
Working Conditions as Risk Factors for Depressive Symptoms among Spanish-Speaking Au Pairs Living in Germany—Longitudinal Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Population
- (1)
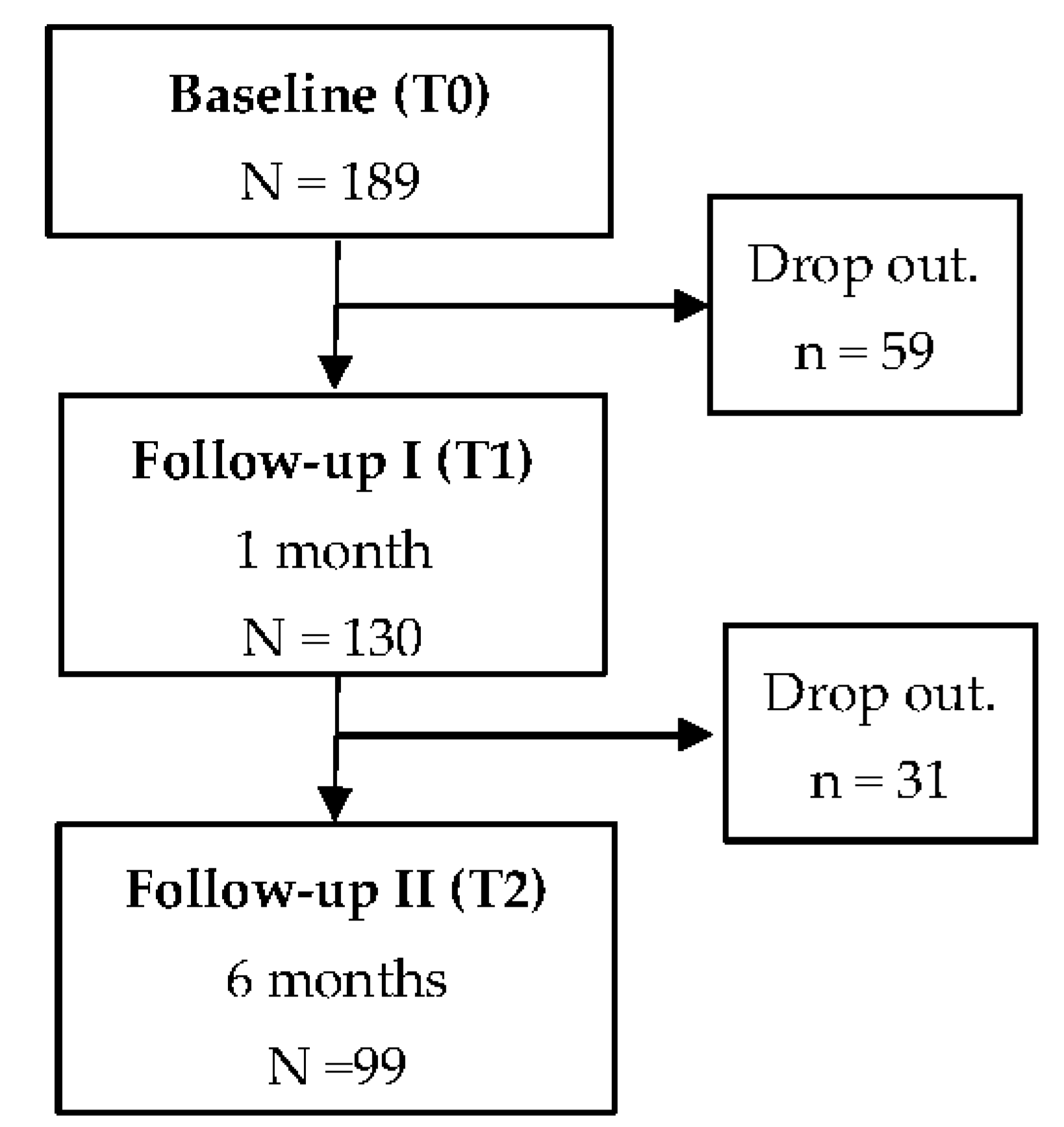
- Baseline (T0): carried out when the au pair arrived in Germany (less or equal to three weeks from arrival).
