Household Food Insecurity: Comparison between Families with and without Members with Disabilities

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Disability-Related Characteristics
2.3. Assessment of Household Food Insecurity
2.4. Other Variables
2.5. Statistical Analyses
3. Results
3.1. Characteristics of Households with and without Persons with Disabilities
3.2. Food Access and Food Security Status
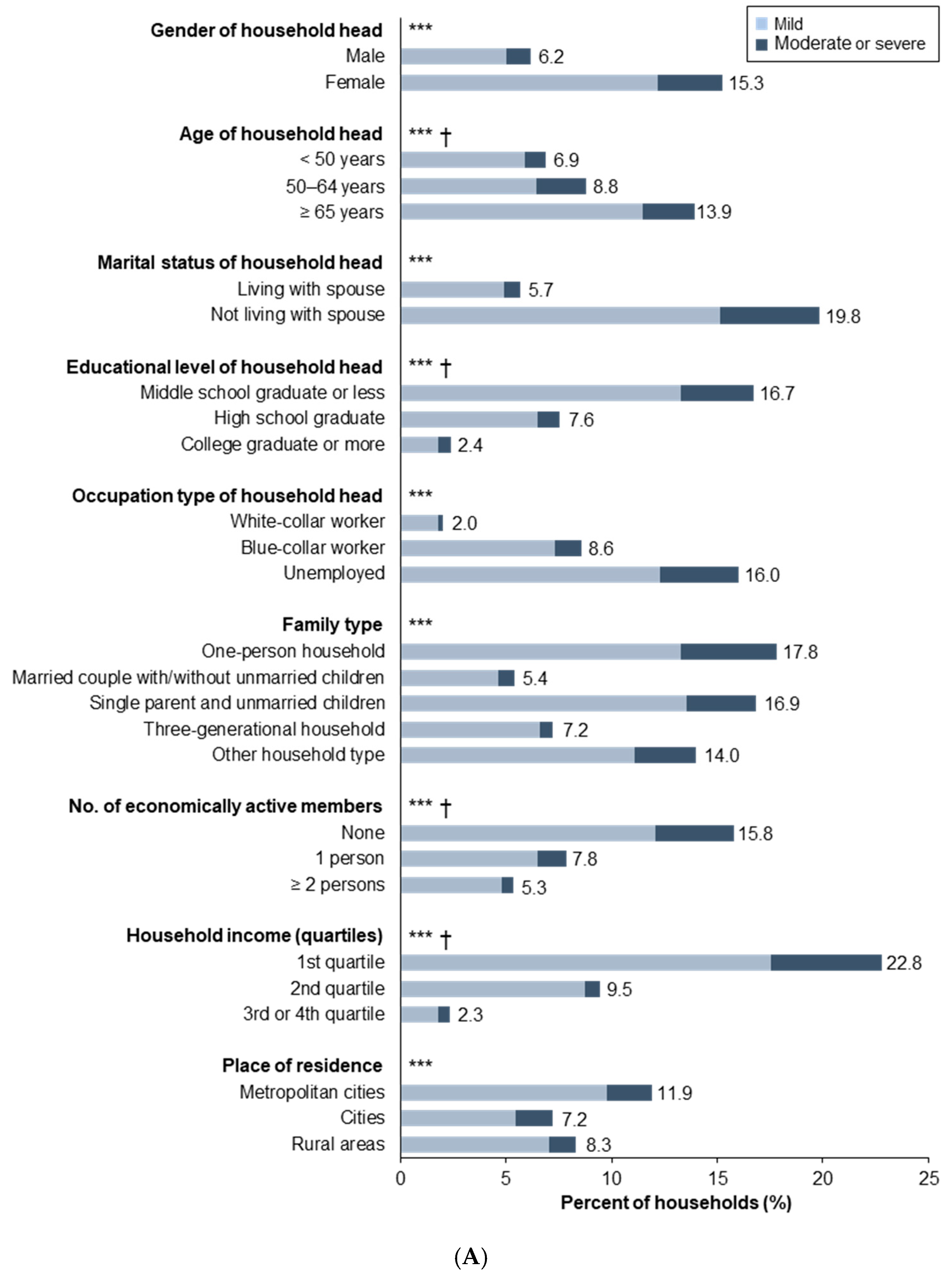
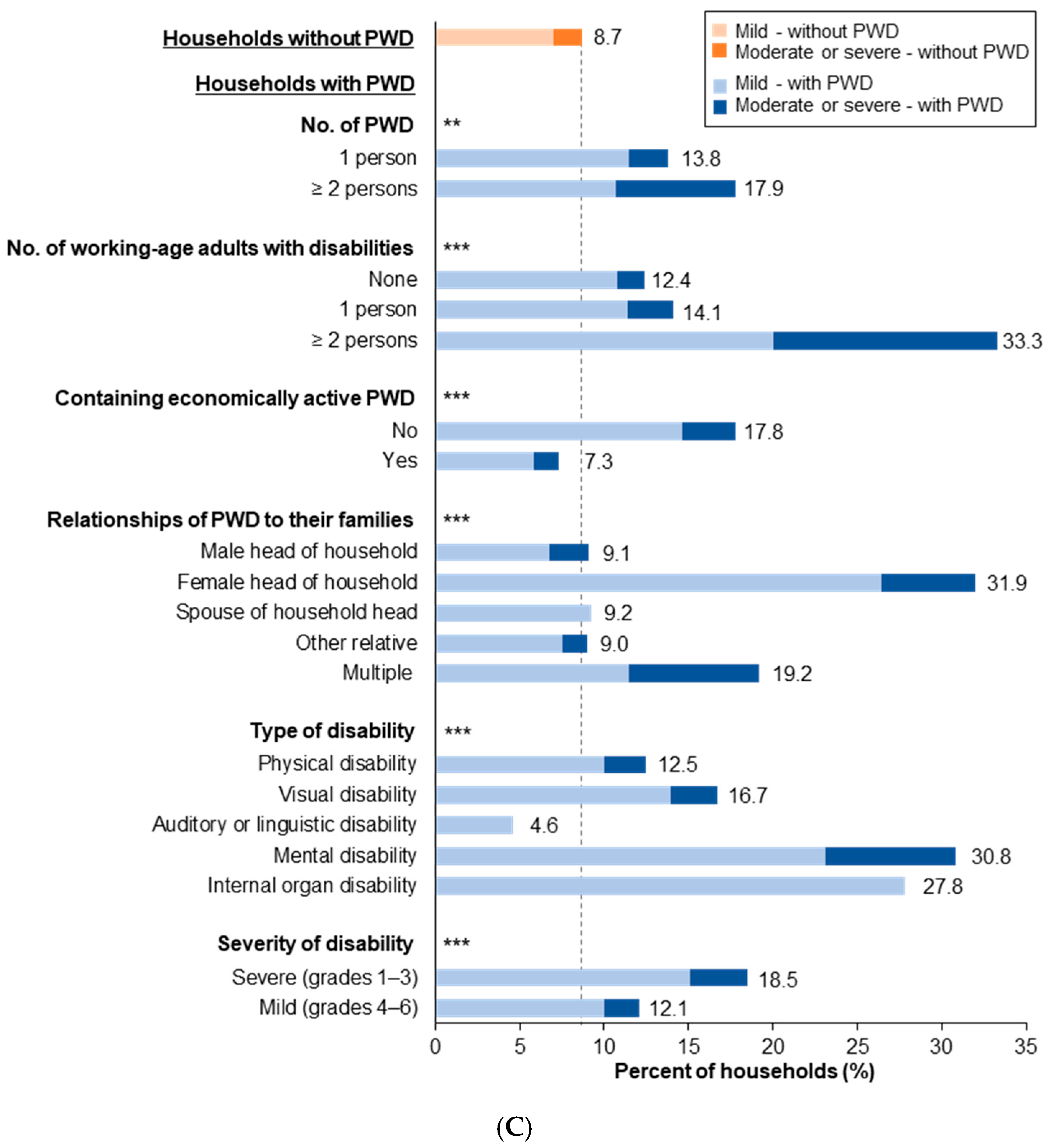
3.3. Prevalence of Household Food Insecurity
3.4. Association between Disability Status of Household Members and Household Food Insecurity
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- OECD. Building Food Security and Managing Risk in Southeast Asia; OECD Publishing: Paris, France, 2017. [Google Scholar]
- European Commission: DG Agriculture and Rural Development. Global Food Security: Challenges and Options; EU Agricultural Market Briefs: Brussels, Belgium, 2015. [Google Scholar]
- Tandon, S.; Landes, M.; Christensen, C.; LeGrand, S.; Broussard, N.; Farrin, K.; Thome, K. Progress and Challenges in Global Food Security; USDA, Economic Research Service: Washington, DC, USA, 2017.
