
Unraveling the Protective Effects of Cognitive Reserve on Cognition and Brain: A Cross-Sectional Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
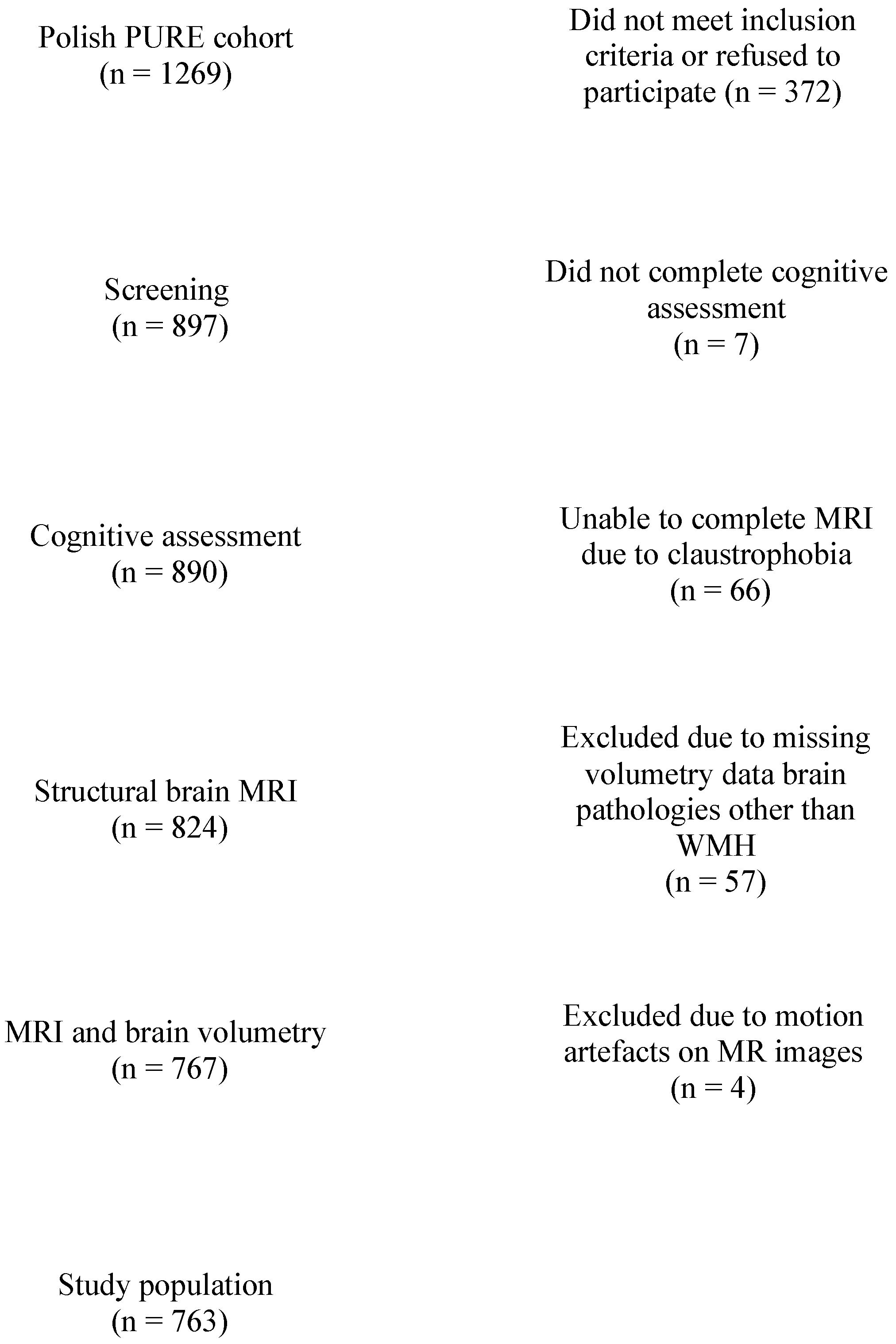
2.1. Population
2.2. Cognitive Reserve and Cognition
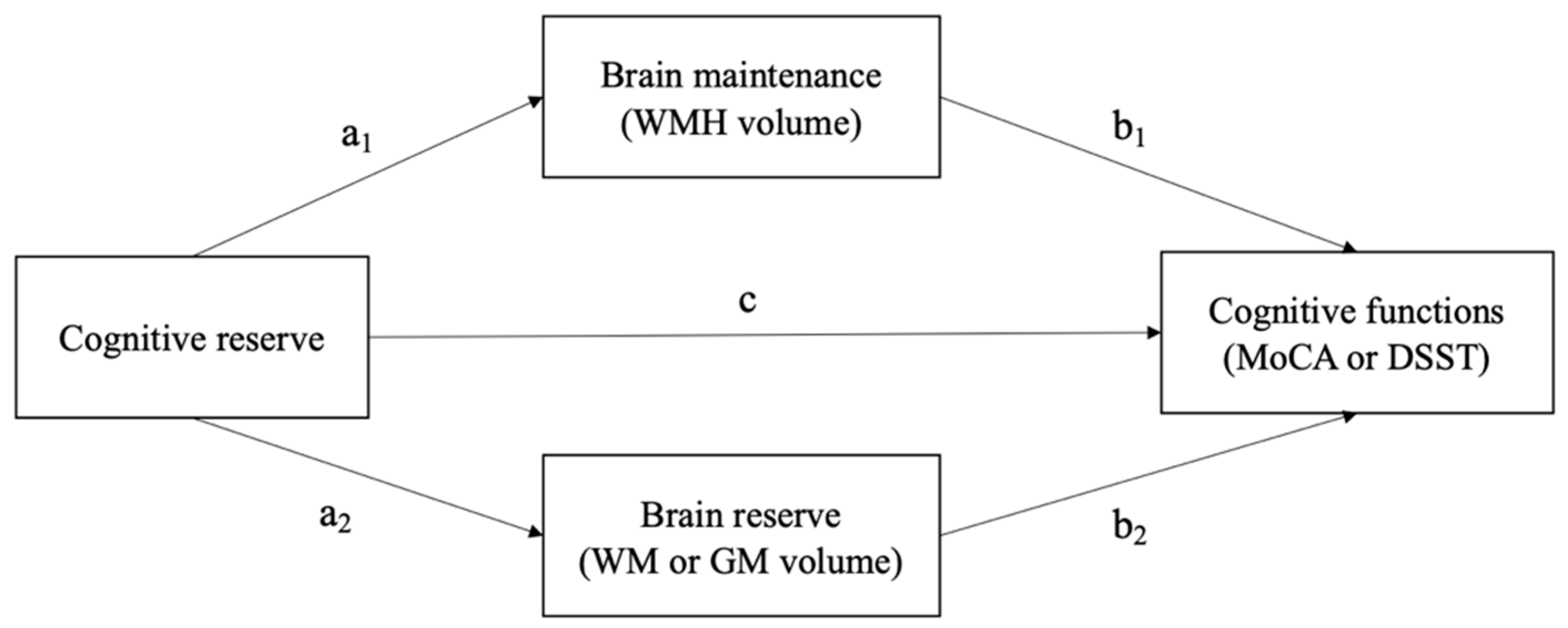
2.3. Brain Reserve and Brain Maintenance
2.4. Ethical Approval
2.5. Statistical Analysis
3. Results
Study Sample
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C.; et al. Dementia Prevention, Intervention, and Care: 2020 Report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Stern, Y. What Is Cognitive Reserve? Theory and Research Application of the Reserve Concept. J. Int. Neuropsychol. Soc. 2002, 8, 448–460. [Google Scholar] [CrossRef] [PubMed]
- Stern, Y.; Arenaza-Urquijo, E.M.; Bartrés-Faz, D.; Belleville, S.; Cantilon, M.; Chetelat, G.; Ewers, M.; Franzmeier, N.; Kempermann, G.; Kremen, W.S.; et al. Whitepaper: Defining and Investigating Cognitive Reserve, Brain Reserve, and Brain Maintenance. Alzheimers. Dement. 2020, 16, 1305–1311. [Google Scholar] [CrossRef] [PubMed]
- Pettigrew, C.; Soldan, A. Defining Cognitive Reserve and Implications for Cognitive Aging. Curr. Neurol. Neurosci. Rep. 2019, 19, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Fleck, J.I.; Kuti, J.; Mercurio, J.; Mullen, S.; Austin, K.; Pereira, O. The Impact of Age and Cognitive Reserve on Resting-State Brain Connectivity. Front. Aging Neurosci. 2017, 9, 392. [Google Scholar] [CrossRef] [PubMed]
- Nyberg, L.; Lövdén, M.; Riklund, K.; Lindenberger, U.; Bäckman, L. Memory Aging and Brain Maintenance. Trends Cogn. Sci. 2012, 16, 292–305. [Google Scholar] [CrossRef] [PubMed]
- Farina, M.; Paloski, L.H.; de Oliveira, C.R.; de Lima Argimon, I.I.; Irigaray, T.Q. Cognitive Reserve in Elderly and Its Connection with Cognitive Performance: A Systematic Review. Ageing Int. 2018, 43, 496–507. [Google Scholar] [CrossRef]
- Jones, R.N.; Manly, J.; Glymour, M.M.; Rentz, D.M.; Jefferson, A.L.; Stern, Y. Conceptual and Measurement Challenges in Research on Cognitive Reserve. J. Int. Neuropsychol. Soc. 2011, 17, 593–601. [Google Scholar] [CrossRef]