- (2)
- 1st follow-up (T1): one month after the initial assessment.
- (3)
- 2nd follow-up (T2): six months after the initial assessment.
2.2. Recruitment of Participants
2.3. Questionnaire Instruments
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sollund, R. Regarding Au Pairs in the Norwegian Welfare State. Eur. J. Women’s Stud. 2010, 17, 143–160. [Google Scholar] [CrossRef]
- Rohde-Abuba, C.; Tkach, O. FINDING ONESELF ABROAD: Au pairs’ strategies of self-positioning in hosting societies. Nord. J. Migr. Res. 2016, 6, 193–198. [Google Scholar] [CrossRef] [Green Version]
- Caudera-Preil, S. Als Au Pair ins Ausland; Falken Verlag: Dresden, Germany, 2001. [Google Scholar]
- Cox, R. Au Pairs’ Lives in Global Context Sisters or Servants? In Migration, Diasporas and Citizenship Series; Palgrave Macmillan: London, England, 2015. [Google Scholar]
- Rohde, C. From Germany with Love: Transnational Family Networks and Daughterhood Constructions of Russian Au Pair Migrants. Transnatl. Soc. Rev. A Soc. Work J. 2014, 2, 121–137. [Google Scholar] [CrossRef]
- Walter-Bolhöfer, C. Konjunkturumfrage 2017: Entwicklungen und Trends im Deutschen Au-Pair-Wesen; Calypso Verlag: Dresden, Germany, 2017. [Google Scholar]
- Walter-Bolhöfer, C. Konjunkturumfrage 2019: Entwicklungen und Trends im Deutschen Au-Pair-Wesen; Calypso Verlag: Neunkirchen-Seelscheid, Germany, 2019. [Google Scholar]
- Durin, S. Ethnicity and the Au Pair Experience: Latin American Au Pairs in Marseille, France. In Au Pairs’ Lives in Global Context; Palgrave Macmillan: New York, NY, USA, 2015. [Google Scholar]
- Espinoza-Castro, B.; Vasquez Rueda, L.E.; Mendoza Lopez, R.V.; Radon, K. Working Below Skill Level as Risk Factor for Distress Among Latin American Migrants Living in Germany: A Cross-Sectional Study. J. Immigr. Minor Health 2019, 21, 1012–1018. [Google Scholar] [CrossRef]
- Würtz, E. Intercultural Communication on Web sites:A Cross-Cultural Analysis of Web site sfrom High-Context Cultures andLow-Context Cultures. J. Comput. Mediat. Commun. 2006, 11, 274–299. [Google Scholar] [CrossRef]
- Avruch, K. Cross-cultural conflict. Confl. Resolut. 2009, 1, 45–57. [Google Scholar]
- Cruz, E.; Van Dijk, F.; Radon, K. Working Conditions and Health of au-Pairs in Germany, A Cross-Sectional Study. Master’s Thesis, LMU, Munich, Germany, 2018. [Google Scholar]
- Bakker, A.B.; Demerouti, E. The Job Demands-Resources model: State of the art. J. Manag. Psychol. 2007, 22, 309–328. [Google Scholar] [CrossRef] [Green Version]
- Løvdal, L. Au Pairs in Norway: Experiences from an Outreach Project. In Migration, Diasporas and Citizenship Series; Palgrave Macmillan: London, UK, 2015; pp. 136–155. [Google Scholar]
- Espinoza-Castro, B.; Weinmann, T.; Mendoza López, R.; Radon, K. Major Depressive Syndrome (MDS) and its Association with Time of Residence among Spanish Speaking Au-Pairs Living in Germany. Int. J. Environ. Res. Public Health 2019, 16, 4764. [Google Scholar] [CrossRef] [Green Version]
- Sander, M. Return Migration and the “Healthy Immigrant Effect”; SOEP Papers; The German Socio-Economic Panel: Berlin, Germany, 2007. [Google Scholar]
- Tolentino, J.C.; Schmidt, S.L. DSM-5 Criteria and Depression Severity: Implications for Clinical Practice. Front. Psychiatry 2018, 9, 450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; (DSM-V); American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Kroenke, K.; Spitzer, R. The PHQ-9: Validity of a brief depression severity measure. JGIM 2001, 16, 606–616. [Google Scholar] [CrossRef]
