
How Did the COVID-19 Pandemic Affect Population Mobility in Taiwan?



Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. COVID-19 Pandemic in Taiwan
2.3. Study Population
2.4. Ethical Issues
2.5. Statistics
3. Results
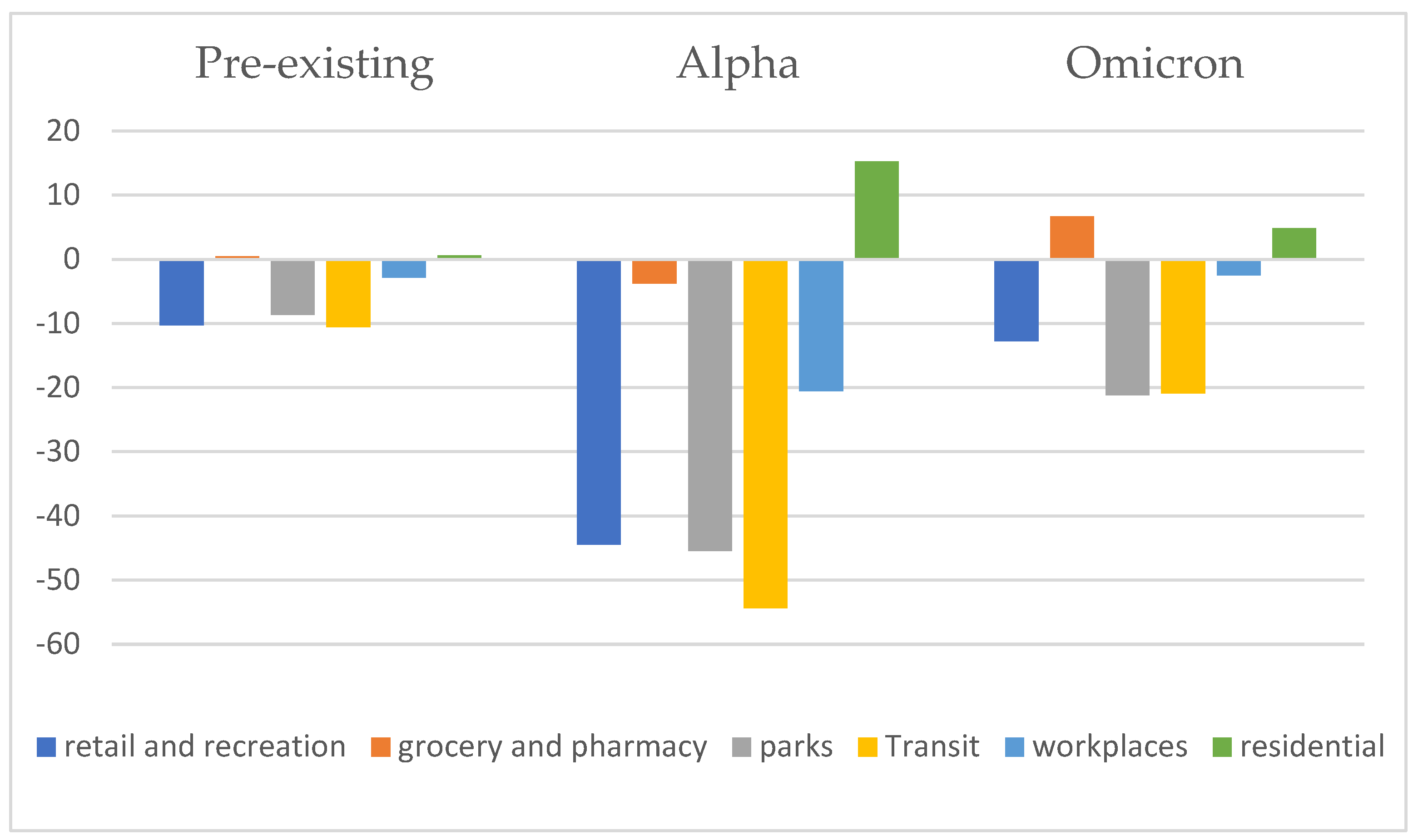
3.1. Changes in the Population Flow at Each Place in the Pre-Existing, Alpha, and Omicron Waves
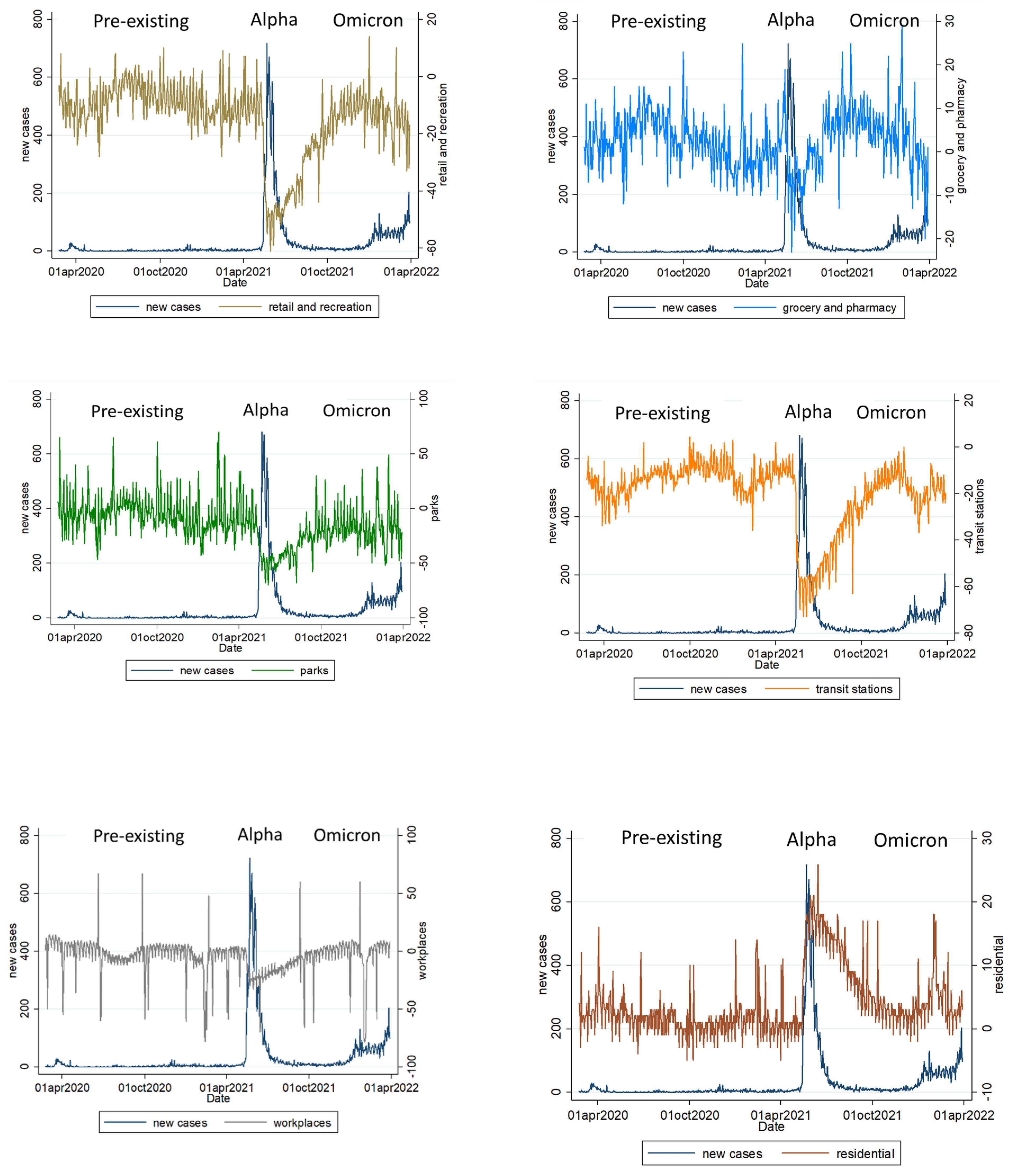
