
Prevalence, Awareness, Treatment and Control of Diabetes Mellitus—A Population Based Study in Shanghai, China

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Sample
2.2. Data Collection
2.3. Disease Definition
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Participants
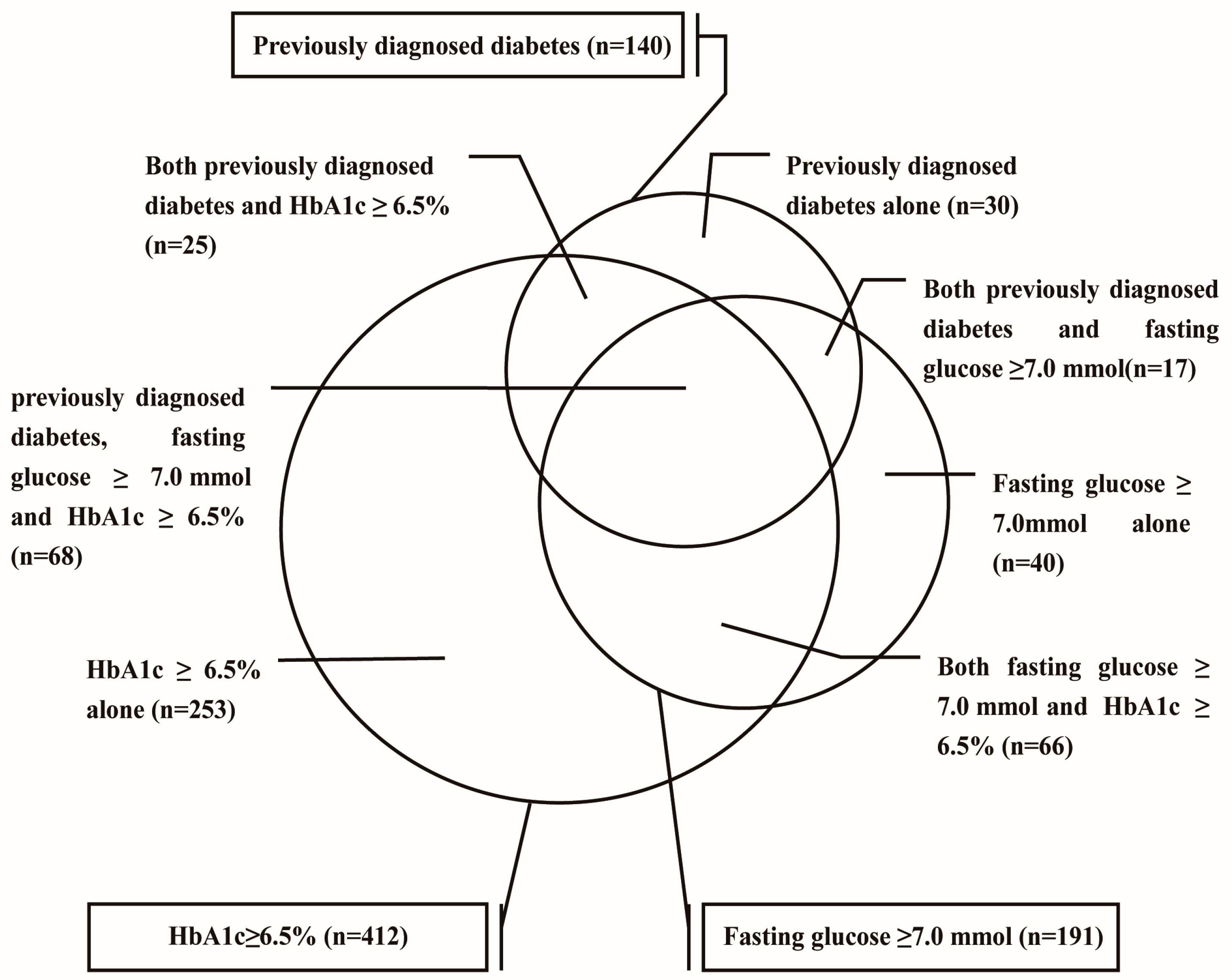
3.2. Prevalences of Diabetes and Prediabetes
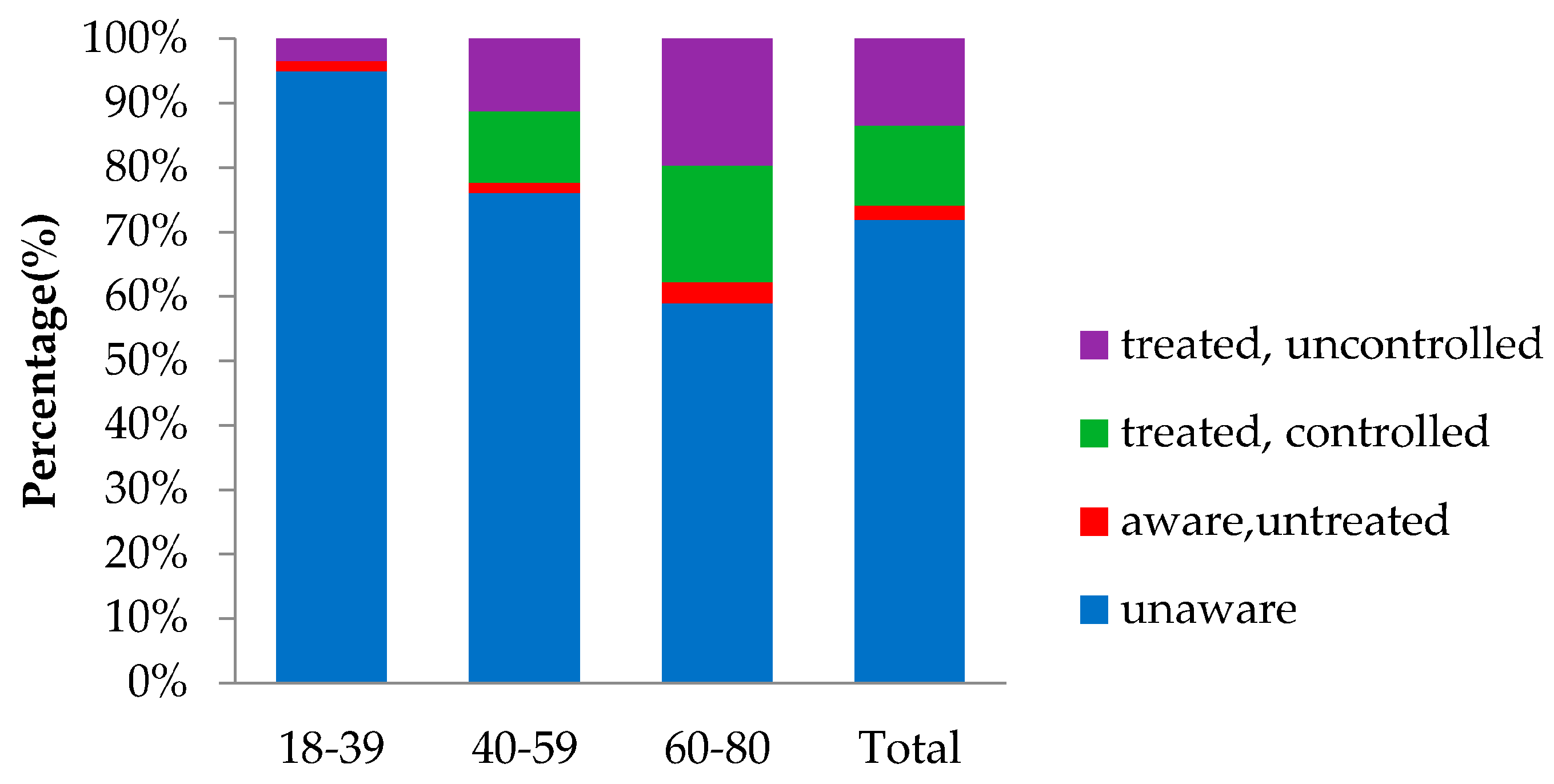
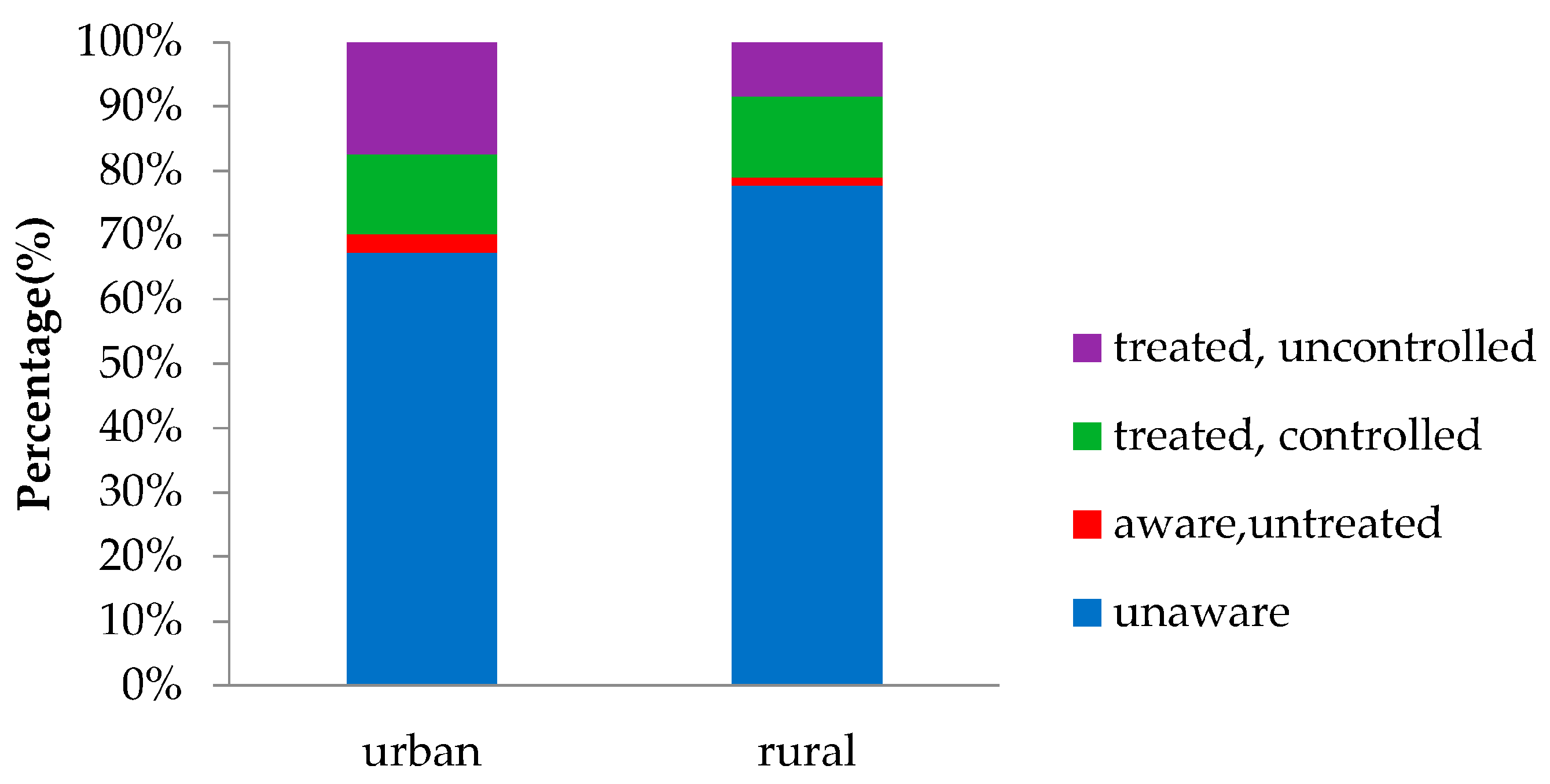
3.3. Awareness, Treatment, and Control of Diabetes
3.4. Associated Factors of Prediabetes and Diabetes
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
| FPG | fasting plasma glucose |
| HbA1c | glycated haemoglobin |
| OGTT | oral glucose-tolerance test |
| BMI | Body mass index |
| ANOVA | analysis of variance |
| SNK-q | Student-Newman-Keuls-q test |
| TC | total cholesterol |
| TG | triglyceride |
| LDL | low-density lipoprotein |
| HDL | high-density lipoprotein |
| GLU | glucose |
| CRP | C-reactive protein |
References
- Pan, C. Diabetes care in China: Meeting the challenge. World Hosp. Health Serv. 2005, 41, 29–30, 32. [Google Scholar] [PubMed]
- He, J.; Gu, D.; Wu, X.; Reynolds, K.; Duan, X.; Yao, C.; Wang, J.; Chen, C.S.; Chen, J.; Wildman, R.P.; et al. Major causes of death among men and women in China. N. Engl. J. Med. 2005, 353, 1124–1134. [Google Scholar] [CrossRef] [PubMed]
- Pan, X.R.; Yang, W.Y.; Li, G.W.; Liu, J. Prevalence of diabetes and its risk factors in China, 1994. National diabetes prevention and control cooperative group. Diabetes Care 1997, 20, 1664–1669. [Google Scholar] [CrossRef] [PubMed]
- National Diabetes Research Group. Diabetes mellitus survey of 300,000 in fourteen provinces and cities of China. Chin. Med. J. 1981, 20, 678–681. [Google Scholar]
- Liu, S.; Wang, W.; Zhang, J.; He, Y.; Yao, C.; Zeng, Z.; Piao, J.; Howard, B.V.; Fabsitz, R.R.; Best, L.; et al. Prevalence of diabetes and impaired fasting glucose in Chinese adults, China national nutrition and health survey, 2002. Prev. Chronic Dis. 2011, 8, A13. [Google Scholar] [PubMed]
