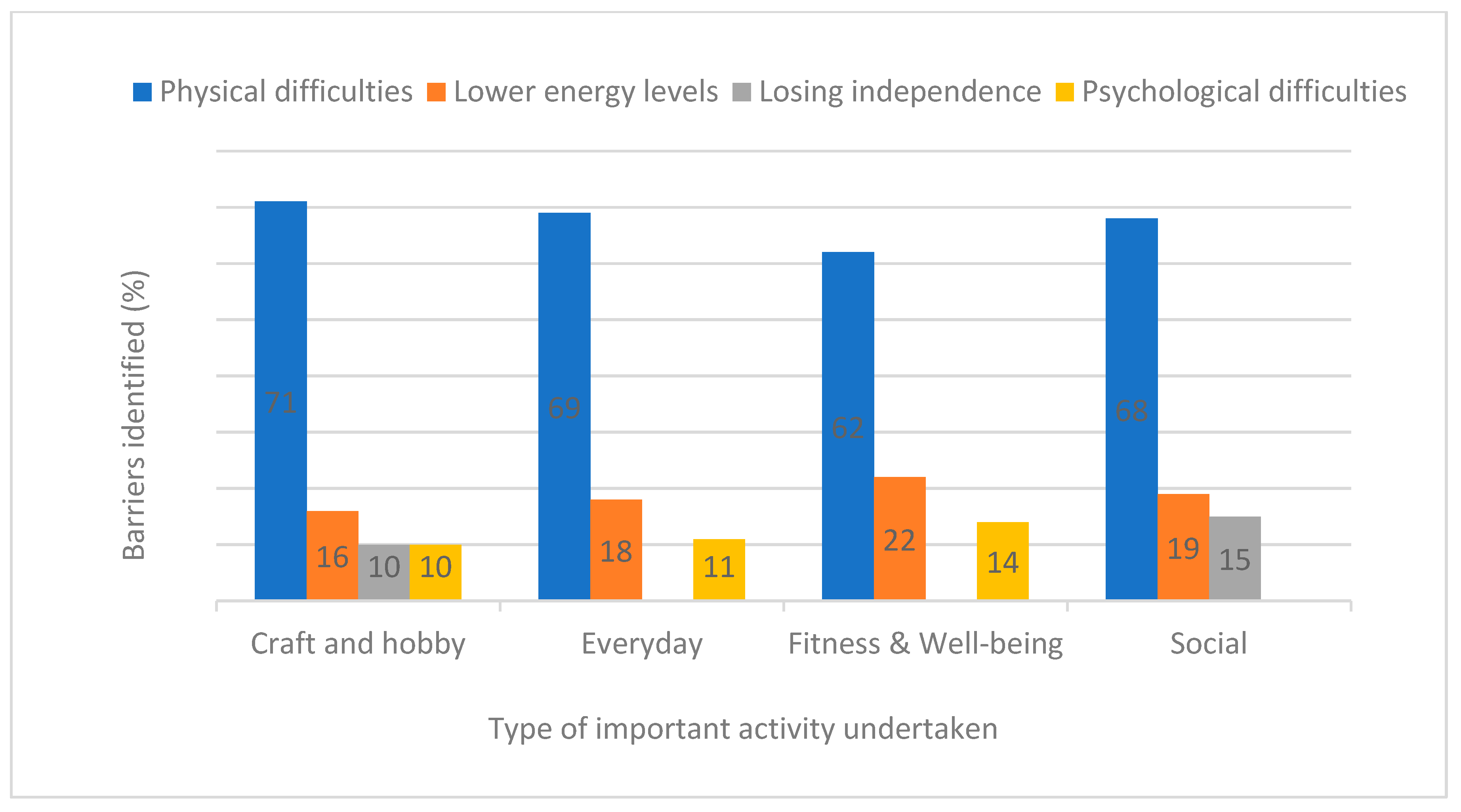
3.2.2. Barriers by Type of Important Activity
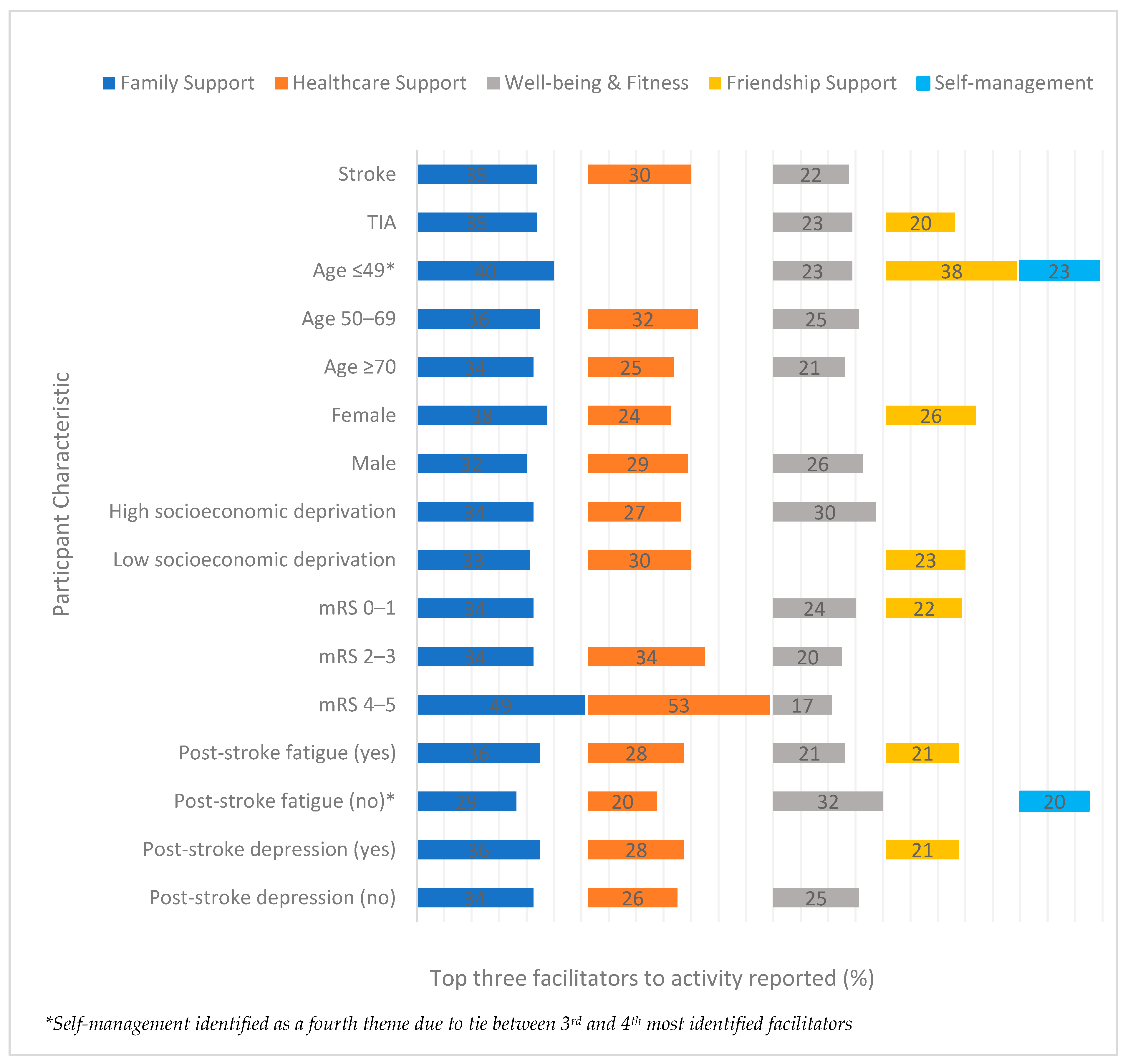
3.2.3. Facilitators: Distribution of Participant Characteristics
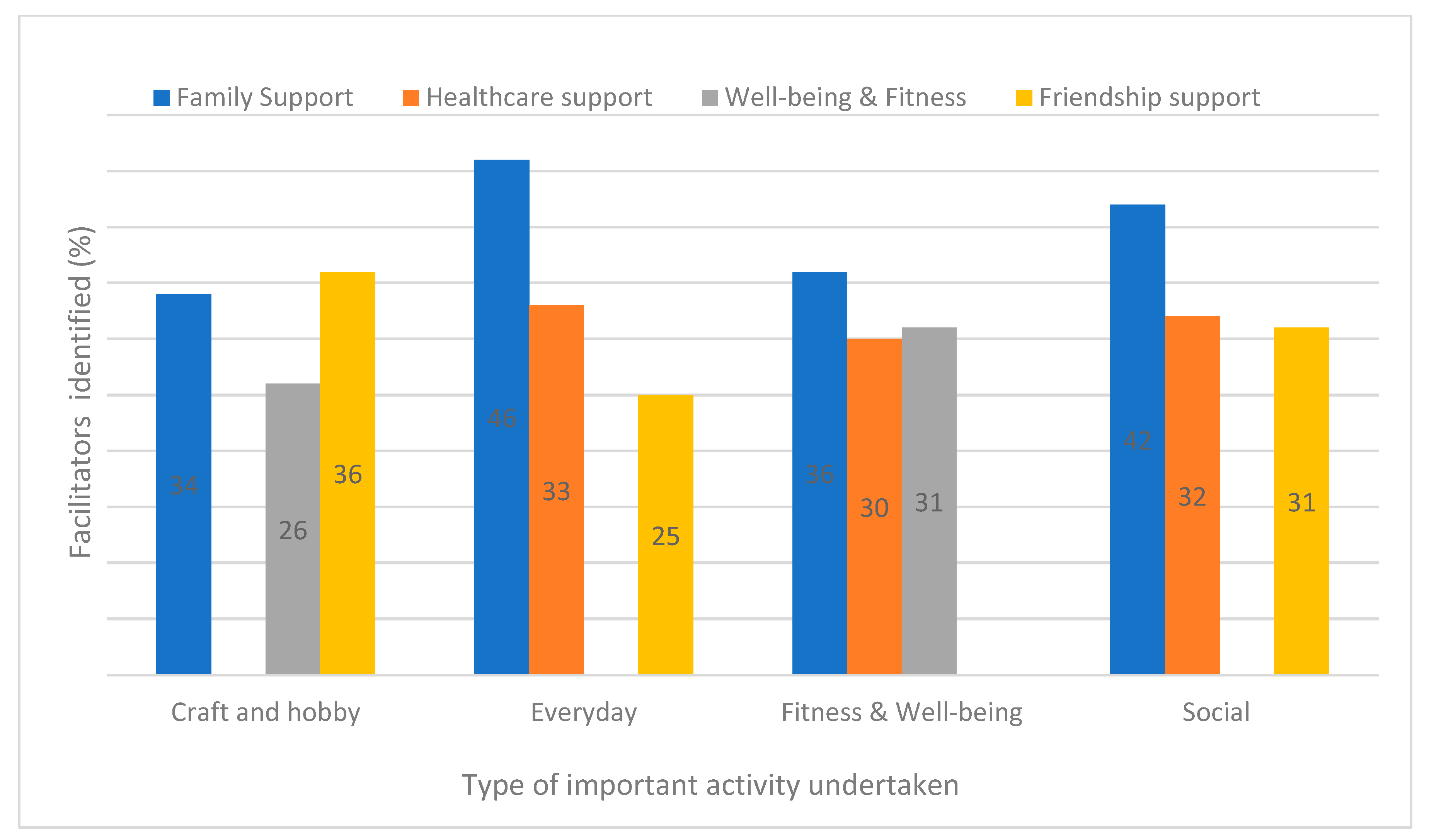
3.2.4. Facilitators by Type of Important Activity
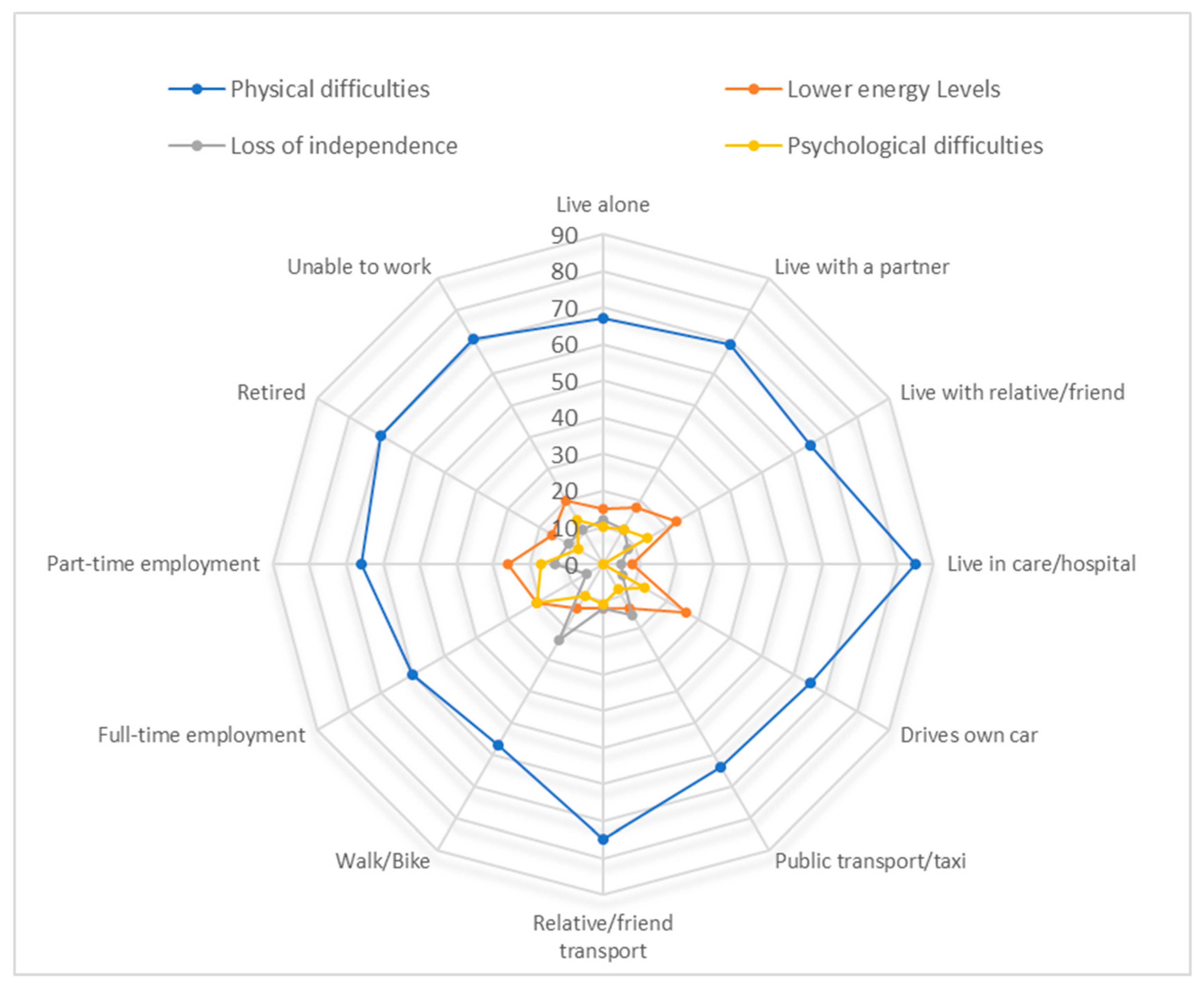
3.2.5. Participants Who Were Older, Female or Living in an Area of High Socioeconomic Deprivation
4. Discussion
4.1. Findings
4.2. Comparison with Existing Literature and Guidelines
4.3. Clinical and Policy Implications
4.4. Strengths and Limitations
4.5. Further Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Katan, M.; Luft, A. Global Burden of Stroke. Semin. Neurol. 2018, 38, 208–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norrving, B.; Kissela, B. The global burden of stroke and need for a continuum of care. Neurology 2013, 80 (Suppl. S2), S5–S12. [Google Scholar] [CrossRef] [PubMed]
- King, D.; Wittenberg, R.; Patel, A.; Quayyum, Z.; Berdunov, V.; Knapp, M. The future incidence, prevalence and costs of stroke in the UK. Age Ageing 2020, 49, 277–282. [Google Scholar] [CrossRef] [PubMed]
- Boysen, G.; Marott, J.L.; Grønbaek, M.; Hassanpour, H.; Truelsen, T. Long-term survival after stroke: 30 years of follow-up in a cohort, the Copenhagen City Heart Study. Neuroepidemiology 2009, 33, 254–260. [Google Scholar] [CrossRef]