- Maske, U.E.; Busch, M.A.; Jacobi, F.; Beesdo-Baum, K.; Seiffert, I.; Wittchen, H.U.; Riedel-Heller, S.; Hapke, U. Current major depressive syndrome measured with the Patient Health Questionnaire-9 (PHQ-9) and the Composite International Diagnostic Interview (CIDI): Results from a cross-sectional population-based study of adults in Germany. BMC Psychiatry 2015, 15, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Publishing: Washington DC, USA, 2000. [Google Scholar]
- Martin, A.; Rief, W.; Klaiberg, A.; Braehler, E. Validity of the Brief Patient Health Questionnaire Mood Scale (PHQ-9) in the general population. Gen. Hosp. Psychiatry 2006, 28, 71–77. [Google Scholar] [CrossRef]
- Benavides, F.; Zímmermann-Verdejo, M.; Campos-Serna, J.; Carmenate, J.; Carmenate, L.; Báez, I.; Nogareda, C.; Molinero Ruiz, E.; Losilla Vidal, J.; Pinilla García, F. Conjunto mínimo básico de ítems para el diseño de cuestionarios sobre condiciones de trabajo y salud. Arch. Prev. Riesg. Labor. 2010, 13, 13–22. [Google Scholar]
- Solar, O.; Bernales, P.; Sembler, C.; Vallebuona, C. Primera Encuesta Nacional de Empleo, Trabajo y Salud ENETS 2009: Diseño Conceptual y Metodológico; Ministerio de Salud/Dirección del Trabajo/Instituto de Seguridad Laboral: Santiago, Chile, 2010. [Google Scholar]
- Shen, C.; Chen, H. Model selection for generalized estimating equations accommodating dropout missingness. Biometrics 2012, 68, 1046–1054. [Google Scholar] [CrossRef]
- Liang, K.; Zeger, S.L. Longitudinal data analysis using generalized linear models. Biometrika 1986, 73, 13–22. [Google Scholar] [CrossRef]
- Fitzmaurice, G.; Davidian, M.; Verbeke, G.; Molenberghs, G. Longitudinal Data Analysis; Chapman & Hall/CRC: Baltimore, MD, USA, 2009; Volume 13. [Google Scholar]
- Shen, C.; Chen, H. Model selection of generalized estimating equations with multiply imputed longitudinal data. Biom J. 2013, 55, 899–911. [Google Scholar] [CrossRef]
- Lipsitz, S.; Fitzmaurice, G. Sample size for repeated measures studies with binary responses. Stat. Med. 1994, 13, 1233–1239. [Google Scholar] [CrossRef]
- DeSouza, C.; Legedza, A.; Sankoh, A. An Overview of Practical Approaches for Handling Missing Data in Clinical Trials. J. Biopharm. Stat. 2009, 19, 1055–1073. [Google Scholar] [CrossRef]
- Wittchen, H.U.; Jacobi, F.; Rehm, J.; Gustavsson, A.; Svensson, M.; Jonsson, B.; Olesen, J.; Allgulander, C.; Alonso, J.; Faravelli, C.; et al. The size and burden of mental disorders and other disorders of the brain in Europe 2010. Eur. Neuropsychopharmacol. 2011, 21, 655–679. [Google Scholar] [CrossRef] [Green Version]
- Janssen-Kallenberg, H.; Schulz, H.; Kluge, U.; Strehle, J.; Wittchen, H.U.; Wolfradt, U.; Koch-Gromus, U.; Heinz, A.; Mosko, M.; Dingoyan, D. Acculturation and other risk factors of depressive disorders in individuals with Turkish migration backgrounds. BMC Psychiatry 2017, 17, 264. [Google Scholar] [CrossRef] [Green Version]
- Løvda, L. Legal Advice for Women; Juridisk Rådgivning for Kvinner: Oslo, Norway, 2013; Volume 64. [Google Scholar]
- Smith, A. Part of the Family? Experiences of Au Pairs in Ireland; Migrant Rights Centre Ireland: London, UK, 2012. [Google Scholar]
- O’Connor, K.; Stoecklin-Marois, M.; Schenker, M.B. Examining nervios among immigrant male farmworkers in the MICASA Study: Sociodemographics, housing conditions and psychosocial factors. J. Immigr. Minority Health 2015, 17, 198–207. [Google Scholar] [CrossRef] [Green Version]
- Vahabi, M.; Wong, J.P.; Lofters, A. Migrant Live-in Caregivers Mental Health in Canada. Community Ment. Health J. 2018, 54, 590–599. [Google Scholar] [CrossRef]
- Caregiving Benefits and Leave—Canada.ca [Internet] Government of Canada “Employment Canada”. Available online: https://www.canada.ca/en/services/benefits/ei/caregiving.html (accessed on 1 August 2019).
