
Promoting Effective Self-Management of the Gluten-Free Diet: Children’s and Adolescents’ Self-Generated Do’s and Don’ts


Abstract
:1. Introduction
- (1)
- Explore self-generated procedures children and adolescents with CD perform when participating in food-related activities in light of their self-management skills and health requirements;
- (2)
- Present an initial database of suggested strategies supporting self-management among children and adolescents with CD using self-management do’s and don’ts that they generated;
- (3)
- Compare the strategies used by children versus adolescents and by time passed since diagnosis.
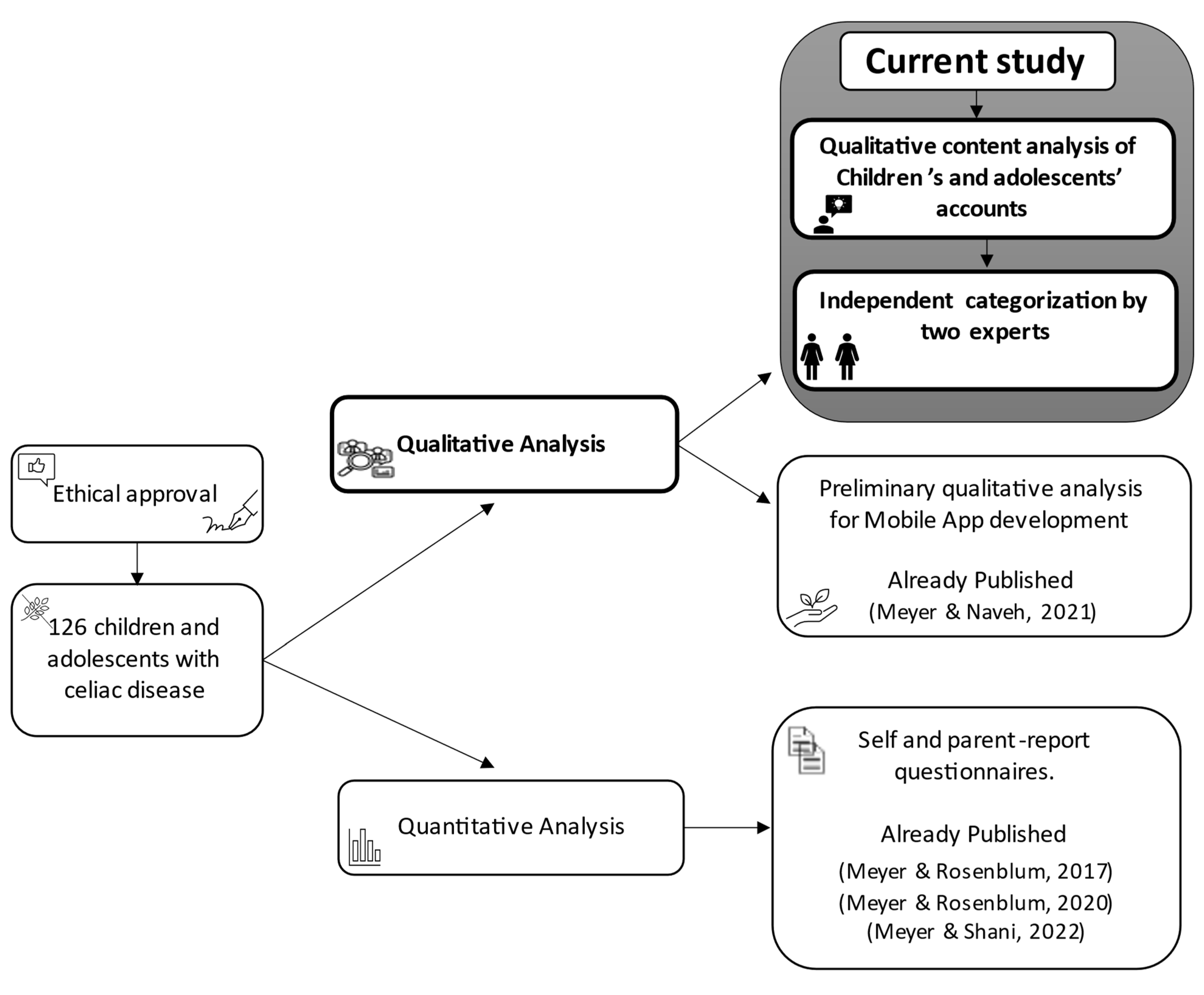
2. Materials and Methods
2.1. Participants and Procedure
2.2. Data Analysis
3. Results
4. Discussion
5. Limitations and Future Research
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Lebwohl, B.; Rubio-Tapia, A. Epidemiology, Presentation, and Diagnosis of Celiac Disease. Gastroenterology 2021, 160, 63–75. [Google Scholar] [CrossRef] [PubMed]
- Makharia, G.K.; Singh, P.; Catassi, C.; Sanders, D.S.; Leffler, D.; Ali, R.A.R.; Bai, J.C. The Global Burden of Coeliac Disease: Opportunities and Challenges. Nat. Rev. Gastroenterol. Hepatol. 2022, 19, 313–327. [Google Scholar] [CrossRef] [PubMed]
- Catassi, C.; Verdu, E.F.; Bai, J.C.; Lionetti, E. Coeliac Disease. Lancet 2022, 399, 2413–2426. [Google Scholar] [CrossRef]
- Wessels, M.; Auricchio, R.; Dolinsek, J.; Donat, E.; Gillett, P.; Mårild, K.; Meijer, C.; Popp, A.; Mearin, M.L. Review on Pediatric Coeliac Disease from a Clinical Perspective. Eur. J. Pediatr. 2022, 181, 1785–1795. [Google Scholar] [CrossRef] [PubMed]
- Myléus, A.; Reilly, N.R.; Green, P.H.R. Rate, Risk Factors, and Outcomes of Nonadherence in Pediatric Patients With Celiac Disease: A Systematic Review. Clin. Gastroenterol. Hepatol. 2020, 18, 562–573. [Google Scholar] [CrossRef] [PubMed]
- See, J.A.; Kaukinen, K.; Makharia, G.K.; Gibson, P.R.; Murray, J.A. Practical Insights into Gluten-Free Diets. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 580–591. [Google Scholar] [CrossRef]
- Crespo-Escobar, P. Gluten Free Diet. In Advances in Celiac Disease; Springer International Publishing: Cham, Switzerland, 2022; pp. 121–136. [Google Scholar]
