1. Introduction
Musculoskeletal system disorders (MSDs) refer to health problems in the locomotive system; that is, muscles, tendons, skeleton, cartilage, joints, ligaments, blood vessels, and tendons [
1,
2]. MSDs are a set of symptoms and injuries (inflammatory or degenerative) of the musculoskeletal system, and are related to the neck, back, and upper and lower extremities of the body [
3]. MSDs are the most common occupational diseases in industry. They derive from various causes, and are divided into two categories: those caused by acute trauma, such as slips or falls, and those due to repetitive exposure to a type of physical activity, known as cumulative trauma disorders (CTDs), meaning that these injuries develop over time, which can be as long as weeks, months, or even years of propensity to repetitive stress, so that they are not due to a single temporary event, as is the case of the first category, but to various micro-traumas [
1,
2].
When MSDs are caused by work-related issues, they are called work-related musculoskeletal disorders (WMSDs) [
4]. For years, studies have focused on ways to reduce WMSDs. General knowledge of the mechanisms and factors that cause the given ailments, among others, has enabled the development of a series of methods for risk occurrence and identification. WMSDs can be prevented through ergonomic interventions, including optimization of posture and working conditions, muscle and movement training, periodic work breaks, and load-dependent work management, through which the load on the musculoskeletal system can be reduced, thus providing workers with a longer working life [
5].
Workers who suffer from this disorder may experience severe pain, which is reflected in a decrease in productivity and quality of work, and can even cause disability, which causes absenteeism from work and leads to increased costs for businesses and for the public health system [
2]. Pain caused by musculoskeletal disorders is the second leading cause of disability [
6], and, according to the International Labour Organization (ILO), it is estimated that occupational accidents and diseases cause the loss of 4% of the gross domestic product (GDP), or about
$2.8 billion in direct and indirect costs.
MSDs occur in different areas of the body, caused by a variety of different types of tasks. In the upper extremities, such as the fingers, hands, wrists, arms, elbows, shoulders, and neck, MSDs can originate from repetitive or lasting static force, leading to tendinitis or nerve entrapment, such as carpal tunnel syndrome (CTS) [
2,
7,
8,
9]. CTS is due to compression of the median nerve inside the carpal tunnel, while flexor tendinitis causes compression of the median nerve by increased pressure in the carpal tunnel due to edema.
Currently, there are several methods that allow us to detect MSDs. For example, CTS is detected by means of palpation tests, such as the Phalen’s and Tinel’s tests, and electromyography. However, the use of thermal imaging may improve medical diagnosis [
10].
Temperature gradient changes (decrease and increase) on the skin surface or in the middle of the body are indicators of disease, allowing the evaluation of changes in metabolism and blood flow, especially in a superficial layer of the skin [
10,
11,
12,
13,
14,
15]. Several studies indicate that the symmetry of the extremities and torso will not have a temperature difference on the two sides along a dermatome or thermatome of more than 0.30 °C, and of no more than 0.90 °C on the forearms [
16]. The diagnosis of neuromuscular pathology by infrared thermography (IT) is based on the existence of thermal symmetry and asymmetry between normal and abnormal sites [
17,
18]. IT works by measuring the temperature distribution of a surface, which offers several advantages, because it is non-invasive, non-contact, non-radioactive, and painless, and the results are easy to reproduce (thermal imaging); it also has a low operating cost [
10,
19,
20,
21]. A broad range of research has proven the effectiveness of IT in diagnosing CTS [
20,
21].
Nowadays, CTS is a pathology of great interest in medical research, since it represents one of the greatest occupational health problems of any upper limb disorder [
22], and yet, the etiology is not appropriately described [
22,
23].
Epidemiological studies have been undertaken to identify risk factors for CTS, and the results are contradictory. However, the most consistent factors have been being female [
22,
23,
24,
25,
26,
27,
28,
29], thirty years or older [
22,
23,
25,
26,
28,
29,
30,
31,
32,
33,
34,
35,
36], having repetitive motor activity, and having a number of systemic diseases, such as diabetes mellitus [
10], rheumatoid arthritis [
37,
38], and hypothyroidism [
37,
39].
Campillo & De la Vega [
40] developed a predictive model for CTDs by using sensory thermography as the main tool. They sought to determine whether there is a relationship between temperature variability and CTD diagnosis and, at the same time, whether there is a gender difference regarding CTDs. However, the model does not explain the temperature variation over time well. In turn, Márquez Gómez [
41] used traditional methods, such as RULA (Rapid Upper Limb Assessment) and OCRA (Occupational Repetitive Action), in combination with statistical techniques for the selection of significant predictor variables for the development of predictive models. Grieco [
42] reported a logarithmic conversion of the relative exposure (OCRA) and injury indices, with which he constructed a simple linear regression model for risk prediction of WRMSDs. In the same context, Álvarez-Tello et al. [
43] developed a predictive model using binary logistic regression and the items of the strain index questionnaire as predictor variables. The aim of this study is to develop quantitative predictive models that integrate risk factors for CTD, such as age, sex, BMI (body mass index), blood pressure (BP), respiratory rate (RR), and heart rate.
2. Materials and Methods
2.1. Recruitment and Selection of Participants
At first, the target company was approached to explain the purposes of the research and to request approval to apply the project by means of a document expressing the objectives, procedures, and analyses to be carried out, as well as estimated times. Once permission was obtained from the business authorities, the study was initiated based on the clinical procedures established by the company’s occupational health department.
Two production areas were assigned, the sanding and tolex areas, which had the highest records for wrist problems among the operators. In the sanding area, the activities of the operators consist of the sanding process of the body, neck, and edges of the wood product using orbital and edge sanders. On the other hand, in the tolex area, the cabinet subassembly and lining process is performed, which includes the activities of vinyl and fabric cutting, gluing, and stapling. Next, each of the areas was visited to learn about their production processes and to determine the experimental space. Afterwards, a questionnaire was given to each operator (a total of 39 persons), designed to select the participants of the study, obtaining their socio-demographic information and health conditions. This phase had an approximate duration of one month, due to the time restriction so as not to affect the daily production goals of the company.
Twenty-three questionnaires were applied in the sanding area and 16 in the tolex area. At the end of the recruitment process, 19 participants were selected from the sanding area (four persons were not selected due to disabilities and diabetes). Sixteen questionnaires were applied in the tolex area, and 14 participants were chosen (one person did not want to participate and another one had epilepsy). One woman and eighteen men participated in the sanding area (average age = 33 ± 9.7 years). Six women and eight men participated in the tolex area (average age = 35 ± 7.45 years). The experimental sample included a total of 33 people.
Then, the vital signs and somatometry of the chosen participants were recorded, including weight, height, body mass index (BMI), blood pressure (BP), heart rate, and respiratory rate (R.R). The sanding area showed an average BMI = 27 kg/m2, BP 78% normal, 13% high, and 9% low; 96% of the participants were right-handed, had an average heart rate of 77.43 beats per minute (BPM), and an RR of 17.63 breaths per minute. In the tolex area, an average BMI of 28.4 kg/m2, BP 75% normal, 12.5% high, and 12.5% low was recorded. All of the participants in this area were right-handed, and had an average heart rate of 94.18 BPM and an RR of 18.5 breaths per minute.
