
‘A Lot of People Just Go for Walks, and Don’t Do Anything Else’: Older Adults in the UK Are Not Aware of the Strength Component Embedded in the Chief Medical Officers’ Physical Activity Guidelines—A Qualitative Study

 ,
, 
Abstract
:1. Introduction
- Research Questions
- 1.
- Are older adults aware of the strength recommendations that have been embedded within the Chief Medical Officers’ physical activity guidelines since 2011?
- 2.
- Do older adults believe they are meeting these strength recommendations? If so, how? That is, what activities are they using to meet the strength recommendations?
2. Materials and Methods
3. Results
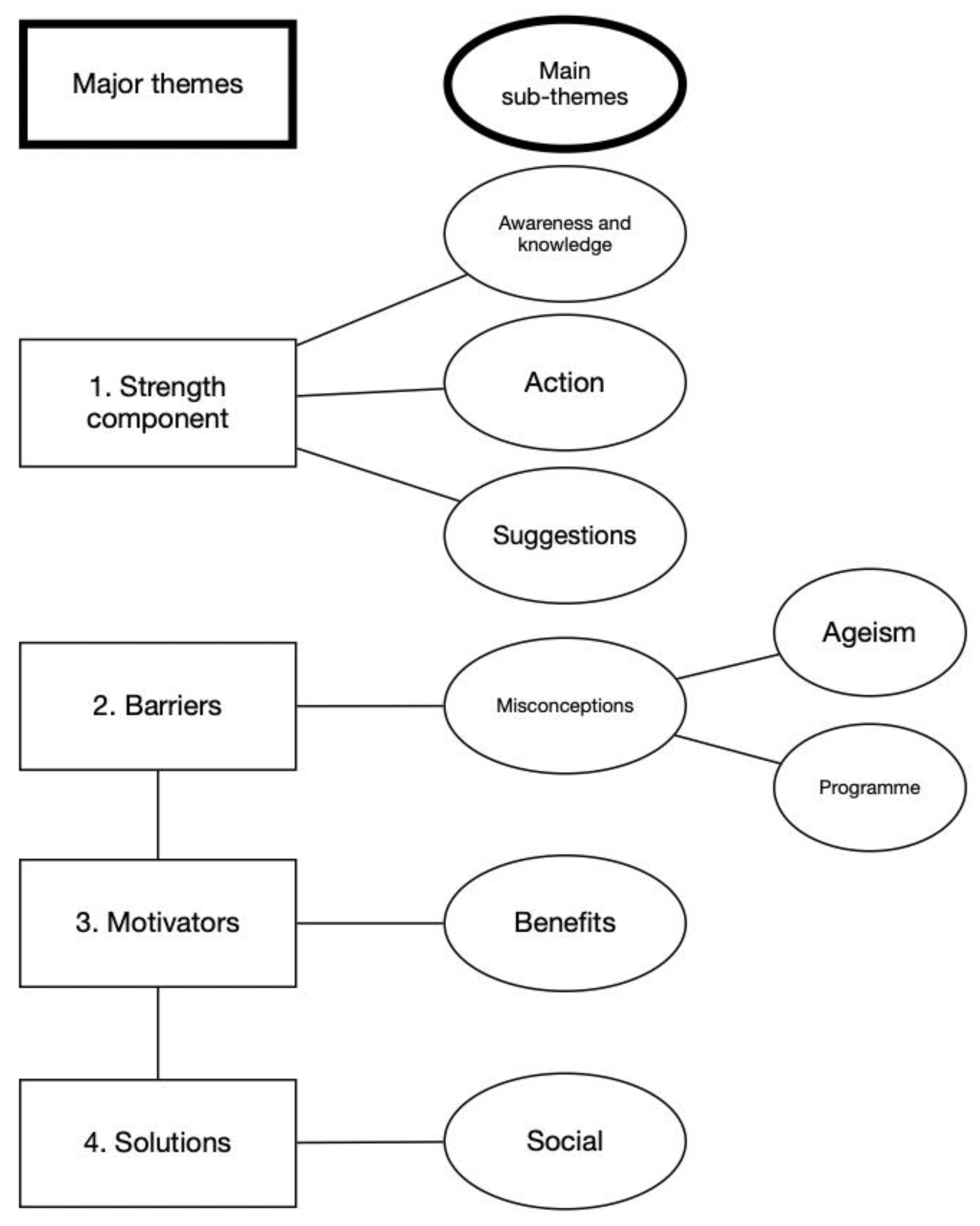
3.1. Major Theme 1—Strength Component of the Chief Medical Officers’ Physical Activity Guidelines (CMO PAG)
3.1.1. Main Sub-Theme 1a—Awareness and Knowledge
I think it’s something around, you know, making sure that you’ve got a…your active enough to make yourself a bit out of breath and exercise at least thirty minutes, I think. I can’t remember any of the other things, I am sure there are more things in it than that.(M5, 65)
I think the advice seems to be to keep moving as much as you can.(F4, 71)
I honestly can’t say that I ever recall seeing that.(M2, 68)
The answer is probably no. So, no, I hadn’t come across the guidelines.(F5, 71)
Well, I’ve not heard of the Government target for that, but I’ve heard people, older people, in particular, talking about that. You know, just to maintain your physical, you know, your skeletal stuff in good order, yes… some kind of weight bearing exercises.(M5, 65)
But, no, because I’ve got my own routine, you know, I hear it, I hear it on news programmes. I don’t pay a lot of notice to it because I’m probably doing that and more anyway.(M8, 67)
…but it seems the lowest amount of time to me, so I think the Government guidelines are probably the minimum, but I don’t know, I’m not an expert.(F4, 71)
3.1.2. Main Sub-Theme 1b—Action
I mean there is a lot of building strength in the [walking] football I do, for instance.(M7, 66)
I do a lot of yoga, so it would be standing postures in yoga, walking uphill, bit of running, that kind of thing…(M4, 69)
I do, I think I’m more than meeting them because I do resistance training in Pilates, I do masses of walking, which is a muscle strengthening thing.(F4, 71)
Certainly, the hydrotherapy session, which I’ve had this morning. The Pilates, yes. The cycling, yes. And the walking, yes.(M3, 71)
I don’t do anything…other than the running and the swimming, I don’t do anything that’s strength-related, or I guess…so I guess there’s nothing for the upper body. I guess my legs get strong with the running.(M2, 68)
I don’t think yoga would because that’s more flexibility, isn’t it, so the answer to that, I think, would be no.(M6, 68)
I’m not as disciplined over that, I guess, as I am the other physical activities that I do.(M5, 65)
I’m not meeting that, no, no.(F1, 68)
3.1.3. Main Sub-Theme 1c—Suggestions for Improvements to the Chief Medical Officers’ Physical Activity Guidelines (CMO PAG)
It’s a bit subjective as to what counts as building strength.(M7, 66)
Depends on what you mean by strength.(M8, 67)
I mean, they’re sort of general, keep active, you know, but really vague. I mean, there’s a lot around prevention of cancer, and I suppose quite a lot about prevention of heart disease. And a lot of the exercise is geared towards heart disease. But, it’s more disease specific, you know, shorter goals, shorter term goals, I suppose.(F3, 71)
GPs could give out the…you know, a more direct message, I just don’t get the feeling that there’s enough. I’m not convinced that as a society we’re putting it in people’s faces enough. If you go to the doctor’s surgery, why is everybody not given a leaflet?(M6, 68)
I don’t know how many GPs do exercise on prescription because that’s another good thing they could do more of.(F7, 70)
3.2. Major Theme 2—Barriers to Strength Training Participation
