
Effectiveness of Epidemic Preventive Policies and Hospital Strategies in Combating COVID-19 Outbreak in Taiwan


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Data Sources
2.3. Study Population
2.4. Statistical Analysis
3. Results
3.1. Epidemiology
3.1.1. Demographic and Clinical Characteristics of Confirmed Cases
3.1.2. Clinical Outcomes
3.1.3. Fatality
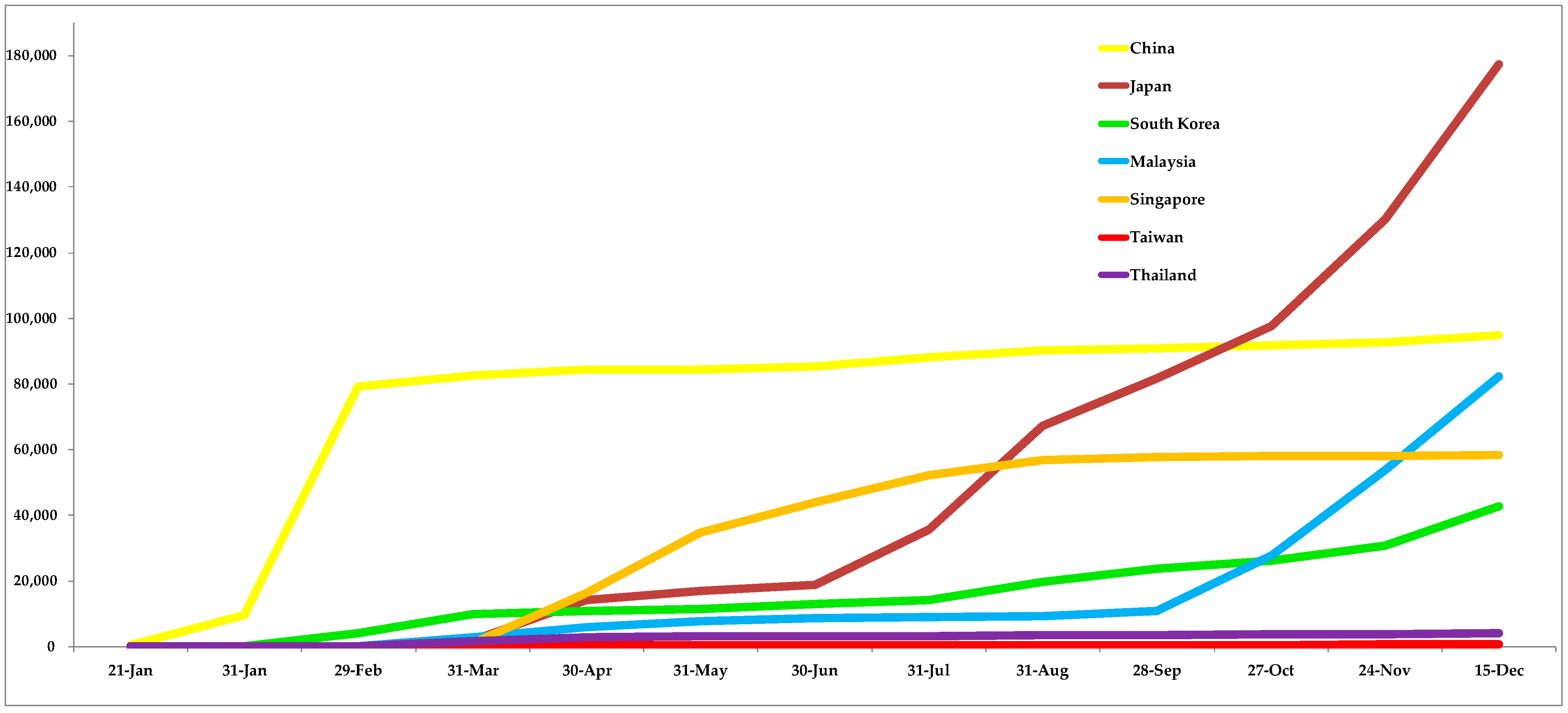
3.1.4. COVID-19 Incidence Rate, Mortality Rate, and Testing Rate of Taiwan and Neighboring Countries with Risk Ratios of Neighboring Countries
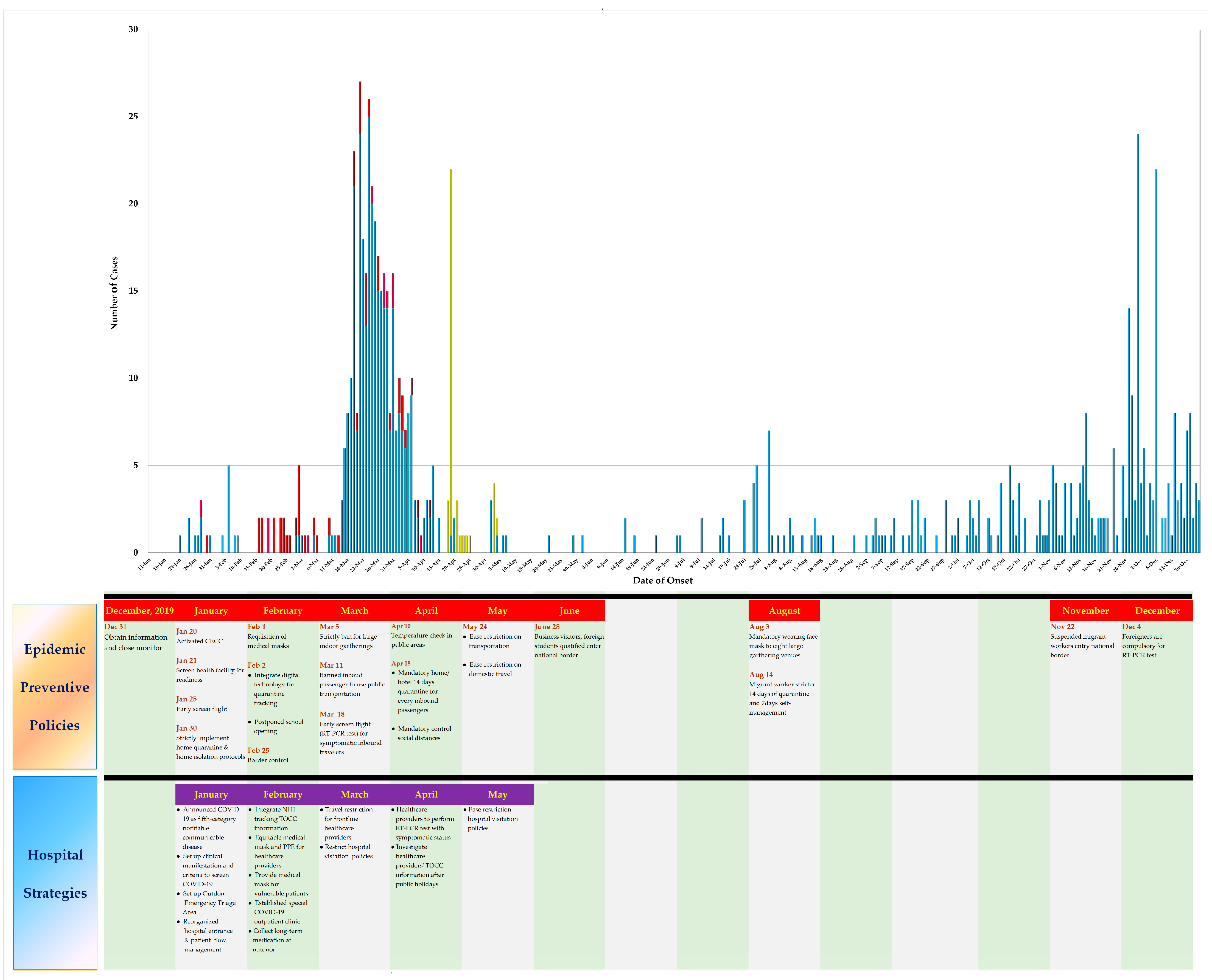
3.2. Summary of the COVID-19 Epidemic Status in Taiwan
3.3. Epidemic Preventive Policies and Hospital Strategies Implemented in Taiwan
3.3.1. Early Response and Centralized Central Epidemic Command Center (CECC) Professionalism
3.3.2. Knowledge and Awareness
3.3.3. Precautionary Measures
3.3.4. Big Data Analytic Tracking System for Case Identification and Large-Scale Surveillance
3.3.5. Border Control and Border Quarantine Measures
3.3.6. Social Distancing Measures
3.3.7. Healthcare Facilities Provisions and Medical Team Preparations
3.3.8. Restrictions for Foreign Migrant Workers
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Ethics Approval and Consent to Participate
References
- Deng, S.-Q.; Peng, H.-J. Characteristics of and Public Health Responses to the Coronavirus Disease 2019 Outbreak in China. J. Clin. Med. 2020, 9, 575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). Available online: https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf (accessed on 5 May 2020).
- McDonald, J. Taiwan News. China Trade Slumps as Anti-Virus Controls Close Factories. Available online: https://www.taiwannews.com.tw/en/news/3892150 (accessed on 26 May 2020).