The selected subjects did not take drugs for the peripheral nervous system (vasodilator, antihypertensive) so as not to interrupt the sympathetic vasoconstrictive response and, therefore, affect their body temperature. Furthermore, they were asked to meet certain criteria in order to take the thermograms listed below. Data collection and thermograms at the company began in February 2019 and ended in June 2019.
A diagram with the measurement methodology appears in
Figure 1.
2.2. Statement of Ethics
This study was conducted in accordance with the written consent granted by the company, which was provided verbally to all participants. The protocol was reviewed and approved by the ethics and bioethics committee of the postgraduate department of the Faculty of Engineering, Architecture, and Design of the Autonomous University of Baja California, according to the NOM-035-STPS-2018 Standard.
2.3. Preliminary Restrictions
Prior to taking the thermograms and in order to eliminate uncertainties in temperature measurements, the following restrictions were imposed on participants, based on the protocols of Glamorgan [
44], Standard Procedures for Infrared Imaging in Medicine [
45], and Design and Application of a Protocol for Acquiring and Processing Infrared Images from the Hands [
46].
Not to smoke in the hours prior to taking the images (12 hours).
Not to drink alcoholic beverages in the hours prior to the exam (12 hours).
Not to drink coffee or tea for several hours before the study (12 hours).
Preferably, not to eat fatty foods before the analysis.
2.4. Experimental Protocol
2.4.1. Environmental Conditions for the Study
To avoid vasomotion phenomena, the controlled temperature of the rooms assigned by each area was kept between 23–24 °C (+/−1 °C). Regarding humidity, its values oscillated between 50–60%, depending on the weather conditions of the region. On days when the humidity of the environment was high, a dehumidifier was required to reduce it to adequate levels. Within the space allocated for the recordings, air drafts on the subjects’ hands and lamps or domes above them were avoided during the taking of the thermal images. The participants were asked to uncover their forearm (if necessary), not to wear bracelets, rings, or wristbands, and to remove earrings, glasses, and caps.
2.4.2. Thermographic Infrared Camera Implementation
The IT camera used in this study was a FLIR ThermaCAM
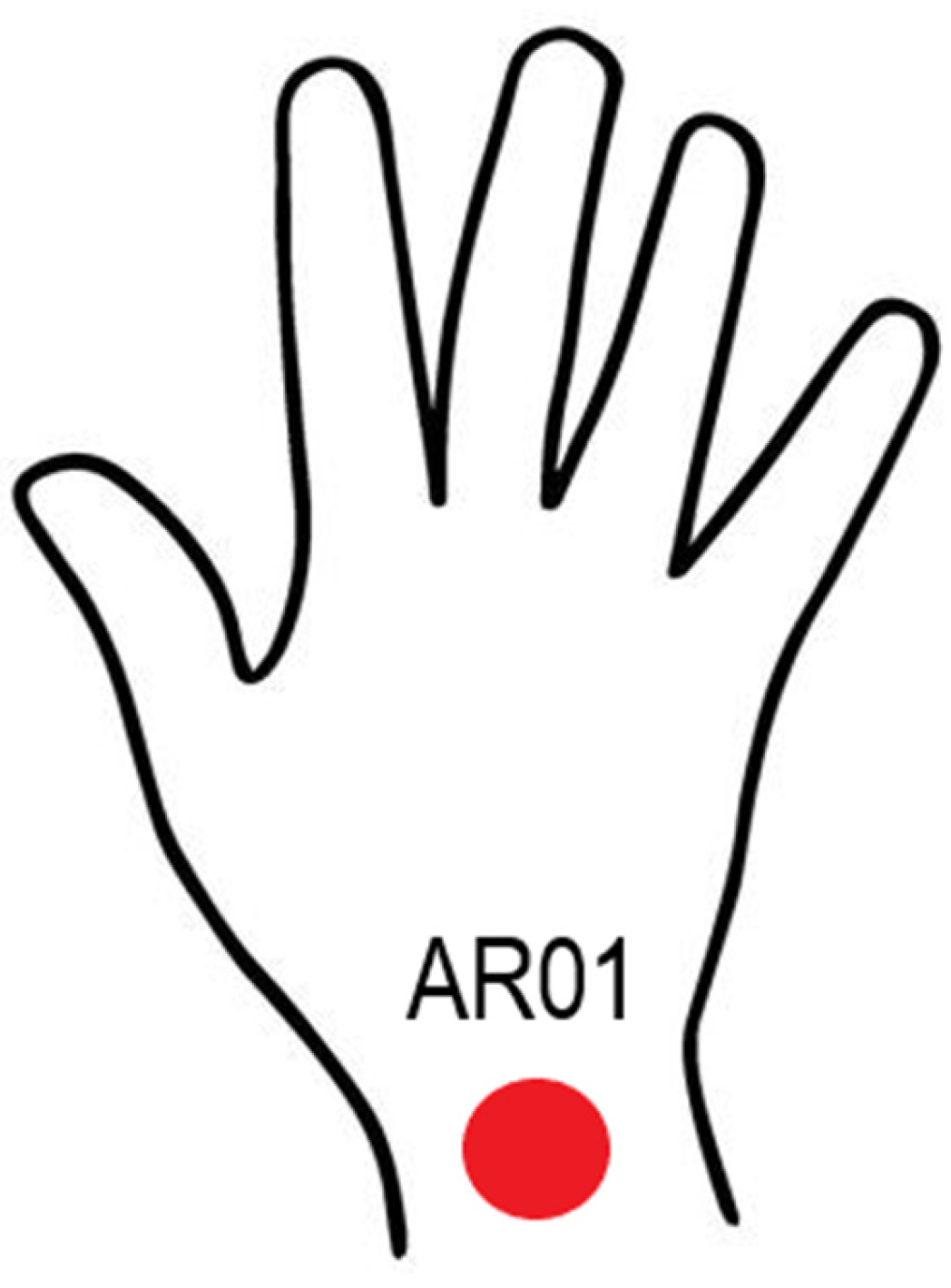
TM E25 model, fabricated by FLIR Systems at Boston, MA, USA, with a resolution of 160 × 120 pixels, an accuracy of ±2 °C/±3.6 °C for ±2% of reading, and a spectral range of 7.5–13 μm. The camera was mounted on a tripod for better handling, with an emissivity of 0.98, as this is the average emissivity of human skin, and thus avoids errors in temperature measurement. Each time the infrared camera was used, the emissivity was set to this value. The chosen region (
Figure 2) was taken for all participants. Before each shot, the camera was kept turned on for 15 minutes to maintain thermal equilibrium with its surroundings. The camera was placed perpendicular to the subject’s hand at a minimum distance of 0.601 m [
46]. For this study, a distance of two meters was considered. It is worth mentioning that a black surface was placed as a background for the image, contributing to the improvement of the reading of the thermograms and reducing the surrounding noise.