3.2. The Relationship between Changes in the Population Visits for Various Locations and the Number of Daily New Confirmed Cases Per Million People (7-Day Rolling Average)
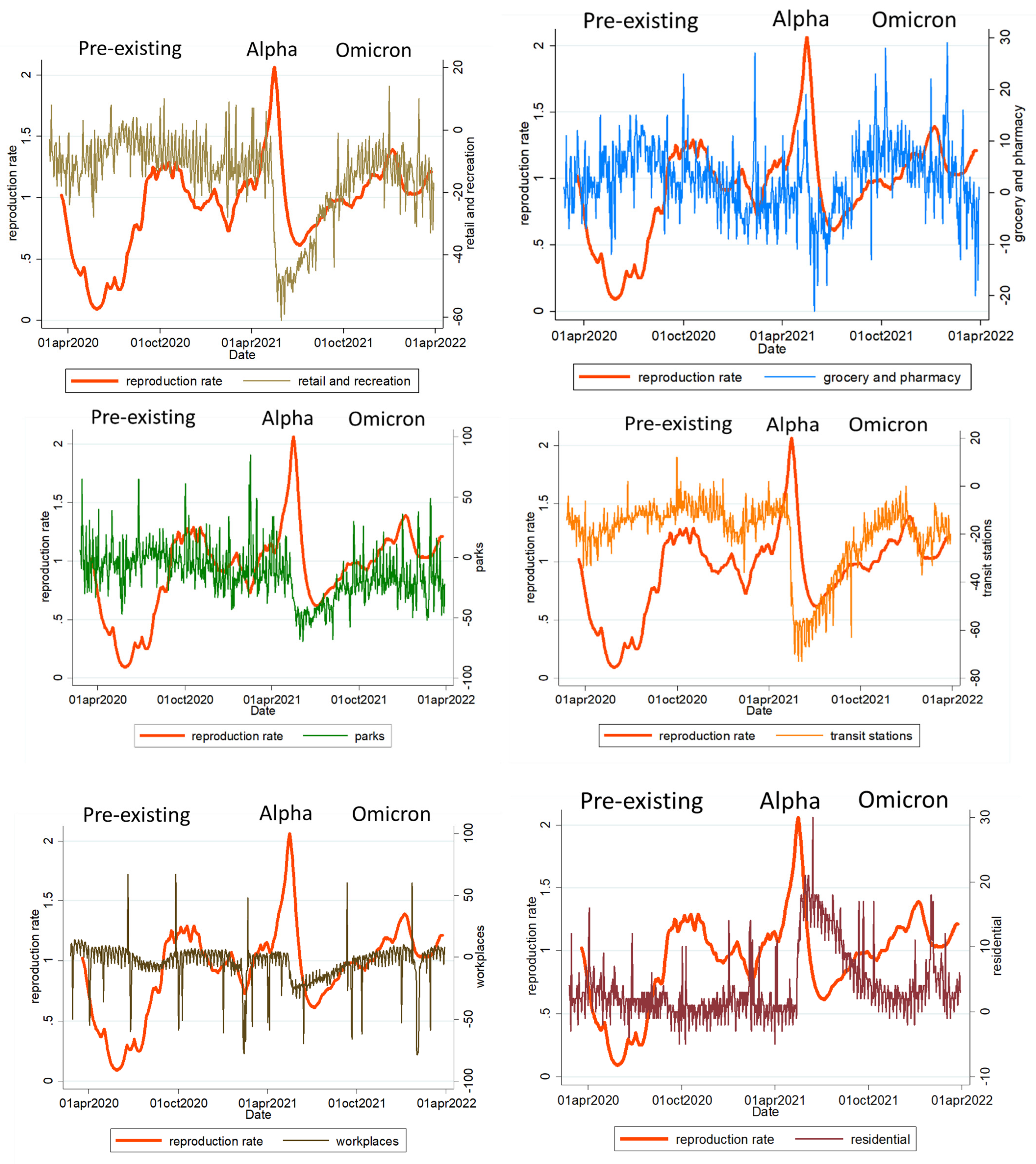
3.3. The Relationship between Changes in the Population Visits of Various Locations and the Reproduction Rate (7-Day Rolling Average)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Coronaviridae Study Group of the International Committee on Taxonomy of Viruses. The species severe acute respiratory syndrome-related coronavirus: Classifying 2019-nCoV and naming it SARS-CoV-2. Nat. Microbiol. 2020, 5, 536–544. [Google Scholar] [CrossRef]
- Cui, J.; Li, F.; Shi, Z.L. Origin and evolution of pathogenic coronaviruses. Nat. Rev. Microbiol. 2019, 17, 181–192. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease 2019 (COVID-19). Situation Report—51. 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200311-sitrep-51-covid-19.pdf?sfvrsn=1ba62e57_10 (accessed on 13 March 2022).
- WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 13 March 2022).
- Zhang, R.; Li, Y.; Zhang, A.L.; Wang, Y.; Molina, M.J. Identifying airborne transmission as the dominant route for the spread of COVID-19. Proc. Natl. Acad. Sci. USA 2020, 117, 14857–14863. [Google Scholar] [CrossRef]
- He, X.; Lau, E.H.Y.; Peng, W.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; et al. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef]
- Petersen, E.; Koopmans, M.; Go, U.; Hamer, D.H.; Petrosillo, N.; Castelli, F.; Storgaard, M.; Al Khalili, S.; Simonsen, L. Comparing SARS-CoV-2 with SARS-CoV and influenza pandemics. Lancet Infect. Dis. 2020, 20, e238–e244. [Google Scholar] [CrossRef]
- Harvey, W.T.; COVID-19 Genomics UK (COG-UK) Consortium; Peacock, S.J.; Robertson, D.L. SARS-CoV-2 variants, spike mutations and immune escape. Nat. Rev. Microbiol. 2021, 19, 409–424. [Google Scholar] [CrossRef] [PubMed]
- UC Davis Health. Omicron Variant: What We Know about This COVID-19 Strain. 2022. Available online: https://health.ucdavis.edu/coronavirus/covid-19-information/omicron-variant (accessed on 1 May 2020).
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.M.; et al. COVID-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef] [PubMed]
- Thompson, M.G.; Natarajan, K.; Irving, S.A.; Rowlet, E.A.; Griggs, E.P.; Gaglani, M.; Klein, N.P.; Grannis, S.J.; DeSilva, M.B.; Stenehjem, E.; et al. Effectiveness of a Third Dose of mRNA Vaccines Against COVID-19–Associated Emergency Department and Urgent Care Encounters and Hospitalizations Among Adults During Periods of Delta and Omicron Variant Predominance—VISION Network, 10 States, August 2021–January 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 139–145. [Google Scholar] [PubMed]
- Taiwan Centers for Disease Control. Attention COVID-19. Available online: https://www.cdc.gov.tw/En (accessed on 1 April 2022).
- Chang, Y.T.; Lin, C.-Y.; Tsai, M.-J.; Hung, C.-T.; Hsu, C.-W.; Lu, P.-L.; Hou, M.F. Infection control measures of a Taiwanese hospital to confront the COVID-19 pandemic. Kaohsiung J. Med. Sci. 2020, 36, 296–304. [Google Scholar] [CrossRef] [PubMed]
- Our World in Data. Explore the Global Data on Confirmed COVID-19 Cases in Taiwan. Available online: https://ourworldindata.org/covid-cases (accessed on 1 April 2022).
- Kephart, J.L.; Delclòs-Alió, X.; Rodríguez, D.A.; Sarmiento, O.L.; Barrientos-Gutiérrez, T.; Ramirez-Zea, M.; Quistberg, D.A.; Bilal, U.; Roux, A.V.D. The effect of population mobility on COVID-19 incidence in 314 Latin American cities: A longitudinal ecological study with mobile phone location data. Lancet Digit Health 2021, 3, e716–e722. [Google Scholar] [CrossRef]
- Drake, T.M.; Docherty, A.B.; Weiser, T.G.; Yule, S.; Sheikh, A.; Harrison, E.M. The effects of physical distancing on population mobility during the COVID-19 pandemic in the UK. Lancet Digit Health 2020, 2, e385–e387. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, Z.; Rader, B.; Li, B.; Wu, C.H.; Whittington, J.D.; Zheng, P.; Stenseth, N.C.; Bjornstad, O.N.; Brownstein, J.S.; et al. Associations between changes in population mobility in response to the COVID-19 pandemic and socioeconomic factors at the city level in China and country level worldwide: A retrospective, observational study. Lancet Digit Health 2021, 3, e349–e359. [Google Scholar] [CrossRef]
- Yuan, B.; Zhao, H.; Li, J. Health policy response to mobility during the pandemic: Evaluating the effectiveness using location-based services big data. Int. J. Health Plan. Manag. 2022. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 Community Mobility Reports. See How Your Community is Moving around Differently due to COVID-19. Available online: https://www.google.com/covid19/mobility/ (accessed on 1 May 2022).