I tried it once or twice, but, you know, they are just too boring… I just couldn’t do it as much as I need to because it just doesn’t grab me enough. I’m easily bored. It’s got to be faster and the constant activity and decision making. I’d rather do something useful. But just going to a gym and doing this for an hour, what’s the point? It doesn’t get you anywhere, does it? Literally.(M7, 66)
I don’t enjoy it. (a) I’ve never done it. (b) I don’t think I would do it properly now. I know there’s trainers there, et cetera, et cetera, et cetera, so I’m sure they could give me the technique, but I don’t know, it’s just, it doesn’t really appeal to me lifting weights.(M6, 68)
It’s alright having YouTube videos on but they were...I think everybody in the country started off with that [during the COVID-19 lockdown] and then it wears off, it gets boring. When you’re doing your own rotation, you cheat, you have poor form, you don’t do it. And, again, it doesn’t do anything for me stood in front of a television.(F1, 68)
If you’re at home, there’s always a million other things to do.(M2, 68)
Yeah, we have got weights. We don’t have a variety of them though.(F7, 70)
I don’t want to go to a gym. I’ve never been, but when you look in, you know, they’re all between 20 and 35, you know?(F3, 71)
I don’t like the atmosphere and the structure of gyms, you know, that people are sort of making lots of [grunting sound effects]. And the smell sometimes, is disgusting, I can’t bear it. I shouldn’t have said that, should I?(F4, 71)
Half the gym are sat there on their phones so you’re not actually working any muscles anyway.(F1, 68)
There’s a big cohort of us that are what you might call recently retired or young old and the provision for us who are fit and active is sadly missing where I am. So, where I am now there are no classes to go to, the nearest one is a Smile class which is seated exercise, and this is my frustration with trying to find something that’s right for me because gyms don’t put on classes for older people and the community classes that are on are always for the older old.(F1, 68)
If you go the gym, you know, you can get all sorts of courses, I understand, for people who are recovering from strokes or have had heart attacks or various kinds of serious life events.(M5, 65)
I don’t need to do chair-based exercises or the walks that are for older people, because I can still walk further than that, so they are just not relevant to me at the moment. I’m not really into the older adults stuff yet. I’m pretending I’m not old.(F7, 70)
The local Good Neighbours do an exercise class for the elderly, but this is for housebound, you know, they sit on a chair and wave their arms up and down, and I’m not there. I think there’s something about lumping old people, you know, the over 70s, and we’re hugely diverse, just as the under 70s are, you know?(F3, 71)
I would just say again this middling thing, about the invisible population because if you’re not on a doctor’s radar, on Social Services’ radar, I could have quite easily retired from work and never crossed my doorstep again because I’m not on anybody’s radar.(F1, 68)
It’s a bone of contention with me because he won’t have an induction and be told what to do. It’s one of these cases of ‘I haven’t got to my age without knowing what I’m supposed to be doing at a gym.’(F1, 68)
I’ve had my vaccinations and the booster. I think it’s a balance, isn’t it? You either do useful exercise and take a bit of a risk or you don’t do exercise and that’s got its own risk as well.(F6, 77)
3.2.1. Main Sub-Theme 2a—Misconceptions-Ageism
You know, you always know, don’t overload yourself…I never push it [heavy loads on strength training machines](M8, 67)
I’m planning my 80th birthday on the top of the mountain but I realize that if I was going to do that, I’d probably have to give up the running.(F5, 71)
I think actually I will plan to pay a little bit more attention to strength as time goes on…when I look at pictures of myself as a college student in the football team and I look at my legs, I can see there’s a lot…like I say to myself I’m the same weight as I was then, but a lot of that weight that was in muscle in my thighs in those days is somewhere else now.(M4, 69)