2.4.3. Handling of the Participants
Prior to the start of the test, each participant was checked for compliance with the requirements, that is, no caffeine, alcohol, vasodilator drugs, or smoking, to continue with the tests. For this purpose, they were given a reminder the day before the tests were to take place. The female menstrual cycle was considered. Nevertheless, none of the participants had their menstrual period during the intakes.
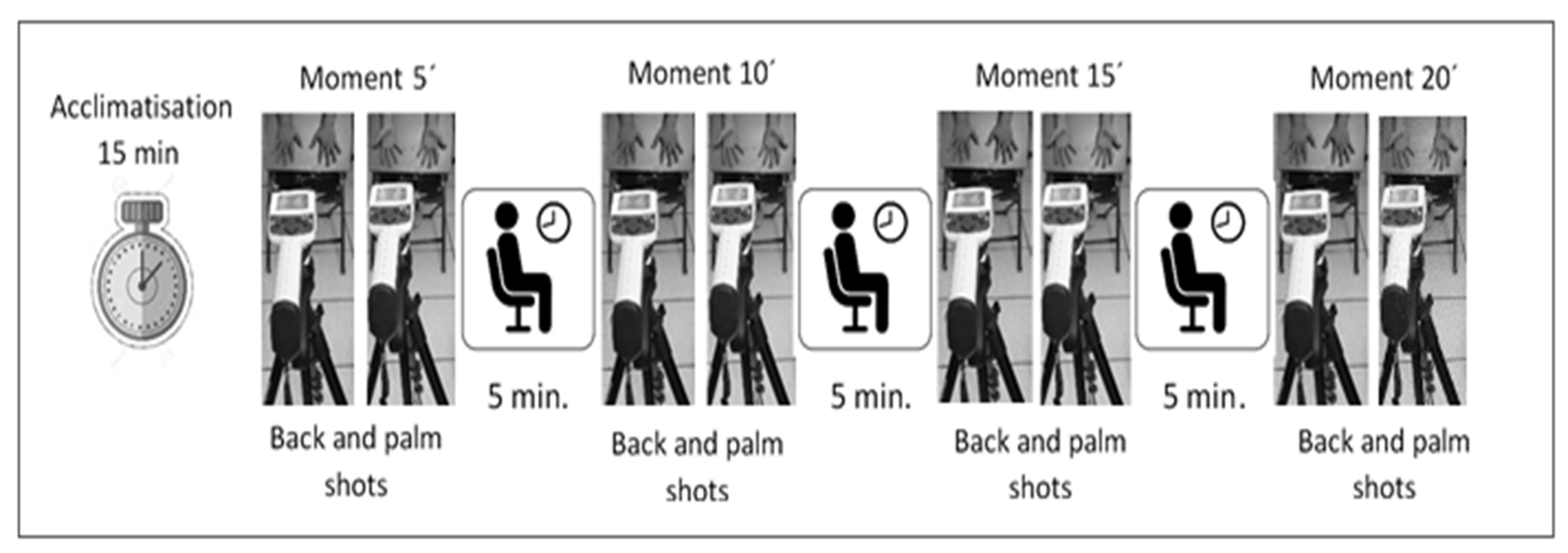
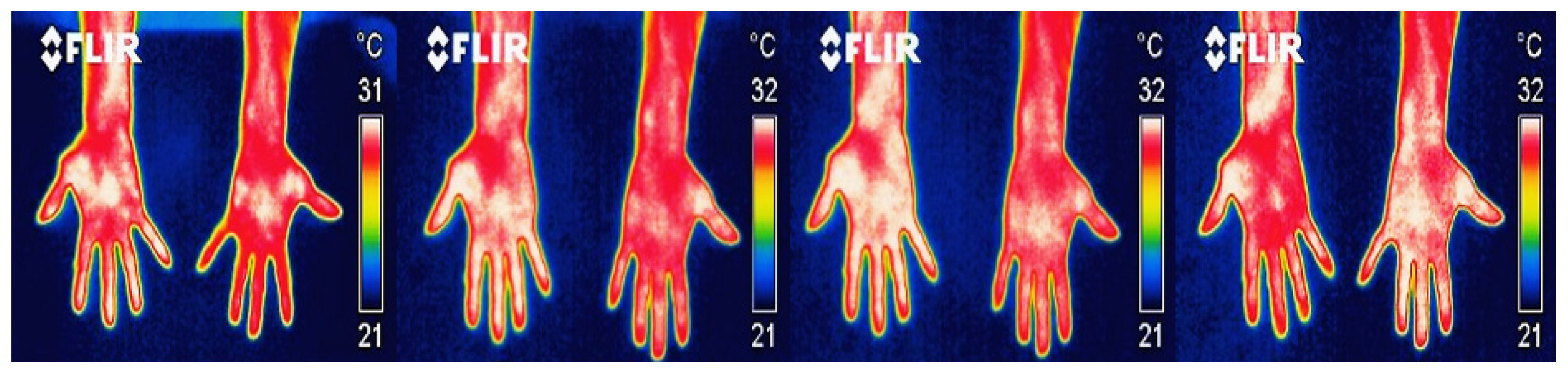
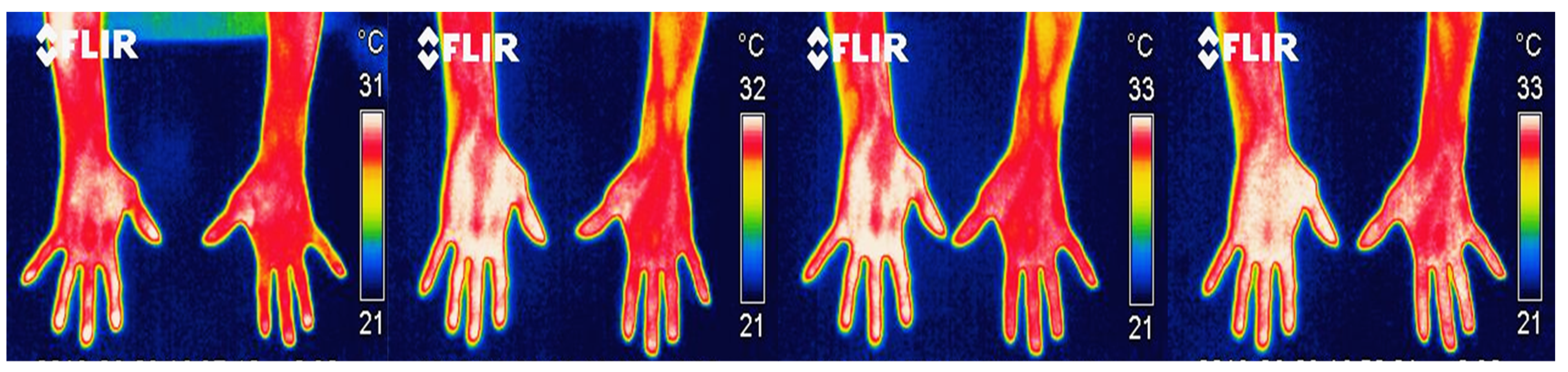
Afterwards, a black board formed of foil wood with plastic laminate was placed on the chair, on which the shots were taken of the palms and backs of the hands. This board had tape markers, which worked as guides to provide precise and reproducible positioning of the hands. Each participant was instructed not to touch the board directly to prevent hand heat from being retained on the board and causing noise on the thermograms. The participant was asked to position him/herself behind the chair and bend down a little until his/her fingers were positioned over the marks. Then, a sequence of infrared images was taken, spaced every 5 min at times 5, 10, 15, and 20 (based on Vardasca, R., E. Francis, J. Ring, P. Plassmann, C.D. Jones, and J. Gabriel [
47], and García, A. [
48]) for each participant (
Figure 3). After each thermal image of the palms and back of the hands was taken, the participant waited seated in another chair, while five minutes remained to continue with the next shot, until the four moments were completed. Thermal imaging sessions were held Monday through Friday from 3:30 to 4:30 pm (hours established by the company), with three participants per day.
