
Variation in Obsessive-Compulsive Disorder Symptoms and Treatments: A Side Effect of COVID-19

Abstract
:1. Introduction
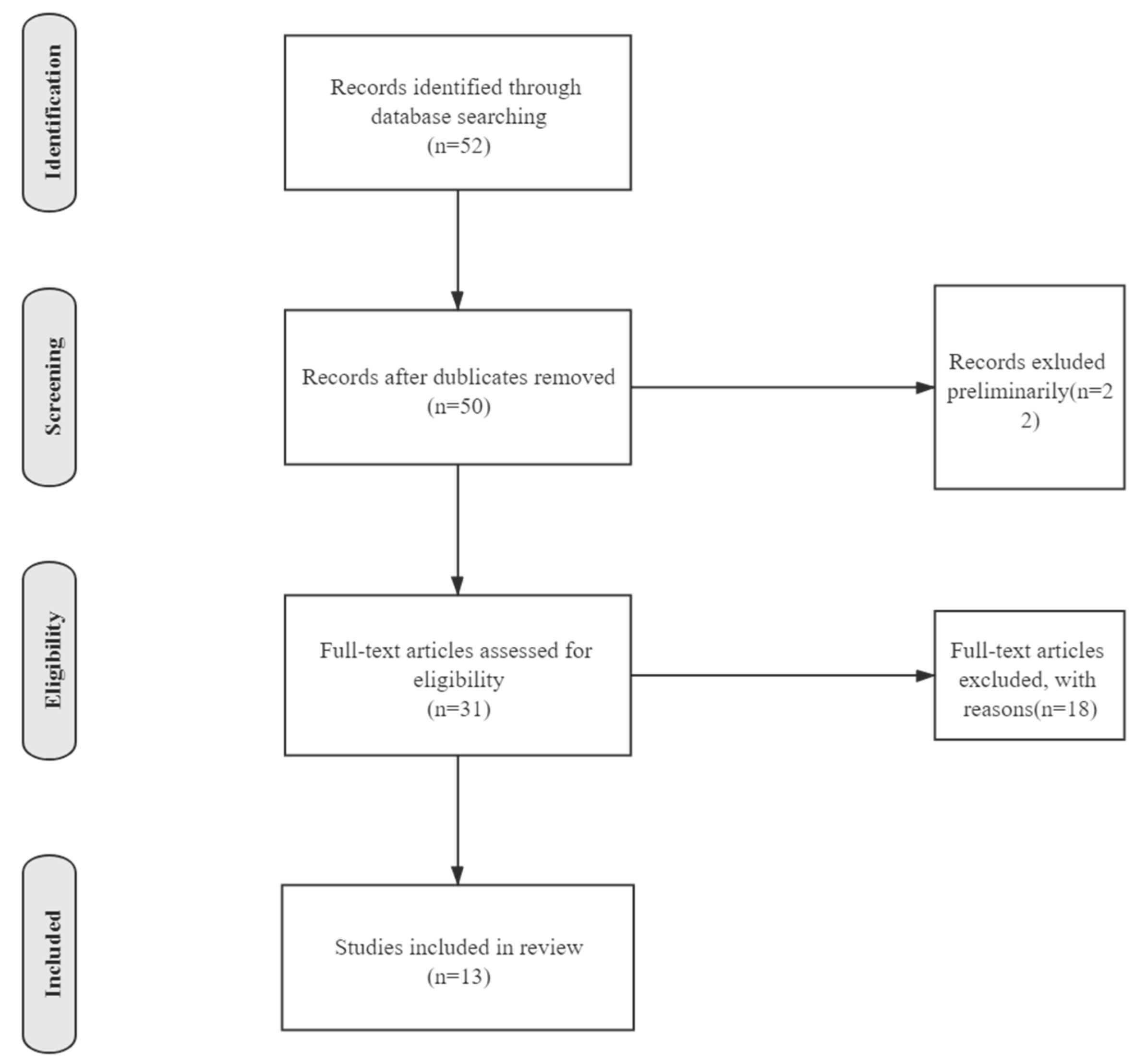
2. Methods
2.1. Search Strategy
2.2. Inclusion and Exclusion Criteria
3. Results
3.1. Studies on OCD Symptoms
3.2. Studies on OCD Treatments
4. Discussion
4.1. OCD Symptoms
4.2. OCD Treatments
4.3. Implications for OCD Investigation, Therapies and Health Policy
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Key Message
Study Limitations
References
- World Health Organization. WHO Director-General’s Opening Remarks at the Media Briefing on COVID-19-11 March 2020. Available online: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-COVID-19---11-march-2020 (accessed on 7 July 2021).
