
Letting the World See through Your Eyes: Using Photovoice to Explore the Role of Technology in Physical Activity for Adolescents Living with Type 1 Diabetes




Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Participants
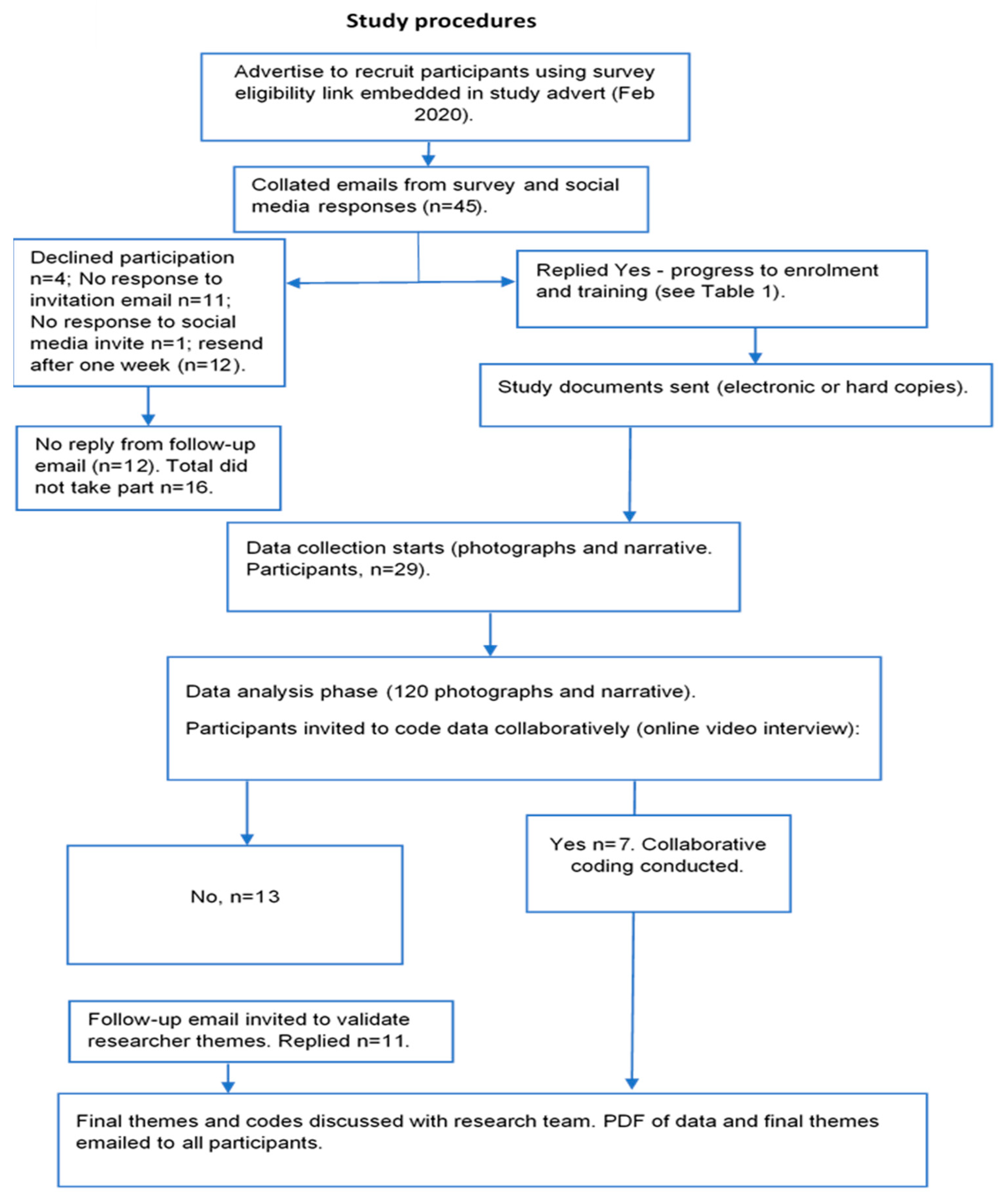
2.3. Procedures
2.4. Ethics, Recruitment and Training
- What technology are you using?
- What physical activity are you doing?
- What support is involved for you to be physically active?
- What other related impact does physical activity have on your lives?
