
Low Sleep Satisfaction Is Related to High Disease Burden in Tinnitus
 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Variables
2.3. Data Preparation
2.4. Statistical Analysis and Model Fitting
2.5. Statistical Software
3. Results
4. Discussion
4.1. Concept of Sleep Satisfaction in Tinnitus
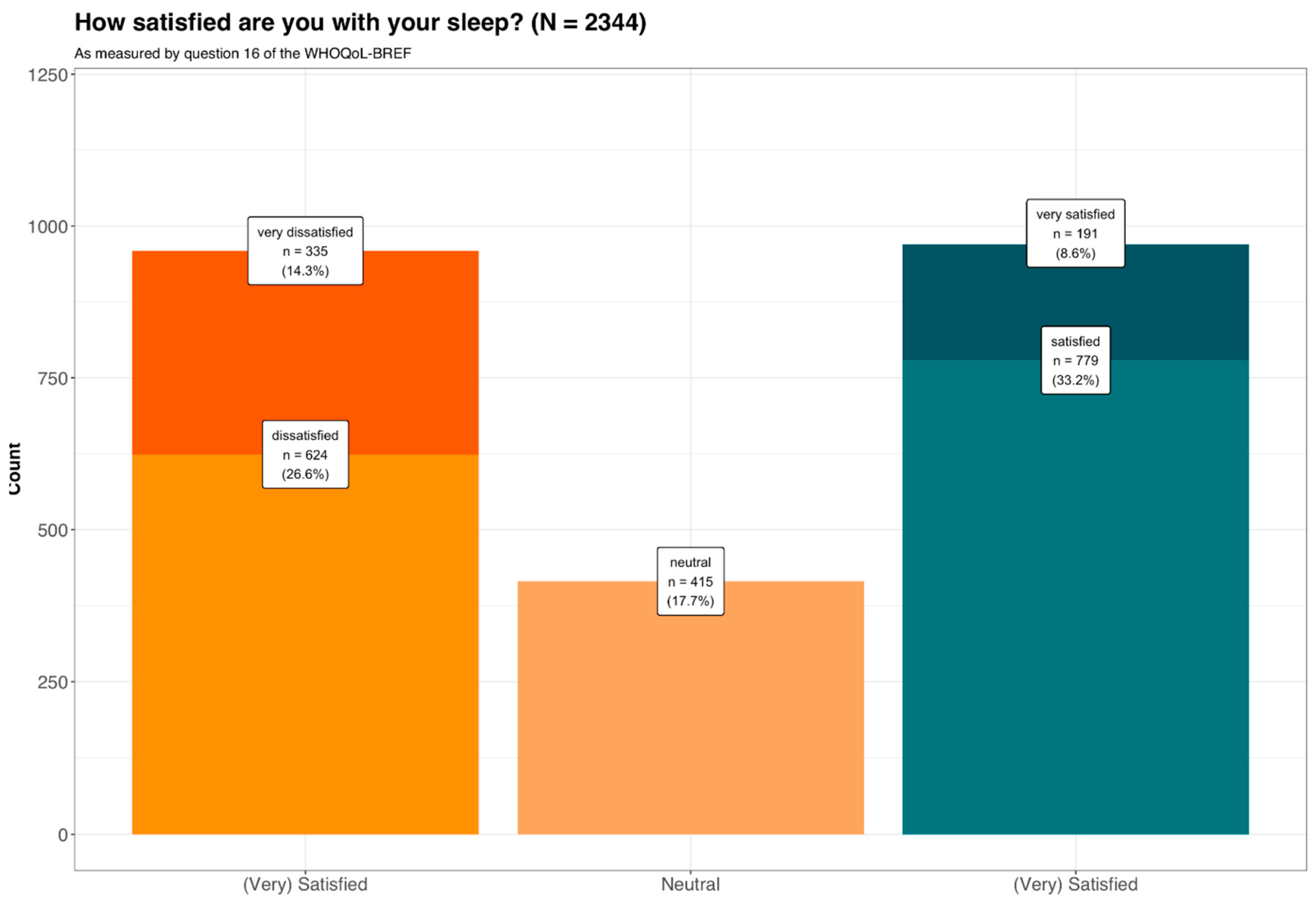
4.2. Distribution of Sleep Satisfaction in Tinnitus
4.3. Higher Burden in Sleep-Dissatisfied Patients: Depression, Tinnitus and Reduced Quality of Life
4.4. More Comorbidities in Sleep-Dissatisfied Patients
4.5. Predictive Accuracy of the Model
4.6. Influencing Factors on the Model
4.7. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baguley, D.; McFerran, D.; Hall, D. Tinnitus. Lancet 2013, 382, 1600–1607. [Google Scholar] [CrossRef]
- Langguth, B.; Kreuzer, P.M.; Kleinjung, T.; De Ridder, D. Tinnitus: Causes and clinical management. Lancet Neurol. 2013, 12, 920–930. [Google Scholar] [CrossRef]
- De Ridder, D.; Schlee, W.; Vanneste, S.; Londero, A.; Weisz, N.; Kleinjung, T.; Shekhawat, G.S.; Elgoyhen, A.B.; Song, J.-J.; Andersson, G.; et al. Tinnitus and tinnitus disorder: Theoretical and operational definitions (an international multidisciplinary proposal). Prog. Brain Res. 2021, 260, 1–25. [Google Scholar] [PubMed]
- Gallus, S.; Lugo, A.; Garavello, W.; Bosetti, C.; Santoro, E.; Colombo, P.; Perin, P.; La Vecchia, C.; Langguth, B. Prevalence and Determinants of Tinnitus in the Italian Adult Population. Neuroepidemiology 2015, 45, 12–19. [Google Scholar] [CrossRef] [PubMed]
- McCormack, A.; Edmondson-Jones, M.; Somerset, S.; Hall, D. A systematic review of the reporting of tinnitus prevalence and severity. Hear Res. 2016, 337, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Bhatt, J.M.; Lin, H.W.; Bhattacharyya, N. Prevalence, Severity, Exposures, and Treatment Patterns of Tinnitus in the United States. JAMA Otolaryngol. Neck Surg. 2016, 142, 959–965. [Google Scholar] [CrossRef]
- Biswas, R.; Lugo, A.; Akeroyd, M.; Schlee, W.; Gallus, S.; Hall, D. Tinnitus prevalence in Europe: A multi-country cross-sectional population study. Lancet Reg. Health Eur. 2021, 12, 100250. [Google Scholar] [CrossRef]
- Stohler, N.A.; Reinau, D.; Jick, S.S.; Bodmer, D.; Meier, C.R. A study on the epidemiology of tinnitus in the United Kingdom. Clin. Epidemiol. 2019, 11, 855–871. [Google Scholar] [CrossRef]
- Schecklmann, M.; Landgrebe, M.; Langguth, B. Phenotypic Characteristics of Hyperacusis in Tinnitus. PLoS ONE 2014, 9, e86944. [Google Scholar] [CrossRef]
- Mazurek, B.; Olze, H.; Haupt, H.; Szczepek, A.J. The More the Worse: The Grade of Noise-Induced Hearing Loss Associates with the Severity of Tinnitus. Int. J. Environ. Res. Public Health 2010, 7, 3071–3079. [Google Scholar] [CrossRef] [Green Version]
- Joo, Y.-H.; Han, K.-D.; Park, K.H. Association of Hearing Loss and Tinnitus with Health-Related Quality of Life: The Korea National Health and Nutrition Examination Survey. PLoS ONE 2015, 10, e0131247. [Google Scholar] [CrossRef] [PubMed]
- Crönlein, T.; Langguth, B.; Geisler, P.; Hajak, G. Tinnitus and insomnia. Prog. Brain Res. 2007, 166, 227–233. [Google Scholar] [PubMed]
- Folmer, R.L.; Griest, S.E. Tinnitus and insomnia. Am. J. Otolaryngol. 2000, 21, 287–293. [Google Scholar] [CrossRef] [PubMed]
- Tyler, R.; Baker, L.J. Difficulties Experienced by Tinnitus Sufferers. J. Speech Hear. Disord. 1983, 48, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Koning, H.M. Sleep Disturbances Associated with Tinnitus: Reduce the Maximal Intensity of Tinnitus. Int. Tinnitus J. 2019, 23, 64–68. [Google Scholar]
- Crönlein, T.; Langguth, B.; Pregler, M.; Kreuzer, P.M.; Wetter, T.C.; Schecklmann, M. Insomnia in patients with chronic tinnitus: Cognitive and emotional distress as moderator variables. J. Psychosom. Res. 2016, 83, 65–68. [Google Scholar] [CrossRef]
- Langguth, B.; Landgrebe, M.; Kleinjung, T.; Sand, G.P.; Hajak, G. Tinnitus and depression. World J. Biol. Psychiatry 2011, 12, 489–500. [Google Scholar] [CrossRef]
- Milerová, J.; Anders, M.; Dvořák, T.; Sand, P.; Königer, S.; Langguth, B. The influence of psychological factors on tinnitus severity. Gen. Hosp. Psychiatry 2013, 35, 412–416. [Google Scholar] [CrossRef]