- Johns Hopkins Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html (accessed on 15 January 2021).
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Fergus, T.A.; McKay, D.; Asmundson, G.J.G. COVID stress syndrome: Concept, structure, and correlates. Depress. Anxiety 2020, 37, 706–714. [Google Scholar] [CrossRef] [PubMed]
- French, I.; Lyne, J. Acute exacerbation of OCD symptoms precipitated by media reports of COVID-19. Irish J. Psychol. Med. 2020, 37, 291–294. [Google Scholar] [CrossRef] [PubMed]
- Rachman, S. Fear of contamination. Behav. Res. Ther. 2004, 42, 1227–1255. [Google Scholar] [CrossRef] [PubMed]
- Seto, W.H.; Tsang, D.; Yung, R.W.; Ching, T.Y.; Ng, T.K.; Ho, M.; Ho, L.M.; Peiris, J.S. Advisors of Expert SARS group of Hospital Authority. Effectiveness of precautions against droplets and contact in prevention of nosocomial transmission of severe acute respiratory syndrome (SARS). Lancet 2003, 361, 1519–1520. [Google Scholar] [CrossRef] [Green Version]
- Cox, R.C.; Olatunji, B.O. Linking insomnia and OCD symptoms during the coronavirus pandemic: Examination of prospective associations. J. Anxiety Disord. 2021, 77, 102341. [Google Scholar] [CrossRef]
- Davide, P.; Andrea, P.; Martina, O.; Andrea, E.; Davide, D.; Mario, A. The impact of the COVID-19 pandemic on patients with OCD: Effects of contamination symptoms and remission state before the quarantine in a preliminary naturalistic study. Psychiatry Res. 2020, 291, 113213. [Google Scholar] [CrossRef] [PubMed]
- Jelinek, L.; Moritz, S.; Miegel, F.; Voderholzer, U. Obsessive-compulsive disorder during COVID-19: Turning a problem into an opportunity? J. Anxiety Disord. 2021, 77, 102329. [Google Scholar] [CrossRef] [PubMed]
- Tanir, Y.; Karayagmurlu, A.; Kaya, I.; Kaynar, T.B.; Türkmen, G.; Dambasan, B.N.; Meral, Y.; Coşkun, M. Exacerbation of obsessive compulsive disorder symptoms in children and adolescents during COVID-19 pandemic. Psychiatry Res. 2020, 293, 113363. [Google Scholar] [CrossRef]
- Khosravani, V.; Aardema, F.; Ardestani, S.M.S.; Bastan, F.S. The impact of the coronavirus pandemic on specific symptom dimensions and severity in OCD: A comparison before and during COVID-19 in the context of stress responses. J. Obsessive-Compuls. Relat. Disord. 2021, 29, 100626. [Google Scholar] [CrossRef]
- Kuckertz, J.M.; Van Kirk, N.; Alperovitz, D.; Nota, J.A.; Falkenstein, M.J.; Schreck, M.; Krompinger, J.W. Ahead of the Curve: Responses From Patients in Treatment for Obsessive-Compulsive Disorder to Coronavirus Disease 2019. Front. Psychol. 2020, 11, 572153. [Google Scholar] [CrossRef]
- McKay, D.; Minaya, C.; Storch, E.A. Conducting exposure and response prevention treatment for contamination fears during COVID-19: The behavioral immune system impact on clinician approaches to treatment. J. Anxiety Disord. 2020, 74, 102270. [Google Scholar] [CrossRef] [PubMed]
- Nissen, J.B.; Højgaard, D.; Thomsen, P.H. The immediate effect of COVID-19 pandemic on children and adolescents with obsessive compulsive disorder. BMC Psychiatry 2020, 20, 511. [Google Scholar] [CrossRef]
- Rosa-Alcázar, Á.; García-Hernández, M.D.; Parada-Navas, J.L.; Olivares-Olivares, P.J.; Martínez-Murillo, S.; Rosa-Alcázar, A.I. Coping strategies in obsessive-compulsive patients during COVID-19 lockdown. Int. J. Clin. Health Psychol. 2021, 21, 100223. [Google Scholar] [CrossRef] [PubMed]
- Seçer, I.; Ulaş, S. An Investigation of the Effect of COVID-19 on OCD in Youth in the Context of Emotional Reactivity, Experiential Avoidance, Depression and Anxiety. Int. J. Ment. Health Addict. 2020, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Storch, E.A.; Sheu, J.C.; Guzick, A.G.; Schneider, S.C.; Cepeda, S.L.; Rombado, B.R.; Gupta, R.; Hoch, C.T.; Goodman, W.K. Impact of the COVID-19 pandemic on exposure and response prevention outcomes in adults and youth with obsessive-compulsive disorder. Psychiatry Res. 2021, 295, 113597. [Google Scholar] [CrossRef]
