
Comparison of Wuqinxi Qigong with Stretching on Single- and Dual-Task Gait, Motor Symptoms and Quality of Life in Parkinson’s Disease: A Preliminary Randomized Control Study

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Sample Size Calculation and Randomization
2.3. Interventions
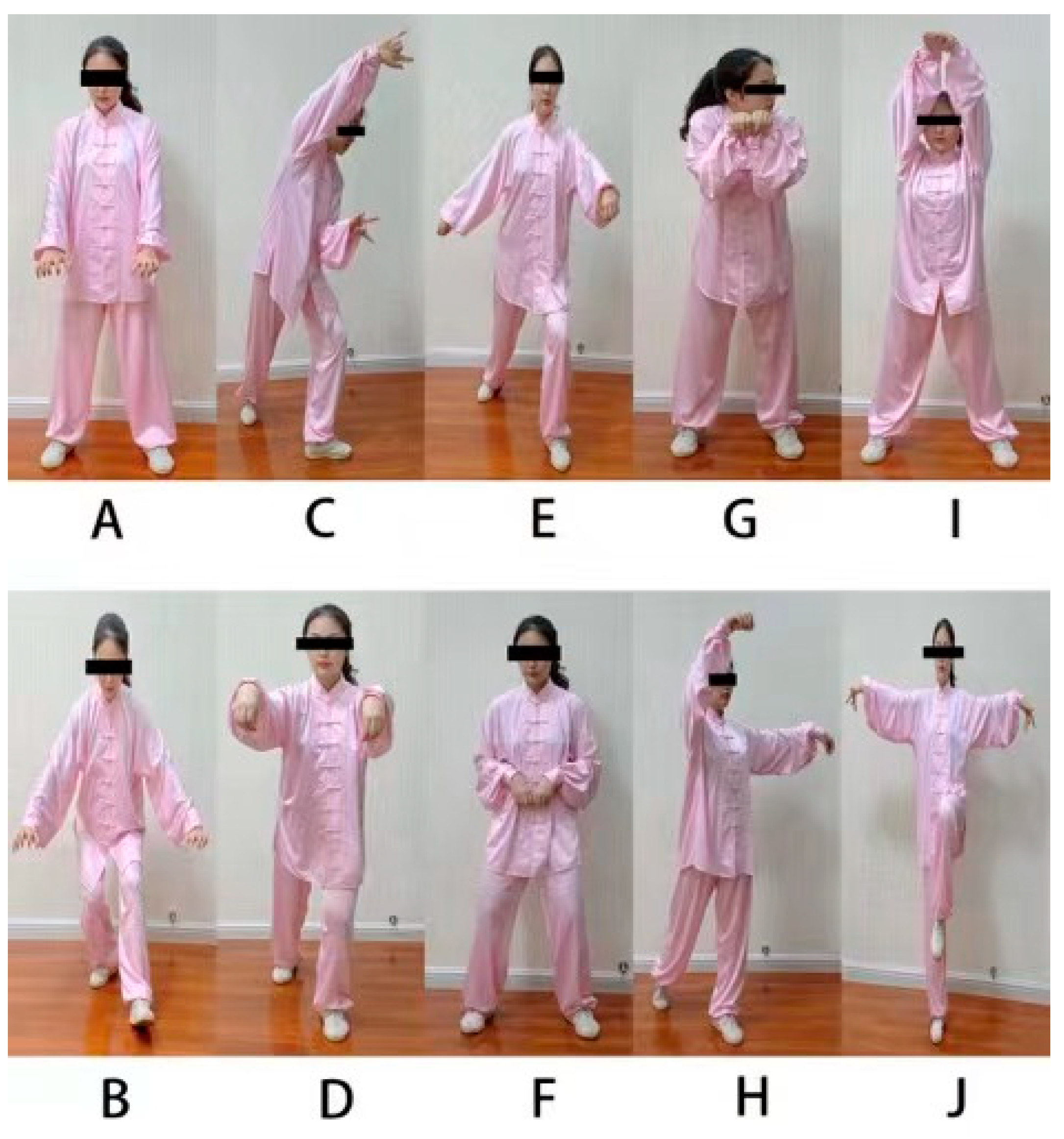
2.3.1. Wuqinxi Qigong Exercise
2.3.2. Stretching Exercise
2.4. Outcome Assessments
2.5. Statistical Analysis
3. Results
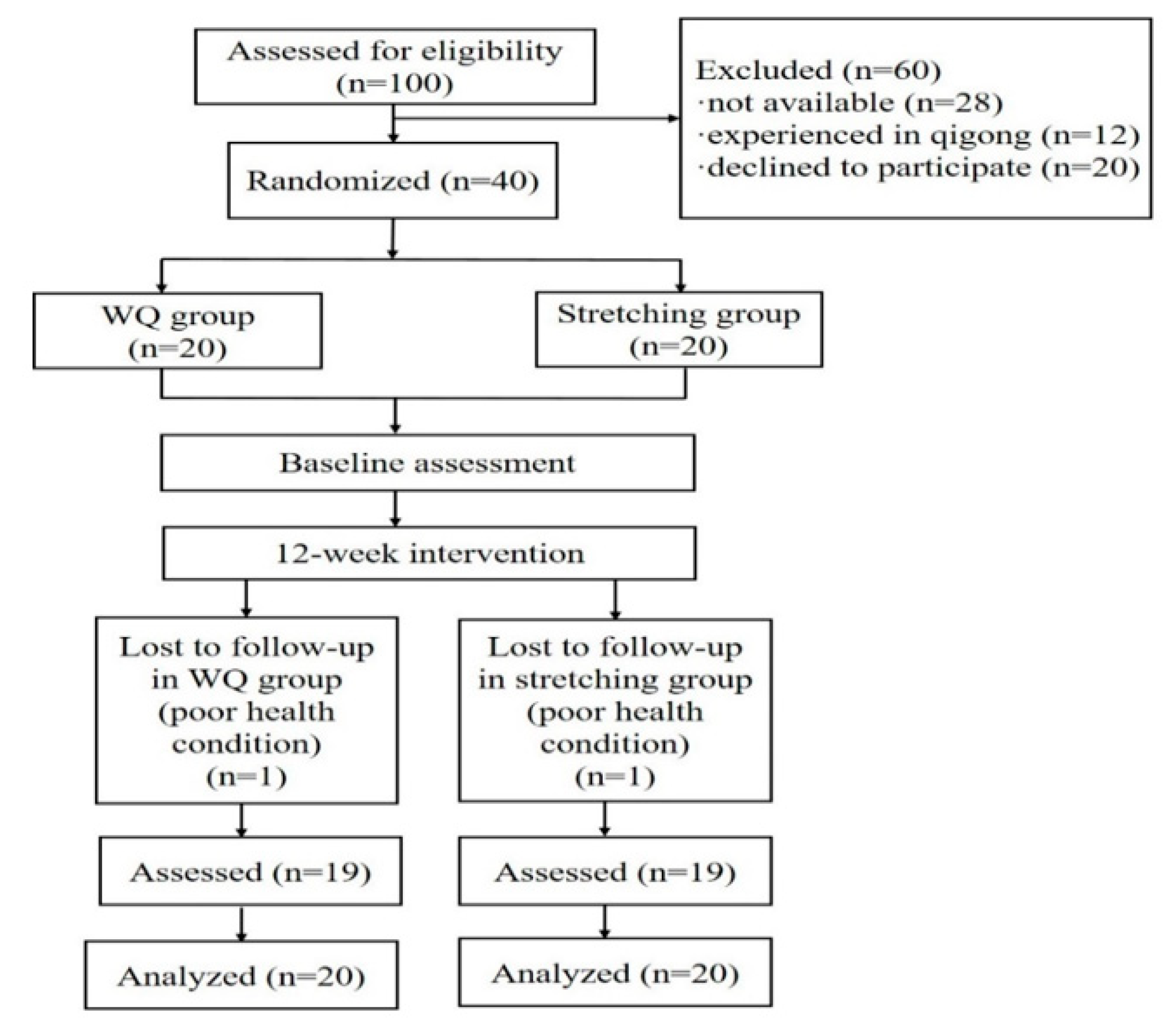
3.1. Participants and Baseline Characteristics
3.2. Intervention Effects in Primary and Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Myers, P.S.; McNeely, M.E.; Pickett, K.A.; Duncan, R.P.; Earhart, G.M. Effects of exercise on gait and motor imagery in people with Parkinson disease and freezing of gait. Parkinsonism Relat. Disord. 2018, 53, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Pelicioni, P.H.S.; Tijsma, M.; Lord, S.R.; Menant, J. Prefrontal cortical activation measured by fNIRS during walking: Effects of age, disease and secondary task. Peer. J. 2019, 7, e6833. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, A.Z.D.; Israel, V.L. Effects of dual-task aquatic exercises on functional mobility, balance and gait of individuals with Parkinson’s disease: A randomized clinical trial with a 3-month follow-up. Complementary Ther. Med. 2019, 42, 119–124. [Google Scholar] [CrossRef] [PubMed]
- Raffegeau, T.E.; Krehbiel, L.M.; Kang, N.; Thijs, F.J.; Altmann, L.J.P.; Cauraugh, J.H.; Hass, C.J. A meta-analysis Parkinson’s disease and dual-task walking. Parkinsonism Relat. Disord. 2019, 62, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Kelly, V.E.; Eusterbrock, A.J.; Shumway-Cook, A. A Review of Dual-Task Walking Deficits in People with Parkinson’s Disease: Motor and Cognitive Contributions, Mechanisms, and Clinical Implications. Parkinson’s Dis. 2012, 2012, 918719. [Google Scholar] [CrossRef] [Green Version]
- Kleiner, A.F.R.; Pagnussat, A.S.; Prisco, G.D.; Vagnini, A.; Stocchi, F.; De Pandis, M.F.; Galli, M. Analyzing gait variability and dual task interference in patients with Parkinson’s disease and freezing by means of the wordcolor Stroop test. Aging Clin. Exp. Res. 2018, 30, 1137–1142. [Google Scholar] [CrossRef]