2.5. Data Analysis and Shared Meaning
3. Results
Photographs with Narrative
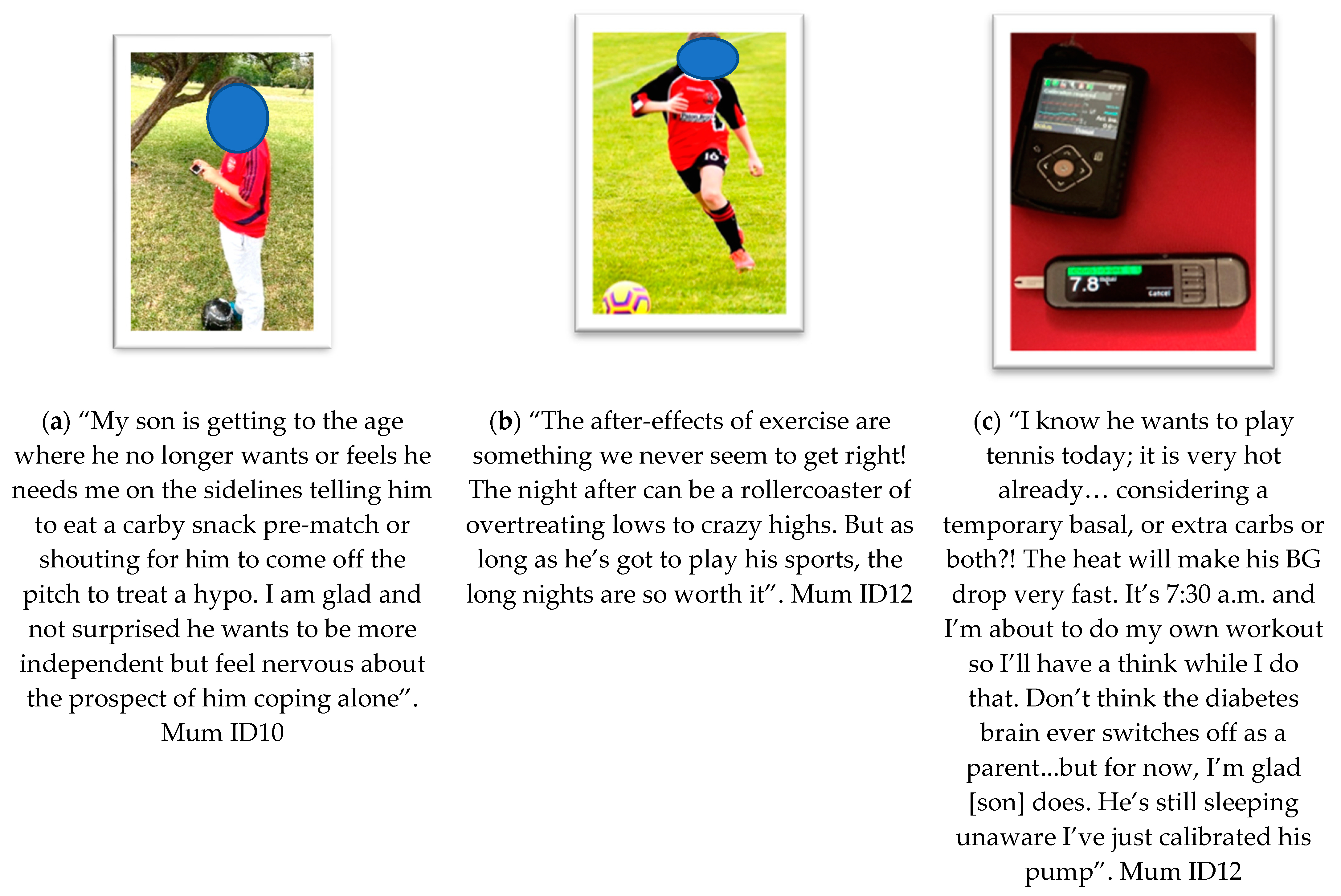
- Theme 1: Benefits of Technology (Figure 2)
- Theme 2: Complexity and Difficulty (Figure 3)
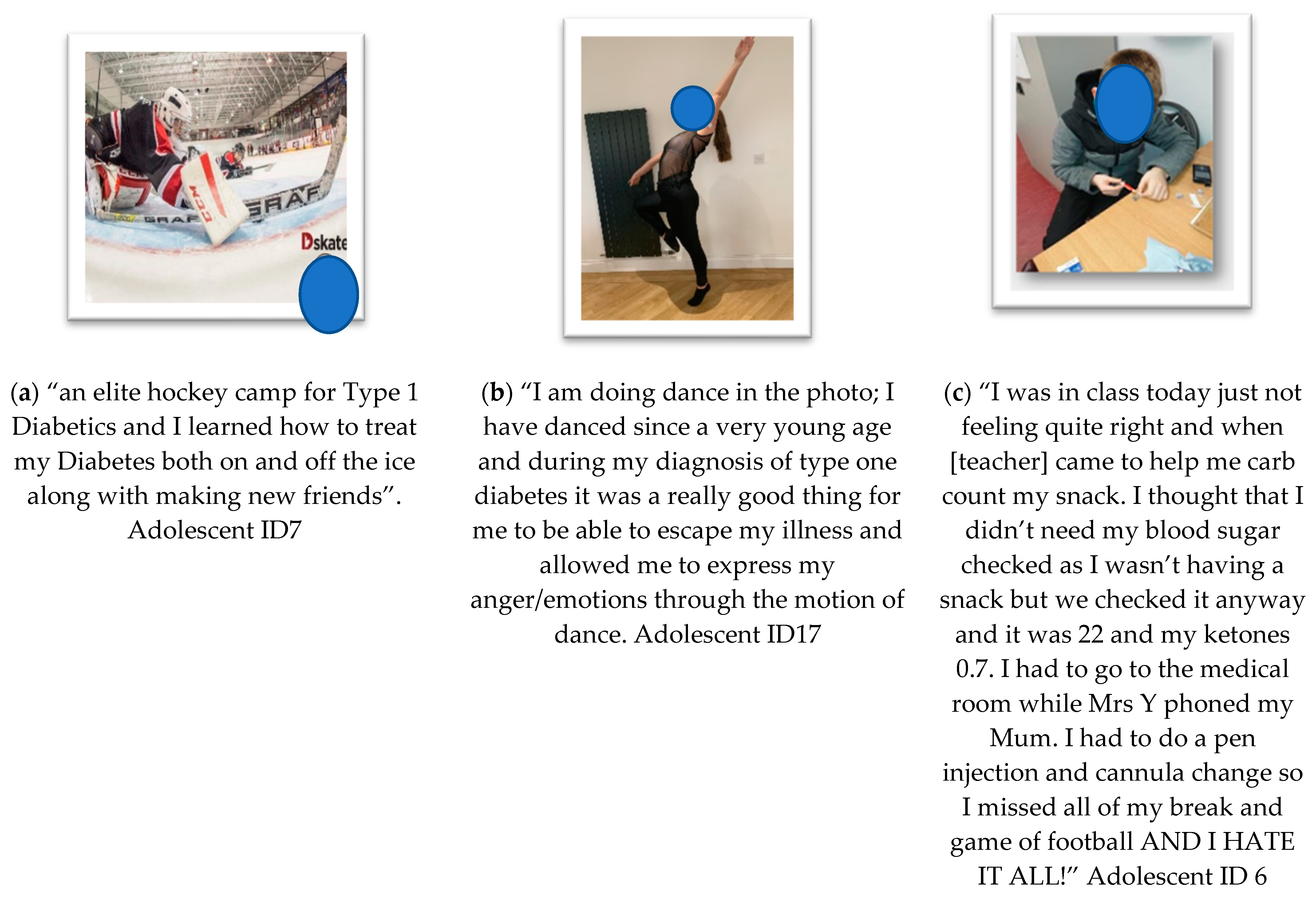
- Theme 3: Emotional Impact (Figure 4)
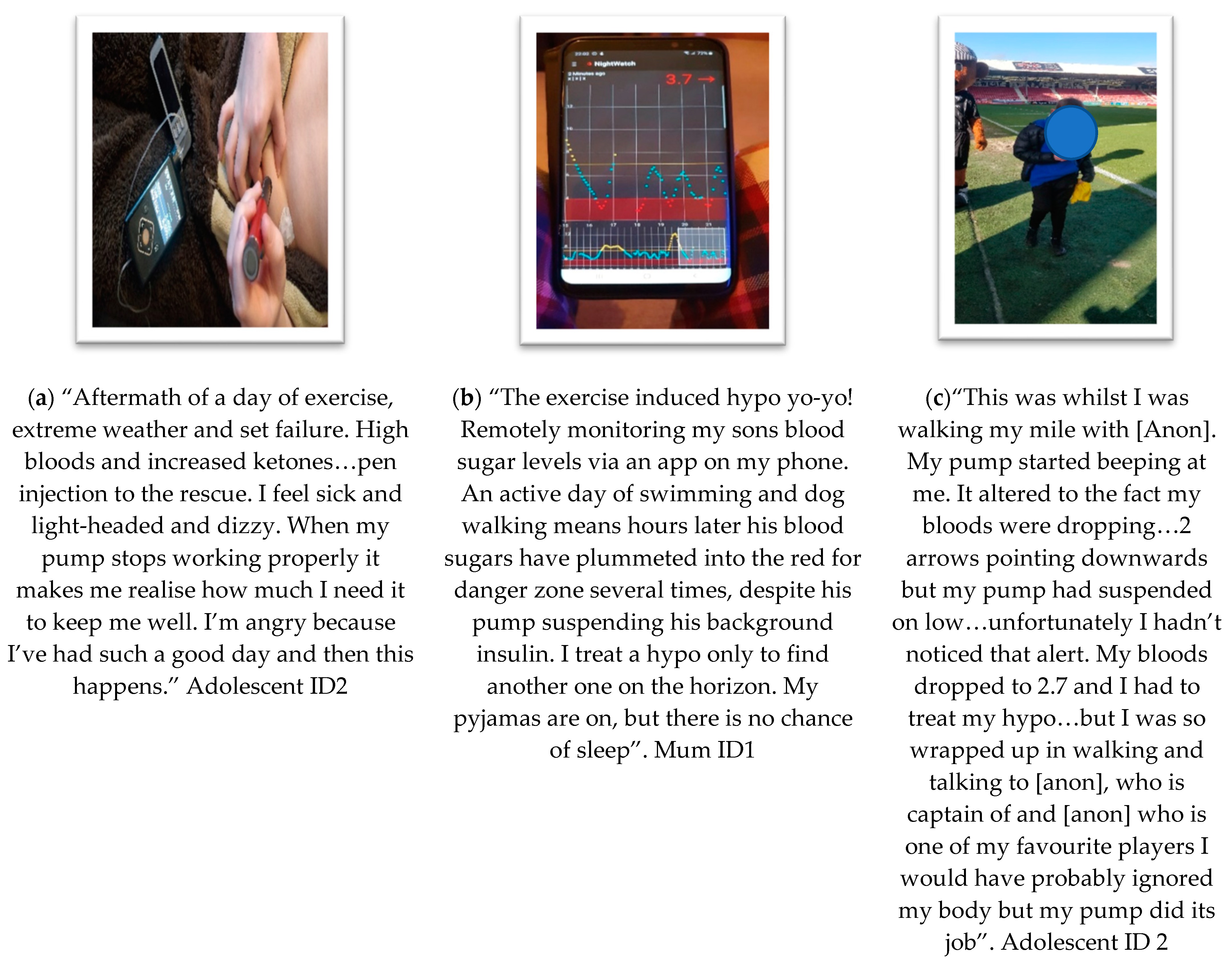
- Theme 4: Reliance and Risk (Figure 5)
4. Discussion
4.1. Benefits of Technology
4.2. Complexity and Difficulty
4.3. Emotional Impact
4.4. Reliance and Risk
4.5. Strengths, Limitations and the Use of Photovoice
5. Conclusions
- (i)
- Diabetes-monitoring technologies and PA devices need to be more interoperable and work more seamlessly together (e.g., accelerometry data and glucose variability). Combining these technologies should seek to incorporate the benefits of “hands-free” experiences using glanceability and data sharing through trusted channels. Interoperability will reduce the amount of devices that people interact with in order to make informed choices about T1D management during periods of PA.
- (ii)
- Interventions need to facilitate and promote peer support which considers adolescents and parents/caregivers as central, active agents in a workshop-led or digitally based education. These support mechanisms are important for continuing to build agency and empowerment to understand technology, as it changes and develops rapidly. Parents also require ongoing support as caregivers and intense users of the technology.