- Yang, W.; Lu, J.; Weng, J.; Jia, W.; Ji, L.; Xiao, J.; Shan, Z.; Liu, J.; Tian, H.; Ji, Q.; et al. Prevalence of diabetes among men and women in China. N. Engl. J. Med. 2010, 362, 1090–1101. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Wang, L.; He, J.; Bi, Y.; Li, M.; Wang, T.; Wang, L.; Jiang, Y.; Dai, M.; Lu, J.; et al. Prevalence and control of diabetes in Chinese adults. JAMA 2013, 310, 948–959. [Google Scholar] [CrossRef] [PubMed]
- Li, M.Z.; Su, L.; Liang, B.Y.; Tan, J.J.; Chen, Q.; Long, J.X.; Xie, J.J.; Wu, G.L.; Yan, Y.; Guo, X.J.; et al. Trends in prevalence, awareness, treatment, and control of diabetes mellitus in mainland China from 1979 to 2012. Int. J. Endocrinol. 2013, 2013, 753150. [Google Scholar] [CrossRef] [PubMed]
- Hu, D.; Fu, P.; Xie, J.; Chen, C.S.; Yu, D.; Whelton, P.K.; He, J.; Gu, D. Increasing prevalence and low awareness, treatment and control of diabetes mellitus among Chinese adults: The interASIA study. Diabetes Res. Clin. Pract. 2008, 81, 250–257. [Google Scholar] [CrossRef] [PubMed]
- Gu, D.; Reynolds, K.; Duan, X.; Xin, X.; Chen, J.; Wu, X.; Mo, J.; Whelton, P.K.; He, J. Prevalence of diabetes and impaired fasting glucose in the Chinese adult population: International collaborative study of cardiovascular disease in Asia (Interasia). Diabetologia 2003, 46, 1190–1198. [Google Scholar] [CrossRef] [PubMed]
- Tian, H.; Song, G.; Xie, H.; Zhang, H.; Tuomilehto, J.; Hu, G. Prevalence of diabetes and impaired fasting glucose among 769,792 rural Chinese adults. Diabetes Res. Clin. Pract. 2009, 84, 273–278. [Google Scholar] [CrossRef] [PubMed]
- Wei, W.; Liu, S.Y.; Zeng, F.F.; Yao, S.P.; Zhang, H.T.; Wan, G.; Zhong, M.; Yang, Z.; Wang, B.Y. Type 2 diabetes and impaired glucose tolerance in north-China-based rural community adults. Public Health 2010, 124, 593–601. [Google Scholar] [CrossRef] [PubMed]