- Langguth, B.; Hund, V.; Landgrebe, M.; Schecklmann, M. Tinnitus Patients with Comorbid Headaches: The Influence of Headache Type and Laterality on Tinnitus Characteristics. Front. Neurol. 2017, 8, 440. [Google Scholar] [CrossRef]
- Kennedy, V.; Wilson, C.; Stephens, D. Quality of life and tinnitus. Audiol. Med. 2004, 2, 29–40. [Google Scholar] [CrossRef]
- McFerran, D.J.; Stockdale, D.; Holme, R.; Large, C.H.; Baguley, D.M. Why Is There No Cure for Tinnitus? Front. Neurosci. 2019, 13, 802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McKenna, L.; Handscomb, L.; Hoare, D.; Hall, D. A Scientific Cognitive-Behavioral Model of Tinnitus: Novel Conceptualizations of Tinnitus Distress. Front. Neurol. 2014, 5, 196. [Google Scholar] [CrossRef]
- Zeman, F.; Koller, M.; Langguth, B.; Landgrebe, M. Which tinnitus-related aspects are relevant for quality of life and depression: Results from a large international multicentre sample. Health Qual. Life Outcomes 2014, 12, 7. [Google Scholar] [CrossRef] [PubMed]
- Asnis, G.M.; Majeed, K.; Henderson, M.A.; Sylvester, C.; Thomas, M.; De La Garza, I.R. An Examination of the Relationship Between Insomnia and Tinnitus: A Review and Recommendations. Clin. Med. Insights Psychiatry 2018, 9, 117955731878107. [Google Scholar] [CrossRef]
- Lai, J.-T.; Shen, P.-H.; Lin, C.-Y.; Liu, C.-L.; Liu, T.-C. Higher prevalence and increased severity of sleep-disordered breathing in male patients with chronic tinnitus: Our experience with 173 cases. Clin. Otolaryngol. 2017, 43, 722–725. [Google Scholar] [CrossRef]
- Lai, J.-T.; Lin, C.-Y.; Yan, Y.-H.; Shen, P.-H. High prevalence of obstructive sleep apnea syndrome in patients with tinnitus. J. Hear. Sci. 2017, 109. [Google Scholar]
- Liu, X.L.; Wang, J.; Hong, Z.J.; Zhongshan, M.F. A preliminary study on the correlation between obstructive sleep apnea hypopnea syndrome and chronic tinnitus. J. Clin. Otorhinolaryngol. Head Neck Surg. 2018, 32, 575–578. [Google Scholar]
- Asplund, R. Nightmares in Relation to Sleep and Sensory Organ Functions in the Elderly. Sleep Hypn. A J. Clin. Neurosci. Psychopathol. 2004, 6, 1–7. [Google Scholar]
- Fagelson, M.A. The Association Between Tinnitus and Posttraumatic Stress Disorder. Am. J. Audiol. 2007, 16, 107–117. [Google Scholar] [CrossRef]
- Hwang, S.-W.; Chu, Y.-C.; Hwang, S.-R.; Hwang, J.-H. Association of periodic limb movements during sleep and tinnitus in humans. Sci. Rep. 2020, 10, 5972. [Google Scholar] [CrossRef]
- Axelsson, A.; Ringdahl, A. Tinnitus—A study of its prevalence and characteristics. Br. J. Audiol. 1989, 23, 53–62. [Google Scholar] [CrossRef] [PubMed]
- Hallam, R. Correlates of Sleep Disturbance in Chronic Distressing Tinnitus. Scand. Audiol. 1996, 25, 263–266. [Google Scholar] [CrossRef] [PubMed]
- Izuhara, K.; Wada, K.; Nakamura, K.; Tamai, Y.; Tsuji, M.; Ito, Y.; Nagata, C. Association between Tinnitus and Sleep Disorders in the General Japanese Population. Ann. Otol. Rhinol. Laryngol. 2013, 122, 701–706. [Google Scholar] [CrossRef] [PubMed]
- Miguel, G.S.; Yaremchuk, K.; Roth, T.; Peterson, E. The Effect of Insomnia on Tinnitus. Ann. Otol. Rhinol. Laryngol. 2014, 123, 696–700. [Google Scholar] [CrossRef]
- Wallhäusser-Franke, E.; Schredl, M.; Delb, W. Tinnitus and insomnia: Is hyperarousal the common denominator? Sleep Med. Rev. 2013, 17, 65–74. [Google Scholar] [CrossRef]
- Harvey, A.G.; Murray, G.; Chandler, R.A.; Soehner, A. Sleep disturbance as transdiagnostic: Consideration of neurobiological mechanisms. Clin. Psychol. Rev. 2011, 31, 225–235. [Google Scholar] [CrossRef]
- Dolsen, M.R.; Asarnow, L.D.; Harvey, A.G. Insomnia as a Transdiagnostic Process in Psychiatric Disorders. Curr. Psychiatry Rep. 2014, 16, 471. [Google Scholar] [CrossRef]
- Fang, H.; Tu, S.; Sheng, J.; Shao, A. Depression in sleep disturbance: A review on a bidirectional relationship, mechanisms and treatment. J. Cell. Mol. Med. 2019, 23, 2324–2332. [Google Scholar] [CrossRef]
- Weber, F.C.; Wetter, T.C. The Many Faces of Sleep Disorders in Post-Traumatic Stress Disorder: An Update on Clinical Features and Treatment. Neuropsychobiology 2021, 81, 85–97. [Google Scholar] [CrossRef]