- Wild, L.B.; de Lima, D.B.; Balardin, J.B.; Rizzi, L.; Giacobbo, B.L.; Oliveira, H.B.; de Lima Argimon, I.I.; Peyré-Tartaruga, L.A.; Rieder, C.R.; Bromberg, E. Characterization of cognitive and motor performance during dual-tasking in healthy older adults and patients with Parkinson’s disease. J. Neurol. 2013, 260, 580–589. [Google Scholar] [CrossRef]
- Isaacson, S.; O’Brien, A.; Lazaro, J.D.; Ray, A.; Fluet, G. The JFK BIG study: The impact of LSVT BIG® on dual task walking and mobility in persons with Parkinson’s disease. J. Phys. Ther. Sci. 2018, 30, 636–641. [Google Scholar] [CrossRef] [Green Version]
- Dockx, K.; Bekkers, E.M.; Van den Bergh, V.; Ginis, P.; Rochester, L.; Hausdorff, J.M.; Mirelman, A.; Nieuwboer, A. Virtual reality for rehabilitation in Parkinson’s disease. Cochrane Database Syst. Rev. 2016, 12, CD010760. [Google Scholar] [CrossRef]
- Fritz, N.E.; Cheek, F.M.; Nichols-Larsen, D.S. Motor cognitive dual-task training in persons with neurologic disorders: A systematic review. J. Neurol. Phys. Ther. 2015, 39, 142–153. [Google Scholar] [CrossRef] [Green Version]
- Geroin, C.; Nonnekes, J.; de Vries, N.M.; Strouwen, C.; Smania, N.; Tinazzi, M.; Nieuwboer, A.; Bloem, B.R. Does dual-task training improve spatiotemporal gait parameters in Parkinson’s disease? Parkinsonism Relat. Disord. 2018, 55, 86–91. [Google Scholar] [CrossRef] [PubMed]
- Maidan, I.; Nieuwhof, F.; Bernad-Elazari, H.; Bloem, B.R.; Giladi, N.; Hausdorff, J.M.; Claassen, J.A.H.R.; Mirelman, A. Evidence for Differential Effects of 2 Forms of Exercise on Prefrontal Plasticity During Walking in Parkinson’s Disease. Neurorehabilit. Neural Repair 2018, 2, 200–208. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Qiu, W.Q.; Hao, Y.L.; Lv, Z.Y.; Jiao, S.J.; Teng, J.F. The efficacy of traditional Chinese Medical Exercise for Parkinson’s disease: A systematic review and meta-analysis. PLoS ONE 2015, 10, e0122469. [Google Scholar] [CrossRef] [PubMed]
- Song, R.; Grabowska, W.; Park, M.; Osypiuk, K.; Vergara-Diaz, G.P.; Bonato, P.; Hausdorff, J.M.; Fox, M.; Sudarsky, L.R.; Macklin, E.; et al. The impact of Tai Chi and Qigong mind-body exercises on motor and non-motor function and quality of life in Parkinson’s disease: A systematic review and meta-analysis. Parkinsonism Relat. Disord. 2017, 41, 3–13. [Google Scholar] [CrossRef]