- Cowie, C.C.; Rust, K.F.; Ford, E.S.; Eberhardt, M.S.; Byrd-Holt, D.D.; Li, C.; Williams, D.E.; Gregg, E.W.; Bainbridge, K.E.; Saydah, S.H.; et al. Full accounting of diabetes and pre-diabetes in the U.S. population in 1988–1994 and 2005–2006. Diabetes Care 2009, 32, 287–294. [Google Scholar] [CrossRef] [PubMed]
- Yang, F.; Qian, D.; Chen, J.; Hu, D.; Hou, M.; Chen, S.; Wang, P. Prevalence, awareness, treatment and control of diabetes mellitus in rural China: Results from Shandong province. Diabet. Med. 2016, 33, 354–358. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.H.; Ma, W.J.; Thomas, G.N.; Xu, Y.J.; Lao, X.Q.; Xu, X.J.; Song, X.L.; Xu, H.F.; Cai, Q.M.; Xia, L.; et al. Diabetes and pre-diabetes as determined by glycated haemoglobin A1c and glucose levels in a developing southern Chinese population. PLoS ONE 2012, 7, e37260. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Wang, R.; Zhao, Y.; Ma, X.; Fang, J.; Yan, H.; Kang, X.; Yin, P.; Hao, Y.; Li, Q.; et al. Systematic investigation of gastrointestinal diseases in China (SILC): Validation of survey methodology. BMC Gastroenterol. 2009, 9, 86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Fifth Population Census in China. Available online: http://www.stats.gov.cn/tjsj/ndsj/renkoupucha/2000pucha/pucha.htm (accessed on 10 May 2016).
- World Health Organization. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 2004, 363, 157–163. [Google Scholar]
- Association, A.D. Standards of medical care in diabetes—2011. Diabetes Care 2011, 34, S11–S61. [Google Scholar] [CrossRef] [PubMed]
- 2014 National Diabetes Statistics Report. Available online: http://www.cdc.gov/diabetes/data/statistics/2014StatisticsReport.html (accessed on 24 September 2014).