- Folmer, R.L. Long-term reductions in tinnitus severity. BMC Ear Nose Throat Disord. 2002, 2, 3. [Google Scholar] [CrossRef]
- Eysel-Gosepath, K.; Selivanova, O. Charakteristik der Schlafstörungen bei Patienten mit Tinnitus. Laryngorhinootologie 2005, 84, 323–327. [Google Scholar] [CrossRef]
- Wakabayashi, S.; Saito, H.; Oishi, N.; Shinden, S.; Ogawa, K. Effects of tinnitus treatments on sleep disorders in patients with tinnitus. Int. J. Audiol. 2017, 57, 110–114. [Google Scholar] [CrossRef]
- Curtis, F.; Laparidou, D.; Bridle, C.; Law, G.R.; Durrant, S.; Rodriguez, A.; Pierzycki, R.H.; Siriwardena, A.N. Effects of cognitive behavioural therapy on insomnia in adults with tinnitus: Systematic review and meta-analysis of randomised controlled trials. Sleep Med. Rev. 2020, 56, 101405. [Google Scholar] [CrossRef] [PubMed]
- Marks, E.; Hallsworth, C.; Vogt, F.; Klein, H.; McKenna, L. Cognitive behavioural therapy for insomnia (CBTi) as a treatment for tinnitus-related insomnia: A randomised controlled trial. Cogn. Behav. Ther. 2022, 1–19. [Google Scholar] [CrossRef] [PubMed]
- Marks, E.; McKenna, L.; Vogt, F. Cognitive behavioural therapy for tinnitus-related insomnia: Evaluating a new treatment approach. Int. J. Audiol. 2019, 58, 311–316. [Google Scholar] [CrossRef] [PubMed]
- Lu, T.; Li, S.; Ma, Y.; Lai, D.; Zhong, J.; Li, G.; Zheng, Y. Positive Correlation between Tinnitus Severity and Poor Sleep Quality Prior to Tinnitus Onset: A Retrospective Study. Psychiatr. Q. 2020, 91, 379–388. [Google Scholar] [CrossRef]
- Oosterloo, B.C.; de Feijter, M.; Croll, P.H.; Baatenburg de Jong, R.J.; Luik, A.I.; Goedegebure, A. Cross-sectional and Longitudinal Associations Between Tinnitus and Mental Health in a Population-Based Sample of Middle-aged and Elderly Persons. JAMA Otolaryngol. Head Neck Surg. 2021, 147, 708–716. [Google Scholar] [CrossRef]
- The WHOQOL Group. Development of the World Health Organization WHOQOL-BREF quality of life assessment. The WHOQOL Group. Psychol. Med. 1998, 28, 551–558. [Google Scholar] [CrossRef]
- Landgrebe, M.; Zeman, F.; Koller, M.; Eberl, Y.; Mohr, M.; Reiter, J.; Staudinger, S.; Hajak, G.; Langguth, B. The Tinnitus Research Initiative (TRI) database: A new approach for delineation of tinnitus subtypes and generation of predictors for treatment outcome. BMC Med. Inform. Decis. Mak. 2010, 10, 42. [Google Scholar] [CrossRef]
- Newman, C.W.; Jacobson, G.P.; Spitzer, J.B. Development of the Tinnitus Handicap Inventory. Arch. Otolaryngol. Head Neck Surg. 1996, 122, 143–148. [Google Scholar] [CrossRef]
- Zeman, F.; Koller, M.; Schecklmann, M.; Langguth, B.; Landgrebe, M. Tinnitus assessment by means of standardized self-report questionnaires: Psychometric properties of the Tinnitus Questionnaire (TQ), the Tinnitus Handicap Inventory (THI), and their short versions in an international and multi-lingual sample. Health Qual. Life Outcomes 2012, 10, 128. [Google Scholar] [CrossRef] [PubMed]
- Zeman, F.; Koller, M.; Figueiredo, R.; Aazevedo, A.; Rates, M.; Coelho, C.; Kleinjung, T.; de Ridder, D.; Langguth, B.; Landgrebe, M. Tinnitus handicap inventory for evaluating treatment effects: Which changes are clinically relevant? Otolaryngol. Head Neck Surg. 2011, 145, 282–287. [Google Scholar] [CrossRef] [PubMed]
- Bech, P.; Rasmussen, N.-A.; Olsen, L.; Noerholm, V.; Abildgaard, W. The sensitivity and specificity of the Major Depression Inventory, using the Present State Examination as the index of diagnostic validity. J. Affect. Disord. 2001, 66, 159–164. [Google Scholar] [CrossRef]
- Olsen, L.R.; Jensen, D.V.; Noerholm, V.; Martiny, K.; Bech, P. The internal and external validity of the Major Depression Inventory in measuring severity of depressive states. Psychol. Med. 2003, 33, 351–356. [Google Scholar] [CrossRef] [PubMed]
- Langguth, B.; Goodey, R.; Azevedo, A.; Bjorne, A.; Cacace, A.; Crocetti, A.; Del Bo, L.; De Ridder, D.; Diges, I.; Elbert, T.; et al. Consensus for tinnitus patient assessment and treatment outcome measurement: Tinnitus Research Initiative meeting, Regensburg, July 2006. Prog. Brain Res. 2007, 166, 525–536. [Google Scholar]
