
Primary Effusion Lymphoma, Multicentric Castleman’s Disease, and Kaposi’s Sarcoma in an HHV-8 and HIV-Positive Patient: A Case Report
 , , , , , , and
, , , , , , and 
Abstract
:1. Introduction
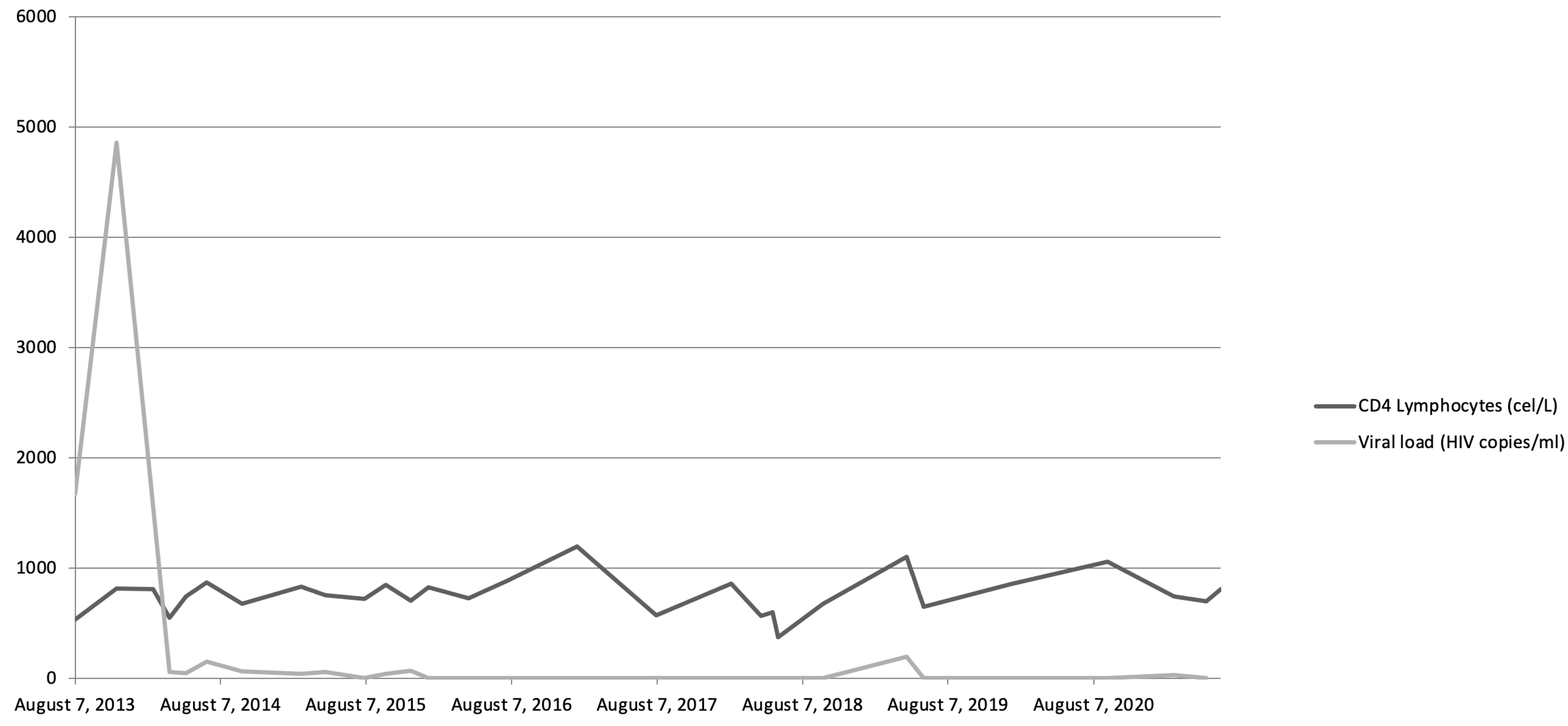
2. Case Presentation
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Liu, C.-Y.; Chen, B.-J.; Chuang, S.-S. Primary Effusion Lymphoma: A Timely Review on the Association with HIV, HHV8, and EBV. Diagnostics 2022, 12, 713. [Google Scholar] [CrossRef] [PubMed]
- Cozzi, I.; Rossi, G.; Rullo, E.; Ascoli, V. Classic KSHV/HHV-8-positive Primary Effusion Lymphoma (PEL): A Systematic Review and Meta-Analysis of Case Reports. Mediterr. J. Hematol. Infect. Dis. 2022, 14, e2022020. [Google Scholar] [CrossRef] [PubMed]
- Chadburn, A.; Said, J.; Gratzinger, D.; Chan, J.K.C.; de Jong, D.; Jaffe, E.S.; Natkunam, Y.; Goodlad, J.R. HHV8/KSHV-Positive Lymphoproliferative Disorders and the Spectrum of Plasmablastic and Plasma Cell Neoplasms: 2015 SH/EAHP Workshop Report-Part 3. Am. J. Clin. Pathol. 2017, 147, 171–187. [Google Scholar] [CrossRef] [PubMed]
- Carbone, A.; Vaccher, E.; Gloghini, A. Hematologic cancers in individuals infected by HIV. Blood 2022, 139, 995–1012. [Google Scholar] [CrossRef]
- Davide, G.; Andrea, C.; Francesco, M.; Elisa, G.; Carmine, P. HIV-related non-Hodgkin Lymphoma. Case report and review of the literature. Acta Bio Med. Atenei Parm. 2018, 89, 576–580. [Google Scholar] [CrossRef]
- Dolcetti, R.; Gloghini, A.; Caruso, A.; Carbone, A. A lymphomagenic role for HIV beyond immune suppression? Blood 2016, 127, 1403–1409. [Google Scholar] [CrossRef]
- Ji, Y.; Lu, H. Malignancies in HIV-Infected and AIDS Patients. In Infectious Agents Associated Cancers: Epidemiology and Molecular Biology; Cai, Q., Yuan, Z., Lan, K., Eds.; Advances in Experimental Medicine and Biology; Springer: Singapore, 2017; pp. 167–179. ISBN 978-981-10-5765-6. [Google Scholar]
- Executive summary of the Consensus Document of GeSIDA and Spanish Secretariat for the National Plan on AIDS on combined antiretroviral treatment in adults infected by the human immunodeficiency virus (January 2013). Enferm. Infecc. Microbiol. Clín. 2013, 31, 604–613. [CrossRef]