- Pan, T.; Yeh, J. Taiwan News. Number of Taiwanese Working in China Hits 10-Year Low. Available online: https://www.taiwannews.com.tw/en/news/3839550 (accessed on 27 May 2020).
- News Release. Directorate General of the Budget and Accounting. Statistics on the Number of Chinese People Working Overseas in 2018. Available online: https://www.dgbas.gov.tw/public/Attachment/91217104242H1AK10HM.pdf (accessed on 27 May 2020). (In Chinese)
- Ministry of Transportation and Communications of Taiwan. Outbound Departures of Nationals of the Republic of China by Destination January 2020. Available online: https://admin.taiwan.net.tw/FileUploadCategoryListC003330.aspx?CategoryID=5d16abba-e4d6-4498-8928-d391c7c7e28a&Year=2020&appname=FileUploadCategoryListC003330 (accessed on 27 May 2020).
- World Health Organization. Weekly Epidemiological Update-22 December 2020. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update---22-december-2020 (accessed on 24 December 2020).
- Reported Cases and Deaths by Country, Territory, or Conveyance. In Coronavirus Worldometer. Available online: https://www.worldometers.info/coronavirus/ (accessed on 25 December 2020).
- Taiwan Centers for Disease Control. COVID-19 (SARS-CoV-2 Infection). Available online: https://sites.google.com/cdc.gov.tw/2019ncov/global (accessed on 30 May 2020).
- Taiwan Centers for Disease Control. CECC Confirms 3 more COVID-19 Cases; Two Are Colleagues of Case #760, and One Arrives in Taiwan from Indonesia. Published 20 December 2020. Available online: https://www.cdc.gov.tw/En/Bulletin/Detail/hQPRmEsFm8ASL0NGWr4Gxg?typeid=158 (accessed on 24 December 2020).
- Taiwan Centers for Disease Control. Preparedness and Contingency Planning in Response to COVID-19 Epidemic. Published 28 February 2020. Available online: https://www.cdc.gov.tw/File/Get/JFnBQLuyGNcuROKLUMjuhA (accessed on 30 May 2020).
- Kao, H.Y.; Ko, H.Y.; Guo, P.; Chen, C.H.; Chou, S.M. Taiwan’s Experience in Hospital Preparedness and Response for Emerging Infectious Diseases. Health Secur. 2017, 15, 175–184. [Google Scholar] [CrossRef]
- Hellewell, J.; Abbott, S.; Gimma, A.; Bosse, N.I.; Jarvis, C.I.; Russell, T.W.; Munday, J.D.; Kucharski, A.J.; Edmunds, W.J.; Sun, F. Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts. Lancet Glob. Health 2020, 8, e488–e496. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.-M.; Jyan, H.-W.; Chien, S.-C.; Jen, H.-H.; Hsu, C.-Y.; Lee, P.-C.; Lee, C.-F.; Yang, Y.-T.; Chen, M.-Y.; Chen, L.-S.; et al. Containing COVID-19 Among 627,386 Persons in Contact with the Diamond Princess Cruise Ship Passengers Who Disembarked in Taiwan: Big Data Analytics. J. Med. Internet Res. 2020, 22, e19540. [Google Scholar] [CrossRef] [PubMed]
- Cheng, H.-Y.; Jian, S.-W.; Liu, D.-P.; Ng, T.-C.; Huang, W.-T.; Lin, H.-H. Contact Tracing Assessment of COVID-19 Transmission Dynamics in Taiwan and Risk at Different Exposure Periods Before and After Symptom Onset. JAMA Intern. Med. 2020, 180, 1156–1163. [Google Scholar] [CrossRef] [PubMed]
- Zou, L.; Ruan, F.; Huang, M.; Liang, L.; Huang, H.; Hong, Z.; Yu, J.; Kang, M.; Song, Y.; Xia, J.; et al. SARS-CoV-2 viral load inupper respiratory specimens of infected patients. N. Engl. J. Med. 2020, 382, 1177–1179. [Google Scholar] [CrossRef] [PubMed]
- Wells, C.R.; Sah, P.; Moghadas, S.M.; Pandey, A.; Shoukat, A.; Wang, Y.; Wang, Z.; Meyers, L.A.; Singer, B.H.; Galvani, A.P. Impact of international travel and border control measures on the global spread of the novel 2019 coronavirus outbreak. Proc. Natl. Acad. Sci. USA 2020, 117, 7504–7509. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, C.J.; Ng, C.Y.; Brook, R.H. Response to COVID-19 in Taiwan: Big Data Analytics, New Technology, and Proactive Testing. JAMA 2020, 323, 1341–1342. [Google Scholar] [CrossRef]
- Klinkenberg, D.; Fraser, C.; Heesterbeek, H. The Effectiveness of Contact Tracing in Emerging Epidemics. PLoS ONE 2006, 1, e12. [Google Scholar] [CrossRef]
- Peak, C.M.; Childs, L.M.; Grad, Y.H.; Buckee, C.O. Comparing nonpharmaceutical interventions for containing emerging epidemics. Proc. Natl. Acad. Sci. USA 2017, 114, 4023–4028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Health Insurance Administration Ministry of Health and Welfare. National Health Insurance in Taiwan. Available online: https://www.nhi.gov.tw/Resource/webdata/Attach_15545_1_NHI%20profile.pdf (accessed on 31 May 2020).