- Skevington, S.M.; Lotfy, M.; O’Connell, K.A. The World Health Organization’s WHOQOL-BREF quality of life assessment: Psychometric properties and results of the international field trial. A report from the WHOQOL group. Qual Life Res. 2004, 13, 299–310. [Google Scholar] [CrossRef] [PubMed]
- Malarvizhi, M.R.; Thanamani, A.S. K-Nearest Neighbor in Missing Data Imputation. Int. J. Eng. Res. Dev. 2012, 5, 5–7. [Google Scholar]
- Holm, S. A Simple Sequentially Rejective Multiple Test Procedure. Scand. J. Stat. 1979, 6, 65–70. [Google Scholar]
- Tibshirani, R. Regression Shrinkage and Selection via the Lasso. J. R. Stat. Soc. Ser. B (Methodol.) 1996, 58, 267–288. [Google Scholar] [CrossRef]
- Kuhn, M.; Silge, J. Tidy Modeling with R; O’Reilly Media, Inc.: Sebastopol, CA, USA, 2022. [Google Scholar]
- Wickham, H.; Averick, M.; Bryan, J.; Chang, W.; McGowan, L.D.A.; François, R.; Grolemund, G.; Hayes, A.; Henry, L.; Hester, J.; et al. Welcome to the Tidyverse. J. Open Source Softw. 2019, 4, 1686. [Google Scholar] [CrossRef]
- Kuhn, M.; Wickham, H. Tidymodels: A Collection of Packages for Modeling and Machine Learning Using Tidyverse Principles. 2020. Available online: https://www.tidymodels.org (accessed on 10 December 2020).
- Ohayon, M.M.; Chen, M.C.; Bixler, E.; Dauvilliers, Y.; Gozal, D.; Plazzi, G.; Vitiello, M.V.; Paskow, M.; Roach, A.; Hirshkowitz, M. A provisional tool for the measurement of sleep satisfaction. Sleep Health 2017, 4, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Ohayon, M.M.; Paskow, M.; Roach, A.; Filer, C.; Hillygus, D.S.; Chen, M.C.; Langer, G.; Hirshkowitz, M. The National Sleep Foundation’s Sleep Satisfaction Tool. Sleep Health 2019, 5, 5–11. [Google Scholar] [CrossRef] [PubMed]
- Buysse, D.J.; Reynolds, C.F., III; Monk, T.H.; Berman, S.R.; Kupfer, D.J. The Pittsburgh sleep quality index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989, 28, 193–213. [Google Scholar] [CrossRef]
- Bastien, C.H.; Vallieres, A.; Morin, C.M. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001, 2, 297–307. [Google Scholar] [CrossRef]
- Morin, C.M.; Belleville, G.; Bélanger, L.; Ivers, H. The Insomnia Severity Index: Psychometric Indicators to Detect Insomnia Cases and Evaluate Treatment Response. Sleep 2011, 34, 601–608. [Google Scholar] [CrossRef] [PubMed]
- Meikle, M.B. Electronic access to tinnitus data: The Oregon Tinnitus Data Archive. Otolaryngol. Neck Surg. 1997, 117, 698–700. [Google Scholar] [CrossRef]
- Sanchez, T.G.; de Medeiros, R.T.; Levy, C.P.D.; Ramalho, J.D.R.O.; Bento, R. Tinnitus in normally hearing patients: Clinical aspects and repercussions. Braz. J. Otorhinolaryngol. 2005, 71, 427–431. [Google Scholar] [CrossRef] [Green Version]
- Hébert, S. Psychological Comorbidities of Tinnitus. Curr. Top. Behav. Neurosci. 2021, 51, 349–359. [Google Scholar]
- Salazar, J.; Meisel, K.; Smith, E.R.; Quiggle, A.; McCoy, D.B.; Amans, M.R. Depression in Patients with Tinnitus: A Systematic Review. Otolaryngol. Neck Surg. 2019, 161, 28–35. [Google Scholar] [CrossRef]
- Hébert, S.; Canlon, B.; Hasson, D.; Hanson, L.L.M.; Westerlund, H.; Theorell, T. Tinnitus Severity Is Reduced with Reduction of Depressive Mood—A Prospective Population Study in Sweden. PLoS ONE 2012, 7, e37733. [Google Scholar]
- Oishi, N.; Shinden, S.; Kanzaki, S.; Saito, H.; Inoue, Y.; Ogawa, K. Influence of depressive symptoms, state anxiety, and pure-tone thresholds on the tinnitus handicap inventory in Japan. Int. J. Audiol. 2011, 50, 491–495. [Google Scholar] [CrossRef]
- Bhatt, J.M.; Bhattacharyya, N.; Lin, H.W. Relationships between tinnitus and the prevalence of anxiety and depression. Laryngoscope 2016, 127, 466–469. [Google Scholar] [CrossRef] [PubMed]
- Ooms, E.; Meganck, R.; Vanheule, S.; Vinck, B.; Watelet, J.-B.; Dhooge, I. Tinnitus severity and the relation to depressive symptoms: A critical study. Otolaryngol. Head Neck Surg. 2011, 26, 667. [Google Scholar] [CrossRef] [PubMed]
- Joos, K.; Vanneste, S.; De Ridder, D. Disentangling Depression and Distress Networks in the Tinnitus Brain. PLoS ONE 2012, 7, e40544. [Google Scholar] [CrossRef] [PubMed]
