
Controlled Trial Examining the Strength-Based Grit Wellbeing and Self-Regulation Program for Young People in Residential Settings for Substance Use
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Participants
2.2.1. Setting
2.2.2. Inclusion Criteria
2.2.3. Recruitment and Consent
2.2.4. Sample Size
2.3. Intervention
2.3.1. Six Week Residential Treatment Program
2.3.2. Grit Program
2.3.3. Grit Training, Facilitation, and Fidelity
2.4. Measures
2.4.1. Demographic and Control Measures
2.4.2. Key Primary Outcomes
2.4.3. Other Outcomes
2.5. Procedure
2.6. Data Analysis
3. Results
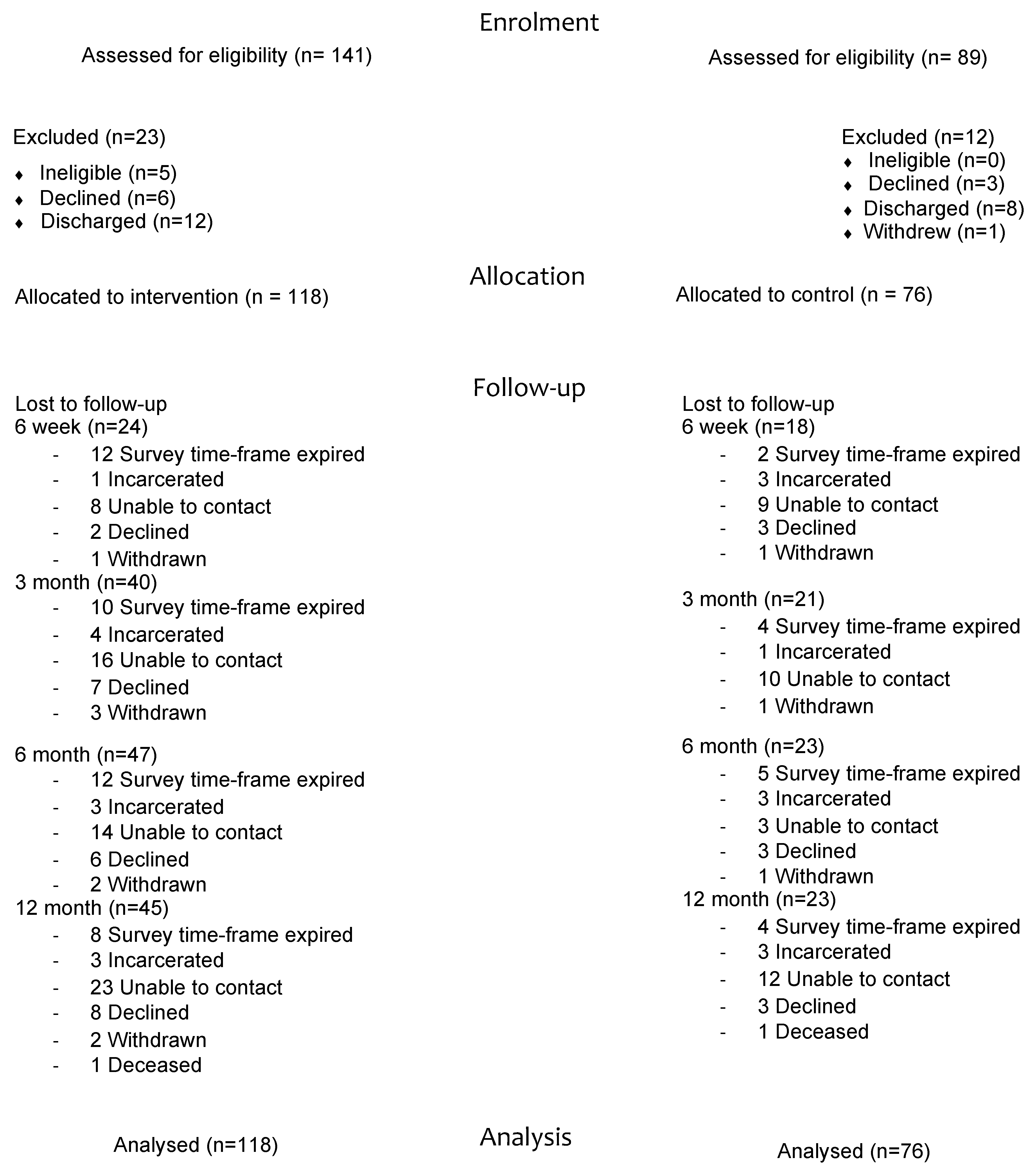
3.1. Participants
3.2. Treatment
3.3. Key Primary Outcomes
Substance Use
3.4. Other Outcomes
3.4.1. Wellbeing
3.4.2. Depression and Anxiety
3.4.3. Vocational Engagement
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Reif, S.; George, P.; Braude, L.; Dougherty, R.H.; Daniels, A.S.; Ghose, S.S.; Delphin-Rittmon, M.E. Residential treatment for individuals with substance use disorders: Assessing the evidence. Psychiatr. Serv. 2014, 65, 301–312. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Constitution of the World Health Organization. 2019. Available online: https://www.who.int/about/governance/constitution (accessed on 31 July 2019).