I think if I felt the need, I do have a slightly dicky knee, and I did get some exercises for that, but I’m not terribly good at doing them regularly. And that’s the kind of thing, you know, if I had something wrong with me, then I think I’d be much more likely to do it more, than I am now. I’m waiting for my body to tell me…because I can still walk ten miles.(F3, 71)
3.2.2. Main Sub-Theme 2a—Misconceptions-Programme
I have been doing [Pilates] intermittently for maybe the last five years but, yeah, I’m now doing at least...I’m doing one class a week and I do a basic set of 20 min or so of exercises most mornings which is very much around stretching as well as some strength stuff.(F5, 71)
That’s the same one [video], it’s a fixed one. I’m happy with that one because you’re doing core work as well as leg work, and that sort of thing.(M1, 76)
There is an instructor at the gym who does the same routine every Friday and he’s done it for the last 30 years, and I don’t go, it’s boring. Yeah, I think the guy that hasn’t changed his routine, because you know what’s coming up you pace yourself and you’re not challenged. And I think oh, this is boring.(M1, 76)
I’m kind of middle class, you know, and I’ve been very lucky, generally, with my health. And so I don’t know that I actually take very much notice [if there were any benefits to be had from strength training participation].(F3, 71)
3.3. Major Theme 3—Motivators to Strength Training Participation
3.3.1. Main Sub-Theme 3a—Benefits of Strength and Strength Training Participation
I mean the one thing that I miss currently…I’ve been doing Pilates as well for quite a few years and I like a fairly challenging Pilates class. This lower back problem that I’ve got, Pilates helps with the core. And there are no Pilates classes at the gym at the moment. And I would dearly love to… And quite a number of other people would as well.(M1, 76)
I can probably make the hip muscle stronger to delay any operation on that hip. Same with my knees, you know, because they’re both arthritic, just keep the muscles there as strong as possible. I think if I can strengthen muscles around that it’s either going to relieve the pain or elongate the time until I might need some surgery intervention.(M8, 67)
I guess at my age with potential for bone loss, that might be an issue where I’m not meeting guidelines, but since I haven’t looked at them, I couldn’t really tell you.(M2, 68)
3.3.2. Minor Sub-Themes in the Major Theme 3—Motivators to Strength Training Participation
I can’t see any barriers. And I mean the one thing is that although I’ve been using the same gym for so many years, when we moved house 15, 16 years ago it happened that we moved nearer to the gym. And no excuse for not going to the gym, it’s 100 yards away.(M1, 76)
I’ve always been into sport and into team sport. And I wasn’t very good at it. It wasn’t because I could shine at it. It was certainly more for the team thing, the camaraderie and that kept me going. And I think kept a lot of my contemporaries going as well. I would say it’s absolutely essential.(M1, 76)
I couldn’t say I was ever active as a child…I probably do more now that I’m retired…(F2, 69)
I’m not self-motivated enough to keep doing it myself. And I’ve always said if I go to a gym I need to go to a class because I can’t walk out of a class.(F1, 68)
I really can see the benefit of a class, that you don’t want to let people down, so you do turn up and it’s not so easy to find excuses for not doing it.(F5, 71)
3.4. Major Theme 4—Solutions to Increasing Strength Training Participation
3.4.1. Main Sub-Theme 4a—Social Interactions
I can see for people in general looking at the patterns of gym attendance, having a café and getting to know some people, I think there is a social side to exercise and that would come into it…(M4, 69)
3.4.2. Minor Sub-Themes in Major Theme 4—Solutions to increasing Strength Training Participation
So, all those pool-based exercises and the Pilates, are based around that. So, it’s about strengthening, to try and maintain my standing strength, my balance. And also, and I think I’m not doing as much as I should be doing on my cardiovascular fitness. And I think that’s probably the only deficit one that I have.(M3, 71)