- FAO; IFAD; UNICEF; WFP; WHO. The State of Food Security and Nutrition in the World 2019: Safeguarding against Economic Slowdowns and Downturns; FAO: Rome, Italy, 2019. [Google Scholar]
- FAO. The State of Food Insecurity in the World 2001; FAO: Rome, Italy, 2002. [Google Scholar]
- Clay, E. Food security: Concepts and Measurement. Paper for FAO Expert Consultation on Trade and Food Security: Conceptualizing the Linkages; FAO: Rome, Italy, 2003. [Google Scholar]
- Coleman-Jensen, A.; Rabbitt, M.P.; Gregory, C.A.; Singh, A. Household Food Security in the United States in 2018; USDA, Economic Research Service: Washington, DC, USA, 2019.
- Bartfeld, J.; Dunifon, R.; Nord, M.; Carlson, S. What Factors Account for State-to-State Differences in Food Security? Economic Information Bulletin NO. 20; USDA: Washington, DC, USA, 2006.
- Kim, K.; Kim, M.K.; Shin, Y.J.; Lee, S.S. Factors related to household food insecurity in the Republic of Korea. Public Health Nutr. 2011, 14, 1080–1087. [Google Scholar] [CrossRef] [Green Version]
- Tarasuk, V.; Vogt, J. Household Food Insecurity in Ontario. Can. J. Public Health 2009, 100, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Krahn, G.L.; Walker, D.K.; Correa-De-Araujo, R. Persons with disabilities as an unrecognized health disparity population. Am. J. Public Health 2015, 105 (Suppl. 2), S198–S206. [Google Scholar] [CrossRef]
- WHO; World Bank. World Report on Disability 2011; WHO: Geneva, Switzerland, 2011. [Google Scholar]
- UN. Report on the World Social Situation 2018: Chapter V Persons with Disabilities: Breaking Down Barriers; UN: New York, NY, USA, 2018; pp. 63–76. [Google Scholar]
- Meisenheimer, M. SNAP Matters for People with Disabilities; Food Research and Action Center: Washington, DC, USA, 2015. [Google Scholar]
- Schwartz, N.; Buliung, R.; Wilson, K. Disability and food access and insecurity: A scoping review of the literature. Health Place 2019, 57, 107–121. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, N.; Tarasuk, V.; Buliung, R.; Wilson, K. Mobility impairments and geographic variation in vulnerability to household food insecurity. Soc. Sci. Med. 2019, 243, 112636. [Google Scholar] [CrossRef] [PubMed]
- Coleman-Jensen, A. U.S. food insecurity and population trends with a focus on adults with disabilities. Physiol. Behav. 2020, 220, 112865. [Google Scholar] [CrossRef]
- Brucker, D.L.; Coleman-Jensen, A. Food Insecurity across the adult life span for persons with disabilities. J. Disabil. Policy Stud. 2017, 28, 109–118. [Google Scholar] [CrossRef]
- Tinson, A.; Ayrton, C.; Barker, K.; Born, T.B.; Aldridge, H.; Kenway, P. Monitoring Poverty and Social Exclusion 2016 (MPSE); Joseph Rowntree Foundation: York, UK, 2016. [Google Scholar]
- Heflin, C.M.; Altman, C.E.; Rodriguez, L.L. Food insecurity and disability in the United States. Disabil. Health J. 2019, 12, 220–226. [Google Scholar] [CrossRef]
- Coleman-Jensen, A.; Nord, M. Food Insecurity among Households with Working-Age Adults with Disabilities; USDA, Economic Research Service: Washington, DC, USA, 2013.
