
Experience with Obese Patients Followed via Telemedicine in a Latin American Tertiary Care Medical Center
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Context
2.2. Overview of the “Siempre” Teleconsultation Program
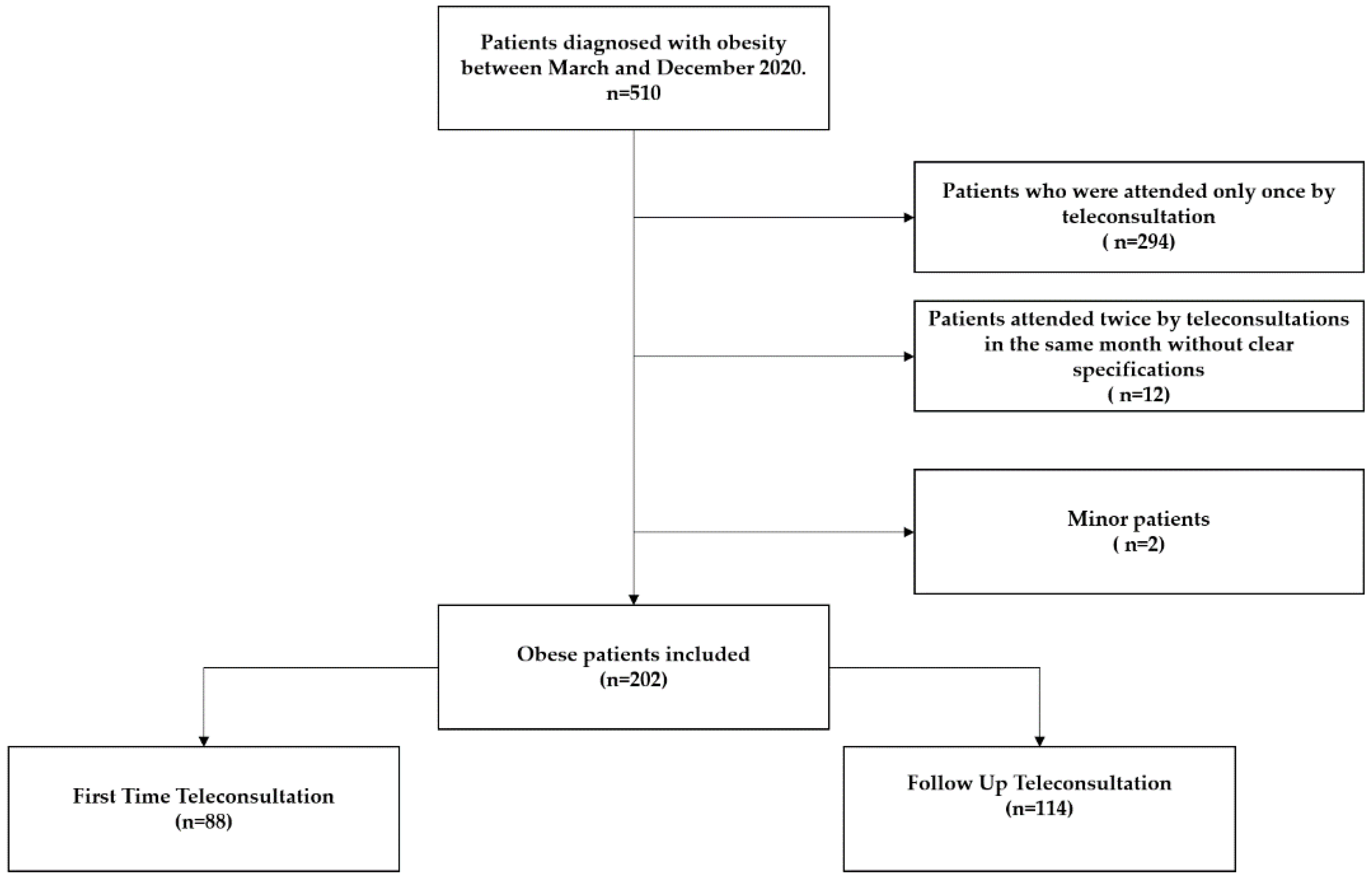
2.3. Population and Sample Size
2.4. Variables
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. Principal Findings
4.2. Results in Context
4.3. Limitations and Strengths
4.4. Future Implications
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chooi, Y.C.; Ding, C.; Magkos, F. The epidemiology of obesity. Metab. Clin. Exp. 2019, 92, 6–10. [Google Scholar] [CrossRef] [PubMed]
- ENSIN: Encuesta Nacional de Situación Nutricional|Portal ICBF—Instituto Colombiano de Bienestar Familiar ICBF. Available online: https://www.icbf.gov.co/bienestar/nutricion/encuesta-nacional-situacion-nutricional#ensin3 (accessed on 17 January 2021).