- Ludvigsson, J.F.; Agreus, L.; Ciacci, C.; Crowe, S.E.; Geller, M.G.; Green, P.H.R.; Hill, I.; Hungin, A.P.; Koletzko, S.; Koltai, T. Transition from Childhood to Adulthood in Coeliac Disease: The Prague Consensus Report. Gut 2016, 65, 1242–1251. [Google Scholar] [CrossRef]
- World Health Organization. Adolescent Development. Available online: http://www.who.int/maternal_child_adolescent/topics/adolescence/dev/en/ (accessed on 1 January 2019).
- Vroman, K. Adolescent Development: Transitioning from Child to Adult. In Occupational Therapy for Children and Adolescents; Case-Smith, J., Clifford O’Brien, J., Eds.; Elsevier: St. Louis, MO, USA, 2015; pp. 102–121. [Google Scholar]
- Rashid, M.; Cranney, A.; Zarkadas, M.; Graham, I.D.; Switzer, C.; Case, S.; Molloy, M.; Warren, R.E.; Burrows, V.; Butzner, J.D. Celiac Disease: Evaluation of the Diagnosis and Dietary Compliance in Canadian Children. Pediatrics 2005, 116, e759. [Google Scholar] [CrossRef] [Green Version]
- Meyer, S.; Rosenblum, S. Development and Validation of the Celiac Disease-Children’s Activities Report (CD-Chart) for Promoting Self-Management among Children and Adolescents. Nutrients 2017, 9, 1130. [Google Scholar] [CrossRef] [Green Version]
- Fishman, L.N.; Kearney, J.; DeGroote, M.; Liu, E.; Arnold, J.; Weir, D.C. Creation of Experience-Based Celiac Benchmarks-The First Step in Pre-Transition Self-Management Assessment. J. Pediatr. Gastroenterol. Nutr. 2018, 67, e6–e10. [Google Scholar] [CrossRef]
- Lorig, K.; Holman, H.R. Self-Management Education: History, Definition, Outcomes, and Mechanisms. Ann. Behav. Med. 2003, 26, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Modi, A.C.; Pai, A.L.; Hommel, K.L.; Hood, K.K.; Cortina, S.; Hilliard, M.E.; Guilfoyle, S.M.; Gray, W.; Drotar, D. Pediatric Self-Management: A Framework for Research, Practice, and Policy. Pediatrics 2012, 129, e485. [Google Scholar] [CrossRef] [Green Version]
- Meyer, S.; Rosenblum, S. Examining Core Self-Management Skills among Adolescents with Celiac Disease. J. Health Psychol. 2020, 26, 2592–2602. [Google Scholar] [CrossRef] [PubMed]