- Ji, L.; Pearlson, G.D.; Zhang, X.; Steffens, D.C.; Ji, X.; Guo, H.; Wang, L. Physical Exercise Increases Involvement of Motor Networks as a Compensatory Mechanism during a Cognitively Challenging Task. Int. J. Geriatr. Psychiatry 2018, 33, 1153–1159. [Google Scholar] [CrossRef]
- Reas, E.T.; Laughlin, G.A.; Bergstrom, J.; Kritz-Silverstein, D.; Richard, E.L.; Barrett-Connor, E.; McEvoy, L.K. Lifetime Physical Activity and Late-Life Cognitive Function: The Rancho Bernardo Study. Age Ageing 2019, 48, 241–246. [Google Scholar] [CrossRef]
- Yates, L.A.; Ziser, S.; Spector, A.; Orrell, M. Cognitive Leisure Activities and Future Risk of Cognitive Impairment and Dementia: Systematic Review and Meta-Analysis. Int. Psychogeriatr. 2016, 28, 1791–1806. [Google Scholar] [CrossRef]
- Evans, I.E.M.; Llewellyn, D.J.; Matthews, F.; Bob, W.; Brayne, C.; Clare, L. Social Isolation, Cognitive Reserve, and Cognition in Older People with Mental Health Problems. Alzheimer’s Dement. 2018, 14, 5–6. [Google Scholar] [CrossRef]
- Sauter, J.; Widmer, E.; Ihle, A.; Kliegel, M. The Association of Leisure Activities in Middle Adulthood with Cognitive Performance in Old Age: Social Capital Mediates Cognitive Reserve Effects. Psychol. Neurosci. 2019, 12, 236–246. [Google Scholar] [CrossRef]
- Clare, L.; Wu, Y.T.; Teale, J.C.; MacLeod, C.; Matthews, F.; Brayne, C.; Woods, B. Potentially Modifiable Lifestyle Factors, Cognitive Reserve, and Cognitive Function in Later Life: A Cross-Sectional Study. PLoS Med. 2017, 14, e1002259. [Google Scholar] [CrossRef]
- Ihle, A.; Oris, M.; Sauter, J.; Rimmele, U.; Kliegel, M. Cognitive Reserve and Social Capital Accrued in Early and Midlife Moderate the Relation of Psychological Stress to Cognitive Performance in Old Age. Dement. Geriatr. Cogn. Disord. 2018, 45, 190–197. [Google Scholar] [CrossRef]
- Miceli, S.; Maniscalco, L.; Matranga, D. Social Networks and Social Activities Promote Cognitive Functioning in Both Concurrent and Prospective Time: Evidence from the SHARE Survey. Eur. J. Ageing 2019, 16, 145–154. [Google Scholar] [CrossRef]
- Ramanoël, S.; Hoyau, E.; Kauffmann, L.; Renard, F.; Pichat, C.; Boudiaf, N.; Krainik, A.; Jaillard, A.; Baciu, M. Gray Matter Volume and Cognitive Performance During Normal Aging. A Voxel-Based Morphometry Study. Front. Aging Neurosci. 2018, 10, 235. [Google Scholar] [CrossRef]
