
Poor Eating Behaviors Related to the Progression of Prediabetes in a Japanese Population: An Open Cohort Study

Abstract
:1. Introduction
2. Materials and Methods
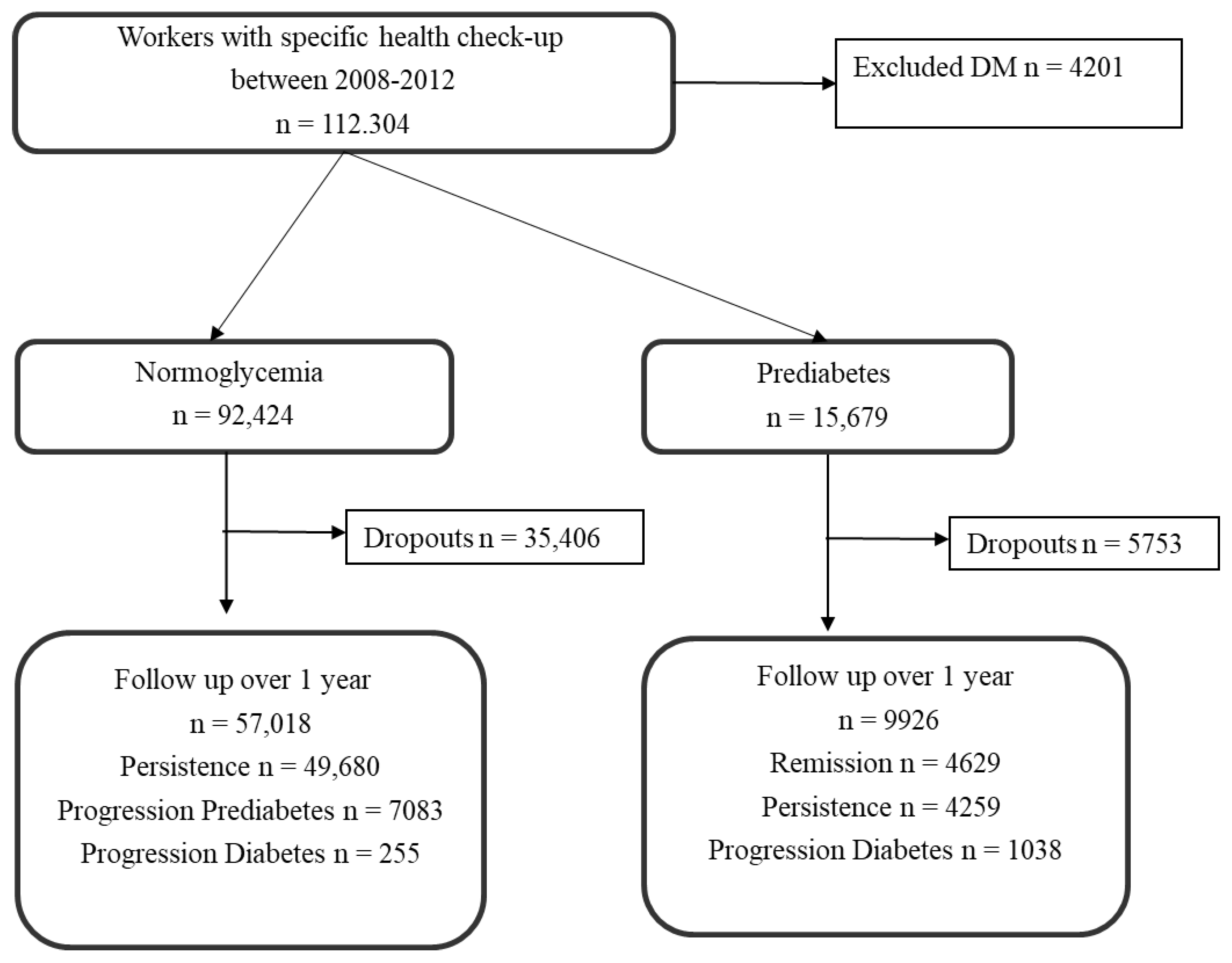
2.1. Survey Procedure, Design, and Participants
2.2. Glucose Tolerance Status
2.3. Lifestyle Behaviors
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Comparison of Baseline Characteristics in Individuals with Normoglycemia and Prediabetes
3.2. Change Rate of Glucose Tolerance and Mean Change in BMI during Follow-Up
3.3. Association between Lifestyle Behaviors and the Change in Glucose Status during Follow-Up
3.4. Sensitivity Analysis of Poor Eating and Exercise Behaviors Associated with Progression to Prediabetes from Normoglycemia
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Bansal, N. Prediabetes diagnosis and treatment: A review. World J. Diabetes 2015, 6, 296–303. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 3. Prevention or delay of type 2 diabetes: Standards of medical care in diabetes—2019. Diabetes Care 2019, 42, S29–S33. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. 2. Classification and diagnosis of diabetes. Diabetes Care 2017, 40, S11–S24. [Google Scholar] [CrossRef] [PubMed]
- Mutie, P.M.; Pomares-Millan, H.; Atabaki-Pasdar, N.; Jordan, N.; Adams, R.; Daly, N.L.; Tajes, J.F.; Giordano, G.N.; Franks, P.W. An investigation of causal relationships between prediabetes and vascular complications. Nat. Commun. 2020, 11, 1–11. [Google Scholar] [CrossRef]
- Baranowska-Jurkun, A.; Matuszewski, W.; Bandurska-Stankiewicz, E. Chronic microvascular complications in prediabetic states-an overview. J. Clin. Med. 2020, 9, 3289. [Google Scholar] [CrossRef]
- Huang, Y.; Cai, X.; Mai, W.; Li, M.; Hu, Y. Association between prediabetes and risk of cardiovascular disease and all cause mortality: Systematic review and meta-analysis. BMJ 2016, 355, i5953. [Google Scholar] [CrossRef]
- Forouhi, N.G.; Luan, J.; Hennings, S.; Wareham, N.J. Incidence of type 2 diabetes in England and its association with baseline impaired fasting glucose: The Ely study 1990–2000. Diabet. Med. 2007, 24, 200–207. [Google Scholar] [CrossRef]
- Glechner, A.; Keuchel, L.; Affengruber, L.; Titscher, V.; Sommer, I.; Matyas, N.; Wagner, G.; Kien, C.; Klerings, I.; Gartlehner, G. Effects of lifestyle changes on adults with prediabetes: A systematic review and meta-analysis. Prim. Care Diabetes 2018, 12, 393–408. [Google Scholar] [CrossRef]
- Apolzan, J.W.; Venditti, E.M.; Edelstein, S.L.; Knowler, W.C.; Dabelea, D.; Boyko, E.J.; Pi-Sunyer, X.; Kalyani, R.R.; Franks, P.W.; Srikanthan, P.; et al. Long-term weight loss with metformin or lifestyle intervention in the Diabetes Prevention Program outcomes study. Ann. Intern. Med. 2019, 170, 682–690. [Google Scholar] [CrossRef]