- Heflin, C.; Altman, C.; Rodriguez, L. Having a Disability Increases the Likelihood of Food Insecurity Despite Federal Programs to Prevent this Hardship; Syracuse University Lerner Center for Public Health Promotion, Research Brief No. 10: New York, NY, USA, 2019. [Google Scholar]
- Gundersen, C.; Ziliak, J.P. Food Insecurity and Health Outcomes. Health Aff. 2015, 34, 1830–1839. [Google Scholar] [CrossRef] [Green Version]
- Darling, K.E.; Fahrenkamp, A.J.; Wilson, S.M.; D’Auria, A.L.; Sato, A.F. Physical and mental health outcomes associated with prior food insecurity among young adults. J. Health Psychol. 2017, 22, 572–581. [Google Scholar] [CrossRef]
- Townsend, M.S.; Peerson, J.; Love, B.; Achterberg, C.; Murphy, S.P. Food insecurity is positively related to overweight in women. J. Nutr. 2001, 131, 1738–1745. [Google Scholar] [CrossRef] [Green Version]
- Brucker, D.L. The association of food insecurity with health outcomes for adults with disabilities. Disabil. Health J. 2017, 10, 286–293. [Google Scholar] [CrossRef]
- Coleman-Jensen, A.; Nord, M. Disability is an Important Risk Factor for Food Insecurity; Amber Waves, USDA, Economic Research Service: Washington, DC, USA, 2013.
- Kweon, S.; Kim, Y.; Jang, M.J.; Kim, Y.; Kim, K.; Choi, S.; Chun, C.; Khang, Y.H.; Oh, K. Data resource profile: The Korea National Health and Nutrition Examination Survey (KNHANES). Int. J. Epidemiol. 2014, 43, 69–77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, W.H.; Park, Y.G.; Shin, H.I.; Im, S.H. The World Report on Disability and recent developments in South Korea. Am. J. Phys. Med. Rehabil. 2014, 93, S58–S62. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Hong, S.A.; Kwon, S.O.; Oh, S.Y. Development of Food Security Measures for Korean National Health and Nutrition Examination Survey. Korean J. Nutr. 2011, 44, 551–561. [Google Scholar] [CrossRef] [Green Version]
- Kim, K.; Hong, S.A.; Kwon, S.O.; Choi, B.Y.; Kim, G.-Y.; Oh, S.-Y. Validation of Food Security Measures for the Korean National Health and Nutrition Examination Survey. Korean J. Community Nutr. 2011, 16, 771–781. [Google Scholar] [CrossRef]
- Huang, J.; Guo, B.R.; Kim, Y. Food insecurity and disability: Do economic resources matter? Soc. Sci. Res. 2010, 39, 111–124. [Google Scholar] [CrossRef] [Green Version]
- Borowko, W. Food Insecurity among Working-Age Canadians with Disabilities. Master’s Thesis, Simon Fraser University, Burnaby, BC, Canada, 20 November 2008. [Google Scholar]
- Cho, S.; Ishdorj, A.; Gregory, C. Food Insecurity and Types of Disability. In Proceedings of the Southern Agricultural Economics Association, 2016 Annual Meeting, San Antonio, TX, USA, 6–9 February 2016. [Google Scholar]
- Kim, K.; Kim, M.K.; Shin, Y.-J. Household Food Insecurity and Its Characteristics in Korea. Health Soc. Welf. Rev. 2009, 29, 268–292. [Google Scholar] [CrossRef]
- Porterfield, S.L. Work choices of mothers in families with children with disabilities. J. Marriage Fam. 2002, 64, 972–981. [Google Scholar] [CrossRef]
- She, P.Y.; Livermore, G.A. Material hardship, poverty, and disability among working-age adults. Soc. Sci. Quart. 2007, 88, 970–989. [Google Scholar] [CrossRef] [Green Version]
- UN. Building Disability-Inclusive Societies in Asia and the Pacific: Assessing Progress of the Incheon Strategy; UN: New York, NY, USA, 2018. [Google Scholar]
- Sonik, R.; Parish, S.L.; Ghosh, S.; Igdalsky, L. Food Insecurity in US Households That Include Children with Disabilities. Except. Child. 2016, 83, 42–57. [Google Scholar] [CrossRef] [Green Version]
- Nielsen, R.B.; Garasky, S.; Chatterjee, S. Food Insecurity and Out-of-Pocket Medical Expenditures: Competing Basic Needs? Fam. Consum. Sci. Res. J. 2010, 39, 137–151. [Google Scholar] [CrossRef]
- Waghorn, G.; Lloyd, C. The Employment of People with Mental Illness. AeJAMH 2005, 4, 129–171. [Google Scholar] [CrossRef] [Green Version]
- OECD; EU. The Labour Market Impacts of Ill-Health. In Health at a Glance: Europe 2016: State of Health in the EU Cycle; OECD Publishing: Paris, France, 2016. [Google Scholar]
- CDC. Health and Economic Costs of Chronic Diseases. Available online: https://www.cdc.gov/chronicdisease/about/costs/index.htm#ref1 (accessed on 10 June 2020).