- Wolf, R.L.; Lebwohl, B.; Lee, A.R.; Zybert, P.; Reilly, N.R.; Cadenhead, J.; Amengual, C.; Green, P.H.R. Hypervigilance to a Gluten-Free Diet and Decreased Quality of Life in Teenagers and Adults with Celiac Disease. Dig. Dis. Sci. 2018, 63, 1438–1448. [Google Scholar] [CrossRef] [PubMed]
- Bodenheimer, T.; Lorig, K.; Holman, H.; Grumbach, K. Patient Self-Management of Chronic Disease in Primary Care. JAMA 2002, 288, 2469–2475. [Google Scholar] [CrossRef]
- Packer, T.L. Self-management Interventions: Using an Occupational Lens to Rethink and Refocus. Aust. Occup. Ther. J. 2013, 60, 1–2. [Google Scholar] [CrossRef]
- Zingone, F.; Massa, S.; Malamisura, B.; Pisano, P.; Ciacci, C. Coeliac Disease: Factors Affecting the Transition and a Practical Tool for the Transition to Adult Healthcare. United Eur. Gastroenterol. J. 2018, 6, 1356–1362. [Google Scholar] [CrossRef]
- Toglia, J.; Foster, E.R. The Multicontext Approach to Cognitive Rehabilitation; Gatekeeper Press: Columbus, OH, USA, 2021. [Google Scholar]
- Coates, V.E.; Boore, J.R.P. Self-Management of Chronic Illness: Implications for Nursing. Int. J. Nurs. Stud. 1995, 32, 628–640. [Google Scholar] [CrossRef]
- American Occupational Therapy Association Occupational Therapy Practice Framework: Domain and Process Fourth Edition. Am. J. Occup. Ther. 2020, 74, 7412410010p1–7412410010p87. [CrossRef]
- Howard, R.A.; Urquhart-Law, G. Psychological Well-Being of Children and Young People with Coeliac Disease. In Paediatric Gastrointestinal Disorders; Martin, C., Dovey, T., Eds.; Radcliffe Publishing Ltd.: London, UK, 2014; pp. 186–207. [Google Scholar]
- Creswell, J.W. Qualitative Inquiry and Research Design: Choosing among Five Approaches, 3rd ed.; SAGE Publications, Incorporated: Thousand Oaks, CA, USA, 2013. [Google Scholar]
- Meyer, S.; Naveh, G. Mobile Application for Promoting Gluten-Free Diet Self-Management in Adolescents with Celiac Disease: Proof-of-Concept Study. Nutrients 2021, 13, 1401. [Google Scholar] [CrossRef]
- Tyano, S. Growth and Development. In Selected Chapters in Psychiatry; Munitz, H., Ed.; Dyonon: Tel Aviv, Israel, 2010; p. 31. [Google Scholar]
- Central Bureau of Statistics-Israel. Available online: https://www.cbs.gov.il/en/Pages/default.aspx (accessed on 22 July 2022).