- Ge, L.; Zheng, Q.X.; Liao, Y.T.; Tan, J.Y.; Xie, Q.L.; Rask, M. Effects of traditional Chinese exercises on the rehabilitation of limb function among stroke patients: A systematic review and meta-analysis. Complementary Ther. Clin. Pract. 2017, 29, 35–47. [Google Scholar] [CrossRef]
- Zhang, Y.; Zhou, J. Analysis of the TCM theory of traditional Chinese health exercise. J. Sport Health Sci. 2013, 2, 204–208. [Google Scholar]
- Guo, Y.; Xu, M.; Wei, Z.; Hu, Q.; Chen, Y.; Yan, J.; Wei, Y. Beneficial Effects of Qigong Wuqinxi in the Improvement of Health Condition, Prevention, and Treatment of Chronic Diseases: Evidence from a Systematic Review. Evid. Based Complement Altern. Med. 2018, 2018, 3235950. [Google Scholar] [CrossRef] [Green Version]
- Wang, K.; Liu, S.; Kong, Z.; Zhang, Y.; Liu, J. Mind-Body Exercise (Wuqinxi) for Patients with Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Int. J. Environ. Res. Public Health 2018, 16, 72. [Google Scholar] [CrossRef] [Green Version]
- Zhang, F.B.Y.; Zhang, J. The Influence of “wuqinxi” exercises on the Lumbosacral Multifidus. J. Phys. Ther. Sci. 2014, 26, 881–884. [Google Scholar] [CrossRef] [Green Version]
- Yao, C.; Li, Z.; Zhang, S.; Wu, Z.; Zhu, Q.; Fang, L. Effects of Wuqinxi in the Patients with Chronic Low Back Pain: A Randomized Controlled Trial. Evid. Based Complement Alternat. Med. 2020, 2020, 1428246. [Google Scholar] [CrossRef]
- Xiao, C.M.; Li, J.J.; Kang, Y.; Zhuang, Y.C. Follow-up of a Wuqinxi exercise at home programme to reduce pain and improve function for knee osteoarthritis in older people: A randomised controlled trial. Age Ageing 2021, 50, 570–575. [Google Scholar] [CrossRef] [PubMed]
- Tolos, E.; Wenning, G.; Poewe, W. The diagnosis of Parkinson’s disease. Neurol. Sci. 2006, 5, 75–86. [Google Scholar] [CrossRef]
- Liu, Y.C.; Yang, Y.R.; Tsai, Y.A.; Wang, R.Y. Cognitive and motor dual task gait training improve dual task gait performance after stroke—A randomized controlled pilot trial. Sci. Rep. 2017, 7, 4070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borg, G. Borg’s Perceived Exertion and Pain Scales; Human Kinetics: Champaign, IL, USA, 1998; p. 104. [Google Scholar]
- Chinese Health Qigong Association. Theoretical Training Course in Health Qigong, 1st ed.; Foreign Languages Press Co., Ltd.: Beijing, China, 2015; pp. 202–203. [Google Scholar]