- Wang, Y.C.; McPherson, K.; Marsh, T.; Gortmaker, S.L.; Brown, M. Health and economic burden of the projected obesity trends in the USA and the UK. Lancet 2011, 378, 815–825. [Google Scholar] [CrossRef]
- Aune, D.; Sen, A.; Prasad, M.; Norat, T.; Janszky, I.; Tonstad, S.; Romundstad, P.; Vatten, L.J. BMI and All Cause Mortality: Systematic Review and Non-Linear Dose-Response Meta-Analysis of 230 Cohort Studies with 3.74 Million Deaths among 30.3 Million Participants; BMJ Publishing Group: London, UK, 2016; Volume 353. [Google Scholar]
- Chin, S.O.; Keum, C.; Woo, J.; Park, J.; Choi, H.J.; Woo, J.-T.; Rhee, S.Y. Successful weight reduction and maintenance by using a smartphone application in those with overweight and obesity. Sci. Rep. 2016, 6, 34563. [Google Scholar] [CrossRef] [PubMed]
- Minsky, N.; Pachter, D.; Zacay, G.; Chishlevitz, N.; Ben-Hamo, M.; Weiner, D.; Segal-Lieberman, G. Managing obesity in lockdown: Survey of health behaviors and telemedicine. Nutrients 2021, 13, 1359. [Google Scholar] [CrossRef]
- Flaudias, V.; Iceta, S.; Zerhouni, O.; Rodgers, R.F.; Billieux, J.; Llorca, P.-M.; Boudesseul, J.; de Chazeron, I.; Romo, L.; Maurage, P.; et al. COVID-19 pandemic lockdown and problematic eating behaviors in a student population. J. Behav. Addict. 2020, 9, 826–835. [Google Scholar] [CrossRef]
- Giorgino, F.; Bhana, S.; Czupryniak, L.; Dagdelen, S.; Galstyan, G.R.; Janež, A.; Lalić, N.; Nouri, N.; Rahelić, D.; Stoian, A.P.; et al. Management of patients with diabetes and obesity in the COVID-19 era: Experiences and learnings from South and East Europe, the Middle East, and Africa. Diabetes Res. Clin. Pract. 2021, 172, 108617. [Google Scholar] [CrossRef]
- Shapiro, S.B.; Lipschitz, N.; Kemper, N.; Zuccarello, M.; Breen, J.T.; Pensak, M.L.; Samy, R.N. Early Experience With Telemedicine in Patients Undergoing Otologic/Neurotologic Procedures. Otol. Neurotol. 2020, 41, e1154–e1157. [Google Scholar] [CrossRef]
- Williams, A.M.; Bhatti, U.F.; Alam, H.B.; Nikolian, V.C. The role of telemedicine in postoperative care. Mhealth 2018, 4, 11. [Google Scholar] [CrossRef]
- Kahan, S.; Look, M.; Fitch, A. The benefit of telemedicine in obesity care. Obesity 2022, 30, 577–586. [Google Scholar] [CrossRef]
- Kichloo, A.; Albosta, M.; Dettloff, K.; Wani, F.; El-Amir, Z.; Singh, J.; Aljadah, M.; Chakinala, R.C.; Kanugula, A.K.; Solanki, S.; et al. Telemedicine, the current COVID-19 pandemic and the future: A narrative review and perspectives moving forward in the USA. Fam. Med. Community Health 2020, 8, e000530. [Google Scholar] [CrossRef]
- Napolitano, M.A.; Hayes, S.; Bennett, G.G.; Ives, A.K.; Foster, G.D. Using facebook and text messaging to deliver a weight loss program to college students. Obesity 2013, 21, 25–31. [Google Scholar] [CrossRef] [PubMed]
- Butryn, M.L.; Webb, V.; Wadden, T.A. Behavioral treatment of obesity. Psychiatr. Clin. N. Am. 2011, 34, 841–859. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Xue, H.; Huang, Y.; Huang, L.; Zhang, D. REVIEW A Systematic Review of Application and Effectiveness of mHealth Interventions for Obesity and Diabetes Treatment and Self-Management. Adv. Nutr. Int. Rev. J. 2017, 8, 449–462. [Google Scholar] [CrossRef] [PubMed]