- Hu, F.B. Globalization of diabetes: The role of diet, lifestyle, and genes. Diabetes Care 2011, 34, 1249–1257. [Google Scholar] [CrossRef] [PubMed]
- Hu, F.B.; Manson, J.E.; Stampfer, M.J.; Colditz, G.; Liu, S.; Solomon, C.G.; Willett, W.C. Diet, lifestyle, and the risk of type 2 diabetes mellitus in women. N. Engl. J. Med. 2001, 345, 790–797. [Google Scholar] [CrossRef] [PubMed]
- Jack, L., Jr.; Boseman, L.; Vinicor, F. Aging Americans and diabetes. A public health and clinical response. Geriatrics 2004, 59, 14–17. [Google Scholar] [PubMed]
- Lovejoy, J.C. The influence of dietary fat on insulin resistance. Curr. Diabetes Rep. 2002, 2, 435–440. [Google Scholar] [CrossRef]
- Li, Y.; Shi, X.M.; Hou, P.S. Scientific evidence of diet, nutrition and major chronic non-communicable disease prevention. Chin. J. Prev. Med. 2011, 45, 459–462. [Google Scholar]
- Zhai, F.; Wang, H.; Du, S.; He, Y.; Wang, Z.; Ge, K.; Popkin, B.M. Prospective study on nutrition transition in China. Nutr. Rev. 2009, 67 (Suppl. 1), S56–S61. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.W.; Norton, E.C.; Popkin, B.M. Why have physical activity levels declined among Chinese adults? Findings from the 1991–2006 China health and nutrition surveys. Soc. Sci. Med. 2009, 68, 1305–1314. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Zhao, W.; Wang, W.; Bi, Y.; Li, J.; Mi, S.; Xu, M.; Lu, J.; Wang, T.; Li, M.; et al. Plasma glucose and hemoglobin a1c for the detection of diabetes in Chinese adults. J. Diabetes 2016, 8, 378–386. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Study | Study Period | Sample Size | Age Range | Screening Method | Diagnostic Criteria | Prevalence of Diabetes |
|---|---|---|---|---|---|---|
| Population-based cross-sectional study in 19 provinces and areas in China [3] | 1994–1995 | 213,515 | 25–64 | OGTT, 2hBG, SR | WHO-1985 | 2.5% |
| Nationally representative sample of the general population in China [10] | 2000–2001 | 15,540 | 35–74 | FPG, SR | ADA | 5.35% |