- de Andrade, D.; Elphinston, R.A.; Quinn, C.; Allan, J.; Hides, L. The effectiveness of residential treatment services for individuals with substance use disorders: A systematic review. Drug Alcohol Depend. 2019, 201, 227–235. [Google Scholar] [CrossRef] [PubMed]
- Witkiewitz, K.; Warner, K.; Sully, B.; Barricks, A.; Stauffer, C.; Thompson, B.L.; Luoma, J.B. Randomized trial comparing mindfulness-based relapse prevention with relapse prevention for women offenders at a residential addiction treatment center. Subst. Use Misuse 2014, 49, 536–546. [Google Scholar] [CrossRef] [PubMed]
- Zoogman, S.; Goldberg, S.B.; Hoyt, W.T.; Miller, L. Mindfulness Interventions with Youth: A Meta-Analysis. Mindfulness 2014, 6, 290–302. [Google Scholar] [CrossRef]
- Davis, J.P.; Berry, D.; Dumas, T.M.; Ritter, E.; Smith, D.C.; Menard, C.; Roberts, B.W. Substance use outcomes for mindfulness based relapse prevention are partially mediated by reductions in stress: Results from a randomized trial. J. Subst. Abus. Treat. 2018, 91, 37–48. [Google Scholar] [CrossRef]
- Shorey, R.C.; Elmquist, J.; Gawrysiak, M.J.; Strauss, C.; Haynes, E.; Anderson, S.; Stuart, G.L. A Randomized Controlled Trial of a Mindfulness and Acceptance Group Therapy for Residential Substance Use Patients. Subst. Use Misuse 2017, 52, 1400–1410. [Google Scholar] [CrossRef]
- Kelly, P.J.; Baker, A.L.; Deane, F.P.; Callister, R.; Collins, C.E.; Oldmeadow, C.; Palazzi, K.L.; Townsend, C.J.; Ingram, I.; Keane, C.A.; et al. Healthy recovery: A stepped wedge cluster randomised controlled trial of a healthy lifestyle intervention for people attending residential alcohol and other drug treatment. Drug Alcohol Depend. 2021, 221, 108557. [Google Scholar] [CrossRef]
- Kelly, P.J.; Baker, A.L.; Deane, F.P.; Kay-Lambkin, F.J.; Bonevski, B.; Tregarthen, J. Prevalence of smoking and other health risk factors in people attending residential substance abuse treatment. Drug Alcohol Rev. 2012, 31, 638–644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vujanovic, A.A.; Meyer, T.D.; Heads, A.M.; Stotts, A.L.; Villarreal, Y.R.; Schmitz, J.M. Cognitive-behavioral therapies for depression and substance use disorders: An overview of traditional, third-wave, and transdiagnostic approaches. Am. J. Drug Alcohol Abus. 2017, 43, 402–415. [Google Scholar] [CrossRef]
- Wolitzky-Taylor, K.; McBeth, J.; Guillot, C.R.; Stone, M.D.; Kirkpatrick, M.G.; Zvolensky, M.J.; Buckner, J.D.; Leventhal, A.M. Transdiagnostic processes linking anxiety symptoms and substance use problems among adolescents. J. Addict. Dis. 2016, 35, 266–277. [Google Scholar] [CrossRef]
- Aldao, A.; Gee, D.G.; De Los Reyes, A.; Seager, I. Emotion regulation as a transdiagnostic factor in the development of internalizing and externalizing psychopathology: Current and future directions. Dev. Psychopathol. 2016, 28 Pt 1, 927–946. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eaton, N.R.; Rodriguez-Seijas, C.; Carragher, N.; Krueger, R.F. Transdiagnostic factors of psychopathology and substance use disorders: A review. Soc. Psychiatry Psychiatr. Epidemiol. 2015, 50, 171–182. [Google Scholar] [CrossRef] [PubMed]