- Joundi, R.A.; Patten, S.B.; Lukmanji, A.; Williams, J.V.A.; Smith, E.E. Association Between Physical Activity and Mortality Among Community-Dwelling Stroke Survivors. Neurology 2021, 97, e1182–e1191. [Google Scholar] [CrossRef]
- Kramer, S.F.; Hung, S.H.; Brodtmann, A. The Impact of Physical Activity Before and After Stroke on Stroke Risk and Recovery: A Narrative Review. Curr. Neurol. Neurosci. Rep. 2019, 19, 28. [Google Scholar] [CrossRef]
- Dorstyn, D.; Roberts, R.; Kneebone, I.; Kennedy, P.; Lieu, C. Systematic review of leisure therapy and its effectiveness in managing functional outcomes in stroke rehabilitation. Top. Stroke Rehabil. 2014, 21, 40–51. [Google Scholar] [CrossRef]
- Tse, T.; Linden, T.; Churilov, L.; Davis, S.; Donnan, G.; Carey, L.M. Longitudinal changes in activity participation in the first year post-stroke and association with depressive symptoms. Disabil. Rehabil. 2019, 41, 2548–2555. [Google Scholar] [CrossRef]
- Agahi, N.; Silverstein, M.; Parker, M.G. Late-Life and Earlier Participation in Leisure Activities: Their Importance for Survival Among Older Persons. Act. Adapt. Aging 2011, 35, 210–222. [Google Scholar] [CrossRef]
- Verberne, D.P.J.; Post, M.W.M.; Köhler, S.; Carey, L.M.; Visser-Meily, J.M.A.; van Heugten, C.M. Course of Social Participation in the First 2 Years After Stroke and Its Associations With Demographic and Stroke-Related Factors. Neurorehabil. Neural Repair 2018, 32, 821–833. [Google Scholar] [CrossRef]