- Driscoll, I.; Davatzikos, C.; An, Y.; Wu, X.; Shen, D.; Kraut, M.; Resnick, S.M. Longitudinal Pattern of Regional Brain Volume Change Differentiates Normal Aging from MCI. Neurology 2009, 72, 1906–1913. [Google Scholar] [CrossRef]
- Scahill, R.I.; Frost, C.; Jenkins, R.; Whitwell, J.L.; Rossor, M.N.; Fox, N.C. A Longitudinal Study of Brain Volume Changes in Normal Aging Using Serial Registered Magnetic Resonance Imaging. Arch. Neurol. 2003, 60, 989–994. [Google Scholar] [CrossRef]
- Steffener, J.; Barulli, D.; Habeck, C.; O’Shea, D.; Razlighi, Q.; Stern, Y. The Role of Education and Verbal Abilities in Altering the Effect of Age-Related Gray Matter Differences on Cognition. PLoS ONE 2014, 9, e91196. [Google Scholar] [CrossRef] [Green Version]
- Kwak, S.; Shin, M.; Kim, H.; Cho, B.; Ha, J.H.; Han, G.; Kim, H.; Koo, Y.; Kwon, S.; Lee, C.; et al. Moderating Effect of Cognitive Reserve on the Association between Grey Matter Atrophy and Memory Varies with Age in Older Adults. Psychogeriatrics 2020, 20, 87–95. [Google Scholar] [CrossRef]
- Christensen, H.; Anstey, K.J.; Parslow, R.A.; Maller, J.; Mackinnon, A.; Sachdev, P. The Brain Reserve Hypothesis, Brain Atrophy and Aging. Gerontology 2007, 53, 82–95. [Google Scholar] [CrossRef]
- Brickman, A.M.; Siedlecki, K.L.; Muraskin, J.; Manly, J.J.; Luchsinger, J.A.; Yeung, L.-K.; Brown, T.R.; DeCarli, C.; Stern, Y. White Matter Hyperintensities and Cognition: Testing the Reserve Hypothesis. Neurobiol. Aging 2011, 32, 1588–1598. [Google Scholar] [CrossRef]
- Pinter, D.; Enzinger, C.; Fazekas, F. Cerebral Small Vessel Disease, Cognitive Reserve and Cognitive Dysfunction. J. Neurol. 2015, 262, 2411–2419. [Google Scholar] [CrossRef]
- Durrani, R.; Friedrich, M.G.; Schulze, K.M.; Awadalla, P.; Balasubramanian, K.; Black, S.E.; Broet, P.; Busseuil, D.; Desai, D.; Dummer, T.; et al. Effect of Cognitive Reserve on the Association of Vascular Brain Injury with Cognition: Analysis of the PURE and CAHHM Studies. Neurology 2021, 97, e1707–e1716. [Google Scholar] [CrossRef]
- Stern, Y.; Gurland, B.; Tatemichi, T.K.; Tang, M.X.; Wilder, D.; Mayeux, R. Influence of Education and Occupation on the Incidence of Alzheimer’s Disease. JAMA 1994, 271, 1004–1010. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Geriatr. Psychiatry Neurol. 2016, 29, 338–343. [Google Scholar] [CrossRef] [PubMed]