- Sloan, E.; Hall, K.; Moulding, R.; Bryce, S.; Mildred, H.; Staiger, P.K. Emotion regulation as a transdiagnostic treatment construct across anxiety, depression, substance, eating and borderline personality disorders: A systematic review. Clin. Psychol. Rev. 2017, 57, 141–163. [Google Scholar] [CrossRef]
- Stanton, K.; Rozek, D.C.; Stasik-O’Brien, S.M.; Ellickson-Larew, S.; Watson, D. A transdiagnostic approach to examining the incremental predictive power of emotion regulation and basic personality dimensions. J. Abnorm. Psychol. 2016, 125, 960–975. [Google Scholar] [CrossRef] [Green Version]
- Chan, A.-W.; Tetzlaff, J.M.; Altman, D.G.; Laupacis, A.; Gøtzsche, P.C.; Karmela, K.; Hróbjartsson, A.; Mann, H.; Dickersin, K.; Berlin, J.A.; et al. SPIRIT 2013 statement: Defining standard protocol items for clinical trials. Ann. Intern. Med. 2013, 158, 200–207. [Google Scholar] [CrossRef] [Green Version]
- Eysenbach, G.; CONSORT-EHEALTH Group. CONSORT-EHEALTH: Improving and standardizing evaluation reports of Web-based and mobile health interventions. J. Med. Internet Res. 2011, 13, e126. [Google Scholar] [CrossRef] [Green Version]
- Dingle, G.A.; da Costa Neves, D.; Alhadad, S.S.J.; Hides, L. Individual and interpersonal emotion regulation among adults with substance use disorders and matched controls. Br. J. Clin. Psychol. 2018, 57, 186–202. [Google Scholar] [CrossRef] [PubMed]
- Newby, J.M.; Twomey, C.; Yuan Li, S.S.; Andrews, G. Transdiagnostic computerised cognitive behavioural therapy for depression and anxiety: A systematic review and meta-analysis. J. Affect. Disord. 2016, 199, 30–41. [Google Scholar] [CrossRef]
- Reinholt, N.; Krogh, J. Efficacy of Transdiagnostic Cognitive Behaviour Therapy for Anxiety Disorders: A Systematic Review and Meta-Analysis of Published Outcome Studies. Cogn. Behav. Ther. 2014, 43, 171–184. [Google Scholar] [CrossRef]
- Norton, P.J.; Paulus, D.J. Toward a Unified Treatment for Emotional Disorders: Update on the Science and Practice. Behav. Ther. 2016, 47, 854–868. [Google Scholar] [CrossRef]
- Chiesa, A.; Serretti, A. Are Mindfulness-Based Interventions Effective for Substance Use Disorders? A Systematic Review of the Evidence. Subst. Use Misuse 2014, 49, 492–512. [Google Scholar] [CrossRef] [PubMed]
- Keyes, C.L. Mental illness and/or mental health? Investigating axioms of the complete state model of health. J. Consult. Clin. Psychol. 2005, 73, 539–548. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tse, S.; Tsoi, E.W.; Hamilton, B.; O’Hagan, M.; Shepherd, G.; Slade, M.; Whitley, R.; Petrakis, M. Uses of strength-based interventions for people with serious mental illness: A critical review. Int. J. Soc. Psychiatry 2016, 62, 281–291. [Google Scholar] [CrossRef] [PubMed]
- Niemiec, R.M. Mindful living: Character strengths interventions as pathways for the five mindfulness trainings. Int. J. Wellbeing 2012, 2, 22–33. [Google Scholar] [CrossRef] [Green Version]
- Hides, L.; Quinn, C. The RAW Wellbeing Program for Adolescents at Risk of Disengaging from Education and Training for at-Risk Adolescents; Education Horizon Research Grant Scheme, Department of Education, Queensland Government: Brisbane, Australia, 2017. [Google Scholar]