- Center for Disease Control and Prevention. Potential Rapid Increase of Omicron Variant Infections in the United States. Available online: https://www.cdc.gov/coronavirus/2019-ncov/science/forecasting/mathematical-modeling-outbreak.html (accessed on 1 May 2022).
- Ren, S.-Y.; Wang, W.-B.; Gao, R.-D.; Zhou, A.-M. Omicron variant (B.1.1.529) of SARS-CoV-2: Mutation, infectivity, transmission, and vaccine resistance. World J. Clin. Cases 2022, 10, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Accorsi, E.K.; Britton, A.; Fleming-Dutra, K.E.; Smith, Z.R.; Shang, N.; Derado, G.; Miller, J.; Schrag, S.J.; Verani, J.R. Association Between 3 Doses of mRNA COVID-19 Vaccine and Symptomatic Infection Caused by the SARS-CoV-2 Omicron and Delta Variants. JAMA 2022, 327, 639–651. [Google Scholar] [CrossRef] [PubMed]
- Altarawneh, H.N.; Hasan, M.R.; Ayoub, H.H.; Qassim, S.; Coyle, P.; Yassine, H.; Al-Khatib, H.A.; Benslimane, F.M.; Al-Kanaani, Z. Protection against the Omicron Variant from Previous SARS-CoV-2 Infection. N. Engl. J. Med. 2022, 386, 1288–1290. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Pre-Existing | Alpha | Omicron | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Average | Medium | Max | Average | Medium | Max | Average | Medium | Max | |
| New case | 4.39 | 4 | 25 | 217.37 | 175 | 723 | 56.91 | 57.5 | 129 |
| retail and recreation | −10.288 | −12 | 7 | −44.51 | −46 | −61 | −12.77 | −11 | −27 |
| grocery and pharmacy | 0.48 | 1 | −11 | −3.82 | −4 | −23 | 6.67 | 4.5 | −6 |
| Parks | −8.71 | −13 | −38 | −45.46 | −45.73 | −70 | −21.22 | −22 | −50 |
| Transit stations | −10.61 | −11 | −18 | −54.4 | −56 | −73 | −20.94 | −20 | −37 |
| Workplaces | −2.90 | 1 | −59 | −20.58 | −22 | −70 | −2.56 | 3 | −79 |
| Residential | 0.60 | 1 | −5 | 15.26 | 16.5 | −1 | 4.84 | 4 | 0 |
| Coef. | 95% CI | p-Value | |
|---|---|---|---|
| Retail and recreation | −1.233 | −2.594~0.128 | 0.076 |
| Grocery and pharmacy | −1.332 | −2.327~−0.338 | 0.009 |
| Park | 0.277 | −0.177~0.731 | 0.231 |
| Transit stations | −1.397 | −2.467~−0.328 | 0.011 |
| workplaces | 0.250 | −0.282–0.781 | 0.357 |
| residential | 3.882 | 1.259–6.504 | 0.004 |
| Coef. | 95% CI | p-Value | |
|---|---|---|---|
| Retail and recreation | −0.023 | −0.044~−0.002 | 0.031 |
| Grocery and pharmacy | 0.007 | −0.008~0.023 | 0.357 |
| Park | −0.005 | −0.013~0.002 | 0.150 |
| Transit stations | 0.023 | 0.006~0.040 | 0.008 |
| Workplaces | −0.008 | −0.017~0.000 | 0.062 |
| Residential | −0.055 | −0.240~0.130 | 0.517 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, S.-F.; Chang, H.-C.; Liu, J.-F.; Kuo, H.-C. How Did the COVID-19 Pandemic Affect Population Mobility in Taiwan? Int. J. Environ. Res. Public Health 2022, 19, 10559. https://doi.org/10.3390/ijerph191710559
Liu S-F, Chang H-C, Liu J-F, Kuo H-C. How Did the COVID-19 Pandemic Affect Population Mobility in Taiwan? International Journal of Environmental Research and Public Health. 2022; 19(17):10559. https://doi.org/10.3390/ijerph191710559
Chicago/Turabian StyleLiu, Shih-Feng, Hui-Chuan Chang, Jui-Fang Liu, and Ho-Chang Kuo. 2022. "How Did the COVID-19 Pandemic Affect Population Mobility in Taiwan?" International Journal of Environmental Research and Public Health 19, no. 17: 10559. https://doi.org/10.3390/ijerph191710559