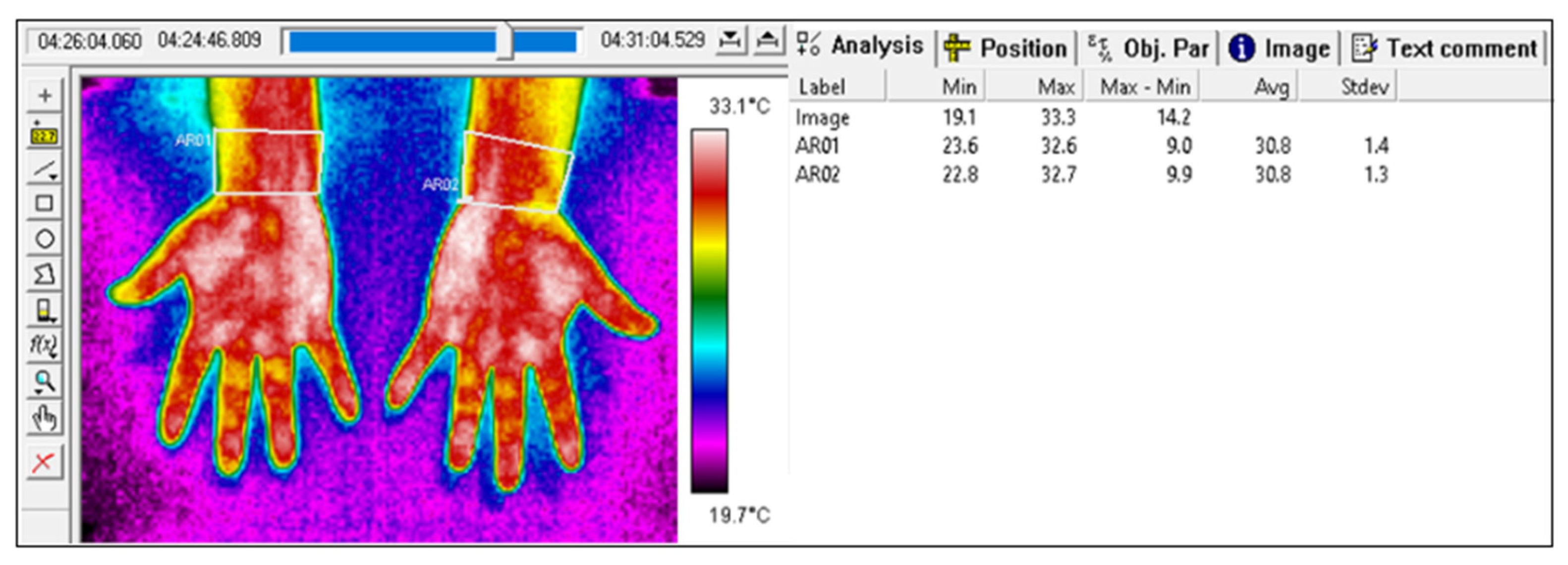
The thermal images were then downloaded and analyzed through the ThermaCAM Researcher Pro 2.10 software, from FLIR Systems company, located at Boston, MA, USA, with which a total of 264 images were reviewed. When analyzing each IT image, the color palette was configured in the rain option. The emissivity (0.98) was already adjusted during the shots. The IR image was delimited according to the ROI in order to measure the temperature in that area. Then, the Results option was activated to display the temperature values of maximum, minimum, max-min, average, and standard deviation (
Figure 4).
Next, the data were exported to Excel to organize and group according to the times in which the temperatures were recorded (5′, 10′, 15′, and 20′). Afterwards, the temperature differences were calculated for the minimum and maximum values of the temperature captured by the thermographic camera. Thereafter, the thermal asymmetries that could represent a possible injury were identified and classified in their levels of alarm and severity, as established by Marins et al. [
49], and as shown in
Table 1.
Subsequently, an OCRA evaluation was performed in the two study areas to compare the results with the proposed model.
2.4.4. Statistical Analysis
For the analysis process of the acquired data, the study factors were grouped together. Age was grouped in young age (<40 years of age) and mature age (≥40 years old), and for gender, value 1 was assigned to male and 0 to female; BMI was classified as non-obese (<30 kg/m2) and obese (≥30 kg/m2). BP was classified in normal, high, and low, with normal and high heart rate, and RR in normal and high. Value 1 was assigned to subjects who had an injury or discomfort, and 0 to participants with no injuries.