- McKevitt, C.; Fudge, N.; Redfern, J.; Sheldenkar, A.; Crichton, S.; Rudd, A.R.; Forster, A.; Young, J.; Nazareth, I.; Silver, L.E.; et al. Self-reported long-term needs after stroke. Stroke 2011, 42, 1398–1403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Walsh, M.E.; Galvin, R.; Loughnane, C.; Macey, C.; Horgan, N.F. Community re-integration and long-term need in the first five years after stroke: Results from a national survey. Disabil. Rehabil. 2015, 37, 1834–1838. [Google Scholar] [CrossRef] [PubMed]
- Rozon, J.; Rochette, A. Changes in life habits affected by mild stroke and their association with depressive symptoms. J. Rehabil. Med. 2015, 47, 495–501. [Google Scholar] [CrossRef] [Green Version]
- Turner, G.M.; McMullan, C.; Atkins, L.; Foy, R.; Mant, J.; Calvert, M. TIA and minor stroke: A qualitative study of long-term impact and experiences of follow-up care. BMC Fam. Pract. 2019, 20, 176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Norlander, A.; Iwarsson, S.; Jönsson, A.C.; Lindgren, A.; Lexell, E.M. Living and ageing with stroke: An exploration of conditions influencing participation in social and leisure activities over 15 years. Brain Inj. 2018, 32, 858–866. [Google Scholar] [CrossRef] [PubMed]
- Reeves, M.J.; Thetford, C.; McMahon, N.; Forshaw, D.; Brown, C.; Joshi, M.; Watkins, C. Life and Leisure Activities following Stroke or Transient Ischaemic Attack (TIA): An Observational, Multi-Centre, 6-Month Follow-Up Study. Int. J. Environ. Res. Public Health 2022, 19, 13848. [Google Scholar] [CrossRef]