- Boutron, I.; Moher, D.; Altman, D.; Schulz, K.; Ravaud, P. Extending the CONSORT statement to randomized trials of nonpharmacologic treatment: Explanation and elaboration. Ann. Intern. Med. 2008, 148, 295–309. [Google Scholar] [CrossRef]
- Humeniuk, R.; Ali, R.; Babor, T.F.; Farrell, M.; Formigoni, M.L.; Jittiwutikarn, J.; de Lacerda, R.B.; Ling, W.; Marsden, J.; Monteiro, M.; et al. Validation of the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST). Addiction 2008, 103, 1039–1047. [Google Scholar] [CrossRef]
- Raymond, I. The Rock and Water program: Empowering youth workers and clients. Youth Stud. Aust. 2005, 24, 34–39. [Google Scholar]
- Ykema, F. The Rock and Water Perspective: Psychophysical Training for Boys (Theory Booklet); Gadaku Institute: Schagen, The Netherlands, 2002. [Google Scholar]
- Bowen, S.; Chawla, N.; Marlatt, G.A. Mindfulness-Based Relapse Prevention for Addictive Behaviors: A Clinician’s Guide; Guilford Press: New York, NY, USA, 2011. [Google Scholar]
- Roos, C.; Kirouac, M.; Stein, E.; Wilson, A.; Bowen, S.; Witkiewitz, K. An open trial of rolling admission mindfulness-based relapse prevention (Rolling MBRP): Feasibility, acceptability, dose-response relations, and mechanisms. Mindfulness 2019, 10, 1062–1073. [Google Scholar] [CrossRef]
- Bentley, S.V.; Greenaway, K.H.; Haslam, S.A.; Cruwys, T.; Steffens, N.K.; Haslam, C.; Cull, B. Social identity mapping online. J. Personal. Soc. Psychol. 2020, 118, 213–241. [Google Scholar] [CrossRef]
- Best, D.; Haslam, C.; Staiger, P.; Dingle, G.; Savic, M.; Bathish, R.; Mackenzie, J.; Beckwith, M.; Lubman, D.I. Social networks and recovery (SONAR): Characteristics of a longitudinal outcome study in five therapeutic communities in Australia. Ther. Communities Int. J. Ther. Communities 2016, 37, 131–139. [Google Scholar] [CrossRef] [Green Version]
- Cruwys, T.; Steffens, N.K.; Haslam, S.A.; Haslam, C.; Jetten, J.; Dingle, G.A. Social Identity Mapping: A procedure for visual representation and assessment of subjective multiple group memberships. Br. J. Soc. Psychol. 2016, 55, 613–642. [Google Scholar] [CrossRef] [PubMed]
- Dingle, G.A.; Ingram, I.; Haslam, C.; Kelly, P.J. Taking Social Identity into Practice. In Handbook of Alcohol Use and Abuse; Frings, D., Ed.; Elsevier: Amsterdam, The Netherlands, 2020. [Google Scholar]
- Haslam, C.; Cruwys, T.; Chang, M.X.L.; Bentley, S.V.; Haslam, S.A.; Dingle, G.A.; Jetten, J. Groups 4 Health Reduces Loneliness and Social Anxiety in Adults With Psychological Distress: Findings From a Randomized Controlled Trial. J. Consult. Clin. Psychol. 2019, 87, 787–801. [Google Scholar] [CrossRef] [PubMed]
- Haslam, C.; Cruwys, T.; Haslam, S.A.; Dingle, G.; Chang, M.X. Groups 4 Health: Evidence that a social-identity intervention that builds and strengthens social group membership improves mental health. J. Affect. Disord. 2016, 194, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Mawson, E.; Best, D.; Beckwith, M.; Dingle, G.A.; Lubman, D.I. Social identity, social networks and recovery capital in emerging adulthood: A pilot study. Subst. Abus. Treat. Prev. Policy 2015, 10, 45. [Google Scholar] [CrossRef] [Green Version]