- Hutchesson, M.J.; Rollo, M.E.; Krukowski, R.; Ells, L.; Harvey, J.; Morgan, P.J.; Callister, R.; Plotnikoff, R.; Collins, C.E. eHealth interventions for the prevention and treatment of overweight and obesity in adults: A systematic review with meta-analysis. Obes. Rev. 2015, 16, 376–392. [Google Scholar] [CrossRef]
- Allen, J.K.; Stephens, J.; Dennison Himmelfarb, C.R.; Stewart, K.J.; Hauck, S. Randomized controlled pilot study testing use of smartphone technology for obesity treatment. J. Obes. 2013, 2013, 151597. [Google Scholar] [CrossRef]
- England, T.N. Reduction of the incidence of type 2 diabetes with lifestyle intervention or metformin. Int. Urol. Nephrol. 2002, 34, 162–163. [Google Scholar]
- Curry, S.J.; Krist, A.H.; Owens, D.K.; Barry, M.J.; Caughey, A.B.; Davidson, K.W.; Doubeni, C.A.; Epling, J.W.; Grossman, D.C.; Kemper, A.R.; et al. Behavioral weight loss interventions to prevent obesity-relatedmorbidity and mortality in adults US preventive services task force recommendation statement. J. Am. Med. Assoc. 2018, 320, 1163–1171. [Google Scholar]
- Kelly, D.M.; Jones, T.H. Testosterone and obesity. Obes. Rev. 2015, 16, 581–606. [Google Scholar] [CrossRef]
- Trasolini, R.; Cox, B.; Galts, C.; Yoshida, E.M.; Marquez, V. Elevated serum ferritin in non-alcoholic fatty liver disease is not predictive of fibrosis. Can. Liver J. 2022, 5, 152–159. [Google Scholar] [CrossRef]
- Bursac, Z.; Gauss, C.H.; Williams, D.K.; Hosmer, D.W. Purposeful selection of variables in logistic regression. Source Code Biol. Med. 2008, 3, 17. [Google Scholar] [CrossRef]
- Halpern, B.; Louzada, M.L.D.C.; Aschner, P.; Gerchman, F.; Brajkovich, I.; Faria-Neto, J.R.; Polanco, F.E.; Montero, J.; Juliá, S.M.M.; Lotufo, P.A.; et al. Obesity and COVID-19 in Latin America: A tragedy of two pandemics—Official document of the Latin American Federation of Obesity Societies. Obes. Rev. 2021, 22, e13165. [Google Scholar] [CrossRef] [PubMed]
- Mechanick, J.I.; Hurley, D.L.; Garvey, W.T. Adiposity-based chronic disease as a new diagnostic term: The American association of clinical endocrinologists and American college of endocrinology position statement. Endocr. Pract. 2017, 23, 372–378. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang-Selfridge, A.A.; Dennis, J.F. Management of obesity using Telemedicine during the COVID-19 pandemic. Mol. Med. 2021, 118, 442. [Google Scholar]
- Alencar, M.K.; Johnson, K.; Mullur, R.; Gray, V.; Gutierrez, E.; Korosteleva, O. The efficacy of a telemedicine-based weight loss program with video conference health coaching support. J. Telemed. Telecare 2019, 25, 151–157. [Google Scholar] [CrossRef]
- Johnson, K.E.; Alencar, M.K.; Coakley, K.E.; Swift, D.L.; Cole, N.H.; Mermier, C.M.; Kravitz, L.; Amorim, F.T.; Gibson, A.L. Telemedicine-Based Health Coaching Is Effective for Inducing Weight Loss and Improving Metabolic Markers. Telemed. e-Health 2019, 25, 85–92. [Google Scholar] [CrossRef] [PubMed]
- Forkmann, K.; Roth, L.; Mehl, N. Introducing zanadio—A Digitalized, Multimodal Program to Treat Obesity. Nutrients 2022, 14, 3172. [Google Scholar] [CrossRef]
- Evans, W.D.; Abroms, L.C.; Broniatowski, D.; Napolitano, M.A.; Arnold, J.; Ichimiya, M.; Agha, S. Digital Media for Behavior Change: Review of an Emerging Field of Study. Int. J. Environ. Res. Public Health 2022, 19, 9129. [Google Scholar] [CrossRef]
- World Health Organization. Global Strategy on Digital Health 2020–2025. 2021. Available online: http://apps.who.int/bookorders (accessed on 24 September 2022).