- Bowen, P.; Rose, R.; Pilkington, A. Mixed Methods—Theory and Practice. Sequential, Explanatory Approach. Int. J. Quant. Qual. Res. Methods 2017, 5, 10–27. [Google Scholar]
- Mahoney, J.; Drinka, T.J.; Abler, R.; Gunter-Hunt, G.; Matthews, C.; Gravenstein, S.; Carnes, M. Screening for depression: Single question versus GDS. J. Am. Geriatr. Soc. 1994, 9, 1006–1008. [Google Scholar]
- Rankin, J. Cerebral vascular accidents in patients over the age of 60: II. Prognosis. Scott. Med. J. 1957, 2, 200–215. [Google Scholar] [CrossRef]
- Corbin, J.; Strauss, A. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory, 2nd ed.; Sage Publications: New York, NY, USA, 2008. [Google Scholar]
- Franco, M.R.; Tong, A.; Howard, K.; Sherrington, C.; Ferreira, P.H.; Pinto, R.Z.; Ferreira, M.L. Older people’s perspectives on participation in physical activity: A systematic review and thematic synthesis of qualitative literature. Br. J. Sports Med. 2015, 49, 1268–1276. [Google Scholar] [CrossRef]
- Robison, J.; Wiles, R.; Ellis-Hill, C.; McPherson, K.; Hyndman, D.; Ashburn, A. Resuming previously valued activities post-stroke: Who or what helps? Disabil. Rehabil. 2009, 31, 1555–1566. [Google Scholar] [CrossRef] [PubMed]
- Norlander, A.; Carlstedt, E.; Jönsson, A.C.; Lexell, E.M.; Ståhl, A.; Lindgren, A.; Iwarsson, S. Long-Term Predictors of Social and Leisure Activity 10 Years after Stroke. PLoS ONE 2016, 11, e0149395. [Google Scholar] [CrossRef] [PubMed]
