
Efficacy of Combining an Extraoral High-Volume Evacuator with Preprocedural Mouth Rinsing in Reducing Aerosol Contamination Produced by Ultrasonic Scaling

 , ,
, , {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Inclusion and Exclusion Criteria
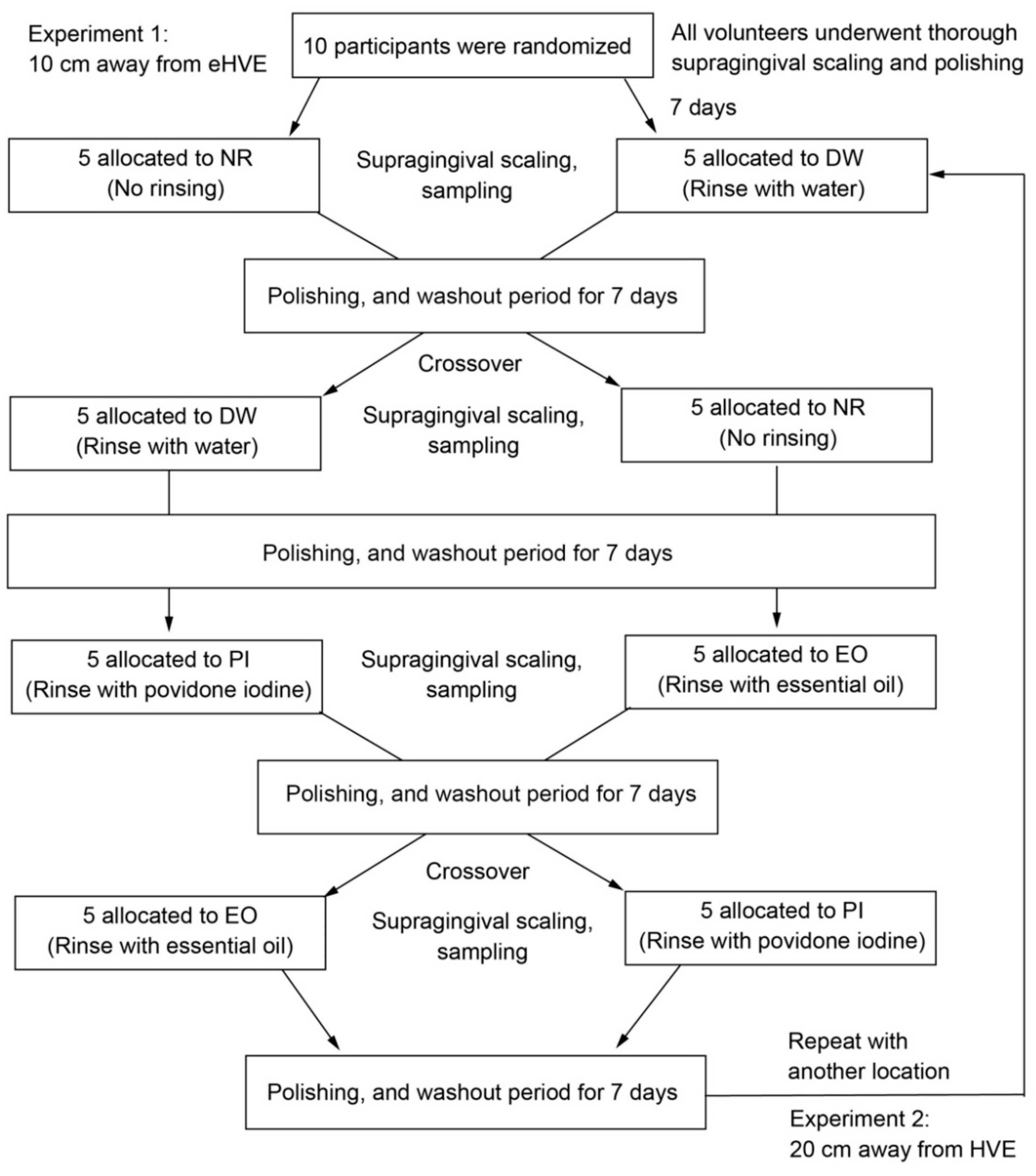
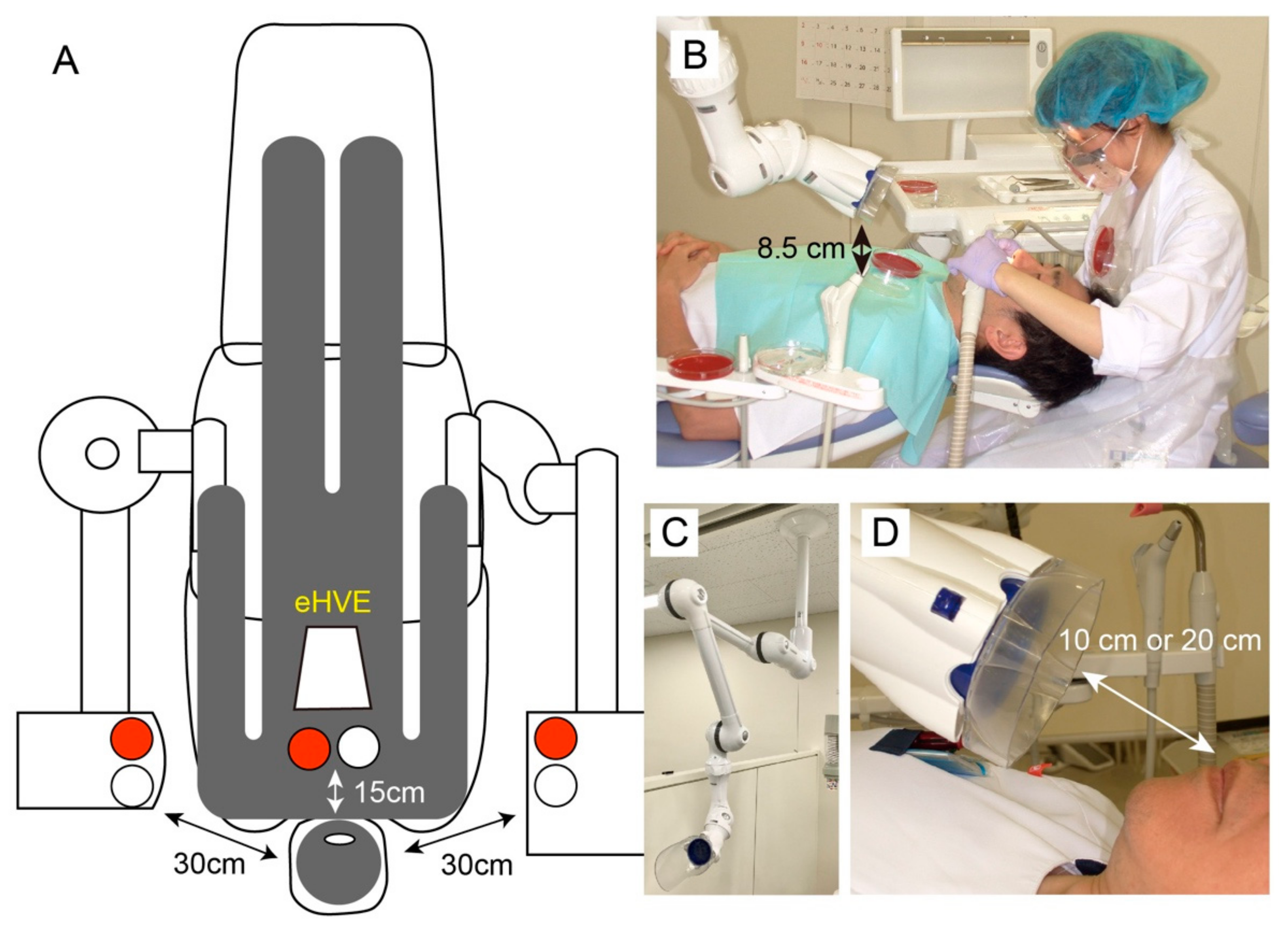
2.3. Study Design
2.4. Total Cell Counting
2.5. Viable Cell Counting in the Mouth after Preprocedural Mouth Rinsing
2.6. Statistical Analysis
3. Results