- Saklofske, D.H.; Schoenberg, M.R. Wechsler Adult Intelligence Scale (All Versions) BT—Encyclopedia of Clinical Neuropsychology; Kreutzer, J.S., DeLuca, J., Caplan, B., Eds.; Springer: New York, NY, USA, 2011; pp. 2675–2680. ISBN 978-0-387-79948-3. [Google Scholar]
- Jaeger, J. Digit Symbol Substitution Test: The Case for Sensitivity Over Specificity in Neuropsychological Testing. J. Clin. Psychopharmacol. 2018, 38, 513–519. [Google Scholar] [CrossRef] [PubMed]
- Kang, J.M.; Cho, Y.S.; Park, S.; Lee, B.H.; Sohn, B.K.; Choi, C.H.; Choi, J.S.; Jeong, H.Y.; Cho, S.J.; Lee, J.H.; et al. Montreal Cognitive Assessment Reflects Cognitive Reserve. BMC Geriatr. 2018, 18, 261. [Google Scholar] [CrossRef] [PubMed]
- Wardlaw, J.M.; Smith, E.E.; Biessels, G.J.; Cordonnier, C.; Fazekas, F.; Frayne, R.; Lindley, R.I.; O’Brien, J.T.; Barkhof, F.; Benavente, O.R.; et al. Neuroimaging Standards for Research into Small Vessel Disease and Its Contribution to Ageing and Neurodegeneration. Lancet. Neurol. 2013, 12, 822–838. [Google Scholar] [CrossRef] [Green Version]
- Fazekas, F.; Chawluk, J.B.; Alavi, A.; Hurtig, H.I.; Zimmerman, R.A. MR Signal Abnormalities at 1.5 T in Alzheimer’s Dementia and Normal Aging. AJR. Am. J. Roentgenol. 1987, 149, 351–356. [Google Scholar] [CrossRef]
- Jacków-Nowicka, J.; Podgórski, P.; Bladowska, J.; Szcześniak, D.; Rymaszewska, J.; Zatońska, K.; Połtyn-Zaradna, K.; Szuba, A.; Sąsiadek, M.; Zimny, A. The Impact of Common Epidemiological Factors on Gray and White Matter Volumes in Magnetic Resonance Imaging—Is Prevention of Brain Degeneration Possible? Front. Neurol. 2021, 12, 633619. [Google Scholar] [CrossRef]
- Rosseel, Y. Lavaan: An R Package for Structural Equation Modeling. J. Stat. Softw. 2012, 48, 1–36. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2013. [Google Scholar]
- Elman, J.A.; Vogel, J.W.; Bocancea, D.I.; Ossenkoppele, R.; van Loenhoud, A.C.; Tu, X.M.; Kremen, W.S. Issues and Recommendations for the Residual Approach to Quantifying Cognitive Resilience and Reserve. Alzheimers. Res. Ther. 2022, 14, 102. [Google Scholar] [CrossRef]