| China National Nutrition and Health Survey [5] | 2002 | 47,729 | 20+ | FPG, SR | ADA-2009 | 2.7% |
| Cross-sectional whole-population health survey in Tianjin rural area [11] | 2004 | 769,792 | 35+ | FBG, SR | WHO-1999 | 9.5% |
| Cross-sectional study on rural residents in North China [12] | 2005 | 1058 | 20+ | OGTT | WHO-1999 | 7.09% |
| National Health and Nutrition Examination Survey in America [13] | 2005–2006 | 2806 | 20+ | OGTT | ADA-1997 | 12.9% |
| China National Diabetes and Metabolic Disorders Study [6] | 2007–2008 | 46,239 | 20+ | OGTT, SR | WHO-1999 | 9.7% |
| Cross-sectional study in Shanghai | 2007–2008 | 3136 | 18–80 | FPG, HbA1c, SR | ADA-2009 | 15.91% |
| Prevalence, awareness, treatment, and control of diabetes mellitus in rural China: results from Shandong Province [14] | 2007 | 16,375 | 25+ | FPG, OGTT | WHO-1999 | 3.5% |
| Guangdong Health Survey [15] | 2010 | 3590 | 18+ | FPG, HbA1c, OGTT | ADA-2009 | 21.7% |
| A cross-sectional survey in a nationally representative sample of 98,658 Chinese adults [7] | 2010 | 98,658 | 18+ | FPG, HbA1c, OGTT | ADA-2010 | 11.6% |
| Cohort | Previously Diagnosed and/or Fasting Plasma Glucose ≥ 7.0 mmol/L and/or HbA1c ≥ 6.5% (Diabetes, n = 499) | Previously Diagnosed Diabetes and/or Fasting Plasma Glucose ≥ 7.0 mmol/L (n = 246) | Previously Diagnosed Diabetes (n = 140) | Fasting Plasma Glucose ≥ 7.0 mmol/L (n = 191) | HbA1c ≥ 6.5% (n = 412) | Prediabetes (n = 1172) |
|---|---|---|---|---|---|---|
| Overall | 15.91 (14.63, 17.19) | 7.84 (6.9, 8.79) | 4.46 (3.74, 5.19) | 6.09 (5.25, 6.93) | 13.14 (11.96, 14.32) | 37.37 (35.68, 39.07) |
| Sex | ||||||
| Female (n = 1743) | 15.15 (13.46, 16.83) | 6.54 (5.38, 7.7) | 3.79 (2.89, 4.68) | 5.05 (4.02, 6.08) | 12.34 (10.79, 13.88) | 40.62 (38.31, 42.93) |
| Male (n = 1393) | 16.87 (14.9, 18.84) | 9.48 (7.94, 11.01) | 5.31 (4.13, 6.49) | 7.39 (6.02, 8.77) | 14.14 (12.31, 15.97) | 33.31 (30.83, 35.78) |