- Patalano, R.; De Luca, V.; Vogt, J.; Birov, S.; Giovannelli, L.; Carruba, G.; Pivonello, C.; Stroetmann, V.; Triassi, M.; Colao, A.; et al. An Innovative Approach to Designing Digital Health Solutions Addressing the Unmet Needs of Obese Patients in Europe. Int. J. Environ. Res. Public Health 2021, 18, 579. [Google Scholar] [CrossRef]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS Guideline for the Management of Overweight and Obesity in Adults: HHS Public Access Preamble and Transition to ACC/AHA Guidelines to Reduce Cardiovascular Risk. Circulation 2014, 129, S102–S138. Available online: http://circ.AHAjournals.org/lookup/suppl/doi:10.1161/01.cir.0000437739.71477.ee/-/DC1 (accessed on 23 August 2022).
- Wadden, T.A.; Webb, V.L.; Moran, C.H.; Bailer, B.A. Lifestyle modification for obesity: New developments in diet, physical activity, and behavior therapy. Circulation 2012, 125, 1157–1170. [Google Scholar] [CrossRef]
- Frühbeck, G.; Busetto, L.; Dicker, D.; Yumuk, V.; Goossens, G.H.; Hebebrand, J.; Halford, J.G.; Farpour-Lambert, N.J.; Blaak, E.E.; Woodward, E.; et al. The ABCD of obesity: An EASO position statement on a diagnostic term with clinical and scientific implications. Obes. Facts 2019, 12, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Bhardwaj, N.N.; Wodajo, B.; Gochipathala, K.; Paul, D.P., III; Coustasse, A. Can mHealth Revolutionize the Way We Manage Adult Obesity? Springer: Berlin/Heidelberg, Germany, 2017. [Google Scholar]
- Ufholz, K.; Bhargava, D. A Review of Telemedicine Interventions for Weight Loss. Curr. Cardiovasc. Risk Rep. 2021, 15, 17. [Google Scholar] [CrossRef] [PubMed]
- Marra, M.V.; Lilly, C.L.; Nelson, K.R.; Woofter, D.R.; Malone, J. A Pilot Randomized Controlled Trial of a Telenutrition Weight Loss Intervention in Middle-Aged and Older Men with Multiple Risk Factors for Cardiovascular Disease. Nutrients 2019, 11, 229. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| First-Time Group (FG), n = 88 | Follow-Up Group (FUG), n = 114 | |
|---|---|---|
| Number of teleconsultations * | 3 (2–5) | 3 (2–4) |
| Age, years * | 39 (32–45) | 41 (33–52) |
| Health Insurance%) | ||
| Contributive | 11 (12.5) | 11 (9.6) |
| Prepaid | 71 (80.6) | 101 (88.5) |