- Uemura, M.; Yatsuya, H.; Hilawe, E.H.; Li, Y.; Wang, C.; Chiang, C.; Otsuka, R.; Toyoshima, H.; Tamakoshi, K.; Aoyama, A. Breakfast skipping is positively associated with incidence of type 2 diabetes mellitus: Evidence from the Aichi Workers’ Cohort Study. J. Epidemiol. 2015, 25, 351–358. [Google Scholar] [CrossRef] [Green Version]
- Mekary, R.A.; Giovannucci, E.; Cahill, L.; Willett, W.C.; van Dam, R.M.; Hu, F.B. Eating patterns and type 2 diabetes risk in older women: Breakfast consumption and eating frequency. Am. J. Clin. Nutr. 2013, 98, 436–443. [Google Scholar] [CrossRef] [PubMed]
- Kudo, A.; Asahi, K.; Satoh, H.; Iseki, K.; Moriyama, T.; Yamagata, K.; Tsuruya, K.; Fujimoto, S.; Narita, I.; Konta, T.; et al. Fast eating is a strong risk factor for new-onset diabetes among the Japanese general population. Sci. Rep. 2019, 9, 8210. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, M.; Nakamura, K.; Miura, K.; Takamura, T.; Yoshita, K.; Nagasawa, S.Y.; Morikawa, Y.; Ishizaki, M.; Kido, T.; Naruse, Y.; et al. Self-reported speed of eating and 7-year risk of type 2 diabetes mellitus in middle-aged Japanese men. Metabolism 2012, 61, 1566–1571. [Google Scholar] [CrossRef] [PubMed]
- Gouda, M.; Matsukawa, M.; Iijima, H. Associations between eating habits and glycemic control and obesity in Japanese workers with type 2 diabetes mellitus. Diabetes Metab. Syndr. Obes. 2018, 11, 647–658. [Google Scholar] [CrossRef]
- Committee of the Japan Diabetes Society on the Diagnostic Criteria of Diabetes Mellitus; Seino, Y.; Nanjo, K.; Tajima, N.; Kadowaki, T.; Kashiwagi, A.; Araki, E.; Ito, C.; Inagaki, N.; Iwamoto, Y.; et al. Report of the committee on the classification and diagnostic criteria of diabetes mellitus. J. Diabetes Investig. 2010, 1, 212–228. [Google Scholar] [CrossRef]
- World Health Organization. Classification of Diabetes Mellitus; WHO: Geneva, Switzerland, 2019.
- Seki, T.; Takeuchi, M.; Kawakami, K. Eating and drinking habits and its association with obesity in Japanese healthy adults: Retrospective longitudinal big data analysis using a health check-up database. Br. J. Nutr. 2021, 126, 1585–1591. [Google Scholar] [CrossRef]
- Umemura, S.; Arima, H.; Arima, S.; Asayama, K.; Dohi, Y.; Hirooka, Y.; Horio, T.; Hoshide, S.; Ikeda, S.; Ishimitsu, T.; et al. The Japanese Society of Hypertension guidelines for the management of hypertension (JSH 2019). Hypertens. Res. 2019, 42, 1235–1481. [Google Scholar] [CrossRef]