- (iii)
- A focus is needed on psycho-educational support for navigating independence for both those living with T1D and their parents/caregivers, especially during transition periods. Physical activity is often performed away from home or in the community where teachers and coaches often lack knowledge of the effects of PA on T1D. This often caused frustration, and anxiety for both parents as caregivers and adolescents living with T1D.
- (iv)
- Digital educational content should be personalisable to person-specific technological choices, i.e., pump users, CGM users, pens/meters, and to teachers and healthcare professionals with accompanying tailored PA advice. Consumer power for choices of technology allows for different technologies to treat T1D. These can impact the choice, duration and type of PA taken.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- International Diabetes Federation. IDF Diaebtes Atlas. 2019. Available online: https://www.diabetesatlas.org/upload/resources/2019/IDF_Atlas_9th_Edition_2019.pdf (accessed on 1 January 2020).
- DCCT. Effect of intensive diabetes treatment on the development and progression of long-term complications in adolescents with insulin-dependent diabetes mellitus: Diabetes Control and Complications Trial. Diabetes Control and Complications Trial Research Group. J. Pediatr. 1994, 125, 177–188. [Google Scholar] [CrossRef]
- Chiang, J.L.; Maahs, D.M.; Garvey, K.C.; Hood, K.K.; Laffel, L.M.; Weinzimer, S.A.; Wolfsdorf, J.I.; Schatz, D. Type 1 Diabetes in Children and Adolescents: A Position Statement by the American Diabetes Association. Diabetes Care 2018, 41, 2026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hood, K.K.; Hilliard, M.; Piatt, G.; Ievers-Landis, C.E. Effective strategies for encouraging behavior change in people with diabetes. Diabetes Manag. 2015, 5, 499–510. [Google Scholar] [CrossRef]
- Dauber, A.; Corcia, L.; Safer, J.; Agus, M.S.; Einis, S.; Steil, G.M. Closed-loop insulin therapy improves glycemic control in children aged < 7 years: A randomized controlled trial. Diabetes Care 2013, 36, 222–227. [Google Scholar] [PubMed] [Green Version]
- Kropff, J.; Del Favero, S.; Place, J.; Toffanin, C.; Visentin, R.; Monaro, M.; Farret, A. 2 month evening and night closed-loop glucose control in patients with type 1 diabetes under free-living conditions: A randomised crossover trial. Lancet Diabetes Endocrinol. 2015, 3, 939–947. [Google Scholar] [CrossRef]
- Phillip, M.; Battelino, T.; Atlas, E.; Kordonouri, O.; Bratina, N.; Miller, S.; Biester, T.; Avbelj Stefanija, M.; Muller, I.; Nimri, R. Nocturnal glucose control with an artificial pancreas at a diabetes camp. N. Engl. J. Med. 2013, 368, 824–833. [Google Scholar] [CrossRef] [Green Version]
- Bergenstal, R.M.; Tamborlane, W.V.; Ahmann, A.; Buse, J.B.; Dailey, G.; Davis, S.N.; Joyce, C.; Peoples, T.; Perkins, B.A.; Welsh, J.B. Effectiveness of sensor-augmented insulin-pump therapy in type 1 diabetes. N. Engl. J. Med. 2010, 363, 311–320. [Google Scholar] [CrossRef] [Green Version]
- Breton, M.D.; Cherñavvsky, D.R.; Forlenza, G.P.; DeBoer, M.D.; Robic, J.; Wadwa, R.P.; Messer, L.H.; Kovatchev, B.P.; Maahs, D.M. Closed-loop control during intense prolonged outdoor exercise in adolescents with type 1 diabetes: The artificial pancreas ski study. Diabetes Care 2017, 40, 1644–1650. [Google Scholar] [CrossRef] [Green Version]
- Tauschmann, M.; Hovorka, R. Technology in the management of type 1 diabetes mellitus—Current status and future prospects. Nat. Rev. Endocrinol. 2018, 14, 464–475. [Google Scholar] [CrossRef]
- Zaharieva, D.P.; Messer, L.H.; Paldus, B.; O’Neal, D.N.; Maahs, D.M.; Riddell, M.C. Glucose Control During Physical Activity and Exercise Using Closed Loop Technology in Adults and Adolescents with Type 1 Diabetes. Can. J. Diabetes 2020, 44, 740–749. [Google Scholar] [CrossRef]
- Asim, Y.; Azam, M.A.; Ehatisham-ul-Haq, M.; Naeem, U.; Khalid, A. Context-aware human activity recognition (CAHAR) in-the-Wild using smartphone accelerometer. IEEE Sens. J. 2020, 20, 4361–4371. [Google Scholar] [CrossRef]
- Kercher, V.M.; Kercher, K.; Bennion, T.; Yates, B.A.; Feito, Y.; Alexander, C.; Han, J. Fitness trends from around the globe. ACSM’s Health Fit. J. 2021, 25, 20–31. [Google Scholar] [CrossRef]
- Department of Health and Social Care. UK Chief Medical Officers’ Physical Activity Guidelines; Department of Health and Social Care: London, UK, 2019.