- Hayes, S.C.; Strosahl, K.D.; Wilson, K.G. Acceptance and Commitment Therapy an Experiential Approach to Behavior Change; The Guilford Press: New York, NY, USA, 1999. [Google Scholar]
- Harris, R. ACT Made Simple: An Easy-To-Read Primer on Acceptance and Commitment Therapy; New Harbinger: Oakland, CA, USA, 2009. [Google Scholar]
- Dingle, G.A.; Carter, N.A. Smoke into Sound: A pilot randomised controlled trial of a music cravings management program for chronic smokers attempting to quit. Music. Sci. 2017, 21, 151–177. [Google Scholar] [CrossRef]
- Dingle, G.A.; Hodges, J.; Kunde, A. Tuned In emotion regulation program using music listening: Effectiveness for adolescents in educational settings. Front. Psychol. 2016, 7, 859. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hides, L.; Dingle, G.; Quinn, C.; Stoyanov, S.R.; Zelenko, O.; Tjondronegoro, D.; Johnson, D.; Cockshaw, W.; Kavanagh, D.J. Efficacy and Outcomes of a Music-Based Emotion Regulation Mobile App in Distressed Young People: Randomized Controlled Trial. JMIR mHealth uHealth 2019, 7, e11482. [Google Scholar] [CrossRef] [Green Version]
- Bartholomew, N.G.; Simpson, D.D.; Chatham, L.R. Straight Ahead: Transition Skills for Recovery. A Training Manual from the TCU/DATAR Project. 1993. Available online: https://ibr.tcu.edu/wp-content/uploads/2021/08/samanual-with-key_AA.pdf (accessed on 5 September 2022).
- Prins, A.; Bovin, M.J.; Smolenski, D.J.; Marx, B.P.; Kimerling, R.; Jenkins-Guarnieri, M.A.; Kaloupek, D.G.; Schnurr, P.P.; Kaiser, A.P.; Leyva, Y.E.; et al. The Primary Care PTSD Screen for DSM-5 (PC-PTSD-5): Development and Evaluation Within a Veteran Primary Care Sample. J. Gen. Intern. Med. 2016, 31, 1206–1211. [Google Scholar] [CrossRef] [Green Version]
- van Dam, D.; Ehring, T.; Vedel, E.; Emmelkamp, P.M. Validation of the Primary Care Posttraumatic Stress Disorder screening questionnaire (PC-PTSD) in civilian substance use disorder patients. J. Subst. Abus. Treat. 2010, 39, 105–113. [Google Scholar] [CrossRef]
- Degenhardt, L.; Hall, W.; Korten, A.; Jablensky, A. Use of a Brief Screening Instrument for Psychosis: Results of an ROC Analysis; National Drug and Alcohol Research Centre: Sydney, Australia, 2005. [Google Scholar]
- WHO ASSIST Working Group. The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): Development, reliability and feasibility. Addiction 2002, 97, 1183–1194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Newcombe, D.A.; Humeniuk, R.E.; Ali, R. Validation of the World Health Organization Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): Report of results from the Australian site. Drug Alcohol Rev. 2005, 24, 217–226. [Google Scholar] [CrossRef]
- Hides, L.; Quinn, C.; Stoyanov, S.; Cockshaw, W.; Mitchell, T.; Kavanagh, D.J. Is the mental wellbeing of young Australians best represented by a single, multidimensional or bifactor model? Psychiatry Res. 2016, 241, 1–7. [Google Scholar] [CrossRef] [Green Version]