| Particular | 6 (6.81) | 2 (1.71) |
| Residence (%) | ||
| Urban | 80 (90.9) | 111 (97.3) |
| Rural | 5 (5.6) | - |
| ND | 3 (3.4) | 3 (2.6) |
| Occupation (%) | ||
| Unemployed | 3 (3.4) | 4 (3.5) |
| Employee | 55 (62.5) | 67 (58.7) |
| Independent | 6 (3.4) | 7 (6.1) |
| Home | 3 (3.4) | 6 (5.2) |
| ND | 21 (23.8) | 30 (26.3) |
| School grade | ||
| High school | 1 (1.1) | 2 (1.7) |
| College | 4 (4.5) | 9 (7.8) |
| Postgraduate | 43 (48.8) | 63 (55.2) |
| Analphabet | 10 (11.3) | 5 (4.3) |
| ND | 30 (34.0) | 35 (30.7) |
| Comorbidities (%) | ||
| No | 30 (34.0) | 31 (27.1) |
| Hypertension | 8 (9.0) | 20 (17.5) |
| Diabetes | 2 (2.2) | 6 (5.2) |
| Dyslipidemia | 10 (11.3) | 15 (13.1) |
| Coronary artery disease | - | 1 (0.8) |
| Thyroid disease | 14 (15.9) | 15 (13.1) |
| Fatty liver | 4 (4.5) | 10 (8.7) |
| Physical activity at first teleconsultation (%) | ||
| No | 50 (56.8) | 36 (31.5) |
| Yes | 23 (26.1) | 57 (5) |
| ND | 15 (17.0) | 21 (18.4) |
| Healthy diet at first teleconsultation (%) | ||
| No | 64 (72.7) | 47 (41.2) |
| Yes | 7 (7.9) | 49 (42.9) |
| SD | 17 (19.3) | 18 (15.7) |
| First-Time Group (FG) n = 88 | Follow-Up Group (FUG) n = 114 | |
|---|---|---|
| Weight, kg * | 82 (73–92) | 80.2 (71.25–97) |
| BMI, kg/m2 * | 30.3 (27.5–33.7) | 30.4 (26.55–33.5) |
| ABCD stage (%) | ||
| stage 0 | 43 (48.8) | 36 (31.5) |
| stage 1 | 44 (50) | 72 (63.1) |
| stage 2 | 1 (1.13) | 6 (5.26) |
| Percentage of body fat by DEXA | 44 (40.4–49) | 46.6 (45–48.5) |
| Total fat weight by DEXA, kg | 38 (32–42.5) | 34.5 (31.1–37.95) |
| Android fat/gynoid fat ratio by DEXA | 1.025 (0.8–1.1) | 0.96 (0.9–1) |
| Fasting blood glucose (mg/dL) | 91.6 (84–98) | 91 (85.5–100) |
| LDL colesterol (mg/dL) | 115.25 (97.3–131.5) | 117 (97–139) |
| HDL colesterol (mg/dL) | 48.9 (42–57.9) | 46 (40–57) |
| Triglycerides (mg/dL) | 134 (90–198) | 121 (88–166) |
| Creatinine (mg/dL) | 0.76 (0.6–0.8) | 0.78 (0.68–0.8) |
| Ferritin (ng/mL) | 92.5 (45–185.5) | 94.9 (44.9–222) |
| Glycosylated hemoglobin (%) | 5.4 (5.2–5.6) | 5.4 (5.2–5.6) |
| Uric acid (mg/dL) | 4.65 (3.9–6) | 4.55 (3.7–5.8) |
| Testosterone (only for men) (ng/mL) | 4 (3.98–5.3) | 4.5 (3.9–17) |
| First-Time Group (FG), n = 88 | Follow-Up Group (FUG), n = 114 | |
|---|---|---|