- Czenczek-Lewandowska, E.; Leszczak, J.; Baran, J.; Weres, A.; Wyszyńska, J.; Lewandowski, B.; Mazur, A. Levels of Physical Activity in Children and Adolescents with Type 1 Diabetes in Relation to the Healthy Comparators and to the Method of Insulin Therapy Used. Int. J. Environ. Res. Public Health 2019, 16, 3498. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacMillan, F.; Kirk, A.; Mutrie, N.; Robertson, K. Physical activity and sedentary behaviour in Scottish youth with type 1 diabetes. Pract. Diabetes 2014, 31, 228–233c. [Google Scholar] [CrossRef]
- Dahl-Jørgensen, K.; Larsen, J.R.; Hanssen, K.F.J.D. Atherosclerosis in childhood and adolescent type 1 diabetes: Early disease, early treatment? Diabetologia 2005, 48, 1445–1453. [Google Scholar] [CrossRef] [Green Version]
- MacMillan, F.; Kirk, A.; Mutrie, N.; Matthews, L.; Robertson, K.; Saunders, D.H. A systematic review of physical activity and sedentary behavior intervention studies in youth with type 1 diabetes: Study characteristics, intervention design, and efficacy. Pediatr. Diabetes 2014, 15, 175–189. [Google Scholar] [CrossRef]
- Czenczek-Lewandowska, E.; Leszczak, J.; Weres, A.; Baran, J.; Wyszyńska, J.; Grzegorczyk, J.; Mazur, A. Sedentary behaviors in children and adolescents with type 1 diabetes, depending on the insulin therapy used. Medicine 2019, 98, e15625. [Google Scholar] [CrossRef]
- de Lima, V.A.; Mascarenhas, L.P.G.; Decimo, J.P.; de Souza, W.C.; Monteiro, A.L.S.; Lahart, I.; França, S.N.; Leite, N. Physical Activity Levels of Adolescents with Type 1 Diabetes Physical Activity in T1D. Pediatr. Exerc. Sci. 2017, 29, 213–219. [Google Scholar] [CrossRef]
- Michaliszyn, S.F.; Faulkner, M.S. Physical activity and sedentary behavior in adolescents with type 1 diabetes. Res. Nurs. Health 2010, 33, 441–449. [Google Scholar] [CrossRef]
- Faulkner, M.S.; Michaliszyn, S.F.; Hepworth, J.T. A personalized approach to exercise promotion in adolescents with type 1 diabetes. Pediatr. Diabetes 2010, 11, 166–174. [Google Scholar] [CrossRef]
- Codella, R.; Terruzzi, I.; Luzi, L. Why should people with type 1 diabetes exercise regularly? Acta Diabetol. 2017, 54, 615–630. [Google Scholar] [CrossRef] [PubMed]
- Riddell, M.C.; Zaharieva, D.P.; Tansey, M.; Tsalikian, E.; Admon, G.; Li, Z.; Beck, R.W. Individual glucose responses to prolonged moderate intensity aerobic exercise in adolescents with type 1 diabetes: The higher they start, the harder they fall. Pediatr. Diabetes 2019, 20, 99–106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacMillan, F.; Kirk, A.; Mutrie, N.; Moola, F.; Robertson, K. Supporting participation in physical education at school in youth with type 1 diabetes: Perceptions of teachers, youth with type 1 diabetes, parents and diabetes professionals. Eur. Phys. Educ. Rev. 2014, 21, 3–30. [Google Scholar] [CrossRef]
- Wang, C.C.; Redwood-Jones, Y.A. Photovoice Ethics: Perspectives from Flint Photovoice. Health Educ. Behav. 2001, 28, 560–572. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. One size fits all? What counts as quality practice in (reflexive) thematic analysis? Qual. Res. Psychol. 2020, 18, 1–25. [Google Scholar] [CrossRef]
- Ciolan, L.; Manasia, L. Reframing photovoice to boost its potential for learning research. Int. J. Qual. Methods 2017, 16, 1609406917702909. [Google Scholar] [CrossRef]
- Barnard, K.D.; Wysocki, T.; Allen, J.M.; Elleri, D.; Thabit, H.; Leelarathna, L.; Gulati, A.; Nodale, M.; Dunger, D.B.; Tinati, T.; et al. Closing the loop overnight at home setting: Psychosocial impact for adolescents with type 1 diabetes and their parents. BMJ Open Diabetes Res. Care 2014, 2, e000025. [Google Scholar] [CrossRef] [Green Version]