- Anderson, B. Stretching: 40th Anniversary Edition; Shelter Publication Inc.: Bolinas, CA, USA, 2020; pp. 108–113. [Google Scholar]
- Fernandes, Â.; Sousa, A.S.; Rocha, N.; Tavares, J.M. Parkinson’s Disease and Cognitive-Motor Dual-Task: Is Motor Prioritization Possible in the Early Stages of the Disease? J. Mot. Behav. 2016, 48, 377–383. [Google Scholar] [CrossRef] [Green Version]
- Liepelt-Scarfone, I.; Lerche, S.; Behnke, S.; Godau, J.; Gaenslen, A.; Pausch, C.; Fassbender, K.; Brockmann, K.; Srulijes, K.; Huber, H.; et al. Clinical characteristics related to worsening of motor function assessed by the Unified Parkinson’s Disease Rating Scale in the elderly population. J. Neurol. 2015, 262, 451–458. [Google Scholar] [CrossRef]
- Benka Wallén, M.; Sorjonen, K.; Löfgren, N.; Franzén, E. Structural Validity of the Mini-Balance Evaluation Systems Test (Mini-BESTest) in People with Mild to Moderate Parkinson Disease. Phys. Ther. 2016, 96, 1799–1806. [Google Scholar] [CrossRef]
- Benavent-Caballer, V.; Sendín-Magdalena, A.; Lisón, J.F.; Rosado-Calatayud, P.; Amer-Cuenca, J.J. Physical factors underlying the Timed “Up and Go” test in older adults. Geriatr. Nurs. 2016, 37, 122–127. [Google Scholar] [CrossRef]
- Li, H.; Jia, J.; Yang, Z. Mini-Mental State Examination in Elderly Chinese: A Population-Based Normative Study. J. Alzheimers Dis. 2016, 53, 487–496. [Google Scholar] [CrossRef]
- Jesus-Ribeiro, J.; Vieira, E.; Ferreira, P.; Januário, C.; Freire, A. Reliability and validity of 39-Item Parkinson’s disease questionnaire and Parkinson’s disease quality of life questionnaire. Acta Med. Port. 2017, 30, 395–401. [Google Scholar] [CrossRef] [Green Version]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences. Technometrics 1988, 31, 499–500. [Google Scholar]
- Wassom, D.J.; Lyons, K.E.; Pahwa, R.; Liu, W. Qigong exercise may improve sleep quality and gait performance in Parkinson’s disease: A pilot study. Int. J. Neurosci. 2015, 125, 578–584. [Google Scholar] [CrossRef] [PubMed]