- Teramoto, T.; Sasaki, J.; Ishibashi, S.; Birou, S.; Daida, H.; Dohi, S.; Egusa, G.; Hiro, T.; Hirobe, K.; Iida, M.; et al. Diagnostic criteria for dyslipidemia. J. Atheroscler. Thromb. 2013, 20, 655–660. [Google Scholar] [CrossRef]
- Campagna, D.; Alamo, A.; di Pino, A.; Russo, C.; Calogero, A.E.; Purrello, F.; Polosa, R. Smoking and diabetes: Dangerous liaisons and confusing relationships. Diabetol. Metab. Syndr. 2019, 11, 85. [Google Scholar] [CrossRef]
- Okamoto, M.; Kobayashi, Y.; Nakamura, F.; Musha, T. Association between nonrestorative sleep and risk of diabetes: A cross-sectional study. Behav. Sleep Med. 2017, 15, 483–490. [Google Scholar] [CrossRef]
- Schellenberg, E.S.; Dryden, D.M.; Vandermeer, B.; Ha, C.; Korownyk, C. Lifestyle interventions for patients with and at risk for type 2 diabetes: A systematic review and meta-analysis. Ann. Intern. Med. 2013, 159, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Owei, I.; Wan, J.; Ebenibo, S.; Dagogo-Jack, S. Adiponectin levels predict prediabetes risk: The Pathobiology of Prediabetes in A Biracial Cohort (POP-ABC) study. BMJ Open Diabetes Res. Care 2016, 4, e000194. [Google Scholar] [CrossRef] [PubMed]
- Brahimaj, A.; Ligthart, S.; Ghanbari, M.; Ikram, M.A.; Hofman, A.; Franco, O.H.; Kavousi, M.; Dehghan, A. Novel inflammatory markers for incident pre-diabetes and type 2 diabetes: The Rotterdam Study. Eur. J. Epidemiol. 2017, 32, 217–226. [Google Scholar] [CrossRef]
- Lazo-Porras, M.; Bernabe-Ortiz, A.; Ruiz-Alejos, A.; Smeeth, L.; Gilman, R.H.; Checkley, W.; Málaga, G.; Miranda, J.J. Regression from prediabetes to normal glucose levels is more frequent than progression towards diabetes: The CRONICAS Cohort Study. Diabetes Res. Clin. Pract. 2020, 163, 107829. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Nemoto, T.; Tobimatsu, S.; Saito, M.; Ebata, M.; Munakata, H.; Nakajima, K. Relationship between skipping breakfast and impaired fasting glucose along with cardiovascular and pre-diabetes condition risk factors in apparently healthy subjects. Endocrinol. Stud. 2011, 1, e17. [Google Scholar] [CrossRef]
- Ballon, A.; Neuenschwander, M.; Schlesinger, S. Breakfast skipping is associated with increased risk of Type 2 diabetes among adults: A systematic review and meta-analysis of prospective cohort studies. J. Nutr. 2019, 149, 106–113. [Google Scholar] [CrossRef]
- Jakubowicz, D.; Wainstein, J.; Ahren, B.; Landau, Z.; Bar-Dayan, Y.; Froy, O. Fasting until noon triggers increased postprandial hyperglycemia and impaired insulin response after lunch and dinner in individuals with type 2 diabetes: A randomized clinical trial. Diabetes Care 2015, 38, 1820–1826. [Google Scholar] [CrossRef]