- Clifford, R.E.; Maihofer, A.X.; Stein, M.B.; Ryan, A.F.; Nievergelt, C.M. Novel Risk Loci in Tinnitus and Causal Inference with Neuropsychiatric Disorders Among Adults of European Ancestry. JAMA Otolaryngol. Neck Surg. 2020, 146, 1015–1025. [Google Scholar] [CrossRef] [PubMed]
- Rauschecker, J.P.; Leaver, A.M.; Mühlau, M. Tuning Out the Noise: Limbic-Auditory Interactions in Tinnitus. Neuron 2010, 66, 819–826. [Google Scholar] [CrossRef]
- De Ridder, D.; Elgoyhen, A.B.; Romo, R.; Langguth, B. Phantom percepts: Tinnitus and pain as persisting aversive memory networks. Proc. Natl. Acad. Sci. USA 2011, 108, 8075–8080. [Google Scholar] [CrossRef]
- Kalmbach, D.A.; Anderson, J.R.; Drake, C.L. The impact of stress on sleep: Pathogenic sleep reactivity as a vulnerability to insomnia and circadian disorders. J. Sleep Res. 2018, 27, e12710. [Google Scholar] [CrossRef] [PubMed]
- van Someren, E.J.W. Brain mechanisms of insomnia: New perspectives on causes and consequences. Physiol. Rev. 2021, 101, 995–1046. [Google Scholar] [CrossRef]
- Park, H.-M.; Jung, J.; Kim, J.-K.; Lee, Y.-J. Tinnitus and Its Association with Mental Health and Health-Related Quality of Life in an Older Population: A Nationwide Cross-Sectional Study. J. Appl. Gerontol. 2022, 41, 181–186. [Google Scholar] [CrossRef] [PubMed]
- Wilson, C.; Lewis, P.; Stephens, D. The short form 36 (SF36) in a specialist tinnitus clinic: La forma corta 36 (SF36) en una clínica especializada en acüfenos. Int. J. Audiol. 2002, 41, 216–220. [Google Scholar] [CrossRef] [PubMed]
- Boecking, B.; Biehl, R.; Brueggemann, P.; Mazurek, B. Health-Related Quality of Life, Depressive Symptoms, Anxiety, and Somatization Symptoms in Male and Female Patients with Chronic Tinnitus. J. Clin. Med. 2021, 10, 2798. [Google Scholar] [CrossRef] [PubMed]
- Szentkiralyi, A.; Madarász, C.Z.; Novak, M. Sleep disorders: Impact on daytime functioning and quality of life. Expert Rev. Pharm. Outcomes Res. 2009, 9, 49–64. [Google Scholar] [CrossRef] [PubMed]
- Edvall, N.; Gunan, E.; Genitsaridi, E.; Lazar, A.; Mehraei, G.; Billing, M.; Tullberg, M.; Bulla, J.; Whitton, J.; Canlon, B.; et al. Impact of Temporomandibular Joint Complaints on Tinnitus-Related Distress. Front. Neurosci. 2019, 13, 879. [Google Scholar] [CrossRef]
- Folmer, R.L.; Griest, S.E.; Martin, W.H. Chronic Tinnitus as Phantom Auditory Pain. Otolaryngol. Neck Surg. 2001, 124, 394–400. [Google Scholar] [CrossRef]
- Møller, A.R. Tinnitus and pain. Prog. Brain Res. 2007, 166, 47–53. [Google Scholar]
- Vanneste, S.; To, W.T.; De Ridder, D. Tinnitus and neuropathic pain share a common neural substrate in the form of specific brain connectivity and microstate profiles. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2019, 88, 388–400. [Google Scholar] [CrossRef]
- Rauschecker, J.P.; May, E.S.; Maudoux, A.; Ploner, M. Frontostriatal Gating of Tinnitus and Chronic Pain. Trends Cogn. Sci. 2015, 19, 567–578. [Google Scholar] [CrossRef]
- Mathias, J.; Cant, M.; Burke, A. Sleep disturbances and sleep disorders in adults living with chronic pain: A meta-analysis. Sleep Med. 2018, 52, 198–210. [Google Scholar] [CrossRef]
- Angst, F.; Benz, T.; Lehmann, S.; Wagner, S.; Simmen, B.R.; Sandòr, P.S.; Gengenbacher, M.; Angst, J. Extended overview of the longitudinal pain-depression association: A comparison of six cohorts treated for specific chronic pain conditions. J. Affect. Disord. 2020, 273, 508–516. [Google Scholar] [CrossRef]
- Boecking, B.; Rose, M.; Brueggemann, P.; Mazurek, B. Two birds with one stone.–Addressing depressive symptoms, emotional tension and worry improves tinnitus-related distress and affective pain perceptions in patients with chronic tinnitus. PLoS ONE 2021, 16, e0246747. [Google Scholar] [CrossRef] [PubMed]
- Niemann, U.; Boecking, B.; Brueggemann, P.; Mazurek, B.; Spiliopoulou, M. Gender-Specific Differences in Patients with Chronic Tinnitus—Baseline Characteristics and Treatment Effects. Front. Neurosci. 2020, 14, 487. [Google Scholar] [CrossRef] [PubMed]