- Perera, S.; Mody, S.H.; Woodman, R.C.; Studenski, S.A. Meaningful change and responsiveness in common physical performance measures in older adults. J. Am. Geriatr. Soc. 2006, 54, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Gao, J.; Yin, B.; Yang, X.; Bai, D. Efficacy of Ba Duan Jin in Improving Balance: A Study in Chinese Community-Dwelling Older Adults. J. Gerontol. Nurs. 2016, 42, 38–46. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sawynok, J.; Lynch, M. Qigong and fibromyalgia: Randomized controlled trials and beyond. Evid. Based Complement Alternat. Med. 2014, 2014, 379715. [Google Scholar] [CrossRef]
- Maidan, I.; Eyal, S.; Kurz, I.; Geffen, N.; Gazit, E.; Ravid, L.; Giladi, N.; Mirelman, A.; Hausdorff, J.M. Age-associated changes in obstacle negotiation strategies: Does size and timing matter? Gait Posture 2017, 59, 242–247. [Google Scholar] [CrossRef]
- Alcock, L.; Galna, B.; Hausdorff, J.M.; Lord, S.; Rochester, L. Gait & Posture Special Issue: Gait adaptations in response to obstacle type in fallers with Parkinson’s disease. Gait Posture 2018, 61, 368–374. [Google Scholar]
- Roiz Rde, M.; Cacho, E.W.; Pazinatto, M.M.; Reis, J.G.; Cliquet, A.; Barasnevicius-Quagliato, E.M. Gait analysis comparing Parkinson’s disease with healthy elderly subjects. Arq. Neuro-Psiquiatr. 2010, 68, 81–86. [Google Scholar] [CrossRef]
- Schaafsma, J.D.; Giladi, N.; Balash, Y.; Bartels, A.L.; Gurevich, T.; Hausdorff, J.M. Gait dynamics in Parkinson’s disease: Relationship to Parkinsonian features, falls and response to levodopa. J. Neurol. Sci. 2003, 212, 47–53. [Google Scholar] [CrossRef]
- Liu, X.L.; Chen, S.; Wang, Y. Effects of health Qigong exercises on relieving symptoms of Parkinson’s disease. Evid. Based Complement Alternat. Med. 2016, 2016, 5935782. [Google Scholar] [CrossRef] [Green Version]
- Klein, P.; Picard, G.; Baumgarden, J.; Schneider, R. Meditative movement, energetic, and physical analyses of three Qigong exercises: Unification of eastern and Western mechanistic exercise theory. Medicines 2017, 4, 69. [Google Scholar] [CrossRef] [Green Version]
- Rochester, L.; Galna, B.; Lord, S.; Burn, D. The nature of dual-task interference during gait in incident Parkinson’s disease. Neuroscience 2014, 265, 83–94. [Google Scholar] [CrossRef] [PubMed]
- Stegemöller, E.L.; Wilson, J.P.; Hazamy, A.; Shelley, M.C.; Okun, M.S.; Altmann, L.J.; Hass, C.J. Associations between cognitive and gait performance during single- and dual-task walking in people with Parkinson disease. Phys. Ther. 2014, 94, 757–766. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yang, Y.R.; Cheng, S.J.; Lee, Y.J.; Liu, Y.C.; Wang, R.Y. Cognitive and motor dual task gait training exerted specific training effects on dual task gait performance in individuals with Parkinson’s disease: A randomized controlled pilot study. PLoS ONE 2019, 14, e0218180. [Google Scholar] [CrossRef] [PubMed]