You know, so, (a) if I could live to be 110 sort of thing, that would do. If me doing whatever I’m doing as long as I can helps with all that other stuff that helps me keep me alive and fit and healthy, then I’ll keep doing it.(M6, 68)
I just tried this week and you’ve got to book online and, you know, I’m reasonably tech savvy but it just was unbelievably complicated to do.(F6, 77)
4. Discussion
4.1. Suggestions for Improvements to the United Kingdom’s Chief Medical Officers’ Physical Activity Guidelines
4.2. Motivators and Barriers to Strength Training Participation
4.3. Suggestions for Strength Training Programmes in the Future
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Public Health England. Wider Impacts of COVID-19 on Physical Activity, Deconditioning and Falls in Older Adults. 2021. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1010501/HEMT_Wider_Impacts_Falls.pdf (accessed on 1 March 2022).
- Office for Health Improvement and Disparities (OHID). Physical Activity: Applying All Our Health. 2022. Available online: https://www.gov.uk/government/publications/physical-activity-applying-all-our-health/physical-activity-applying-all-our-health (accessed on 1 March 2022).
- Office National Statistics. Old Age Structure Variant—UK Population in Age Groups. 2018. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/populationandmigration/populationprojections/datasets/tablel21oldagestructurevariantukpopulationinagegroups (accessed on 1 March 2022).
- The World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour. 2020. Available online: https://www.who.int/teams/health-promotion/physical-activity/developing-guidelines-on-physical-activity-and-sedentary-behaviour (accessed on 1 March 2022).
- Kraschnewski, J.L.; Sciamanna, C.N.; Ciccolo, J.T.; Rovniak, L.S.; Lehman, E.B.; Candotti, C.; Ballentine, N.H. Is exercise used as medicine? Association of meeting strength training guidelines and functional limitations among older US adults. Prev. Med. 2014, 66, 1–5. [Google Scholar] [CrossRef]
- Metter, E.; Talbot, L.; Schrager, M.; Conwit, R. Skeletal Muscle Strength as a Predictor of All-Cause Mortality in Healthy Men. J. Gerontol. A Biol. Sci. 2002, 57A, B359–B365. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, J.R.; Sui, X.; Lobelo, F.; Morrow, J.R., Jr.; Jackson, A.W.; Sjostrom, M.; Blair, S.N. Association between muscular strength and mortality in men: Prospective cohort study. BMJ 2008, 337, a439. [Google Scholar] [CrossRef] [PubMed]
- Shailendra, P.; Baldock, K.L.; Li, L.S.K.; Bennie, J.A.; Boyle, T. Resistance Training and Mortality Risk: A Systematic Review and Meta-Analysis. Am. J. Prev. Med. 2022, 63, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Momma, H.; Kawakami, R.; Honda, T.; Sawada, S.S. Muscle-strengthening activities are associated with lower risk and mortality in major non-communicable diseases: A systematic review and meta-analysis of cohort studies. Br. J. Sports Med. 2022, 56, 755–763. [Google Scholar] [CrossRef]
- Ratamess, N.; Alvar, B.; Evetoch, T.; Housh, T.; Kibler, B.; Kraemer, W.; Triplett, N. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med. Sci. Sports Exerc. 2009, 41, 687–708. [Google Scholar] [CrossRef]
- Fragala, M.; Cadore, E.; Dorgo, S.; Izquierdo, M.; Kraemer, W.; Peterson, M.; Ryan, E. Resistance Training for Older Adults: Position Statement From the National Strength and Conditioning Association. J. Strength Cond. Res. 2019, 33, 2019–2052. [Google Scholar] [CrossRef]
- Gluchowski, A.; Dulson, D.; Merien, F.; Plank, L.; Harris, N. Comparing the effects of two distinct eccentric modalities to traditional resistance training in resistance trained, higher functioning older adults. Exp. Gerontol. 2017, 98, 224–229. [Google Scholar] [CrossRef]
- Chief Medical Officer’s Physical Activity Guidelines. 2019. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/832868/uk-chief-medical-officers-physical-activity-guidelines.pdf (accessed on 1 March 2022).