- Bascuñán, K.A.; Vespa, M.C.; Araya, M. Celiac Disease: Understanding the Gluten-Free Diet. Eur. J. Nutr. 2017, 56, 449–459. [Google Scholar] [CrossRef] [PubMed]
- Holbein, C.E.; Carmody, J.K.; Hommel, K.A. Topical Review: Adherence Interventions for Youth on Gluten-Free Diets. J. Pediatr. Psychol. 2018, 43, 392–401. [Google Scholar] [CrossRef] [PubMed]
- Case, S. The Gluten-Free Diet: How to Provide Effective Education and Resources. Gastroenterology 2005, 128, S134. [Google Scholar] [CrossRef]
- Raiteri, A.; Granito, A.; Giamperoli, A.; Catenaro, T.; Negrini, G.; Tovoli, F. Current Guidelines for the Management of Celiac Disease: A Systematic Review with Comparative Analysis. World J. Gastroenterol. 2022, 28, 154–175. [Google Scholar] [CrossRef]
- Clerx, E.M.; Silvester, J.; Leffler, D.; DeGroote, M.; Fishman, L.N. Sequence of Acquisition of Self-Management Skills to Follow a Gluten-Free Diet by Adults with Celiac Disease. Dig. Liver Dis. 2019, 51, 1096–1100. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. [WHO] World Health International Classification of Functioning, Disability and Health: Children & Youth Version: ICF-CY; WHO: Geneva, Switzerland, 2007. [Google Scholar]
- Anaby, D.; Law, M. The Role of Participation in the Lives of Children and Young People with Neurological and Developmental Conditions. In Life Quality Outcomes in Children and Young People with Neurological and Developmental Conditions; Ronen, G., Rosenbaum, P., Eds.; Mac Keith Press: London, UK, 2013; pp. 51–64. [Google Scholar]
- Imms, C.; Granlund, M.; Wilson, P.H.; Steenbergen, B.; Rosenbaum, P.L.; Gordon, A.M. Participation, Both a Means and an End: A Conceptual Analysis of Processes and Outcomes in Childhood Disability. Dev. Med. Child. Neurol. 2017, 59, 16–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmidt, E.K.; Faieta, J.; Tanner, K. Scoping Review of Self-Advocacy Education Interventions to Improve Care. OTJR Occup. Particip. Health 2020, 40, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Schena, D.; Rosales, R.; Rowe, E. Teaching Self-Advocacy Skills: A Review and Call for Research. J. Behav. Educ. 2022, 1–49. [Google Scholar] [CrossRef]
- Barrio, J.; Cilleruelo, M.L. Quality of Life in Celiac Disease. In Advances in Celiac Disease; Amil-Dias, J., Polanco, I., Eds.; Springer: Berlin/Heidelberg, Germany, 2022; pp. 193–213. [Google Scholar] [CrossRef]