| Weight (kg) | ||
| Value at 3 months | 75 (67.1–81.7) | 73.8 (66–88) |
| Value at 6 months | 72.5 (63–81) | 70.5 (60–83) |
| BMI (kg/m2) | ||
| Value at 3 months | 27.9 (26.1–30.9) | 28 (25.6–31.2) |
| Value at 6 months | 26.6 (24.8–30.3) | 26.35 (24.2–29.2) |
| Fasting blood glucose (mg/dL) | ||
| Value at 3 months | 91.7 (89–105) | 90 (83.5–95) |
| Value at 6 months | 92 (86–98.5) | 89.5 (86–91) |
| LDL cholesterol (mg/dL) | ||
| Value at 3 months | 96 (73–127) | 106 (83–134.3) |
| Value at 6 months | 99.5 (79–116) | 118 (64–135) |
| HDL cholesterol (mg/dL) | ||
| Value at 3 months | 53 (46–62) | 49 (43.25–57.5) |
| Value at 6 months | 45 (41–49) | 51 (42.1–72) |
| Triglycerides (mg/dL) | ||
| Value at 3 months | 92 (88–130) | 119 (93–146) |
| Value at 6 months | 142.5 (109–164) | 97 (86–145) |
| Creatinine (mg/dL) | ||
| Value at 3 months | 0.815 (0.7–0.9) | 0.8 (0.71–0.9) |
| Value at 6 months | 0.77 (0.7–0.9) | 0.8 (0.6–0.8) |
| Ferritin (ng/mL) | ||
| Value at 3 months | 66 (31–133) | 130 (79–249) |
| Value at 6 months | 204 (30.9–625) | 175 (12–268) |
| Glycosylated hemoglobin (%) | ||
| Value at 3 months | 5.4 (5.2–5.8) | 5.42 (5.1–5.5) |
| Value at 6 months | 5.4 (5.37–5.5) | 5.4 (5.2–5.6) |
| Uric acid (mg/dL) | ||
| Value at 3 months | 3.9 (3.6–4.8) | 3.62 (3.38–4.2) |
| Value at 6 months | 4.2 (4.1–4.8) | 4.3 (3.56–4.6) |
| Testosterone (only for men) (ng/mL) | ||
| Value at 3 months | 4.75 (4.75–4.75) | 6.735 (3.07–10.4) |
| Value at 6 months | - | 4.11 (4.11–4.11) |
| Percentage of body fat by DEXA evaluated at last teleconsultation (%) | 41.25 (37–47) | 48 (45–51) |
| Total fat weight by DEXA evaluated at last teleconsultation, kg | 32 (26–34.3) | 42.85 (36–49.7) |
| Android fat/gynoid fat ratio by DEXA at last teleconsultation | 0.965 (0.92–1.06) | 0.96 (0.91–1.01) |
| Physical activity at last teleconsultation (%) | ||
| No | 14 | 10 |
| Yes | 42 | 58 |
| ND | 32 | 46 |
| Healthy diet at last teleconsultation (%) | ||
| No | 9 | 9 |
| Yes | 46 | 63 |
| ND | 33 | 42 |
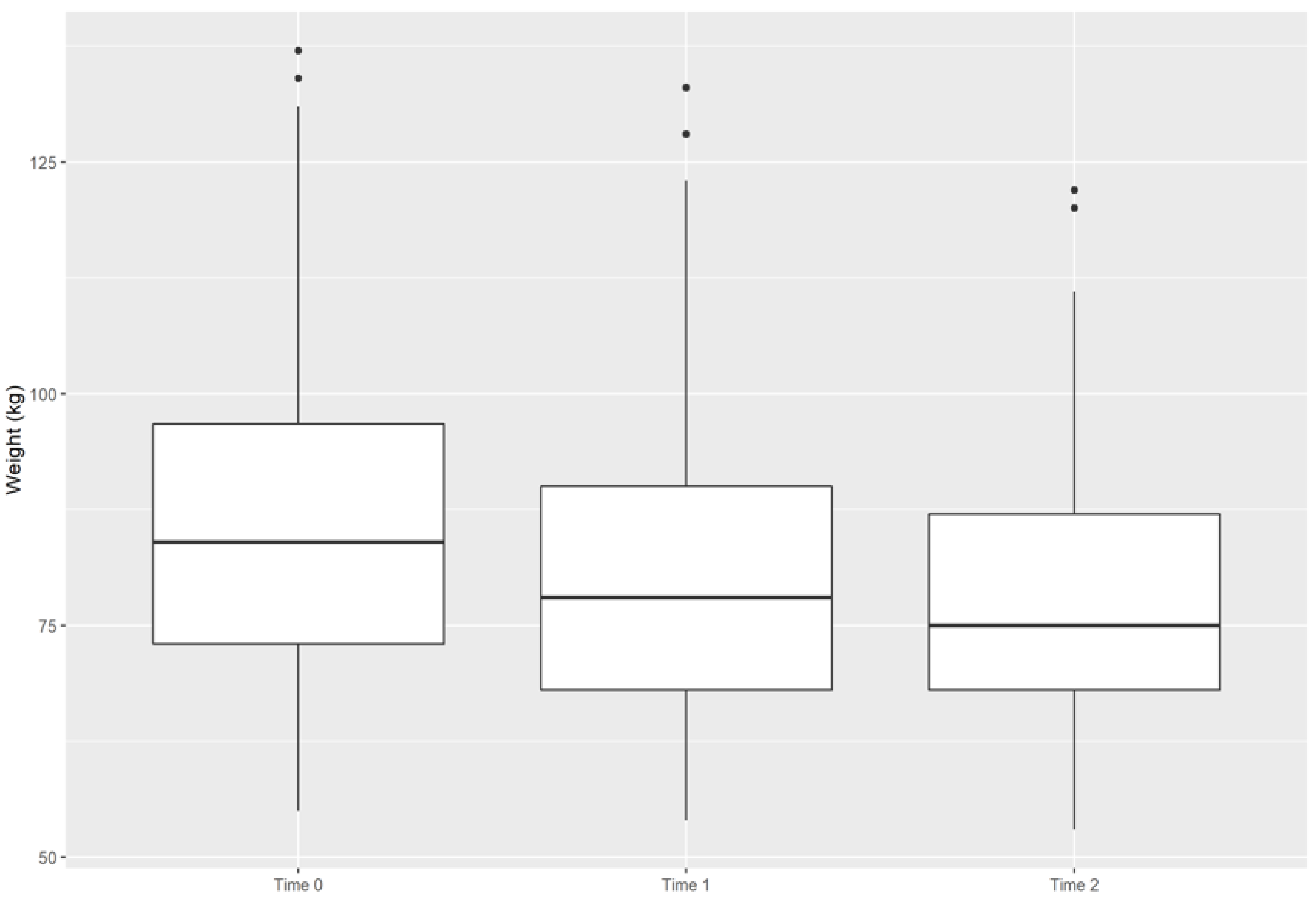
| Time 0, n = 78 | Time 1, n = 63 | Time 2, n = 36 | p Value | |
|---|---|---|---|---|
| General weight, kg | 84.0 (73.0–97.0) | 78.0 (68.0–90.0) | 75.0 (68.0–88.0) | <0.001 |
| Age, years | ||||