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China. JAMA 2020, 323, 1239. [Google Scholar] [CrossRef]
- The Star. Thailand’s Songkran Festival Events Cancelled to Avoid Mass Gatherings on COVID-19 Spread. Published on 20 April 2020. Available online: https://www.malaysiatoday.net/2020/03/07/thailands-songkran-festival-events-cancelledto-avoid-mass-gatherings-on-covid-19-spread/ (accessed on 25 December 2020).
- Tashiro, A.; Shaw, R. COVID-19 Pandemic Response in Japan: What Is behind the Initial Flattening of the Curve? Sustainability 2020, 12, 5250. [Google Scholar] [CrossRef]
- Tantrakarnapa, K.; Bhopdhornangkul, B.; Nakhaapakorn, K. Influencing factors of COVID-19 spreading: A case study of Thailand. J. Public Health 2020, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Shah, A.U.M.; Safri, S.N.A.; Thevadas, R.; Noordin, N.K.; Abd Rahman, A.; Sekawi, Z.; Ideris, A.; Sultan, M.T.H. COVID-19 Outbreak in Malaysia: Actions Taken by the Malaysian Government. Int. J. Infect. Dis. 2020, 97, 108–116. [Google Scholar] [CrossRef] [PubMed]
- Yeh, M.-J.; Cheng, Y. Policies Tackling the COVID-19 Pandemic: A Sociopolitical Perspective from Taiwan. Health Secur. 2020, 18, 427–434. [Google Scholar] [CrossRef]
- Woo, J.J. Policy capacity and Singapore’s response to the COVID-19 pandemic. Policy Soc. 2020, 39, 345–362. [Google Scholar] [CrossRef]
- Kuguyo, O.; Kengne, A.P.; Dandara, C. Singapore COVID-19 Pandemic Response as a Successful Model Framework for Low-Resource Health Care Settings in Africa? OMICS J. Integr. Biol. 2020, 24, 470–478. [Google Scholar] [CrossRef] [PubMed]
- Taiwan Centers for Disease Control. Entry Quarantine Measures for Arrivals Experiencing Symptoms in the Past 14 Days to be Enhanced Starting from November 9. Available online: https://www.cdc.gov.tw/En/Bulletin/Detail/tIZmSyr-uHEaAkxkUd2qjQ?typeid=158 (accessed on 30 December 2020).
- Dighe, A.; Cattarino, L.; Cuomo-Dannenburg, G.; Skarp, J.; Imai, N.; Bhatia, S.; Gaythorpe, K.A.M.; Ainslie, K.E.C.; Baguelin, M.; Bhatt, S.; et al. Response to COVID-19 in South Korea and implications for lifting stringent interventions. BMC Med. 2020, 18, 1–12. [Google Scholar] [CrossRef]
- Ferrari, R.; De Angelis, M. COVID-19 testing. Eur. Heart J. 2020, 41, 2427–2428. [Google Scholar] [CrossRef]
- Mahase, E. Covid-19: Mass testing is inaccurate and gives false sense of security, minister admits. BMJ 2020, 371. [Google Scholar] [CrossRef]
- Canals, M.; Cuadrado, C.; Canals, A.; Yohannessen, K.; Lefio, L.A.; Bertoglia, M.P.; Eguiguren, P.; Siches, I.; Iglesias, V.; Arteaga, O. Epidemic trends, public health response and health system capacity: The Chilean experience in four months of the COVID-19 pandemic. Revista Panamericana de Salud Pública 2020, 44, e99. [Google Scholar] [CrossRef]
- Grech, V.; Borg, M. Influenza vaccination in the COVID-19 era. Early Hum. Dev. 2020, 148, 105116. [Google Scholar] [CrossRef] [PubMed]
- Shaw, R.; Kim, Y.-K.; Hua, J. Governance, technology and citizen behavior in pandemic: Lessons from COVID-19 in East Asia. Prog. Disaster Sci. 2020, 6, 100090. [Google Scholar] [CrossRef]