- Griffiths, M.; Naing, A. Disability in Myanmar-Findings from Contemporary Research; Myanmar Social Policy and Poverty Research Group: Yangon, Myanmar, 2016. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Households with PWD | Households without PWD | p Value | |
|---|---|---|---|
| n (%) | n (%) | ||
| Total Households (n = 2690) | 384 (14.3) | 2306 (85.7) | |
| Characteristics of Household Head | |||
| Gender | 0.02 | ||
| Male | 223 (58.1) | 1484 (64.4) | |
| Female | 161 (41.9) | 822 (35.7) | |
| Age, Years | |||
| Mean ± SD | 60.7 ± 13.0 | 53.0 ± 14.7 | <0.001 |
| <40 | 29 (7.6) | 478 (20.7) | <0.001 |
| 40–49 | 45 (11.7) | 549 (23.8) | |
| 50–59 | 98 (25.5) | 487 (21.1) | |
| 60–69 | 89 (23.2) | 400 (17.4) | |
| ≥70 | 123 (32.0) | 392 (17.0) | |
| Marital Status | 0.81 | ||
| Living with Spouse | 283 (73.7) | 1686 (73.1) | |
| Not Living with Spouse | 101 (26.3) | 620 (26.9) | |
| Educational Level | <0.001 | ||
| Middle School Graduate or Less | 209 (54.4) | 717 (31.1) | |
| High School Graduate | 84 (21.9) | 658 (28.5) | |
| College Graduate or More | 51 (13.3) | 668 (29.0) | |
| Unknown | 44 (10.4) | 263 (11.4) | |
| Type of Occupation | <0.001 | ||
| White-Collar Jobs | 43 (11.2) | 510 (22.1) | |
| Blue-Collar Jobs | 131 (34.1) | 894 (38.8) | |
| Unemployed | 170 (44.3) | 635 (27.5) | |
| Unknown | 40 (10.4) | 267 (11.6) | |
| Characteristics of Household | |||
| Household Size (No. of Household Members) | |||
| Mean ± SD | 2.7 ± 1.2 | 2.8 ± 1.2 | 0.13 |
| 1–2 Persons | 206 (53.7) | 1033 (44.8) | 0.003 |
| 3 Persons | 83 (21.6) | 537 (23.3) | |
| ≥4 Persons | 95 (24.7) | 736 (31.9) | |
| Family Type | <0.001 | ||
| One-Person Household | 55 (14.3) | 411 (17.8) | |
| Married Couple | 116 (30.5) | 441 (19.1) | |
| Married Couple and Unmarried Children | 93 (24.2) | 928 (40.2) | |
| Single Parent and Unmarried Children | 30 (7.8) | 243 (10.5) | |
| Three-Generational Household | 43 (11.2) | 123 (5.3) | |
| Other Household Type | 47 (12.2) | 160 (6.9) | |
| Presence of Children Aged ≤18 Years | <0.001 | ||
| No | 287 (74.7) | 1395 (60.5) | |
| Yes | 97 (25.3) | 911 (39.5) | |
| No. of Economically Active Household Members | <0.001 | ||
| None | 154 (40.1) | 650 (28.2) | |
| 1 Person | 136 (35.4) | 961 (41.7) | |
| ≥2 Persons | 94 (24.5) | 695 (30.1) | |
| Household Income (Quartiles) | <0.001 | ||
| First Quartile (Poorest) | 154 (40.3) | 531 (23.1) | |
| Second Quartile | 86 (22.5) | 612 (26.7) | |
| Third Quartile | 79 (20.7) | 555 (24.2) | |
| Fourth Quartile (Richest) | 63 (16.5) | 597 (26.0) | |
| Place of Residence | 0.10 | ||
| Metropolitan Cities | 173 (45.1) | 995 (43.2) | |
| Cities | 119 (31.0) | 837 (36.3) | |
| Rural Areas | 92 (24.0) | 474 (20.6) | |
| Disability-Related Characteristics | |||
| No. of PWD | |||
| 1 Person | 356 (92.7) | ||
| ≥2 Persons | 28 (7.3) | ||
| No. of Working-Age Adults with Disabilities (Aged 19–64 Years) | |||