| 18–26 | 82.0 (67.0–93.0) | 73.0 (62.0–82.0) | 78.5 (67.5–98.5) | <0.001 |
| 27–59 | 84.0 (73.0–96.0) | 78.5 (69.0–90.0) | 73.0 (68.5–84.5) | <0.001 |
| ≥60 | 98.5 (84–103) | 99.5 (89–102) | 101 (55–104) | >0.99 |
| Type of teleconsultation | ||||
| First time | 83.0 (73.0–90.0) | 78.0 (68.0–85.0) | 71.5 (63.5–83.0) | <0.001 |
| Control | 89.0 (73.0–101.0) | 82.5 (68.0–100.0) | 82.0 (73.0–99.0) | <0.001 |
| Number of teleconsultations | ||||
| 2–3 | 84.0 (73.0–102.0) | 79.0 (68.0–100.0) | 79.0 (69.0–94.0) | <0.001 |
| 4–5 | 84.0 (73.0–91.0) | 75.0 (71.0–87.0) | 72.0 (63.0–82.0) | <0.001 |
| ≥6 | 84.0 (73.0–97.0) | 79.0 (67.5–91.5) | 81.5 (69.0–88.0) | <0.001 |
| ABCD stage | ||||
| 0 | 75.0 (66.0–85.0) | 69.0 (62.0–76.0) | 69.5 (63.0–80.0) | <0.001 |
| 1 | 90.0 (80.0–102.0) | 84.0 (76.0–98.0) | 81.0 (73.0–94.0) | <0.001 |
| 2 | 104.0 (101.0–122.0) | 103.0 (100.0–117.0) | 93.0 (68.5–112.0) | 0.215 |
| Factor | Adjusted Weight Change | p Value |
|---|---|---|
| Time | ||
| Time 0 | - | |
| Time 1 | −4.1 (−5.1–−3.1) | <0.001 |
| Time 2 | −8.6 (−10–−7.3) | <0.001 |
| ABCD stage | ||
| 0 | - | |
| 1 | 15.6 (10.1–21.1) | <0.001 |
| 2 | 28.2 (15.7–40.8) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
López, A.; Escobar, M.F.; Urbano, A.; Alarcón, J.; Libreros-Peña, L.; Martinez-Ruiz, D.M.; Casas, L.Á. Experience with Obese Patients Followed via Telemedicine in a Latin American Tertiary Care Medical Center. Int. J. Environ. Res. Public Health 2022, 19, 12406. https://doi.org/10.3390/ijerph191912406
López A, Escobar MF, Urbano A, Alarcón J, Libreros-Peña L, Martinez-Ruiz DM, Casas LÁ. Experience with Obese Patients Followed via Telemedicine in a Latin American Tertiary Care Medical Center. International Journal of Environmental Research and Public Health. 2022; 19(19):12406. https://doi.org/10.3390/ijerph191912406
Chicago/Turabian StyleLópez, Alejandro, Maria Fernanda Escobar, Alejandra Urbano, Juliana Alarcón, Laura Libreros-Peña, Diana Marcela Martinez-Ruiz, and Luz Ángela Casas. 2022. "Experience with Obese Patients Followed via Telemedicine in a Latin American Tertiary Care Medical Center" International Journal of Environmental Research and Public Health 19, no. 19: 12406. https://doi.org/10.3390/ijerph191912406