- Rawson, K.S.; McNeely, M.E.; Duncan, R.P.; Pickett, K.A.; Perlmutter, J.S.; Earhart, G.M. Exercise and Parkinson Disease: Comparing Tango, Treadmill, and Stretching. J. Neurol. Phys. Ther. 2019, 43, 26–32. [Google Scholar] [CrossRef]
- Mak, M.K.; Wong-Yu, I.S.; Shen, X.; Chung, C.L. Long-term effects of exercise and physical therapy in people with Parkinson disease. Nat. Rev. Neurol. 2017, 13, 689–703. [Google Scholar] [CrossRef]
- Godi, M.; Arcolin, I.; Giardini, M.; Corna, S.; Schieppati, M. Responsiveness and minimal clinically important difference of the Mini-BESTest in patients with Parkinson’s disease. Gait Posture 2020, 80, 14–19. [Google Scholar] [CrossRef]
- Horváth, K.; Aschermann, Z.; Ács, P.; Deli, G.; Janszky, J.; Komoly, S.; Balázs, É.; Takács, K.; Karádi, K.; Kovács, N. Minimal clinically important difference on the Motor Examination part of MDS-UPDRS. Parkinsonism Relat. Disord. 2015, 21, 1421–1426. [Google Scholar] [CrossRef]
- Ying, L. Health Qigong Wuqinxi, 1st ed.; Dalian Maritime University Press: Dalian, China, 2016; pp. 45–95. [Google Scholar]



{kind=link}
{kind=link}
| Demographics and Outcomes | WQ Group (n = 20) | Stretching Group (n = 20) | p |
|---|---|---|---|
| Age (year) | 67.57 ± 3.95 | 70 ± 5.59 | 0.126 |
| Gender (M/F) | 13/7 | 16/4 | 0.288 |
| Education condition (years) | 14.40 ± 1.47 | 14.55 ± 1.36 | 0.739 |
| Disease duration (years) | 6.83 ± 4.09 | 7.76 ± 4.55 | 0.528 |
| H&Y stage, n (%) | 0.631 | ||
| 1–1.5 | 10 (50%) | 7 (35%) | |
| 2–2.5 | 7 (35%) | 9 (45%) | |
| 3 | 3 (15%) | 4 (20%) | |
| Freezing of gait, n (%) | 9 (45%) | 9 (45%) | 1.000 |
| MDS-UPDRS | 25.05 ± 17.45 | 26.79 ± 20.79 | 0.598 |
| MDS-UPDRSIII | 52.19 ± 26.87 | 47.47 ± 29.25 | 0.646 |
| MMSE | 26.79 ± 2.58 | 28.43 ± 2.58 | 0.157 |
| Falls in the 6 months prior to study, n (%) | 3 (15%) | 4 (20%) | 1.000 |
| LEDD (mg/d) | 450 ± 252.98 | 450 ± 164.99 | 1.000 |
| Outcomes | Variables | WQ Group | Stretching Group | Time * Group | ||||
|---|---|---|---|---|---|---|---|---|