| p-value | 0.190 | 0.002 | 0.040 | 0.006 | 0.137 | <0.001 |
| Age (year) | ||||||
| 18–39 (n = 844) | 7.11 (5.38, 8.84) | 1.66 (0.8, 2.52) | 0.36 (0, 0.76) | 1.42 (0.62, 2.22) | 6.40 (4.75, 8.05) | 29.74 (26.66, 32.82) |
| 40–59 (n = 1651) | 15.20 (13.47, 16.93) | 7.45 (6.18, 8.72) | 3.63 (2.73, 4.54) | 6.06 (4.91, 7.21) | 12.48 (10.88, 14.07) | 41.25 (38.87, 43.62) |
| 60–80 (n = 641) | 29.33 (25.8, 32.85) | 17.00 (14.1, 19.91) | 12.01 (9.5, 14.53) | 12.32 (9.78, 14.87) | 23.71 (20.42, 27.01) | 37.44 (33.69, 41.19) |
| p-value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 |
| Region | ||||||
| Urban (n = 1570) | 17.52 (15.64, 19.4) | 8.41 (7.03, 9.78) | 5.73 (4.58, 6.88) | 6.18 (4.99, 7.37) | 15.16 (13.39, 16.93) | 42.74 (40.29, 45.19) |
| Rural (n = 1566) | 14.30 (12.57, 16.04) | 7.28 (5.99, 8.57) | 3.19 (2.32, 4.06) | 6.00 (4.83, 7.18) | 11.11 (9.55, 12.67) | 31.99 (29.68, 34.3) |
| p-value | 0.014 | 0.240 | <0.001 | 0.837 | <0.001 | <0.001 |
| BMI (kg/m2) | ||||||
| <18.5 (n = 194) | 10.31 (6.03, 14.59) | 2.06 (0.06, 4.06) | 1.55 (0, 3.28) | 1.03 (0, 2.45) | 9.28 (5.2, 13.36) | 34.02 (27.35, 40.69) |
| 18.5~ (n = 1352) | 12.20 (10.46, 13.95) | 5.03 (3.86, 6.19) | 3.18 (2.25, 4.12) | 3.92 (2.89, 4.95) | 10.95 (9.28, 12.61) | 36.46 (33.9, 39.03) |
| 23~ (n = 1260) | 17.54 (15.44, 19.64) | 9.52 (7.9, 11.14) | 5.48 (4.22, 6.73) | 7.22 (5.79, 8.65) | 13.81 (11.9, 15.71) | 38.02 (35.34, 40.7) |
| ≥27.5 (n = 326) | 28.22 (23.34, 33.11) | 16.56 (12.53, 20.6) | 7.67 (4.78, 10.56) | 13.80 (10.06, 17.55) | 21.78 (17.3, 26.26) | 41.10 (35.76, 46.45) |
| p-value | <0.001 | <0.001 | <0.001 | <0.001 | <0.001 | 0.313 |
| Characteristic | Normal Participants (n = 1465) | Prediabetes (n = 1172) | Diabetes (n = 499) |
|---|---|---|---|
| Age | |||
| Mean ± SD | 44.53 ± 13.83 | 49.15 ± 13.39 | 54.09 ± 13.85 |