- Wheaton, M.G.; Prikhidko, A.; Messner, G.R. Is Fear of COVID-19 Contagious? The Effects of Emotion Contagion and Social Media Use on Anxiety in Response to the Coronavirus Pandemic. Front. Psychol. 2021, 11, 567379. [Google Scholar] [CrossRef]
- Chakraborty, A.; Karmakar, S. Impact of COVID-19 on Obsessive Compulsive Disorder (OCD). Iran. J. Psychiatry 2020, 15, 256–259. [Google Scholar] [CrossRef]
- Richter, B.P.M.A.; Ramos, R.T. Obsessive-Compulsive Disorder. Am. Acad. Neurol. 2008, 24, 828–844. [Google Scholar] [CrossRef]
- Fenske, J.N.; Petersen, K.; Medical, M.; Arbor, A. Obsessive-Compulsive Disorder: Diagnosis and Management. Am. Fam. Physician 2015, 15, 896–903. [Google Scholar]
- Murphy, D.L.; Timpano, K.R.; Wheaton, M.G.; Greenberg, B.D.; Miguel, E.C. Obsessive-compulsive disorder and its related disorders: A reappraisal of obsessive-compulsive spectrum concepts. Dialogues Clin. Neurosci. 2010, 12, 131–148. [Google Scholar]
- Chandrasekaran, B.; Fernandes, S. Obsessive compulsive symptoms severity among children and adolescents during COVID-19 first wave in Israel. J. Obsessive-Compuls. Relat. Disord. 2020, 14, 337–339. [Google Scholar]
- Abba-Aji, A.; Li, D.; Hrabok, M.; Shalaby, R.; Gusnowski, A.; Vuong, W.; Surood, S.; Nkire, N.; Li, X.-M.; Greenshaw, A.J.; et al. COVID-19 Pandemic and Mental Health: Prevalence and Correlates of New-Onset Obsessive-Compulsive Symptoms in a Canadian Province. Int. J. Environ. Res. Public Health 2020, 17, 6986. [Google Scholar] [CrossRef]
- Banerjee, D.D. The other side of COVID-19: Impact on obsessive compulsive disorder (OCD) and hoarding. Psychiatry Res. 2020, 288. [Google Scholar] [CrossRef] [PubMed]
- Ji, G.; Wei, W.; Yue, K.-C.; Li, H.; Shi, L.-J.; Ma, J.-D.; He, C.-Y.; Zhou, S.-S.; Zhao, Z.; Lou, T.; et al. Effects of the COVID-19 Pandemic on Obsessive-Compulsive Symptoms Among University Students: Prospective Cohort Survey Study. J. Med. Internet Res. 2020, 22, e21915. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Pan, R.; Wan, X.; Tan, Y.; Xu, L.; Mcintyre, R.S. A longitudinal study on the mental health of general population during the COVID-19 epidemic in China. Brain Behav. Immun. J. 2020, 17, 29. [Google Scholar] [CrossRef]
- Zheng, Y.; Xiao, L.; Xie, Y.; Wang, H.; Wang, G. Prevalence and Characteristics of Obsessive-Compulsive Disorder Among Urban Residents in Wuhan During the Stage of Regular Control of Coronavirus Disease-19 Epidemic. Front. Psychiatry 2020, 11, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Benatti, B.; Albert, U.; Maina, G.; Fiorillo, A.; Celebre, L.; Girone, N.; Fineberg, N.; Bramante, S.; Rigardetto, S.; Dell’Osso, B. What Happened to Patients With Obsessive Compulsive Disorder During the COVID-19 Pandemic? A Multicentre Report From Tertiary Clinics in Northern Italy. Front. Psychiatry 2020, 11, 720. [Google Scholar] [CrossRef]
- Krzysz, W.; Ku, M. Treatment of obsessive-compulsive disorders (OCD) and obsessive-compulsive-related disorders (OCRD). Psychiatr. Pol. 2019, 53, 825–843. [Google Scholar]
- Fineberg, N.A.; Van Ameringen, M.; Drummond, L.; Hollander, E.; Stein, D.J.; Geller, D.; Walitza, S.; Nicolini, H.; Osso, B.D. How to manage obsessive-compulsive disorder (OCD) under COVID-19: A clinician’s guide from the International College of Obsessive Compulsive Spectrum Disorders (ICOCS) and the Obsessive-Compulsive and Related Disorders Research Network (OCRN) of the Europe. Compr. Psychiatry 2020, 200, 152174. [Google Scholar] [CrossRef] [PubMed]
- Berman, N.C.; Hezel, D.M.; Wilhelm, S. Is my patient too sad to approach their fear? Depression severity and imaginal exposure outcomes for patients with OCD. J. Behav. Ther. Exp. Psychiatry 2021, 70, 101615. [Google Scholar] [CrossRef]