- Summers, J.; Cheng, H.-Y.; Lin, H.-H.; Barnard, L.T.; Kvalsvig, A.; Wilson, N.; Baker, M.G. Potential lessons from the Taiwan and New Zealand health responses to the COVID-19 pandemic. Lancet Reg. Health Western Pac. 2020, 4, 100044. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Clinical Characteristics | Frequency | Percentage (%) | |
|---|---|---|---|
| Gender | Male | 356 | 46.5 |
| Female | 410 | 53.5 | |
| Age Intervals, y | 0~9 | 5 | 0.7 |
| 10~19 | 33 | 4.3 | |
| 20~29 | 250 | 32.6 | |
| 30~39 | 166 | 21.7 | |
| 40~49 | 154 | 20.1 | |
| 50~59 | 74 | 9.7 | |
| 60~69 | 62 | 8.1 | |
| 70~79 | 18 | 2.3 | |
| 80~89 | 3 | 0.4 | |
| >90 | 1 | 0.1 | |
| Transmission Classifications | Local Transmission | 55 | 7.2 |
| Imported Case | 675 | 88.1 | |
| Navy Dunmu Fleet | 36 | 4.7 | |
| Symptoms | Asymptomatic | 199 | 15.9 |
| Flu Symptoms | 490 | 39.1 | |
| Cough | 236 | 18.8 | |
| Fever (Chills) | 218 | 17.4 | |
| Loss of Smell | 68 | 5.4 | |
| Gastrointestinal Symptoms | 41 | 3.4 | |
| Clinical Measures | Hospitalized | 132 | 17.2 |
| Discharged Alive | 627 | 81.9 | |
| Died | 7 | 0.9 | |
| Countries | Total Covid-19 Confirmed Cases * | Population * | Incidence Rates * (Per Million Population) | Total Deaths * | Mortality Rates * (Per Million Population) | Total Testing * | Testing Rates * (Per Million Population) | Risk Ratio |
|---|---|---|---|---|---|---|---|---|
| Malaysia | 98,737 | 32,564,991 | 30,320 | 444 | 14 | 3,170,140 | 97,348 | 947.5 |
| Singapore | 58,495 | 58,72,383 | 9961 | 29 | 5 | 5,236,487 | 891,714 | 311.3 |
| Japan | 203,113 | 126,289,463 | 1608 | 2994 | 24 | 4,473,256 | 35,420 | 50.3 |
| South Korea | 52,548 | 51,290,555 | 1025 | 739 | 14 | 3,826,570 | 74,606 | 32.0 |
| Thailand | 5829 | 69,884,225 | 83 | 60 | 0.9 | 1,217,873 | 17,427 | 2.6 |
| China | 86,899 | 1,439,323,776 | 60 | 4634 | 3 | 160,000,000 | 111,163 | 1.9 |
| Taiwan | 766 | 23,837,521 | 32 | 7 | 0.3 | 119,405 | 5009 | 1.0 |
| Control Measure | Epidemic Preventive Policies | Hospital Strategies (g. Healthcare Facilities, Provisions, and Medical Team Preparations) |
|---|---|---|
|
| January
|
|
| February Big Data Analytics Tracking System
|
|
| March Perfecting the Healthcare System
|
|
| April Infection Prevention and Control Measures for the Healthcare System
|
|
| |
|
| May
|
|
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tan, T.W.; Tan, H.L.; Chang, M.N.; Lin, W.S.; Chang, C.M. Effectiveness of Epidemic Preventive Policies and Hospital Strategies in Combating COVID-19 Outbreak in Taiwan. Int. J. Environ. Res. Public Health 2021, 18, 3456. https://doi.org/10.3390/ijerph18073456
Tan TW, Tan HL, Chang MN, Lin WS, Chang CM. Effectiveness of Epidemic Preventive Policies and Hospital Strategies in Combating COVID-19 Outbreak in Taiwan. International Journal of Environmental Research and Public Health. 2021; 18(7):3456. https://doi.org/10.3390/ijerph18073456
Chicago/Turabian StyleTan, Ting Wan, Han Ling Tan, Man Na Chang, Wen Shu Lin, and Chih Ming Chang. 2021. "Effectiveness of Epidemic Preventive Policies and Hospital Strategies in Combating COVID-19 Outbreak in Taiwan" International Journal of Environmental Research and Public Health 18, no. 7: 3456. https://doi.org/10.3390/ijerph18073456