| Pre | Post12wk | Pre vs. Post12wk p | Pre | Post12wk | Pre vs. Post12wk p | p | ||
| Primary outcomes | ||||||||
| Single-task | Gait speed (cm/s) | 91.03 ± 9.34 | 97.42 ± 10.85 | 0.000 * | 79.85 ± 10.49 | 80.63 ± 13.12 | 0.650 | 0.964 |
| Stride length (cm) | 101.92 ± 11.57 | 107.78 ± 10.57 | 0.001 * | 95.58 ± 11.45 | 95.92 ± 11.59 | 0.118 | 0.001 * | |
| Double support% | 28.83 ± 5.66 | 28.63 ± 5.87 | 0.548 | 33.27 ± 7.79 | 31.36 ± 8.19 | 0.045 * | 0.031 * | |
| Obstacle crossing | Gait speed (cm/s) | 89.29 ± 13.78 | 89.37 ± 17.67 | 0.978 | 74.14 ± 24.52 | 78.53 ± 23.96 | 0.212 | 0.330 |
| Stride length (cm) | 98.21 ± 13.26 | 102.32 ± 12.29 | 0.145 | 92.83 ± 28.56 | 90.05 ± 27.79 | 0.317 | 0.080 | |
| Double support% | 26.19 ± 4.59 | 24.15 ± 3.60 | 0.004 * | 29.45 ± 9.79 | 30.79 ± 10.19 | 0.259 | 0.012 * | |
| Backward digit span | Gait speed (cm/s) | 77.35 ± 20.95 | 75.23 ± 15.41 | 0.524 | 59.86 ± 23.95 | 60.55 ± 26.59 | 0.783 | 0.500 |
| Stride length (cm) | 85.73 ± 15.36 | 85.55 ± 12.17 | 0.951 | 74.97 ± 26.99 | 73.61 ± 27.47 | 0.608 | 0.754 | |
| Double support% | 32.11 ± 5.60 | 31.49 ± 5.22 | 0.596 | 37.49 ± 11.45 | 38.64 ± 10.93 | 0.251 | 0.250 | |
| Serial-3 subtraction | Gait speed (cm/s) | 64.99 ± 18.12 | 66.52 ± 13.84 | 0.544 | 56.19 ± 21.61 | 59.64 ± 24.29 | 0.291 | 0.633 |
| Stride length (cm) | 77.69 ± 13.03 | 82.73 ± 10.39 | 0.021 * | 71.47 ± 25.30 | 73.09 ± 26.11 | 0.587 | 0.336 | |
| Double support% | 34.27 ± 7.33 | 32.13 ± 5.71 | 0.171 | 39.23 ± 11.78 | 38.49 ± 10.75 | 0.593 | 0.494 | |
| Secondary outcomes | ||||||||
| MDS-UPDRSIII | 21.63 ± 18.36 | 12.95 ± 9.00 | 0.021 * | 24.15 ± 15.89 | 21.55 ± 16.50 | 0.051 | 0.098 | |
| MDS-UPDRS | 43.78 ± 29.95 | 25.33 ± 16.38 | 0.004 * | 46.55 ± 28.77 | 38.95 ± 32.17 | 0.020 * | 0.084 | |
| TUGT (s) | 11.43 ± 3.48 | 10.05 ± 2.01 | 0.005 * | 11.24 ± 3.90 | 13.19 ± 4.48 | 0.029 | 0.001 * | |
| MiniBESTest | 20.05 ± 7.18 | 24.52 ± 4.20 | 0.023 * | 22.15 ± 5.88 | 22.35 ± 5.61 | 0.779 | 0.038 * | |
| PDQ-39 | 30.00 ± 17.24 | 22.37 ± 15.88 | 0.043 * | 26.79 ± 20.29 | 22.42 ± 18.87 | 0.166 | 0.486 | |
| Outcomes | Variables | Pre vs. Post12wk | |||
|---|---|---|---|---|---|
| WQ Group | Stretching Group | p | Effect Size | ||
| Primary outcomes | |||||
| Single-task | Gait speed (cm/s) | −6.39 ± 5.98 | −0.79 ± 7.43 | 0.045 * | 0.105 |