- Burckhardt, M.-A.; Fried, L.; Bebbington, K.; Hancock, M.; Nicholas, J.A.; Roberts, A.; Jones, T.W. Use of remote monitoring with continuous glucose monitoring in young children with Type 1 diabetes: The parents’ perspective. Diabet. Med. 2019, 36, 1453–1459. [Google Scholar] [CrossRef]
- Quirk, H.; Blake, H.; Dee, B.; Glazebrook, C. “You can’t just jump on a bike and go”: A qualitative study exploring parents’ perceptions of physical activity in children with type 1 diabetes. BMC Pediatr. 2014, 14, 313. [Google Scholar] [CrossRef]
- Choudhary, P.; Olsen, B.S.; Conget, I.; Welsh, J.B.; Vorrink, L.; Shin, J.J. Hypoglycemia Prevention and User Acceptance of an Insulin Pump System with Predictive Low Glucose Management. Diabetes Technol. Ther. 2016, 18, 288–291. [Google Scholar] [CrossRef] [Green Version]
- Borus, J.S.; Laffel, L. Adherence challenges in the management of type 1 diabetes in adolescents: Prevention and intervention. Curr. Opin. Pediatr. 2010, 22, 405–411. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maahs, D.M.; Calhoun, P.; Buckingham, B.A.; Chase, H.P.; Hramiak, I.; Lum, J.; Beck, R.W. A Randomized Trial of a Home System to Reduce Nocturnal Hypoglycemia in Type 1 Diabetes. J. Diabetes Care 2014, 37, 1885–1891. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gonder-Frederick, L.; Nyer, M.; Shepard, J.A.; Vajda, K.; Clarke, W. Assessing fear of hypoglycemia in children with Type 1 diabetes and their parents. Diabetes Manag. 2011, 1, 627–639. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Monzon, A.; McDonough, R.; Meltzer, L.J.; Patton, S.R. Sleep and type 1 diabetes in children and adolescents: Proposed theoretical model and clinical implications. Pediatr. Diabetes 2019, 20, 78–85. [Google Scholar] [CrossRef] [Green Version]
- Englert, K.; Ruedy, K.; Coffey, J.; Caswell, K.; Steffen, A.; Levandoski, L. Skin and adhesive issues with continuous glucose monitors: A sticky situation. J. Diabetes Sci. Technol. 2014, 8, 745–751. [Google Scholar] [CrossRef]
- Shivers, J.P.; Mackowiak, L.; Anhalt, H.; Zisser, H. “Turn it off!” Diabetes device alarm fatigue considerations for the present and the future. J. Diabetes Sci. Technol. 2013, 7, 789–794. [Google Scholar] [CrossRef] [Green Version]
- Yi-Frazier, J.P.; Cochrane, K.; Mitrovich, C.; Pascual, M.; Buscaino, E.; Eaton, L.; Panlasigui, N.; Clopp, B.; Malik, F. Using Instagram as a Modified Application of Photovoice for Storytelling and Sharing in Adolescents with Type 1 Diabetes. Qual. Health Res. 2015, 25, 1372–1382. [Google Scholar] [CrossRef]
- Latz, A.O. Photovoice Research in Education and Beyond: A Practical Guide from Theory to Exhibition; Taylor & Francis: London, UK, 2017. [Google Scholar]
- McCarthy, G.M.; Ramirez, E.R.R.; Robinson, B.J. Participatory Design to Address Stigma with Adolescents with Type 1 Diabetes. In Proceedings of the 2017 Conference on Designing Interactive Systems, Edinburgh, UK, 10–14 June 2017; pp. 83–94. [Google Scholar]
- Strack, R.W.; Magill, C.; McDonagh, K. Engaging Youth through Photovoice. Health Promot. Pract. 2004, 5, 49–58. [Google Scholar] [CrossRef] [Green Version]
- Woodgate, R.L.; Zurba, M.; Tennent, P. Worth a Thousand Words? Advantages, Challenges and Opportunities in Working with Photovoice as a Qualitative Research Method with Youth and their Families. Forum Qual. Soc. Res. 2017, 18. Available online: http://www.qualitative-research.net/index.php/fqs/article/view/2659/4045 (accessed on 1 January 2020).