- Meyer, S.; Shani, M. Structural Validation and Dyadic Child-Parent Measurement Invariance of the Celiac Disease Quality of Life Questionnaire. Eur. J. Gastroenterol. Hepatol. 2022, 34, 39–47. [Google Scholar] [CrossRef]
- Test, D.W.; Fowler, C.H.; Wood, W.M.; Brewer, D.M.; Eddy, S. A Conceptual Framework of Self-Advocacy for Students with Disabilities. Remedial Spec. Educ. 2005, 26, 43–54. [Google Scholar] [CrossRef]
- Levush, R. Israel: Military Draft Law and Enforcement; Law Library of Congress, Global Legal Research Directorate: Washington, DC, USA, 2019. Available online: https://www.loc.gov/item/2019713409/ (accessed on 24 July 2022).



{kind=link}
{kind=link}
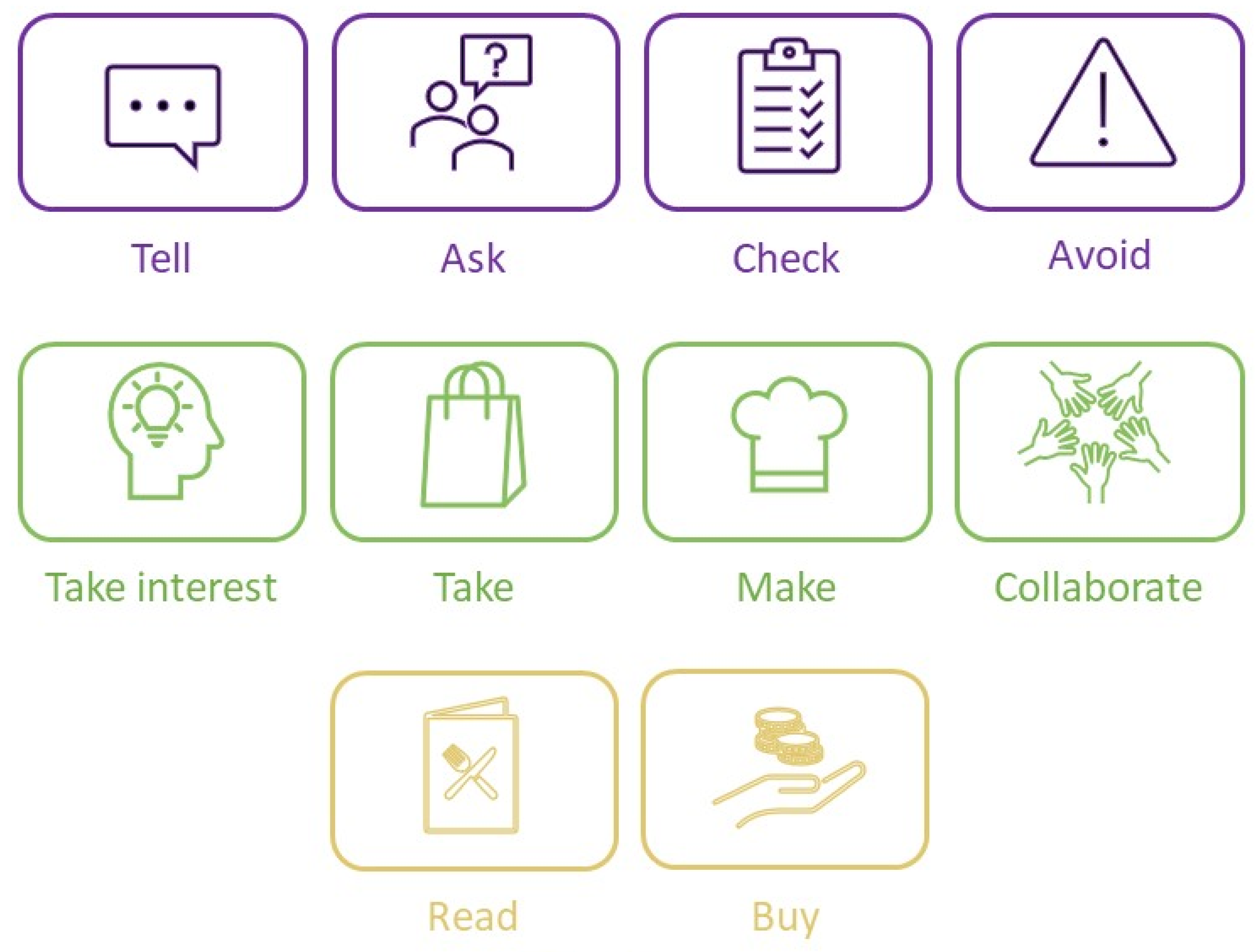
| Action Category | Action | Children (n = 61) | Adolescents (n = 66) |
|---|---|---|---|
| 1. Tell |
| 13 | 7 |
| 0 | 1 | |
| 0 | 1 | |
| 1 | 0 | |
| 0 | 1 | |
| 1 | 1 | |
| 0 | 1 | |
| 0 | 2 | |
| 0 | 1 | |
| 0 | 2 | |
| 3 | 0 | |
| 1 | 1 | |
| 0 | 1 | |
| 0 | 1 | |
| 0 | 1 | |
| 0 | 2 | |
| 0 | 1 | |
| 2 | 0 | |
| 2 | 0 | |
| 0 | 1 | |
| 1 | 2 | |
| 3 | 3 | |
| 2 | 4 | |
| 1 | 0 | |
| 0 | 1 | |
| 2 | 0 | |
| 2 | 0 | |
| 0 | 1 | |
| 0 | 1 | |
| 0 | 1 | |
| 2. Ask |
| 8 | 1 |
| 3 | 6 | |
| 0 | 1 | |
| 0 | 1 | |
| 0 | 4 | |
| 1 | 1 | |
| 0 | 3 | |
| 2 | 0 | |
| 0 | 1 | |
| 0 | 3 | |
| 0 | 5 | |
| 1 | 3 | |
| 3 | 1 | |
| 1 | 3 | |
| 1 | 2 | |
| 0 | 1 | |
| 1 | 3 | |
| 1 | 1 | |
| 2 | 0 | |
| 0 | 2 | |
| 4 | 1 | |
| 2 | 1 | |
| 1 | 4 | |
| 0 | 3 | |
| 3 | 0 | |
| 0 | 1 | |
| 1 | 1 | |
| 1 | 0 | |
| 1 | 0 | |
| 3. Check |
| 2 | 8 |
| 1 | 6 | |
| 1 | 0 | |
| 0 | 1 | |
| 0 | 2 | |
| 5 | 2 | |
| 0 | 1 | |
| 3 | 1 | |
| 2 | 4 | |
| 0 | 4 | |
| 1 | 3 | |
| 1 | 5 | |
| 12 | 4 | |
| 0 | 1 | |
| 0 | 2 | |
| 0 | 1 | |
| 0 | 3 | |
| 4. Avoid |
| 2 | 1 |
| 10 | 7 | |
| 1 | 1 | |
| 2 | 1 | |
| 3 | 4 | |
| 1 | 0 | |
| 2 | 1 | |
| 2 | 0 | |
| 1 | 1 | |
| 2 | 0 | |
| 0 | 2 | |
| 1 | 1 | |
| 5. Take interest |
| 2 | 3 |
| 0 | 2 | |
| 1 | 3 | |
| 1 | 2 | |
| 1 | 0 | |
| 0 | 5 | |
| 0 | 1 | |
| 3 | 8 | |
| 6. Take |
| 12 | 10 |
| 5 | 0 | |
| 1 | 2 | |
| 1 | 5 | |
| 2 | 1 | |
| 1 | 1 | |
| 0 | 1 | |
| 7. Make |
| 2 | 12 |
| 0 | 1 | |
| 0 | 1 | |
| 4 | 8 | |
| 2 | 5 | |
| 2 | 6 | |
| 8. Collaborate |
| 0 | 2 |
| 2 | 1 | |
| 6 | 2 | |
| 1 | 0 | |
| 0 | 1 | |
| 0 | 2 | |
| 9. Read |