- Carlos, J.; Wilson, K. Migration among temporary foreign workers: Examining health and access to health care among Filipina live-in caregivers Soc. Sci. Med. 2018, 209, 117–124. [Google Scholar] [CrossRef]
- Spitzer, D.L.; Bitar, S.; Kalbach, M.; Bernardino, C.; Pereira, I.I. In the Shadows: Live-in Caregivers in Alberta. In Changing Together, A Centre for Immigrant Women, Edmonton; Prairie Metropolis Centre: Calgary, AB, Canada, 2002. [Google Scholar]
- Sekeráková Búriková, Z. ‘Good Families’ and the Shadows of Servitude: Au Pair Gossip and Norms of Au Pair Employment’ in Global Context: Sisters or Servants? Palgrave Macmillan: New York, NY, USA; London, UK, 2015; pp. 36–52. [Google Scholar]
- Wu, Z.; Schimmele, C. The Healthy Migrant Effect on Depression: Variation over Time? Can. Stud. Popul. 2005, 32, 271–295. [Google Scholar] [CrossRef] [Green Version]
- Hondagneu-Sotelo, P. Doméstica: Immigrant Workers Cleaning and Caring in the Shadows of Affluence; University of California Press: Berkeley, CA, USA; Los Angeles, CA, USA; London, UK, 2001. [Google Scholar]
- Atkinson, R.; Flint, J. Accessing Hidden and Hard-to-Reach Populations: Snowball Research Strategies; Gilbert, N., Ed.; Social Research Update: Guildford, UK, 2001. [Google Scholar]
- Baltar, F.; Brunet, I. Social research 2.0: Virtual snowball sampling method using Facebook. Internet Res. 2012, 22, 57–64. [Google Scholar] [CrossRef]
- Göritz, A. Incentives in Web Studies: Methodological Issues and a Review. Int. J. Internet Sci. 2006, 1, 58–70. [Google Scholar]
- Monge, S.; Ronda, E.; Pons-Vigues, M.; Vives Cases, C.; Malmusi, D.; Gil-Gonzalez, D. [Methodological limitations and recommendations in publications on migrant population health in Spain]. Gac. Sanit. 2015, 29, 461–463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rothman, K.J.; Gallacher, J.E.; Hatch, E.E. Why representativeness should be avoided. Int. J. Epidemiol. 2013, 42, 1012–1014. [Google Scholar] [CrossRef] [Green Version]
- Council of Europe. European Agreement on Au Pair Placement. Available online: https://www.coe.int/en/web/conventions/full-list//conventions/rms/090000168007231c (accessed on 6 February 2017).