- Seydel, C.; Haupt, H.; Olze, H.; Szczepek, A.J.; Mazurek, B. Gender and chronic tinnitus: Differences in tinnitus-related distress depend on age and duration of tinnitus. Ear Hear 2013, 34, 661–672. [Google Scholar] [CrossRef] [PubMed]
- Baker, F.C.; Lampio, L.; Saaresranta, T.; Polo-Kantola, P. Sleep and Sleep Disorders in the Menopausal Transition. Sleep Med. Clin. 2018, 13, 443–456. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sample (N = 2344, 100.00%) | (Very) Dissatisfied (N = 959, 40.91%) | Neutral (N = 415, 17.70%) | (Very) Satisfied (N = 970, 41.38%) | Test Statistic (Degrees of Freedom) | p-Value |
|---|---|---|---|---|---|
| Age | H = 3.01 (2) | 1 | |||
| Mean (SD) | 56.6 (12.4) | 55.6 (13.2) | 55.9 (13.7) | ||
| Median [Min, Max] | 57.0 [19.0, 87.0] | 57.0 [0, 90.0] | 56.0 [19.0, 92.0] | ||
| Sex | H = 6.7 (2) | 0.345 | |||
| Female | 366 (38.2%) | 132 (31.8%) | 327 (33.7%) | ||
| Male | 593 (61.8%) | 283 (68.2%) | 643 (66.3%) | ||
| MDI score | H = 619.4 (2) | <0.001 | |||
| Mean (SD) | 21.0 (11.6) | 14.1 (9.81) | 8.94 (7.99) | ||
| Median [Min, Max] | 19.0 [1.00, 50.0] | 11.0 [0, 48.0] | 6.00 [0, 45.0] | ||
| THI score | H = 599.9 (2) | <0.001 | |||
| Mean (SD) | 58.8 (22.0) | 47.9 (21.4) | 36.7 (20.5) | ||
| Median [Min, Max] | 60.0 [2.00, 100] | 46.0 [4.00, 100] | 34.0 [0, 96.0] | ||
| Missing | 6 (0.6%) | 3 (0.7%) | 10 (1.0%) | ||
| TQ Score | H = 586.1 (2) | <0.001 | |||
| Mean (SD) | 49.2 (16.7) | 39.9 (16.3) | 31.6 (15.4) | ||
| Median [Min, Max] | 51.0 [2.00, 83.0] | 40.0 [4.00, 80.0] | 30.0 [0, 79.0] | ||
| Missing | 179 (18.7%) | 73 (17.6%) | 124 (12.8%) | ||
| Physical health (WHOQOL-BREF) | H = 1262.1 (2) | <0.001 | |||
| Mean (SD) | 11.5 (1.60) | 12.7 (1.45) | 13.8 (1.26) | ||
| Median [Min, Max] | 11.0 [5.00, 17.0] | 13.0 [9.00, 18.0] | 14.0 [9.00, 18.0] | ||
| Missing | 7 (0.7%) | 4 (1.0%) | 3 (0.3%) | ||
| Psychological Health (WHOQOL-BREF) | H = 401.7 (2) | <0.001 | |||
| Mean (SD) | 12.9 (2.16) | 13.7 (1.89) | 14.5 (1.68) | ||
| Median [Min, Max] | 13.0 [6.00, 18.0] | 14.0 [7.00, 18.0] | 15.0 [7.00, 18.0] | ||
| Missing | 7 (0.7%) | 3 (0.7%) | 4 (0.4%) | ||
| Social Factors (WHOQOL-BREF) | H = 194.5 (2) | <0.001 | |||
| Mean (SD) | 13.7 (3.43) | 14.6 (3.09) | 15.5 (3.00) | ||
| Median [Min, Max] | 15.0 [4.00, 20.0] | 15.0 [4.00, 20.0] | 16.0 [4.00, 20.0] | ||
| Missing | 10 (1.0%) | 0 (0%) | 7 (0.7%) | ||
| Environment (WHOQOL-BREF) | H = 291.5 (2) | <0.001 | |||
| Mean (SD) | 15.8 (2.31) | 16.5 (2.08) | 17.3 (1.92) | ||
| Median [Min, Max] | 16.0 [6.00, 20.0] | 17.0 [10.0, 20.0] | 18.0 [9.00, 20.0] | ||
| Missing | 4 (0.4%) | 1 (0.2%) | 0 (0%) | ||
| Family Member with Tinnitus | χ2 = 0.3 (2) | 1 | |||
| yes | 242 (25.2%) | 102 (24.6%) | 234 (24.1%) | ||
| no | 693 (72.3%) | 303 (73.0%) | 709 (73.1%) | ||
| Missing | 24 (2.5%) | 10 (2.4%) | 27 (2.8%) | ||
| Tinnitus initial Onset | χ2 = 1.01 (2) | 1 | |||
| gradual | 440 (45.9%) | 183 (44.1%) | 458 (47.2%) | ||
| abrupt | 467 (48.7%) | 212 (51.1%) | 470 (48.5%) | ||
| Missing | 52 (5.4%) | 20 (4.8%) | 42 (4.3%) | ||
| Pulsating Tinnitus | χ2 = 22.9 (4) | 0.002 | |||
| yes, with the heartbeat | 116 (12.1%) | 47 (11.3%) | 79 (8.1%) | ||
| Yes, not with the heartbeat | 113 (11.8%) | 45 (10.8%) | 72 (7.4%) | ||
| no | 704 (73.4%) | 316 (76.1%) | 801 (82.6%) | ||
| Missing | 26 (2.7%) | 7 (1.7%) | 18 (1.9%) | ||
| Tinnitus Location | χ2 = 4.4 (6) | 1 | |||
| Unilateral | 256 (26.7%) | 119 (28.7%) | 291 (30.0%) | ||
| Bilateral | 579 (60.4%) | 247 (59.5%) | 551 (56.8%) | ||
| Head | 103 (10.7%) | 47 (11.3%) | 107 (11.0%) | ||
| Elsewhere | 1 (0.1%) | 0 (0%) | 0 (0%) | ||
| Missing | 20 (2.1%) | 2 (0.5%) | 21 (2.2%) | ||
| Tinnitus Presentation | χ2 = 12.2 (2) | 0.033 | |||
| intermittent | 114 (11.9%) | 77 (18.6%) | 156 (16.1%) | ||
| constant | 832 (86.8%) | 335 (80.7%) | 798 (82.3%) | ||
| Missing | 13 (1.4%) | 3 (0.7%) | 16 (1.6%) | ||
| Loudness Fluctuation | χ2 = 8.8 (2) | 0.145 | |||
| yes | 612 (63.8%) | 279 (67.2%) | 571 (58.9%) | ||
| no | 330 (34.4%) | 132 (31.8%) | 378 (39.0%) | ||
| Missing | 17 (1.8%) | 4 (1.0%) | 21 (2.2%) | ||
| Subjective Loudness | H = 144.3 (2) | <0.001 | |||
| Mean (SD) | 73.7 (64.5) | 68.3 (68.9) | 66.3 (84.4) | ||
| Median [Min, Max] | 70.0 [1.00, 999] | 70.0 [5.00, 999] | 60.0 [0, 999] | ||