- Wang, X.; Zhang, X.; He, J. Challenges to the system of reserve medical supplies for public health emergencies: Reflections on the outbreak of the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) epidemic in China. Biosci. Trends 2020, 14, 3–8. [Google Scholar] [CrossRef] [Green Version]
- Sheu, J.C.; McKay, D.; Storch, E.A. COVID-19 and OCD: Potential impact of exposure and response prevention therapy. J. Anxiety Disord. 2020, 76, 102314. [Google Scholar] [CrossRef]
- Jalal, B.; Chamberlain, S.R.; Robbins, T.W.; Sahakian, B.J. Obsessive–compulsive disorder—contamination fears, features, and treatment: Novel smartphone therapies in light of global mental health and pandemics (COVID-19). CNS Spectrums 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ornell, F.; Braga, D.T.; Bavaresco, D.V.; Francke, I.D.; Scherer, J.N.; Von Diemen, L.; Henrique, F.; Kessler, P. Obsessive-compulsive disorder reinforcement during the COVID-19 pandemic. Trends Psychiatry Psychother. 2021. [Google Scholar] [CrossRef]
- Darvishi, E.; Golestan, S.; Demehri, F.; Jamalnia, S. A Cross-Sectional Study on Cognitive Errors and Obsessive-Compulsive Disorders among Young People During the Outbreak of Coronavirus Disease 2019. Act. Nerv. Super. 2020, 62, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Sharma, L.P.; Balachander, S.; Thamby, A.; Bhattacharya, M.; Kishore, C.; Shanbhag, V.; Sekharan, J.T.; Narayanaswamy, J.C.; Arumugham, S.S.; Reddy, J.Y.C. Impact of the COVID-19 Pandemic on the Short-Term Course of Obsessive-Compulsive Disorder. J. Nerv. Ment. Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Pittenger, C.; Bloch, M. Drug Treatment of Obsessive-Compulsive Disorder: Dark Past, Bright Present, but Glowing Future. Psychiatr. Clin. N. Am. 2014, 37, 375–391. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Author and Year | Purpose | Data Sources | Study Design/Sample Size | Control Variables | Standards | Findings |
|---|---|---|---|---|---|---|
| [7] Cox et al., 2020 | To determine whether insomnia patients are vulnerable to OCD during the pandemic, and whether peculiar symptoms exacerbates under COVID-19 | Questionnaire data | Cross-sectional and panel/n = 379, Slight distinction between different researches | Living state, symptom | Changes in OCIR, ISI, DASS scores | Checking and some symptoms do notincrease. Hoarding and washing exacerbates to some extent. |
| [8] Davide et al., 2020 | To evaluate the changes on OCD symptoms and investigated the effects of contamination symptoms and remission state | Questionnaire data | Cross-sectional/n = 30 | Sex, remission status, social behavior | Increase or decrease in Y-BOCS score | During the quarantine, OCD worsens significantly, particularly amongst the patients withcontamination symptoms |
| [9] Jelinek et al., 2020 | To determine whether OCD worsens more extraordinarily in those who are washers than those non-washers | Questionnaire data | Cross-sectional/n = 394 | Washer and non-washer, symptom | Changes in OCIR scores | The negative effects of COVID-19 were more pronounced in washers than in non-washers. |
| [10] Tanir et al., 2020 | To investigate the effects of home confinement exacerbation of OCD symptoms among young subjects. | Questionnaire data | Cross-sectional/n = 61 | Age, sex, family income, treatment status, information sources, daily preoccupation current OCD diagnosis in parent(s), duration of parents’ education, COVID-19 diagnosis in someone familiar | Changes in CY-BOCS and CGI-S scores | Young subjects with OCD may develop additional symptoms and worsen already existing symptoms of OCD during COVID-19 pandemic. |