| 2 | 0 |
| 17 | 5 | |
| 4 | 0 | |
| 0 | 1 | |
| 0 | 1 | |
| 1 | 0 | |
| 10. Buy |
| 0 | 3 |
| 1 | 0 | |
| 2 | 2 | |
| 0 | 2 |
| Action Category | Entire Sample (N = 126) | Children (n = 61) | Adolescents (n = 65) | χ2 | p |
|---|---|---|---|---|---|
| 1. Tell | 43.7% | 44.3% | 43.1% | 0.018 | 0.893 |
| 2. Ask | 46.8% | 37.7% | 55.4% | 3.950 | 0.047 |
| 3. Check | 47.6% | 44.3% | 50.8% | 0.534 | 0.465 |
| 4. Avoid | 30.2% | 37.7% | 23.1% | 3.197 | 0.074 |
| 5. Take interest | 17.5% | 11.5% | 23.1% | 2.939 | 0.086 |
| 6. Take | 31.7% | 36.1% | 27.7% | 1.018 | 0.313 |
| 7. Make | 29.4% | 16.4% | 41.4% | 9.592 | 0.002 |
| 8. Collaborate | 9.5% | 13.1% | 6.2% | 1.770 | 0.183 |
| 9. Read | 21.4% | 34.4% | 9.2% | 11.865 | 0.001 |
| 10. Buy | 7.1% | 3.3% | 10.8% | 2.662 | 0.103 |
| Action Category | Entire Sample (N = 126) | 6 Mon–1 yr (n = 4) | 1–3 yr (n = 37) | >3 yr (n = 85) | χ2 | p |
|---|---|---|---|---|---|---|
| 1. Tell | 43.7% | 75.0% | 45.9% | 41.2% | 1.889 | 0.389 |
| 2. Ask | 46.8% | 100% | 43.2% | 45.9% | 4.763 | 0.092 |
| 3. Check | 47.6% | 0.0% | 62.2% | 43.5% | 7.344 | 0.025 |
| 4. Avoid | 30.2% | 25.0% | 43.2% | 24.7% | 4.258 | 0.119 |
| 5. Take interest | 17.5% | 50.0% | 18.9% | 15.3% | 3.270 | 0.195 |
| 6. Take | 31.7% | 0.0% | 45.9% | 27.1% | 6.165 | 0.046 |
| 7. Make | 29.4% | 50% | 21.6% | 31.8% | 2.127 | 0.345 |
| 8. Collaborate | 9.5% | 0.0% | 16.2% | 7.1% | 2.944 | 0.230 |
| 9. Read | 21.4% | 25.0% | 18.9% | 22.4% | 0.212 | 0.899 |
| 10. Buy | 7.1% | 0.0% | 8.1% | 7.1% | 0.361 | 0.835 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Meyer, S. Promoting Effective Self-Management of the Gluten-Free Diet: Children’s and Adolescents’ Self-Generated Do’s and Don’ts. Int. J. Environ. Res. Public Health 2022, 19, 14051. https://doi.org/10.3390/ijerph192114051
Meyer S. Promoting Effective Self-Management of the Gluten-Free Diet: Children’s and Adolescents’ Self-Generated Do’s and Don’ts. International Journal of Environmental Research and Public Health. 2022; 19(21):14051. https://doi.org/10.3390/ijerph192114051
Chicago/Turabian StyleMeyer, Sonya. 2022. "Promoting Effective Self-Management of the Gluten-Free Diet: Children’s and Adolescents’ Self-Generated Do’s and Don’ts" International Journal of Environmental Research and Public Health 19, no. 21: 14051. https://doi.org/10.3390/ijerph192114051