- Public Health England. Muscle and Bone Strengthening and Balance Activities for General Health Benefits in Adults and Older Adults. 2018. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/721874/MBSBA_evidence_review.pdf (accessed on 1 March 2022).
- Humphries, B.; Stanton, R.; Scanlan, A.; Duncan, M.J. The prevalence and performance of resistance exercise training activities in an Australian population in relation to health authority guidelines. J. Sci. Med. Sport 2018, 21, 616–620. [Google Scholar] [CrossRef]
- Bennie, J.A.; Pedisic, Z.; van Uffelen, J.G.Z.; Gale, J.; Banting, L.K.; Vergeer, I.; Stamatakis, E.; Bauman, A.E.; Biddle, S.J.H. The descriptive epidemiology of total physical activity, muscle-strengthening exercises and sedentary behaviour among Australian adults—Results from the National Nutrition and Physical Activity Survey. BMC Public Health 2016, 16, 73. [Google Scholar] [CrossRef]
- Chevan, J. Demographic determinants of participation in strength training activities among U.S. adults. J. Strength Cond. Res. 2008, 22, 553–558. [Google Scholar] [CrossRef]
- Ma, J.K.; Leese, J.; Therrien, S.; Hoens, A.M.; Tsui, K.; Li, L.C. A scoping review of interventions to improve strength training participation. PLoS ONE 2022, 17, e0263218. [Google Scholar] [CrossRef]
- Milton, K.; Varela, A.R.; Strain, T.; Cavill, N.; Foster, C.; Mutrie, N. A review of global surveillance on the muscle strengthening and balance elements of physical activity recommendations. J. Frailty Sarcopenia Falls 2018, 3, 114–124. [Google Scholar] [CrossRef]
- Loustalot, F.; Carlson, S.A.; Kruger, J.; Buchner, D.M.; Fulton, J.E. Muscle-Strengthening Activities and Participation Among Adults in the United States. Res. Q. Exerc. Sport 2013, 84, 30–38. [Google Scholar] [CrossRef]
- Colorafi, K.J.; Evans, B. Qualitative Descriptive Methods in Health Science Research. Health Environ. Res. Des. J. 2016, 9, 16–25. [Google Scholar] [CrossRef]
- Thomas, D.R. A General Inductive Approach for Analyzing Qualitative Evaluation Data. Am. J. Eval. 2016, 27, 237–246. [Google Scholar] [CrossRef]
- Chartered Society of Physiotherapists. Strength Messaging Insight. 2020. Available online: https://www.csp.org.uk/publications/strength-messaging-insight-report (accessed on 1 March 2022).
- Bernard, P.L.; Tallon, G.; Ninot, G.; Jaussent, A.; Ramdani, S.; Coste, O.; Picot, M.C.; Blain, H. Influence of a brisk walking program on isokinetic muscular capacities of knee in sedentary older women. Aging Clin. Exp. Res. 2016, 28, 1219–1226. [Google Scholar] [CrossRef]
- Virág, A.; Karóczi, C.K.; Jakab, Á.; Vass, Z.; Kovács, É.; Gondos, T. Short-term and long-term effects of nordic walking training on balance, functional mobility, muscle strength and aerobic endurance among Hungarian community-living older people: A feasibility study. J. Sports Med. Phys. Fitness 2015, 55, 1285–1292. [Google Scholar]
- Foster, C.; Armstrong, M.E.G. What types of physical activities are effective in developing muscle and bone strength and balance? J. Frailty Sarcopenia Falls 2018, 3, 58–65. [Google Scholar] [CrossRef]
- Steele, J.; Fisher, J.; Skivington, M.; Dunn, C.; Arnold, J.; Tew, G.; Batterham, A.M.; Nunan, D.; O’Driscoll, J.M.; Mann, S.; et al. A higher effort-based paradigm in physical activity and exercise for public health: Making the case for a greater emphasis on resistance training. BMC Public Health 2017, 17, 300. [Google Scholar] [CrossRef]
- Centre for Ageing Better. Raising the Bar on Strength and Balance: The Importance of Community-Based Provision. 2019. Available online: https://ageing-better.org.uk/sites/default/files/2021-03/Raising-the-bar-on-strength-and-balance-full-report.pdf (accessed on 1 March 2022).