3.1. Baseline Demographic and Clinical Characteristics
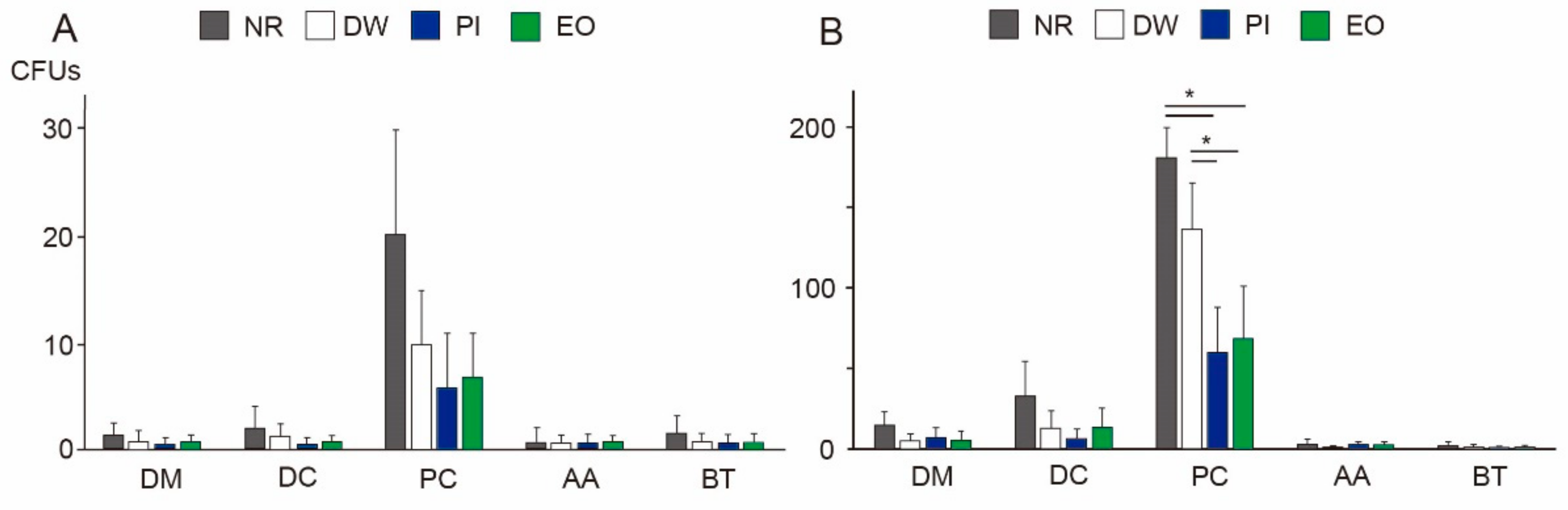
3.2. Viable Bacteria in Dental Aerosols
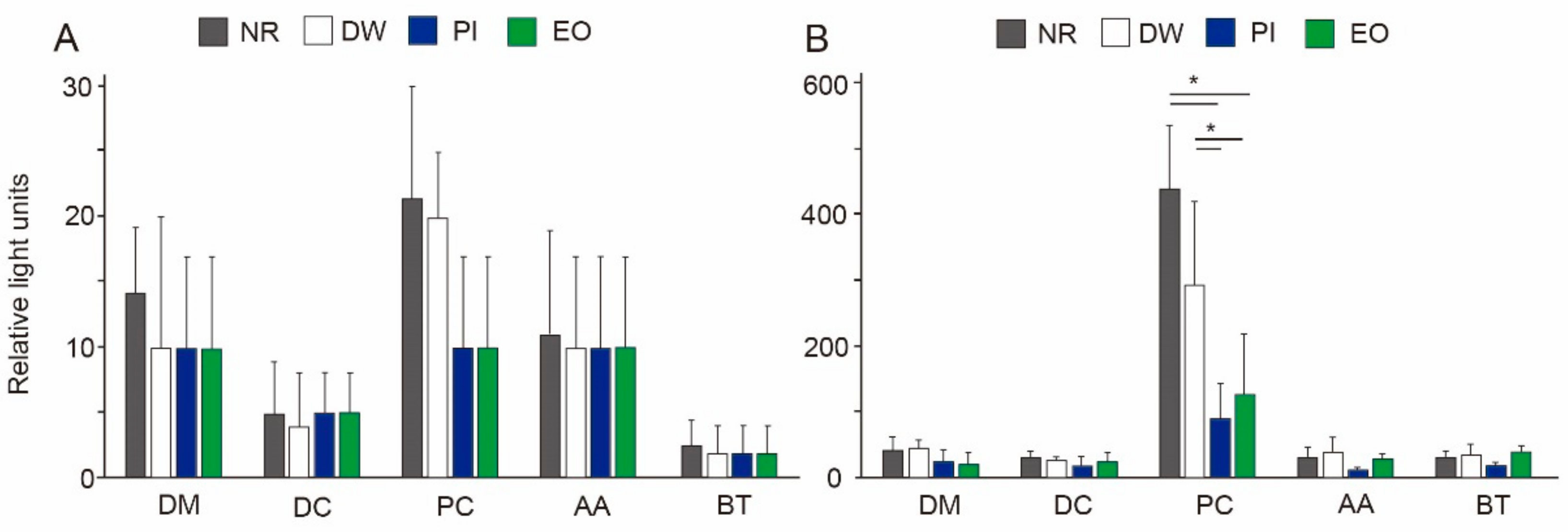
3.3. Total Bacteria in Dental Aerosols
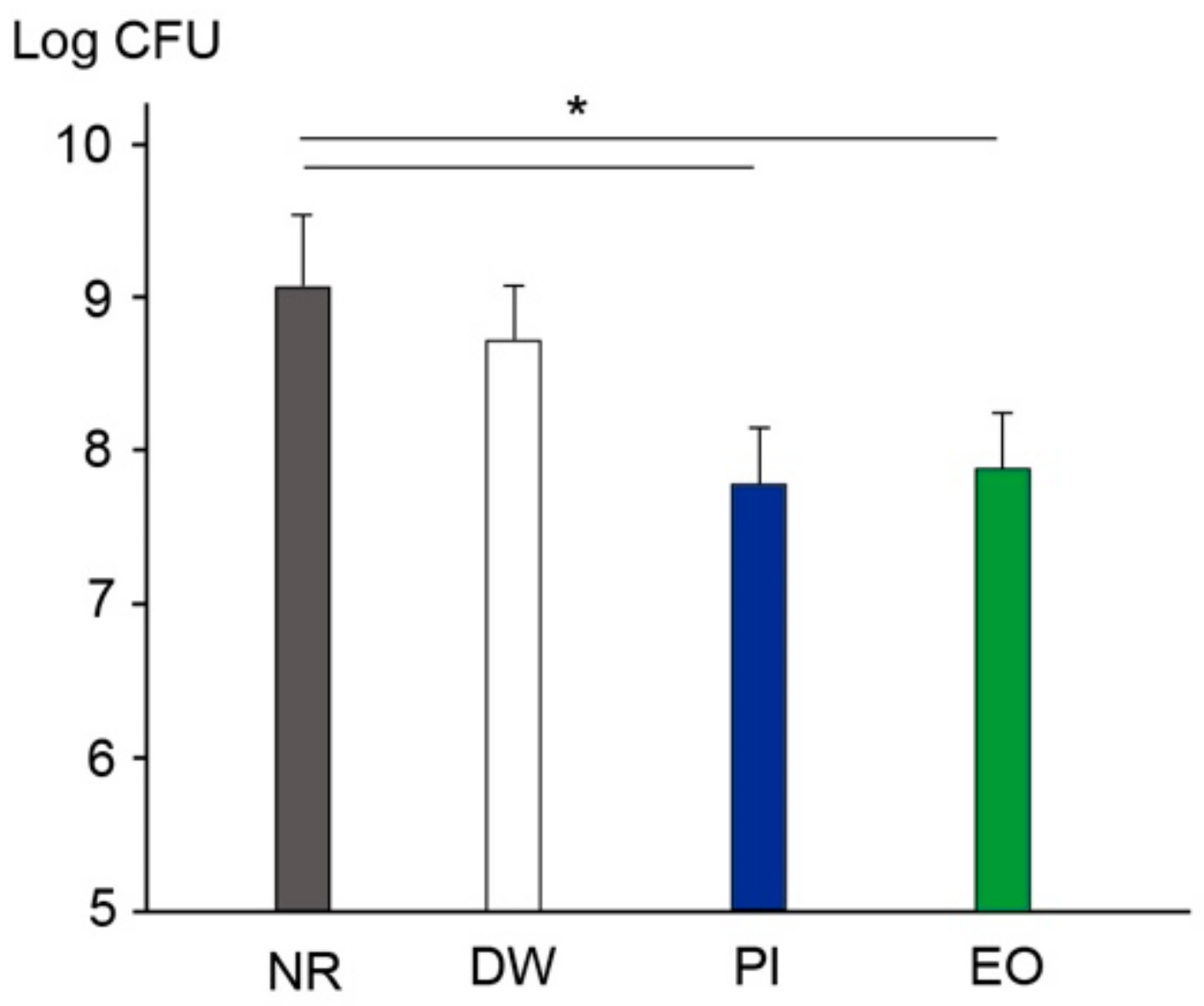
3.4. Viable Cell Counting in the Mouth after Preprocedural Mouth Rinsing
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Coronavirus Disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/ (accessed on 13 May 2022).