- Masterson-Algar, P.; Williams, S.; Burton, C.R.; Arthur, C.A.; Hoare, Z.; Morrison, V.; Radford, K.; Seddon, D.; Elghenzai, S. Getting back to life after stroke: Co-designing a peer-led coaching intervention to enable stroke survivors to rebuild a meaningful life after stroke. Disabil. Rehabil. 2020, 42, 1359–1372. [Google Scholar] [CrossRef] [PubMed]
- Gough, C.; Baker, N.; Weber, H.; Lewis, L.K.; Barr, C.; Maeder, A.; George, S. Integrating community participation in the transition of older adults from hospital to home: A scoping review. Disabil. Rehabil. 2021, 28, 1–13. [Google Scholar] [CrossRef]
- Elloker, T.; Rhoda, A.J. The relationship between social support and participation in stroke: A systematic review. Afr. J. Disabil. 2018, 10, 357. [Google Scholar] [CrossRef] [Green Version]
- Jellema, S.; van Hees, S.; Zajec, J.; van der Sande, R.; van der Sanden, M.W.G.N.; Steultjens, E.M.J. What environmental factors influence resumption of valued activities post stroke: A systematic review of qualitative and quantitative findings. Clin. Rehabil. 2017, 31, 936–947. [Google Scholar] [CrossRef] [Green Version]
- Norlander, A.; Iwarsson, A.S.; Jönsson, A.C.; Lindgren, A.; Lexell, E.M. Participation in social and leisure activities while re-constructing the self: Understanding strategies used by stroke survivors from a long-term perspective. Disabil. Rehabil. 2021, 28, 1–9. [Google Scholar] [CrossRef]
- NICE Guideline 2013. Stroke Rehabilitation in Adults (CG162). Available online: https://www.nice.org.uk/guidance/cg162 (accessed on 11 July 2022).