- Bucht, H.; Donath, L. Sauna Yoga Superiorly Improves Flexibility, Strength, and Balance: A Two-Armed Randomized Controlled Trial in Healthy Older Adults. Int. J. Environ. Res. 2019, 16, 3721. [Google Scholar] [CrossRef] [PubMed]
- Cancela, J.M.; de Oliveira, I.M.; Rodríguez-Fuentes, G. Effects of Pilates method in physical fitness on older adults. A systematic review. Eur. Rev. Aging Phys. Act. 2014, 11, 81–94. [Google Scholar] [CrossRef]
- Roland, K.P.; Jakobi, J.M.; Jones, G.R. Does Yoga Engender Fitness in Older Adults? A Critical Review. J. Aging Phys. Act. 2011, 19, 62–79. [Google Scholar] [CrossRef] [PubMed]
- Bates, A.; Furber, S.; Sherrington, C.; van den Dolder, P.; Ginn, K.; Bauman, A.; Ginn, K.; Bauman, A.; Howard, K.; Kershaw, M.; et al. Effectiveness of workshops to teach a home-based exercise program (BEST at Home) for preventing falls in community-dwelling people aged 65 years and over: A pragmatic randomised controlled trial. BMC Geriatr. 2022, 22, 366. [Google Scholar] [CrossRef]
- Kasper, K. Sports Training Principles. Curr. Sports Med. Rep. 2019, 18, 95–96. [Google Scholar] [CrossRef]
- Izquierdo, M.; Duque, G.; Morley, J.E. Physical activity guidelines for older people: Knowledge gaps and future directions. Lancet Healthy Longev. 2021, 2, 380–383. [Google Scholar] [CrossRef]
- Gluchowski, A.; Warbrick, I.; Oldham, T.; Harris, N. I have a renewed enthusiasm for going to the gym: What keeps resistance-trained older adults coming back to the gym? Qual. Res. Sport Exerc. 2018, 10, 333–345. [Google Scholar] [CrossRef]
- Love, R.; Adams, J.; van Sluijs, E.M.F.; Foster, C.; Humphreys, D. A cumulative meta-analysis of the effects of individual physical activity interventions targeting healthy adults. Obes. Rev. 2018, 19, 1164–1172. [Google Scholar] [CrossRef]
- Williamson, C.; Baker, G.; Tomasone, J.R.; Bauman, A.; Mutrie, N.; Niven, A.; Richards, J.; Oyeyemi, A.; Baxter, B.; Rigby, B.; et al. The Physical Activity Messaging Framework (PAMF) and Checklist (PAMC): International consensus statement and user guide. Int. J. Behav. Nutr. Phys. Act. 2021, 18, 164. [Google Scholar] [CrossRef]
- Vasudevan, A.; Ford, E. Motivational Factors and Barriers Towards Initiating and Maintaining Strength Training in Women: A Systematic Review and Meta-synthesis. Prev. Sci. 2021, 23, 674–695. [Google Scholar] [CrossRef]
- Darr, A.; Astin, F.; Atkin, K. Causal attributions, lifestyle change, and coronary heart disease: Illness beliefs of patients of South Asian and European origin living in the United Kingdom. Heart Lung 2008, 37, 91–104. [Google Scholar] [CrossRef]
- Haskell, W.L.; Lee, I.M.; Pate, R.R.; Powell, K.E.; Blair, S.N.; Franklin, B.A.; Macera, C.A.; Heath, G.W.; Thompson, P.D.; Bauman, A. Physical activity and public health: Updated recommendation for adults from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1423–1434. [Google Scholar] [CrossRef]
- Ige-Elegbede, J.; Pilkington, P.; Gray, S.; Powell, J. Barriers and facilitators of physical activity among adults and older adults from Black and Minority Ethnic groups in the UK: A systematic review of qualitative studies. Prev. Med. Rep. 2019, 15, 100952. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Martin, A.D.; Taunton, J.E.; Rhodes, E.C.; Donnelly, M.; Elliot, J. Factors associated with exercise adherence among older adults. An individual perspective. Sports Med. 1999, 28, 397–411. [Google Scholar] [CrossRef]
- Smith, B.; Williams, O.; Bone, L.; the Moving Social Work Co-production Collective. Co-production: A resource to guide co-producing research in the sport, exercise, and health sciences. In Qualitative Research in Sport, Exercise and Health; Taylor and Francis Ltd.: Oxfordshire, UK, 2022; pp. 1–29. [Google Scholar] [CrossRef]
- Polster, M.; Dooley, E.E.; Olscamp, K.; Piercy, K.L.; Oh, A. Responses to the Physical Activity Guidelines and Dissemination Strategies for Behavior Change in a Representative Sample of US Adults. J. Phys. Act. Health 2021, 18, 1342–1351. [Google Scholar] [CrossRef]