- Ryan, A.; Holmes, J.; Hunt, V.; Dunlop, A.; Mammen, K.; Holland, R.; Sutton, Y.; Sindhusake, D.; Rivas, G.; Lintzeris, N. Validation and implementation of the Australian Treatment Outcomes Profile in specialist drug and alcohol settings. Drug Alcohol Rev. 2014, 33, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Lowe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donohue, M.C.; Aisen, P.S. Mixed model of repeated measures versus slope models in Alzheimer’s disease clinical trials. J. Nutr. Health Aging 2012, 16, 360–364. [Google Scholar] [CrossRef] [PubMed]
- Mallinckrodt, C.H.; Clark, W.S.; David, S.R. Accounting for dropout bias using mixed-effects models. J. Biopharm. Stat. 2001, 11, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Molenberghs, G.; Thijs, H.; Jansen, I.; Beunckens, C.; Kenward, M.G.; Mallinckrodt, C.; Carroll, R.J. Analyzing incomplete longitudinal clinical trial data. Biostatistics 2004, 5, 445–464. [Google Scholar] [CrossRef]
- Degenhardt, L.; Sara, G.; McKetin, R.; Roxburgh, A.; Dobbins, T.; Farrell, M.; Burns, L.; Hall, W.D. Crystalline methamphetamine use and methamphetamine-related harms in Australia. Drug Alcohol Rev. 2017, 36, 160–170. [Google Scholar] [CrossRef]
- Hall, W.D.; Patton, G.; Stockings, E.; Weier, M.; Lynskey, M.; Morley, K.I.; Degenhardt, L. Why young people’s substance use matters for global health. Lancet Psychiatry 2016, 3, 265–279. [Google Scholar] [CrossRef] [Green Version]
- Baker, D.E.; Edmonds, K.A.; Calvert, M.L.; Sanders, S.M.; Bridges, A.J.; Rhea, M.A.; Kosloff, S. Predicting attrition in long-term residential substance use disorder treatment: A modifiable risk factors perspective. Psychol. Serv. 2019, 17, 472–482. [Google Scholar] [CrossRef] [PubMed]
- Mutter, R.; Ali, M.M.; Smith, K.; Strashny, A. Factors associated with substance use treatment completion in residential facilities. Drug Alcohol Depend. 2015, 154, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Allen, R.S.; Olson, B.D. Predicting attrition in the treatment of substance use disorders. Int. J. Ment. Health Addict. 2016, 14, 728–742. [Google Scholar] [CrossRef]
- Eastwood, B.; Peacock, A.; Millar, T.; Jones, A.; Knight, J.; Horgan, P.; Lowden, T.; Willey, P.; Marsden, J. Effectiveness of inpatient withdrawal and residential rehabilitation interventions for alcohol use disorder: A national observational, cohort study in England. J. Subst. Abus. Treat. 2018, 88, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- King, J.; Dow, J.; Stevenson, B. Measuring outcomes for TC clients: Higher Ground Drug Rehabilitation Trust. Ther. Communities Int. J. Ther. Communities 2016, 37, 121–130. [Google Scholar] [CrossRef]
- Malivert, M.; Fatséas, M.; Denis, C.; Langlois, E.; Auriacombe, M. Effectiveness of therapeutic communities: A systematic review. Eur. Addict. Res. 2012, 18, 1–11. [Google Scholar] [CrossRef]
- Rome, A.M.; McCartney, D.; Best, D.; Rush, R. Changes in substance use and risk behaviors one year after treatment: Outcomes associated with a quasi-residential rehabilitation service for alcohol and drug users in Edinburgh. J. Groups Addict. Recovery 2017, 12, 86–98. [Google Scholar] [CrossRef]
- Vanderplasschen, W.; Colpaert, K.; Autrique, M.; Rapp, R.C.; Pearce, S.; Broekaert, E.; Vandevelde, S. Therapeutic communities for addictions: A review of their effectiveness from a recovery-oriented perspective. Sci. World J. 2013, 2013, 427817. [Google Scholar] [CrossRef]