The statistical analyses were carried out in IBM SPSS Statistics v.25
® software, from IBM Corp at Armonk, NY, USA, with which the data normality tests were performed using the Shapiro–Wilk test. Once the normal and non-normal data were identified, non-parametric tests were performed (Mann–Whitney), which were applied to all data due to the small sample size [
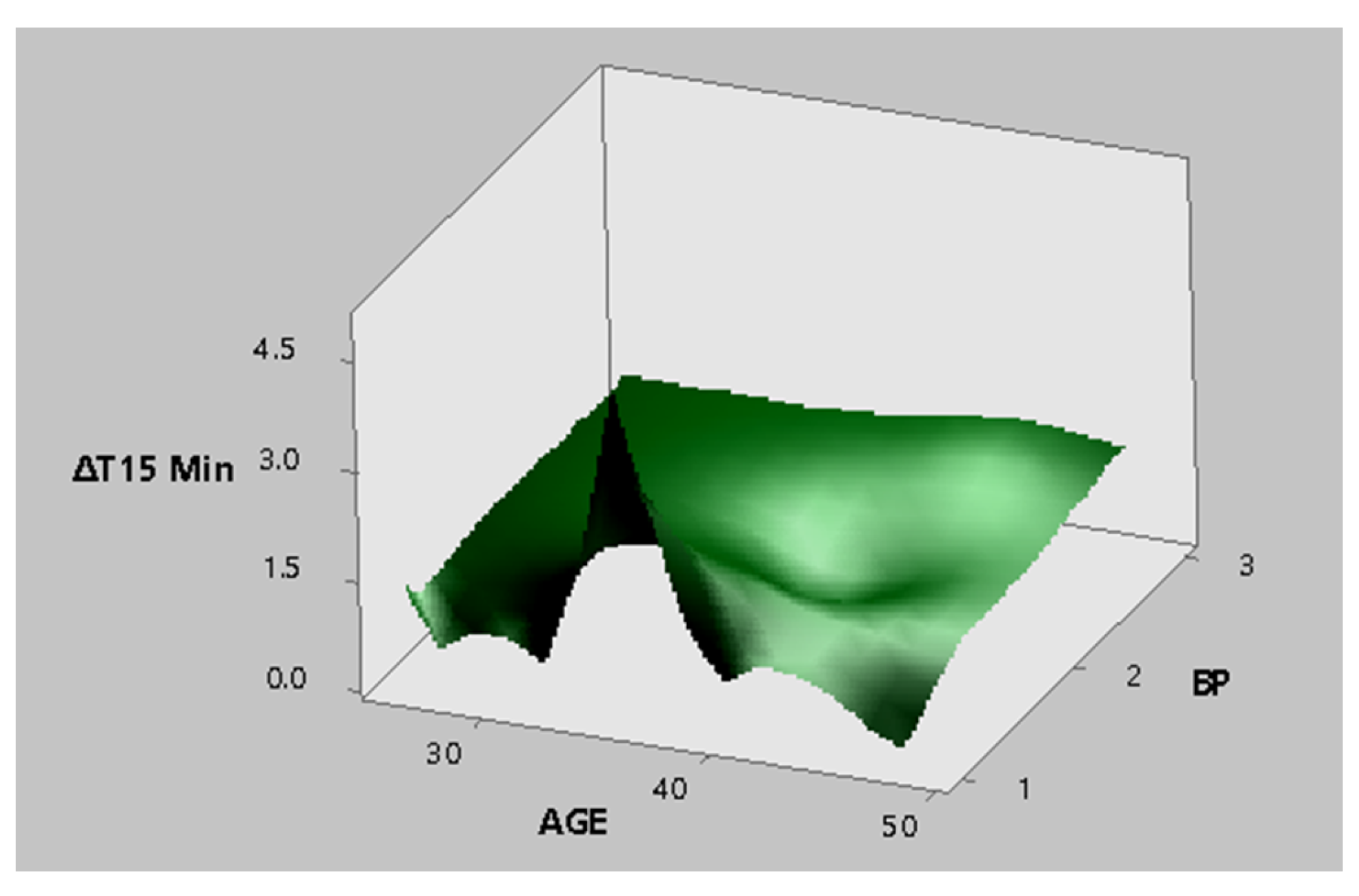
50]. The relationship of the influence of the factors with the temperature differences was determined. Mixed-design analysis of variance was used to identify significant factors. Regression models and response surfaces were generated by Minitab 17. Three types of regression models were constructed using (a) study factors (age, gender, BMI, BP, RR, and heart rate), (b) relevant risk factors in OCRA (recovery factor, strength factor, posture and movement factor, and frequency factor), and (c) all of the above. The differences obtained with
p < 0.05 were considered statistically significant with a 95% confidence interval.
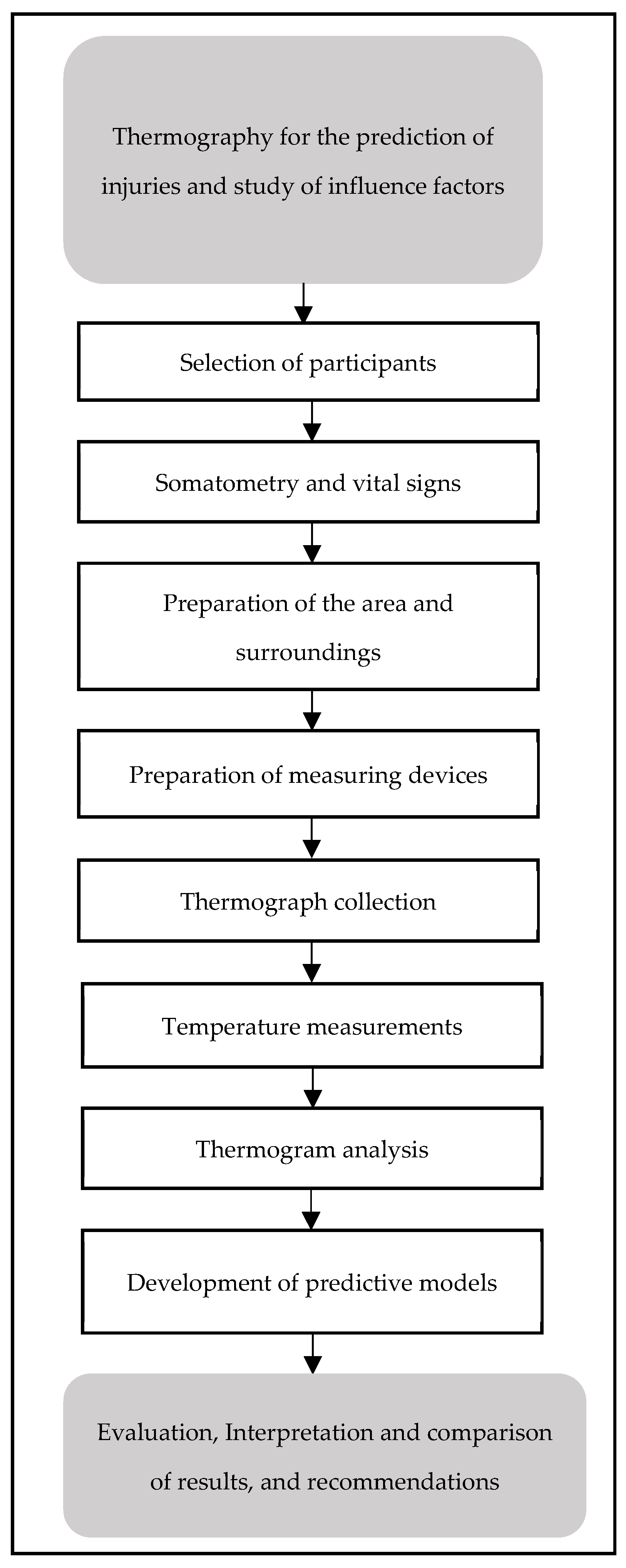
The following flow chart summarizes the procedure carried out to obtain thermal images, up to the generation of the prediction models.
4. Discussions
In this study, 75% of the cases that indicated injury or discomfort were detected by IT in the sanding area, while in the tolex area, just one case was reported. In addition, Papež et al. [
53] and Papež, B., Jesenšek, M. Palfy, M. Mertik and Z. Turk [
54] established that IT allows the correct classification of 72.2% of the hands, healthy and pathological, based on the dorsal part of the hand, while when seriously affected hands and healthy hands are evaluated, the percentage rises to >80%. Palfy and Papez [
55] used 44 thermograms of healthy and pathological hands to determine the effectiveness of IT as a diagnostic method for CTS. Using IT and intelligence systems, they were able to diagnose cases of CTS with a success rate close to or above 80%.