| Missing | 39 (4.1%) | 12 (2.9%) | 43 (4.4%) | ||
| Type of Tinnitus | χ2 = 6.1 (6) | 1 | |||
| tone | 596 (62.1%) | 277 (66.7%) | 602 (62.1%) | ||
| noise | 120 (12.5%) | 39 (9.4%) | 107 (11.0%) | ||
| crickets | 135 (14.1%) | 50 (12.0%) | 149 (15.4%) | ||
| others | 83 (8.7%) | 35 (8.4%) | 85 (8.8%) | ||
| Missing | 25 (2.6%) | 14 (3.4%) | 27 (2.8%) | ||
| Tinnitus Pitch | χ2 = 14.4 (6) | 0.281 | |||
| Very High Frequency | 275 (28.7%) | 108 (26.0%) | 248 (25.6%) | ||
| High Frequency | 481 (50.2%) | 219 (52.8%) | 472 (48.7%) | ||
| Medium Frequency | 136 (14.2%) | 59 (14.2%) | 179 (18.5%) | ||
| Low Frequency | 18 (1.9%) | 8 (1.9%) | 33 (3.4%) | ||
| Missing | 49 (5.1%) | 21 (5.1%) | 38 (3.9%) | ||
| Sounds suppress tinnitus | χ2 = 14.6 (4) | 0.073 | |||
| yes | 594 (61.9%) | 275 (66.3%) | 675 (69.6%) | ||
| no | 201 (21.0%) | 67 (16.1%) | 156 (16.1%) | ||
| not known | 140 (14.6%) | 69 (16.6%) | 125 (12.9%) | ||
| Missing | 24 (2.5%) | 4 (1.0%) | 14 (1.4%) | ||
| Sounds worsens Tinnitus | χ2 = 14.9 (4) | 0.069 | |||
| yes | 554 (57.8%) | 232 (55.9%) | 519 (53.5%) | ||
| no | 210 (21.9%) | 93 (22.4%) | 277 (28.6%) | ||
| not known | 181 (18.9%) | 88 (21.2%) | 161 (16.6%) | ||
| Missing | 14 (1.5%) | 2 (0.5%) | 13 (1.3%) | ||
| Somatic Tinnitus | χ2 = 5.3 (4) | 1 | |||
| yes | 380 (39.6%) | 155 (37.3%) | 355 (36.6%) | ||
| no | 561 (58.5%) | 256 (61.7%) | 598 (61.6%) | ||
| not known | 3 (0.3%) | 1 (0.2%) | 8 (0.8%) | ||
| Missing | 15 (1.6%) | 3 (0.7%) | 9 (0.9%) | ||
| Effect of Naps on Tinnitus | χ2 = 10.9 (6) | 0.799 | |||
| no effect | 626 (65.3%) | 277 (66.7%) | 676 (69.7%) | ||
| no info | 38 (4.0%) | 15 (3.6%) | 30 (3.1%) | ||
| reduces | 81 (8.4%) | 39 (9.4%) | 101 (10.4%) | ||
| worsens | 174 (18.1%) | 68 (16.4%) | 131 (13.5%) | ||
| Missing | 40 (4.2%) | 16 (3.9%) | 32 (3.3%) | ||
| Sleep influences Tinnitus | χ2 = 90.1 (4) | <0.001 | |||
| yes | 269 (28.1%) | 88 (21.2%) | 141 (14.5%) | ||
| no | 245 (25.5%) | 128 (30.8%) | 419 (43.2%) | ||
| Not Known | 408 (42.5%) | 187 (45.1%) | 379 (39.1%) | ||
| Missing | 37 (3.9%) | 12 (2.9%) | 31 (3.2%) | ||
| Effect of Stress on Tinnitus | χ2 = 24.5 (4) | 0.001 | |||
| worsens | 719 (75.0%) | 296 (71.3%) | 650 (67.0%) | ||
| improves | 10 (1.0%) | 8 (1.9%) | 7 (0.7%) | ||
| no effect | 195 (20.3%) | 98 (23.6%) | 285 (29.4%) | ||
| Missing | 35 (3.6%) | 13 (3.1%) | 28 (2.9%) | ||
| Hearing Difficulties | χ2 = 0.03 (2) | 1 | |||
| yes | 572 (59.6%) | 248 (59.8%) | 579 (59.7%) | ||
| no | 366 (38.2%) | 157 (37.8%) | 375 (38.7%) | ||
| Missing | 21 (2.2%) | 10 (2.4%) | 16 (1.6%) | ||
| Wears Hearing Aids | χ2 = 6 (6) | <0.001 | |||
| right | 28 (2.9%) | 11 (2.7%) | 15 (1.5%) | ||
| left | 24 (2.5%) | 8 (1.9%) | 30 (3.1%) | ||
| both | 121 (12.6%) | 55 (13.3%) | 121 (12.5%) | ||
| none | 761 (79.4%) | 332 (80.0%) | 779 (80.3%) | ||
| Missing | 25 (2.6%) | 9 (2.2%) | 25 (2.6%) | ||
| Hyperacusis | χ2 = 53.8 (8) | <0.001 | |||
| never | 76 (7.9%) | 41 (9.9%) | 115 (11.9%) | ||
| rarely | 106 (11.1%) | 56 (13.5%) | 151 (15.6%) | ||
| sometimes | 343 (35.8%) | 158 (38.1%) | 381 (39.3%) | ||
| usually | 172 (17.9%) | 86 (20.7%) | 174 (17.9%) | ||
| always | 248 (25.9%) | 71 (17.1%) | 137 (14.1%) | ||
| Missing | 14 (1.5%) | 3 (0.7%) | 12 (1.2%) | ||
| Pain from Noises | χ2 = 53.5 (8) | <0.001 | |||
| never | 76 (7.9%) | 41 (9.9%) | 115 (11.9%) | ||
| rarely | 106 (11.1%) | 56 (13.5%) | 151 (15.6%) | ||
| sometimes | 343 (35.8%) | 158 (38.1%) | 381 (39.3%) | ||
| usually | 172 (17.9%) | 86 (20.7%) | 174 (17.9%) | ||
| always | 248 (25.9%) | 71 (17.1%) | 137 (14.1%) | ||
| Missing | 14 (1.5%) | 3 (0.7%) | 12 (1.2%) | ||
| Headaches | χ2 = 69.5 (2) | <0.001 | |||
| yes | 443 (46.2%) | 157 (37.8%) | 275 (28.4%) | ||
| no | 492 (51.3%) | 251 (60.5%) | 681 (70.2%) | ||
| Missing | 24 (2.5%) | 7 (1.7%) | 14 (1.4%) | ||
| Vertigo/Dizziness | χ2 = 35.7 (2) | <0.001 | |||
| yes | 371 (38.7%) | 145 (34.9%) | 256 (26.4%) | ||
| no | 555 (57.9%) | 260 (62.7%) | 688 (70.9%) | ||
| Missing | 33 (3.4%) | 10 (2.4%) | 26 (2.7%) | ||
| TMJ | χ2 = 25.8 (2) | <0.001 | |||
| yes | 317 (33.1%) | 110 (26.5%) | 224 (23.1%) | ||