- Toumbourou, J.W.; Stockwell, T.; Neighbors, C.; Marlatt, G.A.; Sturge, J.; Rehm, J. Interventions to reduce harm associated with adolescent substance use. Lancet 2007, 369, 1391–1401. [Google Scholar] [CrossRef]
- Cutcliffe, J.R.; Travale, R.; Richmond, M.M.; Green, T. Considering the Contemporary Issues and Unresolved Challenges Facing Therapeutic Communities for Clients with Alcohol and Substance Abuse. Issues Ment. Health Nurs. 2016, 37, 642–650. [Google Scholar] [CrossRef]


{kind=link}
| Demographics 1 | Total (n = 194) | Intervention (n = 118) | Control (n = 76) | p-Value |
|---|---|---|---|---|
| Age | 27.40 (5.73) | 26.60 (6.04) | 28.61 (4.97) | 0.021 |
| Male | 128 (66.0) | 81 (68.6) | 47 (61.8) | 0.330 |
| Australian born | 193 (90.2) | 108 (91.5) | 67 (89.3) | 0.610 |
| Indigenous | 21 (10.8) | 13 (11.0) | 8 (10.5) | 0.915 |
| Relationship—Single | 152 (78.4) | 92 (78.0) | 60 (78.9) | 0.871 |
| Grade 10 schooling | 106 (54.6) | 67 (56.8) | 39 (51.3) | 0.417 |
| Unemployed | 143 (73.7) | 85 (72.0) | 58 (76.3) | 0.509 |
| Receiving Pension | 159 (82.0) | 92 (78.0) | 67 (88.2) | 0.076 |
| Live with parents/relatives | 82 (42.3) | 51 (43.2) | 31 (40.8) | 0.738 |
| Homeless | 43 (22.2) | 31 (26.3) | 12 (15.8) | 0.084 |
| Have at least one child | 67 (34.5) | 32 (27.1) | 35 (46.1) | 0.007 |
| Primary Drug | 0.754 a | |||
| Methamphetamine | 87 (44.8) | 53 (44.9) | 34 (44.7) | |
| Alcohol | 67 (34.5) | 39 (33.1) | 28 (36.8) | |
| Cannabis | 29 (14.9) | 19 (16.1) | 10 (13.2) | |
| Other | 11 (5.7) | 7 (5.9) | 4 (5.3) | |
| Mental Health | ||||
| PTSD Screen b | 84 (43.3) | 52 (44.1) | 32 (42.1) | 0.834 |
| Psychosis Screen b | 85 (43.8) | 55 (46.6) | 30 (39.5) | 0.381 |
| Depression c | 85 (43.8) | 55 (46.6) | 30 (49.5) | 0.279 |
| Anxiety c | 103 (53.1) | 69 (58.5) | 34 (44.7) | 0.076 |
| Correctional Involvement d | 41 (21.1) | 24 (20.3) | 17 (22.4) | 0.722 |
| Hospitalized d | 61 (31.4) | 34 (28.8) | 27 (35.5) | 0.366 |
| Total n (%) | Intervention n (%) | Control n (%) | p-Value | |
|---|---|---|---|---|
| Early Discharge a | (n = 119) | (n = 74) | (n = 45) | 0.122 |
| Voluntary | 65 (54.60) | 38 (51.40) | 27 (60.00) | |
| Involuntary | 52 (43.70) | 34 (45.90) | 18 (40.00) | |
| Other | 2 (1.60) | 2 (2.70) | 0 (0.00) | |
| 6 weeks | ||||
| Completed 3 weeks a | 138 (71.70) | 79 (66.90) | 59 (77.60) | 0.111 |
| Completed 6 weeks a | 75 (38.70) | 44 (37.30) | 31 (40.80) | 0.625 |
| Average number of days- Residential b | 29.05 (13.66) | 28.29 (13.84) | 30.24 (13.38) | 0.332 |
| 3 months | ||||
| Completed 3 weeks a | 143 (73.70) | 84 (71.2) | 59 (77.6) | 0.321 |
| Completed 6 weeks a | 95 (49.50) | 59 (50.0) | 37 (48.7) | 0.858 |
| Average number of days—Residential b | 37.71 (22.58) | 37.25 (22.87) | 38.41 (22.25) | 0.728 |
| Re-admissions a | 68 (35.0) | 54 (45.8) | 14 (18.4) | 0.001 |
| New Admission a Episodes | 14 (7.22) | 7 (5.93) | 7 (9.21) | 0.389 |
| 12 months | ||||
| Average number of days—Residential c | 43.90 (31.89) | 46.22 (35.76) | 40.30 (24.50) | 0.598 |
| New Admission Episodes a | 44 (22.68) | 12 (15.79) | 32 (27.12) | 0.066 |
| Baseline | 6 Week | 3 Month | 6 Month | 12 Month | ||
|---|---|---|---|---|---|---|