{kind=link}
| Characteristics | Participants | Dropouts | p-Value | |
|---|---|---|---|---|
| N = 99 | N = 90 | |||
| n (%) | n (%) | |||
| Gender | Female | 87 (89.7) | 82 (89.1) | 0.81 |
| Age (years) | 18–21 | 30 (30.9) | 43 (47.3) | 0.03 |
| 22–24 | 44 (45.4) | 25 (28.6) | ||
| 25–28 | 23 (23.7) | 22 (24.2) | ||
| Higher education | Yes | 80 (86.0) | 68 (75.6) | 0.09 |
| Region of origin | Spain | 10 (10.3) | 8 (8.7) | 0.54 |
| Colombia | 53 (54.6) | 40 (43.5) | ||
| Mexico and Central America | 22 (22.7) | 29 (31.5) | ||
| South America (w/o Colombia) | 11 (11.3) | 13 (14.1) | ||
| Settlement of residence * | Towns | 36 (38.3) | 13 (41.2) | 0.84 |
| Minor city | 14 (14.9) | 4 (17.6) | ||
| Major city | 44 (46.8) | 13 (41.2) | ||
| Region of residence in Germany * | Northern | 19 (20.5) | 5 (12.5) | 0.46 |
| Southern | 33 (36.4) | 10 (37.5) | ||
| Eastern | 9 (9.1) | 5 (12.5) | ||
| Western | 31 (34.1) | 10 (37.5) | ||
| Working hours per week * | >40 h | 16 (16.8) | 4 (12.1) | 0.59 |
| Extra hours of babysitting *,# | Yes | 62 (70.3) | 21 (70.0) | 0.82 |
| Working on holidays * | Yes | 31 (35.2) | 11 (35.0) | 0.87 |
| Days off per week * | One day | 26 (27.7) | 11 (35.3) | 0.37 |
| Two days | 68 (72.3) | 19 (64.7) | ||
| Schedule’s adaptation to social & family commitments * | Well | 71 (80.7) | 26 (85.5) | 0.99 |
| Au pair agency contract * | Yes | 46 (52.3) | 15 (50.0) | 0.69 |
| Additional job besides au pair * | Yes | 10 (11.4) | 5 (12.5) | 0.53 |
| Violence at work * | Yes | 8 (5.7) | 1 (2.5) | 0.55 |
| Physical violence by the host children * | Yes | 26 (29.9) | 10 (32.5) | 0.73 |
| Verbal offenses * | Yes | 20 (23.0) | 10 (33.0) | 0.50 |
| Depressive symptoms | DS- | 73 (73.4) | 64 (71.1) | 0.07 |
| DS+ | 15 (15.3) | 8 (8.9) | ||
| ODS | 8 (8.2) | 7 (7.8) | ||
| MDS | 3 (3.1) | 11 (12.2) | ||
| Characteristics | Depressive Symptoms # | p-Value | |
|---|---|---|---|
| n (%) | |||
| Gender | Female | 24 (27.3) | 0.99 |
| Male | 2 (25.0) | ||
| Age (years) | 18–21 | 8 (26.7) | 0.80 |
| 22–24 | 13 (29.5) | ||
| 25–28 | 5 (20.8) | ||
| Higher education | No | 2 (15.4) | 0.51 |
| Yes | 21 (25.9) | ||
| Region of origin | Spain | 4 (40.0) | 0.22 |
| Colombia | 17 (32.1) | ||
| Mexico and Central America | 4 (18.2) | ||
| South America(w/o Colombia) | 1 (8.3) | ||
| Settlement of residence | Towns | 11 (28.9) | 0.81 |
| Cities | 15 (25.0) | ||
| Region of residence in Germany | Northern | 4 (20.0) | 0.85 |
| Southern | 10 (28.6) | ||
| Eastern | 3 (33.3) | ||
| Western | 9 (26.5) | ||
| Working hours per week | ≤40 h | 18 (22.8) | 0.05 |
| >40 h | 8 (44.4) | ||
| Extra hours of babysitting * | No | 4 (19.0) | 0.57 |
| Yes | 22 (28.6) | ||
| Working on holidays | No | 13 (19.1) | 0.02 |
| Yes | 13 (43.3) | ||
| Days off per week | One day | 9 (33.3) | 0.44 |
| Two days | 17 (23.9) | ||