| [11] Khosravani et al., 2020 | To compare a group of patients with OCD before and during COVID-19 on specific obsessive-compulsive symptom dimensions and symptom severity | Questionnaire data | Panel/n = 270 | Symptom | Increase or decrease in Y-BOCS, DOCS, CSS score | The effect of COVID-19 occursacross various symptoms, including responsibility for harm, unacceptable thoughts, and symmetry. |
| [12] Kuckertz et al., 2020 | To evaluate the effectiveness of tradition OCD therapies under COVID-19 | Clinical data | Panel/n = 6 | N/A | N/A | Effective OCD treatment can and should continue despite COVID-19. |
| [13] Mckay et al., 2020 | To investigated the attitudes of mental health practitioners around exposure treatment during the COVID-19 pandemic | Questionnaire data | Cross-sectional/n = 139 | Age, practising year, sex, ethnicity | Changes in CHILL, IUS-SF and TBES scores | Providers’ OCD caseload and a proposed indicator of BIS activation (coldness) significantly predicted their beliefs about exposure. |
| [14] Nissen et al., 2020 | To examine how children/adolescents with OCD react towards COVID-19 crisis | Questionnaire data | Cross-sectional/n = 102 | Age, gender, therapy, symptom | N/A | The study points towards an influence of the OCD phenotype, baseline insight suggesting a continued vulnerability. |
| [15] Rosa-Alcázar et al., 2021 | To investigate coping strategies in OCD patients during COVID-19 lockdown | Questionnaire data | Cross-sectional/n = 122 (OCD patients), n = 115 (healthy people) | Age, sex, educational level, marital status, comorbidity | Results of COPE-28, HADS | Comorbidity affected the greater use of inappropriate strategies. Depression levels were related to the use of less adaptive strategies. |
| [16] Seçer et al., 2020 | To investigate the relationship between fear of COVID-19 and OCD | Questionnaire data | Cross-sectional/n = 598 | Age | Results of OCICV, Experiential Avoidance Questionnaire, DASC and ERS | The effect of COVID-19 fear on OCD is mediated by emotional reactivity, experiential avoidance and depression- anxiety. |
| [17] Storch et al., 2020 | To investigate clinician perceptions regarding the effect of the COVID-19 pandemic on patients with OCD | Questionnaire data | Cross-sectional/n = 102 | Sex, ethnicity, occupation, age | Changes in Y-BOCS and NIMH-GOCS scores | COVID-19 was associated with attenuation of ERP progress from expected rates. |
| [18] Wheaton et al., 2020 | To study the relationship between emotion contagion and mental healthsymptoms during the COVID-19 pandemic. | Questionnaire data | Cross-sectional/n = 603 | Sex, age, ethnicity | Results of CTS, ECS, OCIR, DASS-21 | Greater susceptibility to emotion contagion was associated with greater concern about the spread of COVID-19 and OCD symptoms. |
| [19] Chakraborty et al., 2020 | To determine whether washing compulsion and contamination fear aggravates under COVID-19 | Clinical and questionnaire data | Cross-sectional/n = 104 | Sex, religion, residence, occupation | Increase or decrease in Y-BOCS score | Handwashing protocol does not aggravate the washing compulsion of patients. The fear of infection with COVID-19 does not increase their fear of contamination. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Liu, W.; Zhang, H.; He, Y. Variation in Obsessive-Compulsive Disorder Symptoms and Treatments: A Side Effect of COVID-19. Int. J. Environ. Res. Public Health 2021, 18, 7420. https://doi.org/10.3390/ijerph18147420
Liu W, Zhang H, He Y. Variation in Obsessive-Compulsive Disorder Symptoms and Treatments: A Side Effect of COVID-19. International Journal of Environmental Research and Public Health. 2021; 18(14):7420. https://doi.org/10.3390/ijerph18147420
Chicago/Turabian StyleLiu, Wuqianhui, Haitao Zhang, and Yuan He. 2021. "Variation in Obsessive-Compulsive Disorder Symptoms and Treatments: A Side Effect of COVID-19" International Journal of Environmental Research and Public Health 18, no. 14: 7420. https://doi.org/10.3390/ijerph18147420