| Median | 45.00 | 48.00 | 53.00 |
| Q1, Q3 | 35.00, 52.00 | 41.00, 57.00 | 45.00, 65.00 |
| p-value | 1 | <0.001 * | <0.001 * |
| BMI | |||
| Mean ± SD | 22.74 ± 3.16 | 23.44 ± 3.31 | 24.19 ± 3.43 |
| Median | 22.58 | 23.27 | 24.06 |
| Q1, Q3 | 20.42, 24.80 | 21.23, 25.39 | 21.88, 26.13 |
| p-value | 1 | <0.001 * | <0.001 * |
| TC | |||
| Mean ± SD | 4.78 ± 1.42 | 5.03 ± 0.97 | 5.17 ± 1.16 |
| Median | 4.64 | 4.96 | 5.05 |
| Q1, Q3 | 4.15, 5.26 | 4.34, 5.66 | 4.38, 5.73 |
| p-value | 1 | <0.001 * | <0.001 * |
| TG | |||
| Mean ± SD | 1.31 ± 1.01 | 1.52 ± 1.19 | 1.80 ± 1.48 |
| Median | 1.06 | 1.20 | 1.46 |
| Q1, Q3 | 0.75, 1.53 | 0.86, 1.77 | 0.98,2.17 |
| p-value | 1 | <0.001 * | <0.001* |
| HDL | |||
| Mean ± SD | 1.40 ± 0.33 | 1.39 ± 0.33 | 1.33 ± 0.33 |
| Median | 1.35 | 1.34 | 1.27 |
| Q1, Q3 | 1.15, 1.59 | 1.15, 1.58 | 1.09, 1.50 |
| p-value | 1 | 0.69 * | <0.001 * |
| LDL | |||
| Mean ± SD | 3.04 ± 0.80 | 3.27 ± 0.87 | 3.34 ± 0.88 |
| Median | 3.00 | 3.20 | 3.30 |
| Q1, Q3 | 2.50, 3.50 | 2.65, 3.80 | 2.70, 3.90 |
| p-value | 1 | <0.001 * | <0.001 * |
| GLU | |||
| Mean ± SD | 4.74 ± 0.47 | 5.27±0.73 | 6.95 ± 2.65 |
| Median | 4.70 | 5.30 | 6.20 |
| Q1, Q3 | 4.40, 5.10 | 4.70, 5.80 | 5.30, 7.80 |
| p-value | 1 | <0.001 * | <0.001 * |
| HbA1c | |||
| Mean ± SD | 5.28 ± 0.27 | 5.78 ± 0.32 | 7.98 ± 3.64 |
| Median | 5.30 | 5.80 | 7.00 |
| Q1, Q3 | 5.10, 5.50 | 5.70, 6.00 | 6.50, 8.30 |
| p-value | 1 | <0.001 * | <0.001 * |
| CRP | |||
| Mean ± SD | 1.17 ± 2.73 | 1.47±3.30 | 2.46 ± 7.03 |
| Median | 0.47 | 0.61 | 0.91 |
| Q1, Q3 | 0.23, 1.13 | 0.31,1.46 | 0.38, 2.22 |
| p-value | 1 | <0.001 * | <0.001 * |
| Independent Variables | Diabetes | p-Value | Prediabetes | p-Value | ||
|---|---|---|---|---|---|---|
| OR | 95% CI | OR | 95% CI | |||
| Sex | ||||||
| Female | 1 | Ref | 1 | Ref | ||
| Male | 1.61 | 0.86–1.57 | 0.33 | 0.67 | 0.52–0.86 | 0.0019 |
| Age (year) | ||||||