- Nakajima, K.; Suwa, K. Association of hyperglycemia in a general Japanese population with late-night-dinner eating alone, but not breakfast skipping alone. J. Diabetes Metab. Disord. 2015, 14, 16. [Google Scholar] [CrossRef]
- Sato, M.; Nakamura, K.; Ogata, H.; Miyashita, A.; Nagasaka, S.; Omi, N.; Yamaguchi, S.; Hibi, M.; Umeda, T.; Nakaji, S.; et al. Acute effect of late evening meal on diurnal variation of blood glucose and energy metabolism. Obes. Res. Clin. Pract. 2011, 5, e169–e266. [Google Scholar] [CrossRef]
- Munakata, M.; Honma, H.; Akasi, M.; Araki, T.; Kawamura, T.; Kubota, M.; Yokokawa, T.; Numata, Y.; Toyonaga, T.; J-STOP-MetS Study Group. Repeated counselling improves the antidiabetic effects of limited individualized lifestyle guidance in metabolic syndrome: J-STOP-METS final results. Hypertens. Res. 2011, 34, 612–616. [Google Scholar] [CrossRef] [Green Version]
- Hrubeniuk, T.J.; Bouchard, D.R.; Goulet, E.D.B.; Gurd, B.; Senechal, M. The ability of exercise to meaningfully improve glucose tolerance in people living with prediabetes: A meta-analysis. Scand. J. Med. Sci. Sports 2020, 30, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, M.; Kudo, A.; Asahi, K.; Machii, N.; Iseki, K.; Satoh, H.; Moriyama, T.; Yamagata, K.; Tsuruya, K.; Fujimoto, S.; et al. Fast walking is a preventive factor against new-onset diabetes mellitus in a large cohort from a Japanese general population. Sci. Rep. 2021, 11, 716. [Google Scholar] [CrossRef] [PubMed]
- Willi, C.; Bodenmann, P.; Ghali, W.A.; Faris, P.D.; Cornuz, J. Active smoking and the risk of Type 2 Diabetes: A systematic review and meta-analysis. JAMA 2007, 298, 2654–2664. [Google Scholar] [CrossRef] [PubMed]
- Śliwińska-Mossoń, M.; Milnerowicz, H. The impact of smoking on the development of diabetes and its complications. Diab. Vasc. Dis. Res. 2017, 14, 265–276. [Google Scholar] [CrossRef] [PubMed]
- Baliunas, D.O.; Taylor, B.J.; Irving, H.; Roerecke, M.; Patra, J.; Mohapatra, S.; Rehm, J. Alcohol as a risk factor for type 2 diabetes: A systematic review and meta-analysis. Diabetes Care 2009, 32, 2123–2132. [Google Scholar] [CrossRef] [PubMed]
- Ueda, N.; Yamamoto, M.; Nakamura, M.; Motooka, Y.; Nakayama, Y.; Nonoyama, Y.; Oba, S.; Horikawa, Y.; Nagata, C.; Yabe, D.; et al. Alcohol-induced impaired insulin secretion in a Japanese population: 5-year follow up in the Gifu diabetes study. J Diabetes Investig. 2020, 11, 1207–1214. [Google Scholar] [CrossRef]
- Diabetes Prevention Program (DPP) Research Group. The Diabetes Prevention Program (DPP): Description of lifestyle intervention. Diabetes Care 2002, 25, 2165–2171. [Google Scholar] [CrossRef]