| None | 185 (48.2) | ||
| 1 Person | 184 (47.9) | ||
| ≥2 Persons | 15 (3.9) | ||
| No. of Economically Active PWD | |||
| None | 247 (64.3) | ||
| 1 Person | 132 (34.4) | ||
| ≥2 Person | 5 (1.3) | ||
| Relationships of PWD to Their Families | |||
| Male Head of Household | 132 (34.4) | ||
| Female Head of Household | 72 (18.8) | ||
| Spouse of Household Head | 87 (22.7) | ||
| Son/Daughter of Household Head | 33 (8.6) | ||
| Other Relative | 34 (8.9) | ||
| Multiple (e.g., Household Head and Spouse, Household Head and Others, and Spouse and Others) | 26 (6.8) | ||
| Type of Disability | |||
| Physical Disability | 240 (62.5) | ||
| Visual Disability | 36 (9.4) | ||
| Auditory or Linguistic Disability | 44 (11.5) | ||
| Mental Disability | 26 (6.8) | ||
| Internal Organ Disability | 18 (4.7) | ||
| Unknown | 20 (5.2) | ||
| Severity of Disability | |||
| Severe (Grades 1–3) | 119 (31.0) | ||
| Mild (Grades 4–6) | 240 (62.5) | ||
| Unknown | 25 (6.5) |
| Households with PWD | Households without PWD | p Value | |
|---|---|---|---|
| n (%) | n (%) | ||
| Participation in Food Assistance Programs during the Last 12 Months | <0.001 | ||
| No | 333 (86.7) | 2158 (93.6) | |
| Yes | 51 (13.3) | 148 (6.4) | |
| Experiences of Food Insufficiency during the Last 12 Months | 0.001 | ||
| Food-Sufficient | 344 (89.6) | 2168 (94.0) | |
| Food-Insufficient | 40 (10.4) | 138 (6.0) | |
| Percentage of Households Reporting Insecurity for Every Indicator of HFI during the Last 12 Months | |||
| The Food that We Bought just did not Last and We did not Have Money to Get More | 42 (10.9) | 182 (7.9) | 0.04 |
| Worried whether Food would Run Out before We Got Money to Buy More | 100 (26.0) | 371 (16.1) | <0.001 |
| Could not Afford to Eat Balanced Meals | 97 (25.3) | 401 (17.4) | <0.001 |
| Cut Size of Meals or Skipped Meals | 12 (3.1) | 54 (2.3) | 0.36 |
| Ate Less than Felt should | 34 (8.9) | 133 (5.8) | 0.02 |
| Hungry but did not Eat Because could not Afford Food | 14 (3.7) | 50 (2.2) | 0.08 |
| Lost Weight Because Not Enough Money for Food | 15 (3.9) | 35 (1.5) | 0.001 |
| Did not Eat for Whole Day because Not Enough Money for Food | 1 (0.3) | 12 (0.5) | 0.50 |
| Household’s Food Security Status | 0.004 | ||
| Food-Secure | 330 (85.9) | 2105 (91.3) | |
| Mildly Food-Insecure | 44 (11.5) | 162 (7.0) | |
| Moderately or Severely Food-Insecure | 10 (2.6) | 39 (1.7) |
| Model 1 a | p Value | Model 2 b | p Value | Model 3 c | p Value | |
|---|---|---|---|---|---|---|
| Adjusted OR (95% CI) d | Adjusted OR (95% CI) d | Adjusted OR (95% CI) d | ||||
| Households without PWD (Reference Group) | 1.00 | 1.00 | ||||
| Households with PWD | ||||||
| All Households with PWD | 1.64 (1.16–2.31) | 0.005 | 1.41 (0.99–2.00) | 0.06 | 1.30 (0.91–1.87) | 0.15 |
| Number of PWD (Per Person) | 1.51 (1.13–2.02) | 0.006 | 1.35 (1.01–1.81) | 0.05 | 1.25 (0.92–1.69) | 0.15 |