- Rees, E.E.; Rodin, R.; Ogden, N.H. Population surveillance approach to detect and respond to new clusters of COVID-19. Can. Commun. Dis. Rep. 2021, 47, 243–250. [Google Scholar] [CrossRef] [PubMed]
- Verbeek, H.; Gerritsen, D.L.; Backhaus, R.; de Boer, B.S.; Koopmans, R.T.C.M.; Hamers, J.P.H. Allowing visitors back in the nursing home during the COVID-19 crisis: A Dutch national study into first experiences and impact on well-being. J. Am. Med. Dir. Assoc. 2020, 21, 900–904. [Google Scholar] [CrossRef] [PubMed]
- Carter, B.; Collins, J.T.; Barlow-Pay, F.; Rickard, F.; Bruce, E.; Verduri, A.; Quinn, T.J.; Mitchell, E.; Price, A.; Vilches-Moraga, A.; et al. Nosocomial COVID-19 infection: Examining the risk of mortality. The COPE-Nosocomial Study (COVID in Older People). J. Hosp. Infect. 2020, 106, 376–384. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Ouyang, W.; Chua, M.L.K.; Xie, C. SARS-CoV-2 transmission in patients with cancer at a tertiary care hospital in Wuhan, China. JAMA Oncol. 2020, 6, 1108–1110. [Google Scholar] [CrossRef] [Green Version]
- Chan, J.F.W.; Yuan, S.; Kok, K.H.; To, K.K.W.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.Y.; Poon, R.W.S.; et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [Green Version]
- Gold, J.A.W.; Gettings, J.R.; Kimball, A.; Franklin, R.; Rivera, G.; Morris, E.; Scott, C.; Marcet, P.L.; Hast, M.; Swanson, M.; et al. Clusters of SARS-CoV-2 infection among elementary school educators and students in one school distict- Georgia, December 2020- January 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 289–292. [Google Scholar] [CrossRef]
- Furuse, Y.; Sando, E.; Tsuchiya, N.; Miyahara, R.; Yasuda, I.; Ko, Y.K.; Saito, M.; Morimoto, K.; Imamura, T.; Shobugawa, Y.; et al. Clusters of coronavirus disease in communities, Japan, January–April 2020. Emerg. Infect. Dis. 2020, 26, 2176–2179. [Google Scholar] [CrossRef]
- McMullen, K.M.; Smith, B.A.; Rebmann, T. Impact of SARS-CoV-2 on hospital acquired infection rates in the United States: Predictions and early results. Am. J. Infect. Control. 2020, 48, 1409–1411. [Google Scholar] [CrossRef]
- Woodford, N.; Livermore, D.M. Infections caused by Gram-positive bacteria: A review of the global challenge. J. Infect. 2009, 59 (Suppl. 1), S4–S16. [Google Scholar] [CrossRef]
- Chong, J.; Caya, C.; Lévesque, S.; Quach, C. Heteroresistant vancomycin intermediate coagulase negative Staphylococcus in the NICU: A systematic review. PLoS ONE 2016, 11, e0164136. [Google Scholar] [CrossRef] [Green Version]
- CDC. Standard Precautions. Available online: https://www.cdc.gov/oralhealth/infectioncontrol/summary-infection-prevention-practices/standard-precautions.html (accessed on 13 May 2022).