Tkáčová et al. [
20] recorded 14 thermal images to determine the level of effectiveness of IT for diagnosing CTS. The success rates found in the classification of healthy and pathological hands for were close to 80%. In the same context, Tchou et al. [
56] recorded 122 thermograms, and obtained success rates for the classification of healthy hands with CTS pathologies close to or higher than 80%.
Therefore, IT has been shown to be remarkably effective in detecting asymmetries, which are known to be disease indicators, particularly CTS. However, our research detected asymmetries in the dorsal and palmar surfaces of the hand, contrary to other studies [
20,
21,
53,
54,
55,
56], who concluded that the dorsal side of the hand provides more satisfactory results when diagnosing CTS than the palmar area of the hand.
Ninety percent of the participants from the sanding area exhibited asymmetries with alert or serious attention. Out of the 17 subjects with asymmetries, 76% exhibited levels outside the normal range in at least one of the study factors (age, BMI, BP, heart rate, or RR), while 79% of the participants from the tolex area exhibited asymmetries with alert or serious levels. Out of the 11 subjects with asymmetries, 73% had levels outside the normal range in at least one of the study factors.
As for the sanding area, 94% of the participants with asymmetries are men (with less than one year working in the area), and the other 6% is the only female operator in the area. Regarding the tolex area, 36% of the participants with asymmetries are women, while 64% are men (the subjects have been working in the area for two to eight years.) It should be inferred that the sanding area would have a higher percentage of injuries, due to the fact that the production activities that are carried out demand more movement for the wrists than for the tolex area.