| Household Head’s Gender | ||||||
| Male-Headed Households with PWD | 1.20 (0.72–2.01) | 0.48 | 1.11 (0.65–1.87) | 0.57 | 0.96 (0.56–1.65) | 0.32 |
| Female-Headed Households with PWD | 2.11 (1.37–3.25) | 0.007 | 1.68 (1.08–2.59) | 0.06 | 1.63 (1.04–2.55) | 0.04 |
| Household Head’s Disability Status | ||||||
| Households with A Household Head without A Disability | 1.31 (0.73–2.35) | 0.74 | 1.20 (0.66–2.18) | 0.85 | 1.11 (0.61–2.05) | 0.79 |
| Households with A Male Head with A Disability | 1.30 (0.69–2.45) | 0.75 | 1.06 (0.55–2.03) | 0.51 | 0.90 (0.47–1.76) | 0.31 |
| Households with A Female Head with A Disability | 2.37 (1.40–4.02) | 0.02 | 1.99 (1.16–3.39) | 0.05 | 1.98 (1.14–3.43) | 0.03 |
| Containing Working-Age adults with Disabilities (Aged 19–64 Years) | ||||||
| No | 1.16 (0.71–1.90) | 0.34 | 1.04 (0.63–1.71) | 0.31 | 0.98 (0.59–1.63) | 0.30 |
| Yes | 2.23 (1.44–3.44) | 0.003 | 1.84 (1.18–2.88) | 0.02 | 1.70 (1.07–2.70) | 0.04 |
| Containing Economically Active PWD | ||||||
| No | 1.98 (1.35–2.91) | 0.005 | 1.63 (1.09–2.44) | 0.05 | 1.53 (1.01–2.31) | 0.06 |
| Yes | 0.96 (0.49–1.91) | 0.28 | 0.93 (0.46–1.86) | 0.38 | 0.84 (0.41–1.72) | 0.30 |
| Type of Disability | ||||||
| Physical Disability | 1.39 (0.90–2.15) | 0.40 | 1.19 (0.77–1.84) | 0.32 | 1.16 (0.74–1.82) | 0.52 |
| Visual Disability | 2.15 (0.84–5.52) | 0.62 | 1.87 (0.72–4.85) | 0.66 | 1.38 (0.53–3.57) | 0.99 |
| Auditory or Linguistic Disability | 0.44 (0.10–1.89) | 0.04 | 0.45 (0.10–1.92) | 0.06 | 0.47 (0.11–2.04) | 0.10 |
| Mental Disability | 4.19 (1.69–10.36) | 0.04 | 3.87 (1.53–9.78) | 0.04 | 2.81 (1.08–7.28) | 0.12 |
| Internal Organ Disability | 4.65 (1.54–14.09) | 0.05 | 3.93 (1.20–12.86) | 0.08 | 4.38 (1.21–15.79) | 0.05 |
| Severity of Disability | ||||||
| Severe (Grades 1–3) | 2.13 (1.27–3.56) | 0.14 | 1.87 (1.11–3.17) | 0.15 | 1.73 (1.01–2.99) | 0.14 |
| Mild (Grades 4–6) | 1.39 (0.89–2.17) | 0.82 | 1.19 (0.76–1.86) | 0.73 | 1.13 (0.72–1.78) | 0.90 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, J.E.; Kim, S.Y.; Kim, S.H.; Jeoung, E.J.; Park, J.H. Household Food Insecurity: Comparison between Families with and without Members with Disabilities. Int. J. Environ. Res. Public Health 2020, 17, 6149. https://doi.org/10.3390/ijerph17176149
Park JE, Kim SY, Kim SH, Jeoung EJ, Park JH. Household Food Insecurity: Comparison between Families with and without Members with Disabilities. International Journal of Environmental Research and Public Health. 2020; 17(17):6149. https://doi.org/10.3390/ijerph17176149
Chicago/Turabian StylePark, Jong Eun, So Young Kim, Se Hee Kim, Eun Ju Jeoung, and Jong Hyock Park. 2020. "Household Food Insecurity: Comparison between Families with and without Members with Disabilities" International Journal of Environmental Research and Public Health 17, no. 17: 6149. https://doi.org/10.3390/ijerph17176149