- Lindström, J.; Peltonen, M.; Eriksson, J.G.; Aunola, S.; Hämäläinen, H.; Ilanne-Parikka, P.; Keinänen-Kiukaanniemi, S.; Uusitupa, M.; Tuomilehto, J.; Finnish Diabetes Prevention Study (DPS) Group. Determinants for the effectiveness of lifestyle intervention in the Finnish Diabetes Prevention Study. Diabetes Care 2008, 31, 857–862. [Google Scholar] [CrossRef]
- Miyagi, S.; Takamura, T.; Nguyen, T.T.T.; Tsujiguchi, H.; Hara, A.; Nakamura, H.; Suzuki, K.; Tajima, A.; Kannon, T.; Toyama, T.; et al. Moderate alcohol consumption is associated with impaired insulin secretion and fasting glucose in non-obese non-diabetic men. J. Diabetes Investig. 2021, 12, 869–876. [Google Scholar] [CrossRef]
- Morgan, L.M.; Shi, J.W.; Hampton, S.M.; Frost, G. Effect of meal timing and glycaemic index on glucose control and insulin secretion in healthy volunteers. Br. J. Nutr. 2012, 108, 1286–1291. [Google Scholar] [CrossRef] [Green Version]
- Selvin, E.; Crainiceanu, C.M.; Brancati, F.L.; Coresh, J. Short-term variability in measures of glycemia and implications for the classification of diabetes. Arch. Intern. Med. 2007, 167, 1545–1551. [Google Scholar] [CrossRef] [PubMed]
- Grintsova, O.; Maier, W.; Mielck, A. Inequalities in health care among patients with type 2 diabetes by individual socio-economic status (SES) and regional deprivation: A systematic literature review. Int. J. Equity Health 2014, 13, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Normoglycemia | Prediabetes | p-Value | |||
|---|---|---|---|---|---|
| Number | 57,018 | 9926 | |||
| Age (years) | 36.0 † | (30–45) ‡ | 49.0 † | (39–57) ‡ | <0.001 |
| Male | 30,427 | (53.4) | 6830 | (68.8) | <0.001 |
| BMI (kg/m2) | 21.6 † | (19.7–23.9) ‡ | 23.9 † | (21.6–26.4) ‡ | <0.001 |
| Family history of diabetes | 1329 | (2.3) | 249 | (2.5) | 0.281 |
| Hypertension | 17,048 | (29.9) | 5727 | (57.7) | <0.001 |
| Dyslipidemia | 5195 | (9.1) | 3148 | (31.7) | <0.001 |
| Lifestyle behaviors | |||||
| Physical activities | |||||
| Less physically activity | 34,132 | (60.5) | 6220 | (63.6) | <0.001 |
| Non-regular exercise | 47,896 | (84.5) | 7884 | (80.2) | <0.001 |
| Not walking fast | 29,706 | (52.8) | 5041 | (52.0) | 0.176 |
| Eating speed | <0.001 | ||||
| Normal | 33,188 | (58.2) | 5936 | (59.8) | |
| Fast | 17,853 | (31.3) | 3266 | (32.9) | |
| Late dinner/snacking | 26,691 | (46.8) | 4590 | (46.2) | 0.378 |
| Skipping breakfast | 17,249 | (30.5) | 2423 | (24.7) | <0.001 |
| Insufficient sleep | 25,264 | (44.8) | 4179 | (42.8) | <0.001 |
| Smoking | 18,328 | (32.1) | 3329 | (33.5) | 0.006 |
| Heavy alcohol consumption | 5348 | (9.5) | 1456 | (14.9) | <0.001 |
| Progress to Prediabetes from Normoglycemia during Follow-Up | Return to Normoglycemia from Prediabetes during Follow-Up | |||||||