Moreover, other hypotheses are based on the production rate that has been increasing by 50%, leading to faster movements in the wrists, thus hurting them. Given that seven out of eight people with injuries from the sanding area have been working there for such a short time (less than a year), this is alarming. In fact, one operator who had been working in the area for only six months was disabled due to tendinitis during the study; this was contrary for the participants from the tolex area who have been working there for two to eight years. Another participant was also diagnosed with tendinitis, although it was not detected by IT.
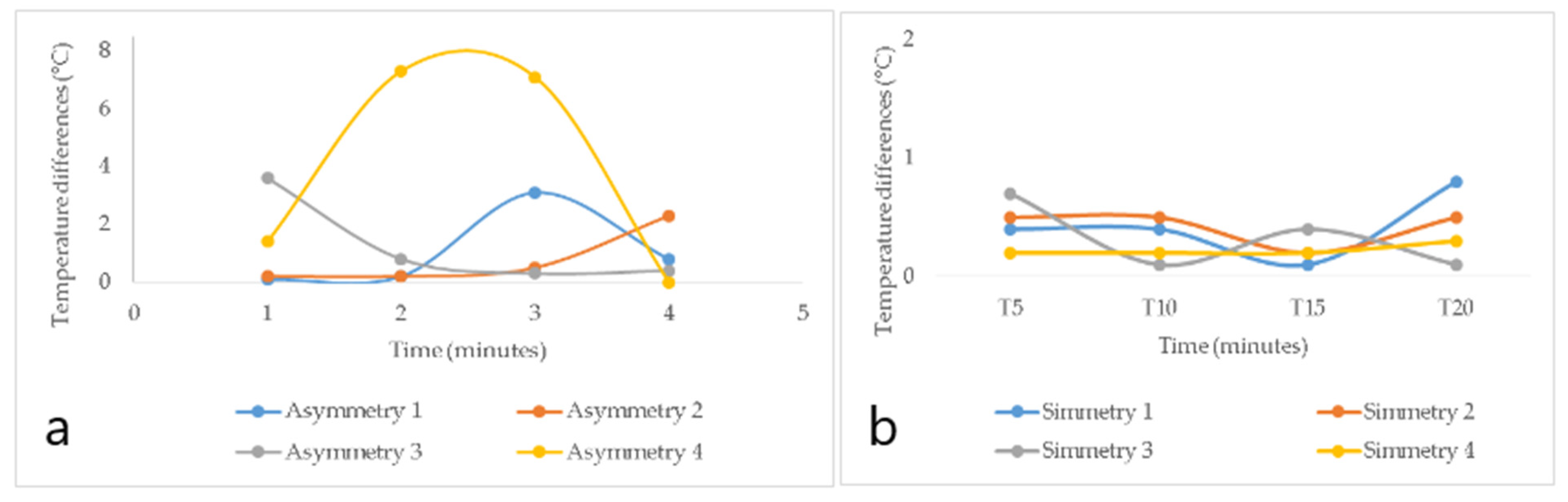
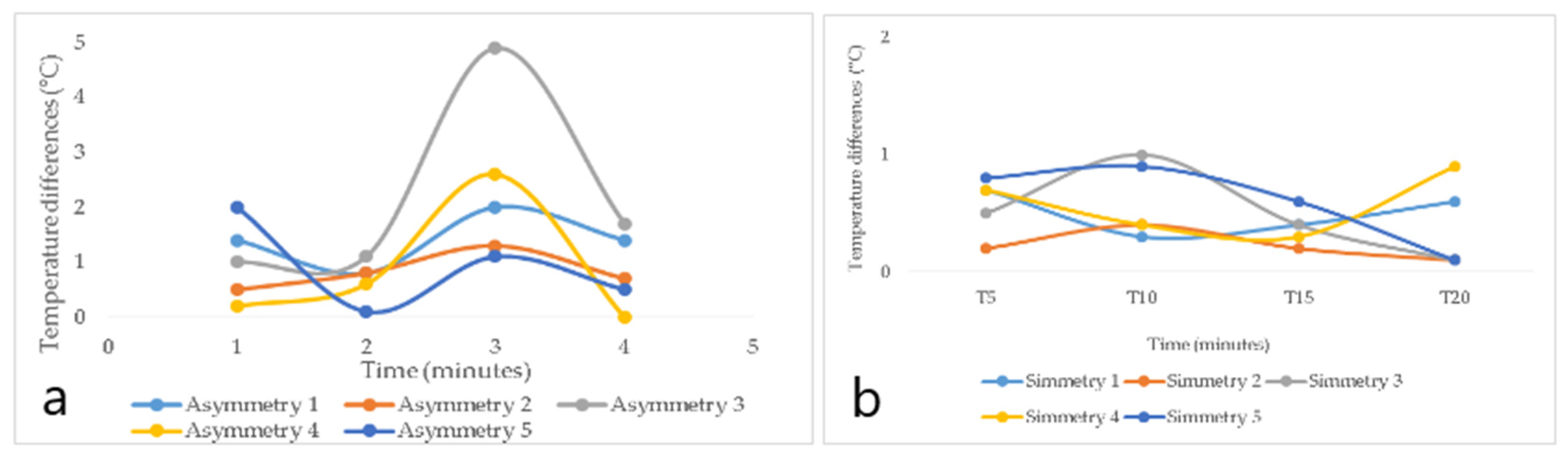
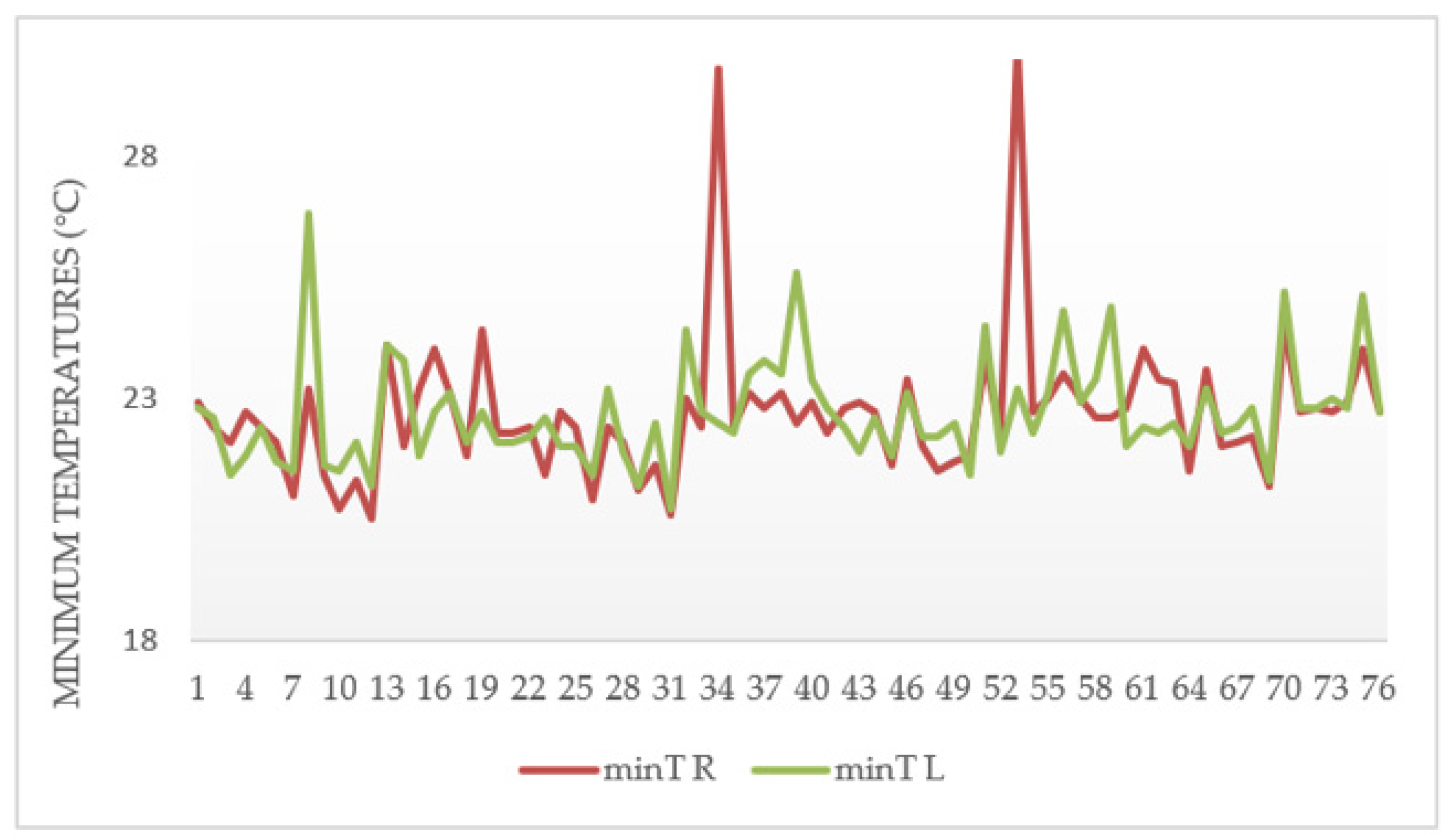
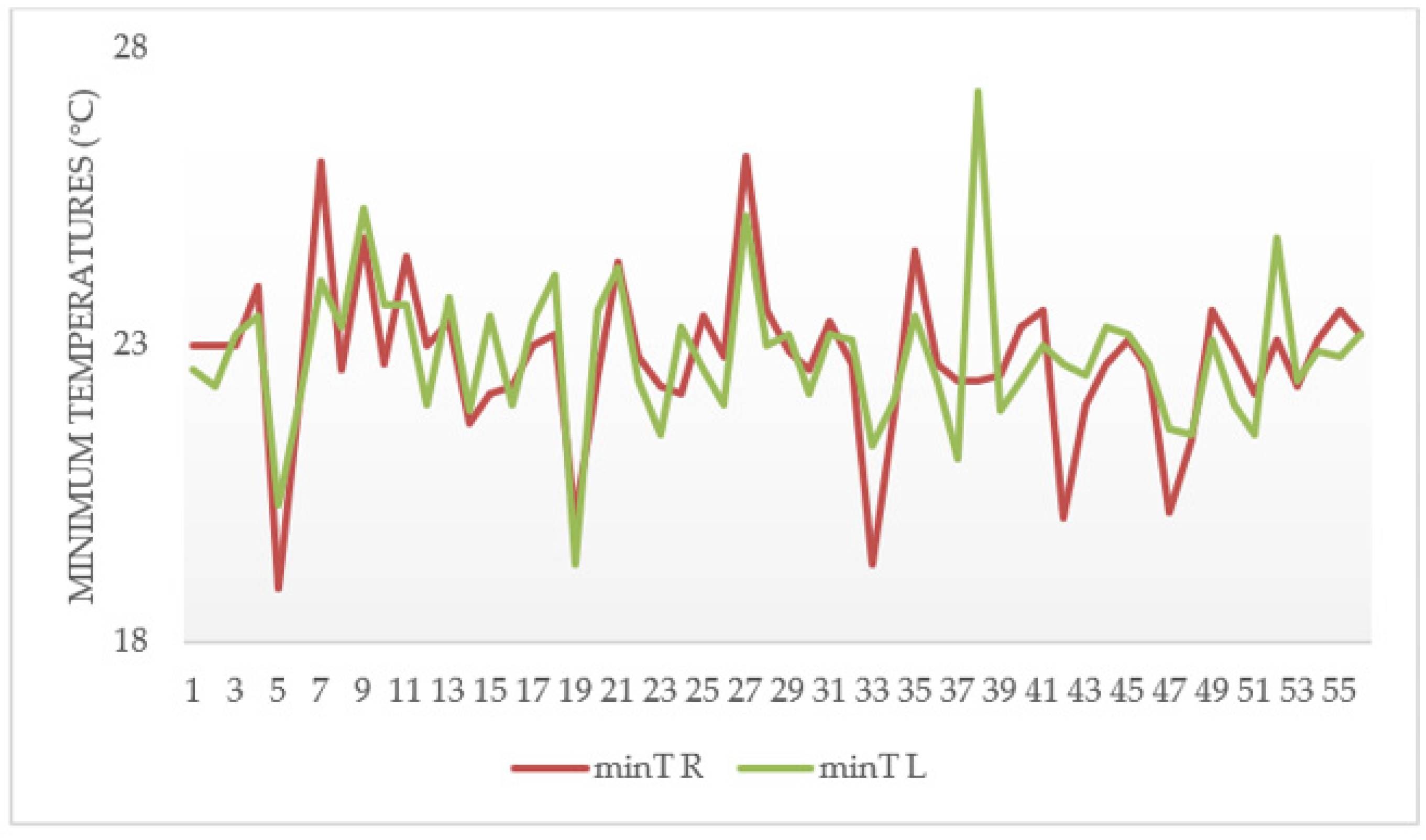
By analyzing the behavior of the minimum and maximum temperature differences by time, the highest value of 6.5 °C (temperature difference between the back of the right and left hand) was identified for the sanding area in the minimum temperature values, in a time of 15 min for the back of the hand section. For the tolex area, the minimum temperature differences with the highest value on the back of the hand were shown in time 10′ (2.6 °C). For the maximum temperature differences, the highest value (1.6 °C) was recorded at time 15′. In the palms section, its maximum value in the sanding area was 7.3 °C for the minimum temperature difference between the right and left palm, recorded in time 10′. In the case of the tolex area, for the palmar region of the hand, the highest value was in time 15′with 5 °C for the minimum temperature difference. On the other hand, for the maximum temperature difference, its highest value was 1.1 °C in time 20′.