- Conti, L.; Riccitelli, G.C.; Preziosa, P.; Vizzino, C.; Marchesi, O.; Rocca, M.A.; Filippi, M. Effect of Cognitive Reserve on Structural and Functional MRI Measures in Healthy Subjects: A Multiparametric Assessment. J. Neurol. 2021, 268, 1780–1791. [Google Scholar] [CrossRef]
- Lee, D.H.; Lee, P.; Seo, S.W.; Roh, J.H.; Oh, M.; Oh, J.S.; Oh, S.J.; Kim, J.S.; Jeong, Y. Neural Substrates of Cognitive Reserve in Alzheimer’s Disease Spectrum and Normal Aging. Neuroimage 2019, 186, 690–702. [Google Scholar] [CrossRef]
- Jia, F.; Wang, J.; Wei, N.; Sun, D.; Cao, F. Depression, Cognitive Reserve Markers, and Dementia Risk in the General Population. Aging Ment. Health 2021, 26, 1–8. [Google Scholar] [CrossRef]
- Lara, E.; Martín-María, N.; Miret, M.; Olaya, B.; Haro, J.M.; Ayuso-Mateos, J.L. Is There a Combined Effect of Depression and Cognitive Reserve on Cognitive Function? Findings from a Population-Based Study. Psychol. Health 2021, 37, 1132–1147. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Characteristics | No. (%) or Mean (SD) | |
|---|---|---|
| Age | Mean in years | 61.11 ± 9.0 |
| Sex | Female | 481 (63) |
| Male | 282 (37) | |
| Living location | Urban | 598 (78) |
| Rural | 165 (22) | |
| Cognitive reserve (CR) | ||
| Education level | Primary | 38 (5) |
| Trade school | 78 (10) | |
| Secondary/High school | 333 (44) | |
| College/University | 314 (41) | |
| Marital status | Common married/living with the partner | 578 (75.5) |
| Divorced | 68 (9) | |
| Never married | 60 (8) | |
| Widowed | 56 (7) | |
| Unknown | 1 (0.5) | |
| Employment | Yes | 523 (79) |
| No | 240 (30) | |
| No date | 3 (1) | |
| Leisure time physically active | Yes | 73 (14) |
| No | 459 (60) | |
| Unknown | 231 (26) | |
| Participation in social groups | Yes | 95 (13) |
| No | 668 (87) | |
| Cognitive functioning | MoCA < 26 | 296 (39) |
| MoCA mean score | 25.91 ± 2.7 | |
| DSST mean score | 60.18 ± 14.9 | |
| Brain maintenance (WMH) | Fazekas grade | |
| (periventricular + subcortical) | ||
| 0 | 169 (22) | |
| 1 | 173 (23) | |
| 2 | 310 (41) | |
| 3 | 55 (7) | |
| 4 | 36 (4.5) | |
| 5 | 8 (1) | |
| 6 | 12 (1.5) | |
| WMH volume | 1.95 ± 2.4 | |
| Brain reserve | WM volume | 501.07 ± 61.3 |
| GM volume | 572.72 ± 54.4 | |
| Depressive symptoms | CES-d mean | 10.0 ± 8.1 |
| General activity | SAGE mean score | 2.47 ± 2.9 |