| Stride length (cm) | −5.85 ± 6.49 | −0.34 ± 0.90 | 0.014 * | 0.152 | |
| Double support% | 0.20 ± 1.49 | 1.53 ± 3.12 | 0.135 | 0.059 | |
| Obstacle crossing | Gait speed (cm/s) | −0.08 ± 12.42 | −4.39 ± 14.76 | 0.041 * | 0.108 |
| Stride length (cm) | −4.11 ± 12.09 | 2.78 ± 11.78 | 0.195 | 0.045 | |
| Double support% | 2.05 ± 2.78 | −1.34 ± 5.02 | 0.041 * | 0.108 | |
| Backward digit span | Gait speed (cm/s) | 2.12 ± 14.62 | −0.70 ± 10.89 | 0.862 | 0.001 |
| Stride length (cm) | 0.17 ± 12.17 | 1.36 ± 11.37 | 0.094 | 0.074 | |
| Double support% | 0.62 ± 5.15 | −1.15 ± 4.22 | 0.025 * | 0.128 | |
| Serial-3 subtraction | Gait speed (cm/s) | −1.52 ± 11.01 | −3.44 ± 13.81 | 0.200 | 0.044 |
| Stride length (cm) | −5.04 ± 8.98 | −1.62 ± 12.76 | 0.201 | 0.044 | |
| Double support% | 2.14 ± 6.74 | 0.74 ± 5.91 | 0.047 * | 0.103 | |
| Secondary outcomes | |||||
| MDS-UPDRSIII | 8.68 ± 14.96 | 2.60 ± 5.58 | 0.165 | 0.053 | |
| MDS-UPDRS | 18.44 ± 23.34 | 7.60 ± 13.43 | 0.339 | 0.025 | |
| TUGT (s) | 1.38 ± 1.98 | −1.95 ± 3.71 | 0.155 | 0.051 | |
| MiniBESTest | −4.48 ± 8.33 | −0.20 ± 3.14 | 0.981 | 0.000 | |
| PDQ-39 | 7.63 ± 15.30 | 4.37 ± 13.16 | 0.774 | 0.002 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Z.; Wang, T.; Shen, M.; Song, T.; He, J.; Guo, W.; Wang, Z.; Zhuang, J. Comparison of Wuqinxi Qigong with Stretching on Single- and Dual-Task Gait, Motor Symptoms and Quality of Life in Parkinson’s Disease: A Preliminary Randomized Control Study. Int. J. Environ. Res. Public Health 2022, 19, 8042. https://doi.org/10.3390/ijerph19138042
Li Z, Wang T, Shen M, Song T, He J, Guo W, Wang Z, Zhuang J. Comparison of Wuqinxi Qigong with Stretching on Single- and Dual-Task Gait, Motor Symptoms and Quality of Life in Parkinson’s Disease: A Preliminary Randomized Control Study. International Journal of Environmental Research and Public Health. 2022; 19(13):8042. https://doi.org/10.3390/ijerph19138042
Chicago/Turabian StyleLi, Zhenlan, Tian Wang, Mengyue Shen, Tao Song, Jie He, Wei Guo, Zhen Wang, and Jie Zhuang. 2022. "Comparison of Wuqinxi Qigong with Stretching on Single- and Dual-Task Gait, Motor Symptoms and Quality of Life in Parkinson’s Disease: A Preliminary Randomized Control Study" International Journal of Environmental Research and Public Health 19, no. 13: 8042. https://doi.org/10.3390/ijerph19138042