- Kohn, W.G.; Collins, A.S.; Cleveland, J.L.; Harte, J.A.; Eklund, K.J.; Malvitz, D.M.; Centers for Disease Control and Prevention (CDC). Guidelines for infection control in dental health-care settings—2003. MMWR Recomm. Rep. 2003, 52, 1–61. [Google Scholar]
- Meng, L.; Hua, F.; Bian, Z. Coronavirus Disease 2019 (COVID-19): Emerging and future challenges for dental and oral medicine. J. Dent. Res. 2020, 99, 481–487. [Google Scholar] [CrossRef] [Green Version]
- Peng, X.; Xu, X.; Li, Y.; Cheng, L.; Zhou, X.; Ren, B. Transmission routes of 2019-nCoV and controls in dental practice. Int. J. Oral Sci. 2020, 12, 9. [Google Scholar] [CrossRef]
- Johnson, I.G.; Jones, R.J.; Gallagher, J.E.; Wade, W.G.; Al-Yaseen, W.; Robertson, M.D.; McGregor, S.; Sukriti, K.; Innes, N.P.; Harris, R.V. Dental periodontal procedures: A systematic review of contamination (splatter, droplets and aerosol) in relation to COVID-19. BDJ Open. 2021, 7, 15. [Google Scholar] [CrossRef]
- Suprono, M.S.; Won, J.; Savignano, R.; Zhong, Z.; Ahmed, A.; Roque-Torres, G.; Zhang, W.; Oyoyo, U.; Richardson, P.; Caruso, J.; et al. A clinical investigation of dental evacuation systems in reducing aerosols. J. Am. Dent. Assoc. 2021, 152, 455–462. [Google Scholar] [CrossRef]
- Ou, Q.; Placucci, R.G.; Danielson, J.; Anderson, G.; Olin, P.; Jardine, P.; Madden, J.; Yuan, Q.; Grafe, T.H.; Shao, S.; et al. Characterization and mitigation of aerosols and spatters from ultrasonic scalers. J. Am. Dent. Assoc. 2021, 152, 981–990. [Google Scholar] [CrossRef]
- Teanpaisan, R.; Taeporamaysamai, M.; Rattanachone, P.; Poldoung, N.; Srisintorn, S. The usefulness of the modified extra-oral vacuum aspirator (EOVA) from household vacuum cleaner in reducing bacteria in dental aerosols. Int. Dent. J. 2001, 51, 413–416. [Google Scholar] [CrossRef]
- Cochran, M.A.; Miller, C.H.; Sheldrake, M.A. The efficacy of the rubber dam as a barrier to the spread of microorganisms during dental treatment. J. Am. Dent. Assoc. 1989, 119, 141–144. [Google Scholar] [CrossRef]
- Nagraj, S.K.; Eachempati, P.; Paisi, M.; Nasser, M.; Sivaramakrishnan, G.; Verbeek, J.H. Interventions to reduce contaminated aerosols produced during dental procedures for preventing infectious diseases. Cochrane Database Syst. Rev. 2020, 10, CD013686. [Google Scholar] [CrossRef]
- Gupta, G.; Mitra, D.; Ashok, K.P.; Gupta, A.; Soni, S.; Ahmed, S.; Arya, A. Efficacy of preprocedural mouth rinsing in reducing aerosol contamination produced by ultrasonic scaler: A pilot study. J. Periodontol. 2014, 85, 562–568. [Google Scholar] [CrossRef]
- Retamal-Valdes, B.; Soares, G.M.; Stewart, B.; Figueiredo, L.C.; Faveri, M.; Miller, S.; Zhang, Y.P.; Feres, M. Effectiveness of a pre-procedural mouthwash in reducing bacteria in dental aerosols: Randomized clinical trial. Braz. Oral Res. 2017, 31, e21. [Google Scholar] [CrossRef] [Green Version]
- Veksler, A.E.; Kayrouz, G.A.; Newman, M.G. Reduction of salivary bacteria by pre-procedural rinses with chlorhexidine 0.12%. J. Periodontol. 1991, 62, 649–651. [Google Scholar] [CrossRef]