- Budzynski-Seymour, E.; Milton, K.; Mills, H.; Wade, M.; Foster, C.; Vishnubala, D.; Baxter, B.; Williamson, C.; Steele, J. A Rapid Review of Communication Strategies for Physical Activity Guidelines and Physical Activity Promotion: A Review of Worldwide Strategies. SportRxiv Preprint 2020, 18, 1014–1027. [Google Scholar] [CrossRef]
- Czosnek, L.; Rankin, N.; Zopf, E.; Richards, J.; Rosenbaum, S.; Cormie, P. Implementing Exercise in Healthcare Settings: The Potential of Implementation Science. Sports Med. 2020, 50, 1–14. [Google Scholar] [CrossRef]
- Tankard, M.; Paluck, E. Norm Perception as a Vehicle for Social Change. Soc. Issues Policy Rev. 2016, 10, 181–211. [Google Scholar] [CrossRef]
- Wade, M.; Brown, N.; Steele, J.; Mann, S.; Dancy, B.; Winter, S.; Majumdar, A. The impact of participant pathways on the effectiveness of a community-based physical activity intervention grounded in motivational interviewing. SportRxiv Preprint 2020. [Google Scholar] [CrossRef]
- Liddle, J.; Lovarini, M.; Clemson, L.; Mackenzie, L.; Tan, A.; Pit, S.W.; Poulos, R.; Tiedemann, A.; Sherrington, C.; Roberts, C.; et al. Making fall prevention routine in primary care practice: Perspectives of allied health professionals. BMC Health Serv. Res. 2018, 18, 598. [Google Scholar] [CrossRef]
- Burton, E.; Farrier, K.; Lewin, G.; Pettigrew, S.; Hill, A.-M.; Airey, P.; Bainbridge, L.; Hill, K. Motivators and Barriers for Older People Participating in Resistance Training: A Systematic Review. J. Aging Phys. Act. 2017, 25, 311–324. [Google Scholar] [CrossRef]
- de Lacy-Vawdon, C.J.; Klein, R.; Schwarzman, J.; Nolan, G.; de Silva, R.; Menzies, D.; Smith, B.J. Facilitators of Attendance and Adherence to Group-Based Physical Activity for Older Adults: A Literature Synthesis. J. Aging Phys. Act. 2018, 26, 155–167. [Google Scholar] [CrossRef]
- Collado-Mateo, D.; Lavin-Perez, A.M.; Penacoba, C.; Del Coso, J.; Leyton-Roman, M.; Luque-Casado, A.; Gasque, P.; Fernández-Del-Olmo, M.; Amado-Alonso, D. Key Factors Associated with Adherence to Physical Exercise in Patients with Chronic Diseases and Older Adults: An Umbrella Review. Int. J. Environ. Res. Public Health 2021, 18, 2023. [Google Scholar] [CrossRef]
- Hartley, S.E.; Yeowell, G. Older adults’ perceptions of adherence to community physical activity groups. Ageing Soc. 2014, 35, 1635–1656. [Google Scholar] [CrossRef]
- Beauchamp, M.R.; Ruissen, G.R.; Dunlop, W.L.; Estabrooks, P.A.; Harden, S.M.; Wolf, S.A.; Liu, Y.; Schmader, T.; Puterman, E.; Sheel, A.W.; et al. Group-based physical activity for older adults (GOAL) randomized controlled trial: Exercise adherence outcomes. Health Psychol. 2018, 37, 451–461. [Google Scholar] [CrossRef]
- Foyster, J.M.; Rebar, A.; Guy, J.H.; Stanton, R. If they can do it, I can do it: Experiences of older women who engage in powerlifting training. J. Women Aging 2020, 34, 54–64. [Google Scholar] [CrossRef]
- Gentil, P.; Steele, J.; Fisher, J. Why intensity is not a bad word—Benefits and practical aspects of high effort resistance training to the older. Clin. Nutr. 2017, 36, 1454–1455. [Google Scholar] [CrossRef]
- Boulton, E.; Weber, M.; Hawley-Hague, H.; Bergquist, R.; Van Ancum, J.; Jonkman, N.H.; Taraldsen, K.; Helbostad, J.L.; Maier, A.B.; Becker, C.; et al. Attitudes Towards Adapted Lifestyle-Integrated Functional Exercise Developed for 60-70-Year-Olds: Perceptions of Participants and Trainers. Gerontology 2019, 65, 599–609. [Google Scholar] [CrossRef]
- Steele, J.; Malleron, T.; Har-Nir, I.; Androulakis-Korakakis, P.; Wolf, M.; Fisher, J.; Halperin, I. Are we lifting heavy enough? Self-selected loads in resistance exercise: A scoping review and exploratory meta-analysis. Sports Med. 2022. [Google Scholar] [CrossRef]
- Bennett, E.V.; Hurd Clarke, L.; Wolf, S.A.; Dunlop, W.L.; Harden, S.M.; Liu, Y.; Estabrooks, P.; Rhodes, R.; Bealuchamp, M. Older adults’ experiences of group-based physical activity: A qualitative study from the ‘GOAL’ randomized controlled trial. Psychol. Sport Exerc. 2018, 39, 184–192. [Google Scholar] [CrossRef]