- Razzaque, R.; Wood, L. Open Dialogue and its Relevance to the NHS: Opinions of NHS Staff and Service Users. Community Ment. Health J. 2015, 51, 931–938. [Google Scholar] [CrossRef]
- Fernández-Peña, R.; Molina, J.L.; Valero, O. Personal Network Analysis in the Study of Social Support: The Case of Chronic Pain. Int. J. Environ. Res. Public Health 2018, 15, 2695. [Google Scholar] [CrossRef] [Green Version]
- Langhorne, P.; Baylan, S.; Early Supported Discharge Trialists. Early supported discharge services for people with acute stroke. Cochrane Database Syst. Rev. 2017, 7, CD000443. [Google Scholar] [CrossRef] [Green Version]
- Simpson, S.; Furlong, M.; Giebel, C. Exploring the enablers and barriers to social prescribing for people living with long-term neurological conditions: A focus group investigation. BMC Health Serv. Res. 2021, 21, 1230. [Google Scholar] [CrossRef] [PubMed]
- Burton, C.R.; Fargher, E.; Plumpton, C.; Roberts, G.W.; Owen, H.; Roberts, E. Investigating preferences for support with life after stroke: A discrete choice experiment. BMC Health Serv. Res. 2014, 14, 63. [Google Scholar] [CrossRef] [PubMed]
- Boland, P.; Connell, L.; Thetford, C.; Janssen, J. Exploring the factors influencing the use of electrically assisted bikes (e-bikes) by stroke survivors: A mixed methods multiple case study. Disabil. Rehabil. 2022, 44, 1389–1398. [Google Scholar] [CrossRef] [PubMed]
- White, J.; Janssen, H.; Jordan, L.; Pollack, M. Tablet technology during stroke recovery: A survivor’s perspective. Disabil. Rehabil. 2015, 37, 1186–1192. [Google Scholar] [CrossRef] [PubMed]
- Lemke, M.; Rodríguez Ramírez, E.; Robinson, B.; Signal, N. Motivators and barriers to using information and communication technology in everyday life following stroke: A qualitative and video observation study. Disabil. Rehabil. 2020, 42, 1954–1962. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant Characteristics | Respondents to 6M Questionnaire n = 2000 | Respondents to Barrier Question n = 1045 | Respondents to Facilitator Question n = 820 |
|---|---|---|---|
| Event type, n (%) | |||
| Stroke | 1549 (77.5) | 872 (83.4) | 673 (82.1) |
| TIA | 451 (22.6) | 173 (16.6) | 147 (17.9) |
| Age, n (%) | |||
| ≤49 | 104 (5.2) | 66 (6.3) | 47 (5.7) |
| 50–69 | 633 (31.7) | 315 (30.2) | 238 (29.0) |
| ≥70 | 1263 (63.2) | 664 (63.5) | 535 (65.2) |
| Age, median (IQR) | 73 (65–80) | 74 (64–81) | 73 (65–80) |
| Sex, n (%) | |||
| Male | 1167 (58.3) | 569 (54.5) | 474 (57.8) |
| Female | 833 (41.7) | 476 (45.6) | 346 (42.2) |
| Ethnicity, n (%) | |||
| White | 1942 (97.1) | 1013 (97.0) | 794 (96.8) |
| Asian | 24 (1.2) | 16 (1.5) | 10 (1.2) |
| Black | 16 (0.8) | 6 (0.6) | 8 (1.0) |
| Mixed | 7 (0.4) | 4 (0.4) | 2 (0.2) |
| Other | 11 (0.6) | 6 (0.6) | 6 (0.7) |
| Socioeconomic Deprivation quintile, n (%) * | |||
| 1st (High deprivation) | 286 (14.3) | 160 (15.3) | 99 (12.1) |
| 2nd | 353 (17.7) | 186 (17.8) | 147 (17.9) |
| 3rd | 445 (22.3) | 234 (22.4) | 171 (20.9) |
| 4th | 448 (22.4) | 210 (20.1) | 203 (24.8) |
| 5th (Low deprivation) | 467 (23.4) | 255 (24.4) | 200 (24.4) |
| modified Rankin Scale, n (%) | |||
| 0–1 (no symptoms-no significant disability) | 1211 (60.6) | 456 (43.6) | 515 (62.8) |
| 2–3 (slight to moderate disability) | 569 (28.5) | 423 (40.5) | 239 (29.1) |
| 4–5 (severe disability) | 192 (9.6%) | 147 (14.1) | 59 (7.2) |
| Unknown | 28 (1.4%) | 19 (1.8) | 7 (0.9) |
| Theme n (%) | Description | Quotes |
|---|---|---|
| Physical difficulties 717 (69%) | Physical difficulties that restricted or curtailed the ability to undertake activity. This included mobility problems such as walking and balance, communication issues, and loss of fine movement for undertaking crafts or playing an instrument. | “I used to walk about 5 miles each day, now, although I am improving, I can’t walk far at all” “Gardening-lack of balance when bending” “Loss of fine motor movements in both hands make it difficult to write and impossible to do the crafts I enjoyed doing”“change of voice leading to not being able to enjoy amateur dramatics again” |