| M (SE) | M (SE) | M (SE) | M (SE) | M (SE) | ||
| Global ASSIST | Grit | 130.48 (5.39) | - | 76.86 (5.98) | 64.89 (6.52) | 77.17 (6.40) |
| Control | 110.57 (6.47) | - | 75.27 (7.22) | 61.38 (7.81) | 64.14 (7.65) | |
| Total | 120.52 (4.24) | - | 76.06 (4.70) | 63.13 (5.09) | 70.65 (5.00) | |
| Total ASSIST | Grit | 108.88 (4.93) | - | 55.91 (5.50) | 41.10 (6.02) | 53.07 (5.94) |
| Control | 90.54 (5.93) | - | 56.34 (6.66) | 39.20 (7.16) | 41.96 (7.05) | |
| Total | 99.71 (3.88) | - | 56.12 (4.32) | 40.15 (4.68) | 47.51 (4.62) | |
| Alcohol ASSIST | Grit | 17.49 (1.21) | - | 9.31 (1.35) | 11.12 (1.46) | 12.5 (1.46) |
| Control | 18.66 (1.46) | - | 10.65 (1.63) | 9.8 (1.72) | 12.19 (1.72) | |
| Total | 18.07 (0.95) | - | 9.98 (1.06) | 10.46 (1.13) | 12.35 (1.13) | |
| Methamphetamine ASSIST | Grit | 22.66 (1.28) | - | 10.04 (1.40) | 9.92 (1.51) | 11.98 (1.54) |
| Control | 17.35 (1.54) | - | 10.39 (1.69) | 9.38 (1.79) | 9.12 (1.84) | |
| Total | 20.01 (1.01) | - | 10.22 (1.10) | 9.65 (1.17) | 10.55 (1.20) | |
| Cannabis ASSIST | Grit | 15.54 (1.15) | - | 8.24 (1.26) | 8.64 (1.30) | 10.16 (1.34) |
| Control | 10.59 (1.38) | - | 8.48 (1.51) | 7.55 (1.54) | 7.37 (1.60) | |
| Total | 13.07 (0.91) | - | 8.36 (0.99) | 8.10 (1.02) | 8.76 (1.05) | |
| Wellbeing (MHC-SF) | Grit | 33.52 (1.69) | 45.84 (1.82) | 46.94 (1.93) | 42.75 (2.17) | 42.59 (2.07) |
| Control | 36.86 (2.06) | 50.22 (2.28) | 44.86 (2.36) | 40.50 (2.47) | 41.15 (2.41) | |
| Total | 35.19 (1.34) | 48.03 (1.46) | 45.90 (1.52) | 41.62 (1.65) | 41.87 (1.59) | |
| Depression (PHQ-9) | Grit | 14.76 (0.73) | 9.13 (0.77) | 8.47 (0.79) | 8.60 (0.85) | 8.90 (0.85) |
| Control | 12.32 (0.87) | 7.32 (0.95) | 7.36 (0.98) | 8.42 (0.98) | 8.45 (1.00) | |
| Total | 13.54 (0.57) | 8.23 (0.61) | 7.91 (0.63) | 8.51 (0.65) | 8.67 (0.66) | |
| Anxiety (GAD-7) | Grit | 12.46 (6.34) | 8.63 (6.55) | 6.66 (6.00) | 6.40 (6.36) | 6.35 (5.79) |
| Control | 10.18 (6.51) | 6.25 (5.54) | 6.56 (6.58) | 7.36 (5.88) | 7.74 (6.37) | |
| Total | 11.58 (6.48) | 7.76 (6.26) | 6.62 (6.21) | 6.81 (6.14) | 6.90 (6.03) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quinn, C.A.; Walter, Z.C.; de Andrade, D.; Dingle, G.; Haslam, C.; Hides, L. Controlled Trial Examining the Strength-Based Grit Wellbeing and Self-Regulation Program for Young People in Residential Settings for Substance Use. Int. J. Environ. Res. Public Health 2022, 19, 13835. https://doi.org/10.3390/ijerph192113835
Quinn CA, Walter ZC, de Andrade D, Dingle G, Haslam C, Hides L. Controlled Trial Examining the Strength-Based Grit Wellbeing and Self-Regulation Program for Young People in Residential Settings for Substance Use. International Journal of Environmental Research and Public Health. 2022; 19(21):13835. https://doi.org/10.3390/ijerph192113835
Chicago/Turabian StyleQuinn, Catherine A., Zoe C. Walter, Dominique de Andrade, Genevieve Dingle, Catherine Haslam, and Leanne Hides. 2022. "Controlled Trial Examining the Strength-Based Grit Wellbeing and Self-Regulation Program for Young People in Residential Settings for Substance Use" International Journal of Environmental Research and Public Health 19, no. 21: 13835. https://doi.org/10.3390/ijerph192113835