The factors age, BMI, heart rate, and RR have data with a normal distribution, whereas the factors gender, dominant hand, and BP exhibited abnormal distribution for the sanding area. In the tolex area, normality tests identified age and BMI as data with normal distribution, and the factors gender, BP, injury, heart rate, and RR exhibited abnormal distribution.
When carrying out the non-parametric tests for the back of the hand, the influence of the BP on the maximum temperature difference in time 10′ for the sanding area was verified. The relationship between the minimum temperature differences and BP for the palmar section of the hand was identified in time 10; heart rate in times 10′and 15′; and finally, RR in the minimum temperature difference in time 20′. An influence relationship between RR and the maximum temperature differences for the section of the back of the hand was found in time 15′. As for the tolex area, an influence relationship between RR and the maximum temperature differences for the back section of the hand was found in time 15′. There was no influence relationship for the palmar region of the hand.
The factors that influence the minimum temperature differences on the back of the hand for the sanding area are BP in time 15′, heart rate in times 10′ and 15′, and RR in time 20′. A relationship with BP in time 10′ was identified for the maximum temperature differences.
Regarding the non-parametric tests in the tolex area, in the section of the back of the hand, an influence relationship was found between RR and the maximum temperature differences in time 15′. In the palmar section of the hand, an influence was identified between age and the minimum temperature differences in time 10′. Concerning the factors that influence the minimum temperature differences in the palm of the hand for the sanding area, these are BP in time 10′, heart rate in times 10′ and 15′, and RR in time 20′.
The results indicate that the interaction between the significant factors for the sanding area and the main asymmetries had a low BP. On the other hand, in the tolex area, 80% of the asymmetries had normal BP. With regard to heart rate, for the palm of the hand in the sanding area, one out of three asymmetries were observed with a high heart rate (the highest value) for time 10′, while in time 15′, two out of three asymmetries exhibited a high heart rate. In the tolex area, 80% of the asymmetries included normal heart rhythms. For the RR, both areas were found to have normal RR for the diagnosed asymmetries. Regarding age, in the tolex area, 100% were young, both for time 10′. In contrast, other research [
23,
30,
32,
35] established that CTS increases with age, while several studies establish that age is associated with the prevalence of CTS [
22,
31,
33,
57].
In the area of sanding, it was not possible to evaluate the gender factor, since there is only one woman in this section. However, various studies [
22,
24,
29,
30,
35] found an association between CTS and the female gender. However, there is also research that found no relationship between gender and CTS [
27]. In the present study, BMI was not determined to be a significant risk factor, whereas other studies have found a strong association with CTS [
22,
30,
33,
35,
57,
58,
59,
60,
61].
When carrying out the mixed-design analysis of variance for the sanding area, BP and heart rate turned out to be significant factors for the back and palm. Based on the mixed-design analysis of variance, for the tolex area, factors were determined to be non-significant. The regression models developed with the study factors obtained a coefficient of determination of 0.9737 for the sanding palm area, and a coefficient of determination of 0.9667 for the tolex palm area. It is worth mentioning that, to attain these percentages, all of the study factors are included in the equations, since omitting them would considerably reduce the determination coefficients.
On the other hand, the models constructed using the OCRA method generated lower coefficients of determination. For sanding palm, R
2 = 0.5854 and for tolex palm, R
2 = 0.3481. However, when both groups of factors were integrated into a single regression model, the best results were obtained with the following coefficients of determination: 0.9850 for sanding palm and 0.9871 for tolex palm. Meanwhile, research conducted by Márquez Gómez, M. [
41] achieved an accuracy of 83.91% and a kappa index of 63.14% in their statistical model for the prediction of WRMSD-related (work-related musculoskeletal disorders) discomfort in the hands/wrists, in which they considered six factors: postural overload, repetitiveness of movements, gender, medical history related to MSD, frequency of household chores, and job rotation. In another study, multiple regression models were developed to predict the combined frequency and severity of the pain from WRMSDs, achieving an R-squared of 32.9% [
62]. In addition, Sasikumar, V. and S. Binoosh [
63] employed various machine learning algorithms in their predictive model for WRMSDs among computer professionals, considering postural, physiological, and work-related factors, with an accuracy of 81.25%.
6. Conclusions
This research proved the effectiveness of IT in the detection of suspected CTS injuries by means of thermal asymmetries in the wrists. Three temperature prediction models were developed based on the study factors, two for the sanding area, with which it is possible to make predictions of the temperature differences for times of 10 and 15 min to determine whether or not the subject exhibits thermal asymmetries that could lead to injury, and another for the tolex area, with predictions for times of 15 min. The maximum thermal asymmetries were registered for the minimum temperature differences, both in the sections of the back of the hand and in the palm of the hand in both study areas.
Ninety-four percent of the participants in the sanding area had thermal asymmetries with a degree of alert or seriousness attention, while for the tolex area, only 73 percent had them. In the tolex area, 36% of the participants with thermal asymmetries with a degree of alert or seriousness attention are women, while 64% are men. The subjects have been working in this area from two to eight years. In the area of sanding, 94% of the participants with asymmetries (alert or seriousness level) are men, and have been working in the area for less than one year.
Factors such as age, BP, heart rate, and RR were found to highly influence injuries in participants. However, no strong association with BMI was found. It is inferred that participants who exhibit levels out of the normal range for at least one of the factors, such as advanced age (≥40 years), BMI, BP, heart rate, or RR, are highly likely to have wrist injuries with a level of attention that is alarming or serious, so it is important to follow up with staff who exhibit such characteristics and consider these results during the recruitment process. In this study, in sanding area, the RR factor stands out, with a high level in personnel with thermal asymmetries of alert or seriousness, while for the tolex area, advanced age predominates.
Finally, these are preliminary results from a limited number of thermal images, so in the next section proposals are made that include increasing the sample size.


 ,
, 


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}