| Lower energy Levels 179 (17%) | A decline in energy levels described by participants as tiredness or fatigue, lack of stamina, needing to lie down or sleep and having to do things slowly. | “My hobby is cars and bikes but I get tired very easily then have to pack up” “My stamina is now significantly less, e.g., walking, in the garden, shopping, etc. My social-stamina is less because too much talking gives me a headache” “A sense of fatigue. Having to do things like gardening more slowly” |
| Loss of independence 111 (11%) | A loss of independence, in particular the ability to drive, inhibited engagement in activities away from the home. Alternative travel arrangements often required substantial planning and reliance on others. This restriction often led to low mood. The loss of driving as an enjoyable activity also had a negative impact. | “Not being able to drive makes it difficult to carry tools/plants down to my allotment. I wait until someone is available to give me a lift or I call a taxi” “Needing to make a plan for any activities and checking somebody can take me is very depressing” “I have been the family driver for fifty-eight years and have found it difficult to give up driving which I’ve always enjoyed” |
| Psychological difficulties 109 (10%) | Fear and anxiety were notable psychological difficulties including a fear of falling when outside, anxiety about having another stroke or feeling vulnerable from being out alone. Others reported a lack of confidence in resuming activity and some felt that it was other people who indicated uncertainty in their ability, resulting in feelings of frustration and anger. Feelings of low mood, depression and apathy were also often reported as a barrier to resuming activity. | “I am a boat owner and very keen angler but since my stroke I am very nervous about going to sea on my own” “I find that I have lost a lot of self -confidence in my game (golf). This has resulted in me being very upset when I play badly and affects my engagement and my readiness to be involved”. “I have been ‘petted’ on the head and shoulders by people, as if I am a bewildered child-this makes me want to stay home” |
| Hidden Disabilities 69 (7%) | Hidden disabilities such as a lack of concentration or maintaining focus were sometimes a barrier to undertaking everyday activities, hobbies and crafts. Memory problems and feeling overwhelmed by the environment affected confidence, especially for activities that required focus or socialising. | “Reading was a great pleasure but issues with sight and concentration mean it is now too difficult” “My memory is not as good as it was. This is so for general conversation. I avoid quiz games and find spelling more difficult” “Sensitivity to busy environments, noise and lights made things difficult” |
| Delay or lack of healthcare provision 31 (3%) | A lack of healthcare support such as physiotherapy provision and home adaptations typically delayed recovery and a return to activity (getting out of the house or care home). | “Lack of immediate support. It took over 12 weeks for physio to start and for adaptions and support to be arranged” “We still can’t get out due to no ramp/rails waiting to be put in place-very frustrating” |
| Theme n (% of Response) | Description | Quotes |
|---|---|---|
| Family Support 286 (35%) | Family support was both emotional and practical in nature. Encouragement and reassurance from family members helped to build confidence in returning to activities, from lunches out with family, to more organised activities such as attending a social club. Family support also included practical help with transport, mobility and facilitating a return to activities in addition to help with chores, hospital visits, etc. | “Partner has helped in giving me encouragement to return to singing with the choir” “Family support has been vital to resuming my favourite activities” “My daughter takes me out as much as possible and arranged art club bingo and takes me swimming/shopping and helps me with everything” |