| Age Group | 39–49 | 50–59 | 60–69 | ≥70 | p Value * |
|---|---|---|---|---|---|
| No | 110 | 216 | 302 | 135 | |
| MoCA mean score | 27.40 ± 2.3 | 26.29 ± 2.6 | 25.58 ± 2.4 | 24.81 ± 2.9 | <0.001 |
| DSST | 74.54 ± 14.4 | 64.64 ± 13.4 | 56.63 ± 11.6 | 49.26 ± 12.5 | <0.001 |
| Fazekas mean score (WMH) | 0.74 ± 0.8 | 1.22 ± 1.0 | 1.73 ± 1.1 | 2.57 ± 1.4 | <0.001 |
| WMH Volume | 1.21 ± 0.8 | 1.54 ± 1.3 | 1.94 ± 1.4 | 3.23 ± 4.6 | <0.001 |
| GM Volume | 622.69 ± 48.7 | 588.0 ± 49.7 | 562.9 ± 46.9 | 529.6 ±38.3 | <0.001 |
| WM Volume | 542.1 ± 61.4 | 516.6 ± 61.5 | 493.9 ± 54.3 | 458.7 ± 43.7 | <0.001 |
| Effect | Coefficient | SE | z-Value | p-Value | |
|---|---|---|---|---|---|
| CR~MoCA (through WMH vol and WM vol) | Direct effect of CR on MoCA (c) | 0.286 | 0.068 | 4.224 | <0.001 |
| Direct effect of CR on WMH (a1) | −0.142 | 0.064 | −2.220 | 0.03 | |
| Direct effect of CR on WM vol (a2) | 0.029 | 0.023 | 1.287 | 0.198 | |
| Direct effect of WMH on MoCA (b1) | −0.187 | 0.039 | −4.841 | <0.001 | |
| Direct effect of WM on MoCA (b2) | 0.420 | 0.091 | 4.628 | <0.001 | |
| Indirect effect (through WMH) of CR on MoCA (a1b1) | 0.026 | 0.013 | 2.018 | 0.04 | |
| Indirect effect (through WM vol) of CR on MoCA (a2b2) | 0.012 | 0.010 | 1.240 | 0.215 | |
| Total effect of CR on MoCA (a1b1 + a2b2 + c) | 0.324 | 0.067 | 4.826 | <0.001 | |
| CR~MoCA (through WMH vol and GM vol) | Direct effect of CR on MoCA (c) | 0.270 | 0.068 | 3.987 | <0.001 |
| Direct effect of CR on WMH (a1) | −0.170 | 0.064 | −2.631 | 0.009 | |
| Direct effect of CR on GM vol (a2) | 0.054 | 0.021 | 2.567 | 0.01 | |
| Direct effect of WMH on MoCA (b1) | −0/161 | 0.038 | −4.207 | <0.001 | |
| Direct effect of GM on MoCA (b2) | 0.549 | 0.090 | 6.086 | <0.001 | |
| Indirect effect (through WMH) of CR on MoCA (a1b1) | 0.027 | 0.012 | 2.231 | 0.026 | |
| Indirect effect (through GM vol) of CR on MoCA (a2b2) | 0.030 | 0.013 | 2.365 | 0.018 | |
| Total effect of CR on MoCA (a1b1 + a2b2 + c) | 0.327 | 0.067 | 4.897 | <0.001 | |
| CR~DSST (through WMH vol and WM vol) | Direct effect of CR on DSST (c) | 1.780 | 0.327 | 5.447 | <0.001 |
| Direct effect of CR on WMH (a1) | −0.142 | 0.064 | −2.220 | 0.03 | |
| Direct effect of CR on WM vol (a2) | 0.029 | 0.023 | 1.287 | 0.198 | |