- O’Bryan, S.J.; Giuliano, C.; Woessner, M.N.; Vogrin, S.; Smith, C.; Duque, G.; Levinger, I. Progressive Resistance Training for Concomitant Increases in Muscle Strength and Bone Mineral Density in Older Adults: A Systematic Review and Meta-Analysis. Sports Med. 2022, 52, 1939–1960. [Google Scholar] [CrossRef] [PubMed]
- Lo, O.Y.; Kahya, M.; Manor, B. Powering Through Daily Activities in Older Age-Will Power Training Replace Strength Training in Later Life? JAMA Netw. Open 2022, 5, e2211631. [Google Scholar] [CrossRef] [PubMed]
- Balachandran, A.T.; Steele, J.; Angielczyk, D.; Belio, M.; Schoenfeld, B.J.; Quiles, N.; Askin, N.; Abou-Setta, A.M. Comparison of Power Training vs Traditional Strength Training on Physical Function in Older Adults: A Systematic Review and Meta-analysis. JAMA Netw. Open 2022, 5, e2211623. [Google Scholar] [CrossRef] [PubMed]
- Meigh, N.J.; Davidson, A.R.; Keogh, J.W.L.; Hing, W. Older adults’ experiences of supervised hardstyle kettlebell training: A qualitative study from the BELL pragmatic controlled trial. medRxiv 2021. [Google Scholar] [CrossRef]
- Cavill, N.A.; Foster, C.E.M. Enablers and barriers to older people’s participation in strength and balance activities: A review of reviews. J. Frailty Sarcopenia Falls 2018, 3, 105–113. [Google Scholar] [CrossRef]
- Rhodes, R.E.; Lithopoulos, A. Understanding action control of resistance training among adults. Psychol. Sport Exerc. 2022, 59, 102108. [Google Scholar] [CrossRef]
- Bauman, A.E.; Reis, R.S.; Sallis, J.F.; Wells, J.C.; Loos, R.J.F.; Martin, B.W. Correlates of physical activity: Why are some people physically active and others not? Lancet 2012, 380, 258–271. [Google Scholar] [CrossRef]
- Hawley-Hague, H.; Horne, M.; Skelton, D.A.; Todd, C. Older Adults’ Uptake and Adherence to Exercise Classes: Instructors’ Perspectives. J. Aging Phys. Act. 2016, 24, 119–128. [Google Scholar] [CrossRef]
- Ajzen, I. Attitudes, Personality and Behavior; Open University Press: Maidenhead, UK, 1988. [Google Scholar]
- Budzynski-Seymour, E.; Jones, M.; Steele, J. ‘A Physically Active Experience’: Setting the Stage for a New Approach to Engage Children in Physical Activity Using Themed Entertainment Experiences. Sports Med. 2022. [Google Scholar] [CrossRef]
- Fetherman, D.L.; Hakim, R.M.; Sanko, J.P. A Pilot Study of the Application of the Transtheoretical Model During Strength Training in Older Women. J. Women Aging 2011, 23, 58–76. [Google Scholar] [CrossRef]
- Franco, M.R.; Tong, A.; Howard, K.; Sherrington, C.; Ferreira, P.H.; Pinto, R.Z.; Ferreira, M.L. Older people’s perspectives on participation in physical activity: A systematic review and thematic synthesis of qualitative literature. Br. J. Sports Med. 2015, 49, 1268–1276. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
|
|
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gluchowski, A.; Bilsborough, H.; Mcdermott, J.; Hawley-Hague, H.; Todd, C. ‘A Lot of People Just Go for Walks, and Don’t Do Anything Else’: Older Adults in the UK Are Not Aware of the Strength Component Embedded in the Chief Medical Officers’ Physical Activity Guidelines—A Qualitative Study. Int. J. Environ. Res. Public Health 2022, 19, 10002. https://doi.org/10.3390/ijerph191610002
Gluchowski A, Bilsborough H, Mcdermott J, Hawley-Hague H, Todd C. ‘A Lot of People Just Go for Walks, and Don’t Do Anything Else’: Older Adults in the UK Are Not Aware of the Strength Component Embedded in the Chief Medical Officers’ Physical Activity Guidelines—A Qualitative Study. International Journal of Environmental Research and Public Health. 2022; 19(16):10002. https://doi.org/10.3390/ijerph191610002
Chicago/Turabian StyleGluchowski, Ashley, Helena Bilsborough, Jane Mcdermott, Helen Hawley-Hague, and Chris Todd. 2022. "‘A Lot of People Just Go for Walks, and Don’t Do Anything Else’: Older Adults in the UK Are Not Aware of the Strength Component Embedded in the Chief Medical Officers’ Physical Activity Guidelines—A Qualitative Study" International Journal of Environmental Research and Public Health 19, no. 16: 10002. https://doi.org/10.3390/ijerph191610002