|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | Z-Value | HR | 95% CI | p-Value | Z-Value | |
| Baseline BMI (kg/m2) | 1.08 | 1.07–1.09 | <0.001 | 21.39 | 0.94 | 0.93–0.95 | <0.001 | −13.90 |
| Change in BMI | 1.05 | 1.03–1.07 | <0.001 | 4.83 | 0.95 | 0.93–0.97 | <0.001 | −4.24 |
| Less physical activity | 0.98 | 0.93–1.03 | 0.396 | −0.85 | 1.01 | 0.95–1.08 | 0.724 | 0.35 |
| Non-regular exercise | 1.05 | 0.98–1.12 | 0.171 | 1.37 | 0.99 | 0.91–1.07 | 0.724 | −0.35 |
| Not walking fast | 1.01 | 0.96–1.06 | 0.716 | 0.36 | 0.97 | 0.91–1.03 | 0.270 | −1.10 |
| Eating speed (ref: “slow”) | ||||||||
| Normal | 1.13 | 1.03–1.24 | 0.013 | 2.49 | 1.07 | 0.96–1.20 | 0.235 | 1.19 |
| Fast | 1.06 | 0.96–1.17 | 0.268 | 1.11 | 1.05 | 0.93–1.18 | 0.441 | 0.77 |
| Late dinner/snacking | 1.16 | 1.10–1.22 | <0.001 | 5.80 | 0.98 | 0.92–1.04 | 0.430 | −0.79 |
| Skipping breakfast | 1.12 | 1.06–1.18 | <0.001 | 3.85 | 1.02 | 0.95–1.09 | 0.648 | 0.46 |
| Insufficient sleep | 1.01 | 0.96–1.06 | 0.721 | 0.36 | 0.99 | 0.93–1.06 | 0.820 | −0.23 |
| Smoking | 0.98 | 0.93–1.04 | 0.564 | -0.58 | 1.03 | 0.96–1.10 | 0.436 | 0.78 |
| Heavy alcohol consumption | 1.33 | 1.24–1.42 | <0.001 | 8.19 | 1.05 | 0.96–1.14 | 0.265 | 1.11 |
| HR | 95% CI | p-Value | Z-Value | p-Trend | |
|---|---|---|---|---|---|
| Baseline BMI (kg/m2) | 1.08 | 1.07–1.08 | <0.001 | 21.33 | |
| Change in BMI | 1.05 | 1.03–1.07 | <0.001 | 5.16 | |
| Poor eating behaviors (ref: “no”) | <0.001 | ||||
| Single | 1.06 | 1.00–1.13 | 0.040 | 2.05 | |
| Double | 1.14 | 1.07–1.22 | <0.001 | 3.88 | |
| Triple | 1.21 | 1.10–1.34 | <0.001 | 3.80 | |
| Poor exercise behaviors (ref: “no”) | 0.308 | ||||
| Single | 1.05 | 0.95–1.16 | 0.318 | 1.00 | |
| Double | 1.02 | 0.93–1.12 | 0.624 | 0.49 | |
| Triple | 1.06 | 0.97–1.16 | 0.218 | 1.23 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Otsuka, Y.; Nakagami, T. Poor Eating Behaviors Related to the Progression of Prediabetes in a Japanese Population: An Open Cohort Study. Int. J. Environ. Res. Public Health 2022, 19, 11864. https://doi.org/10.3390/ijerph191911864
Otsuka Y, Nakagami T. Poor Eating Behaviors Related to the Progression of Prediabetes in a Japanese Population: An Open Cohort Study. International Journal of Environmental Research and Public Health. 2022; 19(19):11864. https://doi.org/10.3390/ijerph191911864
Chicago/Turabian StyleOtsuka, Yuichiro, and Tomoko Nakagami. 2022. "Poor Eating Behaviors Related to the Progression of Prediabetes in a Japanese Population: An Open Cohort Study" International Journal of Environmental Research and Public Health 19, no. 19: 11864. https://doi.org/10.3390/ijerph191911864