| Healthcare Support 221 (27%) | Provision of rehabilitation therapies offered from healthcare services such as physiotherapy, occupational therapy and speech therapy were thought to be beneficial in improving ability such as balance and movement and subsequently enabling engagement in activity. Therapists also helped to install confidence that patients would return to activities in time. Stroke services including follow-ups, early supported discharge teams and the Stroke Association were referred to as informative, helpful and encouraging. Provision of mobility aids, equipment and appropriate medication were also reported as beneficial. | “Physios/OTs helped a lot from Stroke Team when I was discharged from hospital. Huge help to get me walking with my dog again (alone). Gave me more confidence” “I am sure with my physio’s help I will get back to my clubs and coffees/lunches out with friends” “All of the help and support of the stroke team has helped me with exercises and food a great deal” |
| Well-being and fitness 183 (22%) | Improving well-being was a means to re-engaging in activities and was practised by eating well, giving up smoking, losing weight and achieving a better work/life balance. Needing more rest was often necessary and was achieved through sitting breaks, sleeps during the day, regular bedtime, and more relaxation. Exercise and keeping active helped to improve general fitness for other activities, and walking was a popular choice. Many participants also enjoyed returning to previously enjoyed activities such as the gym, yoga or golf. | “Sleeping more and keeping the nutrition good” “Wanting to get fit and keeping healthy, by going back into the gym now, I feel a lot better in my mind, and health” “Walking also benefits my balance particularly when I’m playing the guitar and singing with a band” |
| Friendship Support 164 (20%) | As with family support, friends provided encouragement and practical help in returning to social activity. In addition, the continuation of previous social patterns and maintaining friendship was valued and provided further encouragement to move forward with recovery. | “My friends at my sheltered dwelling have encouraged me to help out making afternoon tea for our regular get togethers” “Friends in a fishing club have helped me fishing by carrying fishing tackle etc and helping me setting up if I need” “The fact that these activities are part of my social life where I meet friends and that continuing as before, has helped me move on” |
| Self-management 152 (19%) | Self-management techniques such as taking things slowly, setting goals and acceptance of limitations helped to build confidence. Self-belief, determination and a positive attitude were also beneficial in getting through difficulties and not giving up. Having the motivation to do activities again for pleasure, fitness or wanting to be part of life also helped to build resilience, adapt to changes and overcome difficulties. | “Taking things slowly and not thinking it will be just as it was. Enjoying what you can do, not what you can’t do” “I am also very independent and strong-willed, so very determined to get on as well as possible” “Positive mental attitude and a ‘can do’ approach-adapt and overcome” |
| Returning to normality 70 (9%) | The desire to get back to normal or return to old routines was a motivator for resuming activity. Returning to previous routines also offered a sense of reassurance that pre-stroke activities were possible. Time and patience were mentioned as a means of achieving the goal of returning to normal. Managing change helped to form a new normality. | “Getting back to normal, doing the things I like doing” “I think it’s putting everything behind me and focussing on having a normal life as before’ ‘Managing change and finding new ways of thinking and doing” |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harrison, J.; Thetford, C.; Reeves, M.J.; Brown, C.; Joshi, M.; Watkins, C. Returning to Leisure Activity Post-Stroke: Barriers and Facilitators to Engagement. Int. J. Environ. Res. Public Health 2022, 19, 14587. https://doi.org/10.3390/ijerph192114587
Harrison J, Thetford C, Reeves MJ, Brown C, Joshi M, Watkins C. Returning to Leisure Activity Post-Stroke: Barriers and Facilitators to Engagement. International Journal of Environmental Research and Public Health. 2022; 19(21):14587. https://doi.org/10.3390/ijerph192114587
Chicago/Turabian StyleHarrison, Joanna, Clare Thetford, Matthew J. Reeves, Christopher Brown, Miland Joshi, and Caroline Watkins. 2022. "Returning to Leisure Activity Post-Stroke: Barriers and Facilitators to Engagement" International Journal of Environmental Research and Public Health 19, no. 21: 14587. https://doi.org/10.3390/ijerph192114587