- Foster-Fishman, P.; Nowell, B.; Deacon, Z.; Nievar, M.A.; McCann, P. Using methods that matter: The impact of reflection, dialogue, and voice. Am. J. Community Psychol. 2005, 36, 275–291. [Google Scholar] [CrossRef]
- Racadio, R.; Rose, E.J.; Kolko, B.E. Research at the margin: Participatory design and community based participatory research. In Proceedings of the 13th Participatory Design Conference: Short Papers, Industry Cases, Workshop Descriptions, Doctoral Consortium papers, and Keynote abstracts—Volume 2, Windhoek, Namibia, 6–10 October 2014; pp. 49–52. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant ID | Description | Age of Adolescent (Years) |
|---|---|---|
| 1 | Mother & son | 9 |
| 2 | Mother & son | 11 |
| 3 | Mother & daughter | 14 |
| 4 | Adolescent female | 14 |
| 5 | Adolescent female | 14 |
| 6 | Mother & son | 10 |
| 7 | Mother | 17 |
| 8 | Mother | 16 |
| 9 | Father | 10 |
| 10 | Mother & son | 15 |
| 11 | Mother & son | 16 |
| 12 | Mother | 13 |
| 13 | Mother & daughter | 12 |
| 14 | Mother & son | 10 |
| 15 | Adolescent female | 16 |
| 16 | Adolescent female | 13 |
| 17 | Adolescent female | 17 |
| 18 | Adolescent male | 10 |
| 19 | Mother | 11 |
| 20 | Adolescent female | 11 |
| Mean | 12.95 |
| Narrative | Initial Researcher Codes | Collaborative Codes with Co-Researchers | Theme Refinement |
|---|---|---|---|
| Adolescent ID11: “I use the phone to message my mum when I’m in my room or when she is out of the house. (Mum ID11: It’s a good thing because he can just message me). Adolescent ID11: “It makes me feel safer because I can use the phone to send my blood readings a to my mum. It is also good because it distracts me from my diabetes, and I can think about other things that are not to do with diabetes.” | Teen messaging mum—helps independence. Perceived as good by mum Feeling safe Messaging blood sugar data to mum when away Freedom from thinking about diabetes | Benefits of technology—communicating remotely about T1D for parental support Parental emotions: peace of mind Technology improves T1D perceived safety Teen resilience | Communication and immediate support (Benefits of technology) Emotional impact Resilience & positivity |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Morrow, D.; Kirk, A.; Muirhead, F.; Lennon, M. Letting the World See through Your Eyes: Using Photovoice to Explore the Role of Technology in Physical Activity for Adolescents Living with Type 1 Diabetes. Int. J. Environ. Res. Public Health 2022, 19, 6315. https://doi.org/10.3390/ijerph19106315
Morrow D, Kirk A, Muirhead F, Lennon M. Letting the World See through Your Eyes: Using Photovoice to Explore the Role of Technology in Physical Activity for Adolescents Living with Type 1 Diabetes. International Journal of Environmental Research and Public Health. 2022; 19(10):6315. https://doi.org/10.3390/ijerph19106315
Chicago/Turabian StyleMorrow, Diane, Alison Kirk, Fiona Muirhead, and Marilyn Lennon. 2022. "Letting the World See through Your Eyes: Using Photovoice to Explore the Role of Technology in Physical Activity for Adolescents Living with Type 1 Diabetes" International Journal of Environmental Research and Public Health 19, no. 10: 6315. https://doi.org/10.3390/ijerph19106315