| Schedule’s adaptation to social & family commitments | Bad | 13 (56.5) | 0.01 |
| Well | 13 (17.3) | ||
| Au pair agency contract | No | 12 (25.0) | 0.82 |
| Yes | 14 (28.0) | ||
| Additional job besides au pair | No | 23 (26.4) | 0.99 |
| Yes | 3 (27.3) | ||
| Violence at work | No | 22 (24.4) | 0.02 |
| Yes | 3 (100.0) | ||
| Physical violence by the host children | No | 11 (16.9) | 0.01 |
| Yes | 14 (51.9) | ||
| Verbal offenses | No | 14 (20.3) | 0.02 |
| Yes | 9 (45.0) | ||
| Depressive Symptoms # | T2 | p-Value | ||
|---|---|---|---|---|
| No | Yes | |||
| n (%) | n (%) | |||
| T0 | No | 61 (82.4) | 13 (17.6) | 0.83 |
| Yes | 11 (45.8) | 13 (54.2) | ||
| T1 | No | 61 (83.6) | 12 (16.4) | 0.99 |
| Yes | 11 (44.0) | 14 (56.0) | ||
| Characteristics | Crude OR | Adjusted OR | |
|---|---|---|---|
| (95% CI) | (95% CI) | ||
| Working hours per week | ≤40 h | 1 | 1 |
| >40 h | 2.88 (1.32–6.28) | 3.47 (1.46–8.28) | |
| Extra hours of babysitting * | No | 1 | N/A |
| Yes | 1.88 (0.32–11.09) | ||
| Working on holidays | No | 1 | 1 |
| Yes | 2.66 (1.25–5.66) | 1.50 (0.71–3.18) | |
| Days off per week | One day | 1 | N/A |
| Two days | 0.67 (0.30–1.49) | ||
| Schedule’s adaptation to social & family commitments | Good | 1 | 1 |
| Bad | 1.31 (1.34–8.20) | 2.24 (0.95–5.28) | |
| Au pair agency contract | No | 1 | N/A |
| Yes | 1.70 (0.71–4.05) | ||
| Additional job besides au pair | No | 1 | N/A |
| Yes | 0.68 (0.23–2.02) | ||
| Violence at work | No | 1 | N/A |
| Yes | 0.78 (0.13 −4.49) | ||
| Physical violence by the host children | No | 1 | 1 |
| Yes | 5.34 (2.33–12.21) | 4.95 (2.16–9.75) | |
| Verbal offenses | No | 1 | 1 |
| Yes | 4.38 (1.91–10.06) | 1.63 (0.66–4.03) | |
| Follow-up time+ | T0 | 1 | 1 |
| T1 | 1.08 (0.73–1.58) | 1.05 (0.53–1.50) | |
| T2 | 0.99 (0.61–1.61) | 0.81 (0.42–1.58) | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Espinoza-Castro, B.; Weinmann, T.; Mendoza López, R.; Radon, K. Working Conditions as Risk Factors for Depressive Symptoms among Spanish-Speaking Au Pairs Living in Germany—Longitudinal Study. Int. J. Environ. Res. Public Health 2021, 18, 6940. https://doi.org/10.3390/ijerph18136940
Espinoza-Castro B, Weinmann T, Mendoza López R, Radon K. Working Conditions as Risk Factors for Depressive Symptoms among Spanish-Speaking Au Pairs Living in Germany—Longitudinal Study. International Journal of Environmental Research and Public Health. 2021; 18(13):6940. https://doi.org/10.3390/ijerph18136940
Chicago/Turabian StyleEspinoza-Castro, Bernarda, Tobias Weinmann, Rossana Mendoza López, and Katja Radon. 2021. "Working Conditions as Risk Factors for Depressive Symptoms among Spanish-Speaking Au Pairs Living in Germany—Longitudinal Study" International Journal of Environmental Research and Public Health 18, no. 13: 6940. https://doi.org/10.3390/ijerph18136940