| no | 621 (64.8%) | 296 (71.3%) | 735 (75.8%) | ||
| Missing | 21 (2.2%) | 9 (2.2%) | 11 (1.1%) | ||
| Neck Pain | χ2 = 58.4 (2) | <0.001 | |||
| yes | 623 (65.0%) | 246 (59.3%) | 469 (48.4%) | ||
| no | 314 (32.7%) | 159 (38.3%) | 482 (49.7%) | ||
| Missing | 22 (2.3%) | 10 (2.4%) | 19 (2.0%) | ||
| Psychiatric Treatment | χ2 = 49.2 (2) | <0.001 | |||
| yes | 241 (25.1%) | 88 (21.2%) | 124 (12.8%) | ||
| no | 703 (73.3%) | 322 (77.6%) | 836 (86.2%) | ||
| Missing | 15 (1.6%) | 5 (1.2%) | 10 (1.0%) |
| (Very) Dissatisfied | Neutral | (Very) Satisfied | |
|---|---|---|---|
| Age | 0.11 | −0.03 | |
| MDI Score | 0.35 | −0.14 | |
| THI Score | −0.04 | ||
| TQ Score | 0.23 | −0.15 | |
| Physical Health (WHOQOL-BREF) | −0.64 | 1.14 | |
| Psychological Health (WHOQOL-BREF) | 0.18 | −0.09 | |
| Social Factors (WHOQOL-BREF) | |||
| Environmental Factors (WHOQOL-BREF) | 0.05 | ||
| Subjective Loudness (TSCHQ) | 0.00 | ||
| Sex (reference: Female) | |||
| Male | −0.20 | ||
| Family Member with Tinnitus (reference: Yes) | |||
| No | −0.04 | ||
| Tinnitus initial Onset (reference: Gradual) | |||
| Abrupt | −0.04 | 0.05 | |
| Pulsating Tinnitus (reference: yes, with the heartbeat) | |||
| Yes, not with the heartbeat | |||
| No | 0.37 | ||
| Tinnitus Location (reference: elsewhere) | |||
| Unilateral | −0.02 | 0.22 | |
| Bilateral | |||
| Inside the head | −0.05 | 0.02 | |
| Tinnitus Presentation (reference: intermittent) | |||
| Constant | 0.05 | −0.10 | |
| Loudness Fluctuations (reference: yes) | |||
| No | 0.05 | −0.05 | |
| Type of Tinnitus (reference: tone) | |||
| Noise | 0.14 | ||
| Crickets | −0.10 | 0.14 | |
| Other | 0.06 | ||
| Tinnitus Pitch (reference: low frequency) | |||
| High Frequency | 0.01 | ||
| Medium Frequency | 0.11 | ||
| Sounds Suppress Tinnitus (reference: yes) | |||
| no | −0.03 | ||
| not known | |||
| Sounds Worsens Tinnitus (reference: yes) | |||
| no | 0.12 | ||
| not known | 0.13 | −0.14 | |
| Somatic Tinnitus (reference: yes) | |||
| no | 0.03 | −0.08 | |
| Effect of Naps on Tinnitus (reference: not know) | |||
| no effect | |||
| improves tinnitus | −0.10 | 0.02 | |
| worsens tinnitus | 0.02 | −0.21 | |
| Sleep influences Tinnitus (reference: yes) | |||
| no | −0.10 | 0.34 | |
| not known | −0.23 | ||
| No effect | 0.06 | ||
| Hearing Difficulties (reference: yes) | |||
| no | 0.01 | −0.07 | |
| Wears Hearing Aid (reference: one ear) | |||
| Both Ears | 0.20 | ||
| None | 0.01 | −0.02 | |
| Hyperacusis (reference: never) | |||
| Rarely | 0.02 | −0.03 | |
| Sometimes | 0.03 | ||
| Usually | −0.15 | ||
| Always | 0.10 | ||
| Pain from Noises (reference: never) | |||
| Rarely | |||
| Sometimes | |||
| Usually | 0.01 | ||
| Always | −0.01 | ||
| Headaches (reference: yes) | |||
| No | −0.20 | ||
| Vertigo (reference: yes) | |||
| No | 0.11 | −0.14 | |
| TMJ (reference: yes) | |||
| No | −0.05 | ||
| Neck Pain (reference: Yes) | |||
| No | −0.11 | 0.18 | |
| Psychiatric Treatment (reference: Yes) | |||
| No | −0.16 |
| True Group | |||
|---|---|---|---|
| Model Prediction | (Very) Dissatisfied | Neutral | (Very) Satisfied |
| (very) dissatisfied | 151 | 37 | 22 |
| Neutral | 0 | 0 | 1 |
| (very) satisfied | 31 | 48 | 165 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Weber, F.C.; Schlee, W.; Langguth, B.; Schecklmann, M.; Schoisswohl, S.; Wetter, T.C.; Simões, J. Low Sleep Satisfaction Is Related to High Disease Burden in Tinnitus. Int. J. Environ. Res. Public Health 2022, 19, 11005. https://doi.org/10.3390/ijerph191711005
Weber FC, Schlee W, Langguth B, Schecklmann M, Schoisswohl S, Wetter TC, Simões J. Low Sleep Satisfaction Is Related to High Disease Burden in Tinnitus. International Journal of Environmental Research and Public Health. 2022; 19(17):11005. https://doi.org/10.3390/ijerph191711005
Chicago/Turabian StyleWeber, Franziska C., Winfried Schlee, Berthold Langguth, Martin Schecklmann, Stefan Schoisswohl, Thomas C. Wetter, and Jorge Simões. 2022. "Low Sleep Satisfaction Is Related to High Disease Burden in Tinnitus" International Journal of Environmental Research and Public Health 19, no. 17: 11005. https://doi.org/10.3390/ijerph191711005