- Fine, D.H.; Mendieta, C.; Barnett, M.L.; Furgang, D.; Meyers, R.; Olshan, A.; Vincent, J. Efficacy of preprocedural rinsing with an antiseptic in reducing viable bacteria in dental aerosols. J. Periodontol. 1992, 63, 821–824. [Google Scholar] [CrossRef]
- Human Microbiome Project Consortium. A framework for human microbiome research. Nature 2012, 486, 215–221. [Google Scholar] [CrossRef] [Green Version]
- Kroes, I.; Lepp, P.W.; Relman, D.A. Bacterial diversity within the human subgingival crevice. Proc. Natl. Acad. Sci. USA 1999, 96, 14547–14552. [Google Scholar] [CrossRef] [Green Version]
- Aas, J.A.; Paster, B.J.; Stokes, L.N.; Olsen, I.; Dewhirst, F.E. Defining the normal bacterial flora of the oral cavity. J. Clin. Microbiol. 2005, 43, 5721–5732. [Google Scholar] [CrossRef] [Green Version]
- Yoon, J.G.; Yoon, J.; Song, J.Y.; Yoon, S.Y.; Lim, C.S.; Seong, H.; Noh, J.Y.; Cheong, H.J.; Kim, W.J. Clinical significance of a high SARS-CoV-2 viral load in the saliva. J. Korean Med. Sci. 2020, 35, e195. [Google Scholar] [CrossRef]
- Seneviratne, C.J.; Balan, P.; Ko, K.K.K.; Udawatte, N.S.; Lai, D.; Ng, D.H.L.; Venkatachalam, I.; Lim, K.S.; Ling, M.L.; Oon, L.; et al. Efficacy of commercial mouth-rinses on SARS-CoV-2 viral load in saliva: Randomized control trial in Singapore. Infection 2021, 49, 305–311. [Google Scholar] [CrossRef] [PubMed]
- US National Library of Medicine. Povidone-Iodine vs. Essential Oil vs. Tap Water Gargling for COVID-19 Patients (GARGLES), NCT04410159. Available online: https://clinicaltrials.gov/ct2/show/NCT04410159 (accessed on 13 May 2022).
- Garcia-Sanchez, A.; Peña-Cardelles, J.F.; Ordonez-Fernandez, E.; Montero-Alonso, M.; Kewalramani, N.; Salgado-Peralvo, A.O.; Végh, D.; Gargano, A.; Parra, G.; Guerra-Guajardo, L.I.; et al. Povidone-iodine as a pre-procedural mouthwash to reduce the salivary viral load of SARS-CoV-2: A systematic review of randomized controlled trials. Int. J. Environ. Res. Public Health 2022, 19, 2877. [Google Scholar] [CrossRef] [PubMed]
- The Guidelines of Ministry of Heath, Labour and Welfare in Japan. Available online: https://www.mhlw.go.jp/www1/topics/kenko21_11/b5.html (accessed on 9 May 2022).
- Naksagoon, T.; Ohsumi, T.; Takenaka, S.; Nagata, R.; Hasegawa, T.; Maeda, T.; Noiri, Y. Effect of water aging on the anti-biofilm properties of glass ionomer cement containing fluoro-zinc-silicate fillers. Biofouling 2020, 36, 1090–1099. [Google Scholar] [CrossRef] [PubMed]
- Tada, A.; Takeuchi, H.; Shimizu, H.; Tadokoro, K.; Tanaka, K.; Kawamura, K.; Yamaguchi, T.; Egashira, T.; Nomura, Y.; Hanada, N. Quantification of periodontopathic bacteria in saliva using the invader assay. Jpn. J. Infect. Dis. 2012, 65, 415–423. [Google Scholar] [CrossRef] [Green Version]
- Samaranayake, L.P.; Fakhruddin, K.S.; Buranawat, B.; Panduwawala, C. The efficacy of bio-aerosol reducing procedures used in dentistry: A systematic review. Acta Odontol. Scand. 2021, 79, 69–80. [Google Scholar] [CrossRef]
- Horsophonphong, S.; Chestsuttayangkul, Y.; Surarit, R.; Lertsooksawat, W. Efficacy of extraoral suction devices in aerosol and splatter reduction during ultrasonic scaling: A laboratory investigation. J. Dent. Res. Dent. Clin. Dent. Prospect. 2021, 15, 197–202. [Google Scholar] [CrossRef]