| Direct effect of WMH on DSST (b1) | −1.241 | 0.212 | −5.865 | <0.001 | |
| Direct effect of WM on DSST (b2) | 3.042 | 0.498 | 6.107 | <0.001 | |
| Indirect effect (through WMH) of CR on DSST (a1b1) | 1.176 | 0.085 | 2.076 | 0.04 | |
| Indirect effect (through WM vol) of CR on DSST (a2b2) | 0.089 | 0.070 | 1.260 | 0.208 | |
| Total effect of CR on DSST (a1b1 + a2b2 + c) | 2.044 | 0.317 | 6.454 | <0.001 | |
| CR~DSST (through WMH vol and GM vol) | Direct effect of CR on DSST (c) | 1.649 | 0.328 | 5.032 | <0.001 |
| Direct effect of CR on WMH (a1) | −0.170 | 0.064 | −2.631 | 0.009 | |
| Direct effect of CR on GM vol (a2) | 0.054 | 0.021 | 2.567 | 0.01 | |
| Direct effect of WMH on DSST (b1) | −1.052 | 0.208 | −5.060 | <0.001 | |
| Direct effect of GM on DSST (b2) | 4.088 | 0.491 | 8.318 | <0.001 | |
| Indirect effect (through WMH) of CR on DSST (a1b1) | 0.179 | 0.076 | 2.334 | 0.02 | |
| Indirect effect (through GM vol) of CR on DSST (a2b2) | 0.223 | 0.091 | 2.453 | 0.01 | |
| Total effect of CR on DSST (a1b1 + a2b2 + c) | 2.051 | 0.317 | 6.475 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szcześniak, D.; Lenart-Bugla, M.; Misiak, B.; Zimny, A.; Sąsiadek, M.; Połtyn-Zaradna, K.; Zatońska, K.; Zatoński, T.; Szuba, A.; Smith, E.E.; et al. Unraveling the Protective Effects of Cognitive Reserve on Cognition and Brain: A Cross-Sectional Study. Int. J. Environ. Res. Public Health 2022, 19, 12228. https://doi.org/10.3390/ijerph191912228
Szcześniak D, Lenart-Bugla M, Misiak B, Zimny A, Sąsiadek M, Połtyn-Zaradna K, Zatońska K, Zatoński T, Szuba A, Smith EE, et al. Unraveling the Protective Effects of Cognitive Reserve on Cognition and Brain: A Cross-Sectional Study. International Journal of Environmental Research and Public Health. 2022; 19(19):12228. https://doi.org/10.3390/ijerph191912228
Chicago/Turabian StyleSzcześniak, Dorota, Marta Lenart-Bugla, Błażej Misiak, Anna Zimny, Marek Sąsiadek, Katarzyna Połtyn-Zaradna, Katarzyna Zatońska, Tomasz Zatoński, Andrzej Szuba, Eric E. Smith, and et al. 2022. "Unraveling the Protective Effects of Cognitive Reserve on Cognition and Brain: A Cross-Sectional Study" International Journal of Environmental Research and Public Health 19, no. 19: 12228. https://doi.org/10.3390/ijerph191912228