| <40 | 1 | Ref | 1 | Ref | ||
| 40–59 | 2.07 | 1.50–2.86 | <0.001 | 1.96 | 1.59–2.42 | <0.001 |
| 60–80 | 4.73 | 3.26–6.87 | <0.001 | 2.30 | 1.71–3.09 | <0.001 |
| Region | ||||||
| Urban | 1 | Ref | 1 | Ref | ||
| Rural | 1.04 | 0.77–1.41 | 0.11 | 0.60 | 0.50–0.72 | <0.001 |
| BMI (kg/m2) | ||||||
| Low weight (<18.5) | 1.04 | 0.62–1.72 | 0.90 | 0.93 | 0.66–1.30 | 0.65 |
| Normal weight (18.5~) | 1 | Ref | 1 | Ref | ||
| Preobesity (23~) | 1.28 | 1.01–1.62 | 0.04 | 1.04 | 0.87–1.25 | 0.66 |
| Obesity (≥27.5) | 2.34 | 1.71–3.21 | <0.001 | 1.79 | 1.32–2.43 | <0.001 |
| Education | ||||||
| Primary education or below | 1 | Ref | 1 | Ref | ||
| Secondary education | 1.04 | 0.77–1.41 | 0.79 | 0.95 | 0.73–1.23 | 0.69 |
| Higher education | 0.60 | 0.37–0.97 | 0.04 | 1.12 | 0.77–1.61 | 0.56 |
| LDL | 1.06 | 0.91–1.24 | 0.46 | 1.25 | 1.06–1.48 | 0.01 |
| TG | 1.16 | 1.07–1.26 | <0.001 | 1.13 | 1.04–1.24 | 0.01 |
| CRP | 1.05 | 1.02–1.07 | <0.001 | 1.02 | 0.99–1.04 | 0.27 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Qin, Y.; Wang, R.; Ma, X.; Zhao, Y.; Lu, J.; Wu, C.; He, J. Prevalence, Awareness, Treatment and Control of Diabetes Mellitus—A Population Based Study in Shanghai, China. Int. J. Environ. Res. Public Health 2016, 13, 512. https://doi.org/10.3390/ijerph13050512
Qin Y, Wang R, Ma X, Zhao Y, Lu J, Wu C, He J. Prevalence, Awareness, Treatment and Control of Diabetes Mellitus—A Population Based Study in Shanghai, China. International Journal of Environmental Research and Public Health. 2016; 13(5):512. https://doi.org/10.3390/ijerph13050512
Chicago/Turabian StyleQin, Yuchen, Rui Wang, Xiuqiang Ma, Yanfang Zhao, Jian Lu, Cheng Wu, and Jia He. 2016. "Prevalence, Awareness, Treatment and Control of Diabetes Mellitus—A Population Based Study in Shanghai, China" International Journal of Environmental Research and Public Health 13, no. 5: 512. https://doi.org/10.3390/ijerph13050512