- Marui, V.C.; Souto, M.L.S.; Rovai, E.S.; Romito, G.A.; Chambrone, L.; Pannuti, C.M. Efficacy of preprocedural mouthrinses in the reduction of microorganisms in aerosol: A systematic review. J. Am. Dent. Assoc. 2019, 150, 1015–1026.e1. [Google Scholar] [CrossRef]
- Chaudhary, P.; Melkonyan, A.; Meethil, A.; Saraswat, S.; Hall, D.L.; Cottle, J.; Wenzel, M.; Ayouty, N.; Bense, S.; Casanova, F.; et al. Estimating salivary carriage of severe acute respiratory syndrome coronavirus 2 in nonsymptomatic people and efficacy of mouthrinse in reducing viral load: A randomized controlled trial. J. Am. Dent. Assoc. 2021, 152, 903–908. [Google Scholar] [CrossRef]
- Elzein, R.; Abdel-Sater, F.; Fakhreddine, S.; Hanna, P.A.; Feghali, R.; Hamad, H.; Ayoub, F. In vivo evaluation of the virucidal efficacy of chlorhexidine and povidone-iodine mouthwashes against salivary SARS-CoV-2. A randomized-controlled clinical trial. J. Evid. Based Dent. Pract. 2021, 21, 101584. [Google Scholar] [CrossRef]
- Paul, B.; Baiju, R.M.; Raseena, N.B.; Godfrey, P.S.; Shanimole, P.I. Effect of aloe vera as a preprocedural rinse in reducing aerosol contamination during ultrasonic scaling. J. Indian Soc. Periodontol. 2020, 24, 37. [Google Scholar] [CrossRef]
- Logothetis, D.D.; Martinez-Welles, J.M. Reducing bacterial aerosol contamination with a chlorhexidine gluconate pre-rinse. J. Am. Dent. Assoc. 1995, 126, 1634–1639. [Google Scholar] [CrossRef]
- Feres, M.; Figueiredo, L.C.; Faveri, M.; Stewart, B.; de Vizio, W. The effectiveness of a preprocedural mouthrinse containing cetylpyridinium chloride in reducing bacteria in the dental office. J. Am. Dent. Assoc. 2010, 141, 415–422. [Google Scholar] [CrossRef]
- Brookes, Z.L.S.; Belfield, L.A.; Ashworth, A.; Casas-Agustench, P.; Raja, M.; Pollard, A.J.; Bescos, R.J. Effects of chlorhexidine mouthwash on the oral microbiome. J. Dent. 2021, 113, 103768. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takenaka, S.; Sotozono, M.; Yashiro, A.; Saito, R.; Kornsombut, N.; Naksagoon, T.; Nagata, R.; Ida, T.; Edanami, N.; Noiri, Y. Efficacy of Combining an Extraoral High-Volume Evacuator with Preprocedural Mouth Rinsing in Reducing Aerosol Contamination Produced by Ultrasonic Scaling. Int. J. Environ. Res. Public Health 2022, 19, 6048. https://doi.org/10.3390/ijerph19106048
Takenaka S, Sotozono M, Yashiro A, Saito R, Kornsombut N, Naksagoon T, Nagata R, Ida T, Edanami N, Noiri Y. Efficacy of Combining an Extraoral High-Volume Evacuator with Preprocedural Mouth Rinsing in Reducing Aerosol Contamination Produced by Ultrasonic Scaling. International Journal of Environmental Research and Public Health. 2022; 19(10):6048. https://doi.org/10.3390/ijerph19106048
Chicago/Turabian StyleTakenaka, Shoji, Maki Sotozono, Asaka Yashiro, Rui Saito, Niraya Kornsombut, Traithawit Naksagoon, Ryoko Nagata, Takako Ida, Naoki Edanami, and Yuichiro Noiri. 2022. "Efficacy of Combining an Extraoral High-Volume Evacuator with Preprocedural Mouth Rinsing in Reducing Aerosol Contamination Produced by Ultrasonic Scaling" International Journal of Environmental Research and Public Health 19, no. 10: 6048. https://doi.org/10.3390/ijerph19106048