- Broussard, G.; Damania, B. Regulation of KSHV Latency and Lytic Reactivation. Viruses 2020, 12, 1034. [Google Scholar] [CrossRef]
- Angius, F.; Ingianni, A.; Pompei, R. Human Herpesvirus 8 and Host-Cell Interaction: Long-Lasting Physiological Modifications, Inflammation and Related Chronic Diseases. Microorganisms 2020, 8, 388. [Google Scholar] [CrossRef]
- Govender, R.D.; Hashim, M.J.; Khan, M.A.; Mustafa, H.; Khan, G. Global Epidemiology of HIV/AIDS: A Resurgence in North America and Europe. J. Epidemiol. Glob. Health 2021, 11, 296–301. [Google Scholar] [CrossRef]
- Infection of KSHV and Interaction with HIV: The Bad Romance | SpringerLink. Available online: https://link.springer.com/chapter/10.1007/978-981-10-5765-6_15 (accessed on 8 September 2022).
- Pantanowitz, L.; Carbone, A.; Dolcetti, R. Microenvironment and HIV-related lymphomagenesis. Semin. Cancer Biol. 2015, 34, 52–57. [Google Scholar] [CrossRef] [PubMed]
- Ibragimova, M.K.; Tsyganov, M.M.; Litviakov, N.V. Natural and chemotherapy-induced clonal evolution of tumors. Biochem. Mosc. 2017, 82, 413–425. [Google Scholar] [CrossRef] [PubMed]
- Dumic, I.; Radovanovic, M.; Igandan, O.; Savic, I.; Nordstrom, C.W.; Jevtic, D.; Subramanian, A.; Ramanan, P. A Fatal Case of Kaposi Sarcoma Immune Reconstitution Syndrome (KS-IRIS) Complicated by Kaposi Sarcoma Inflammatory Cytokine Syndrome (KICS) or Multicentric Castleman Disease (MCD): A Case Report and Review. Am. J. Case Rep. 2020, 21, e926433-1–e926433-7. [Google Scholar] [CrossRef]
- Polizzotto, M.N.; Uldrick, T.S.; Wyvill, K.M.; Aleman, K.; Marshall, V.; Wang, V.; Whitby, D.; Pittaluga, S.; Jaffe, E.S.; Millo, C.; et al. Clinical Features and Outcomes of Patients With Symptomatic Kaposi Sarcoma Herpesvirus (KSHV)-associated Inflammation: Prospective Characterization of KSHV Inflammatory Cytokine Syndrome (KICS). Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2016, 62, 730–738. [Google Scholar] [CrossRef] [PubMed]
- Cesarman, E.; Chadburn, A.; Rubinstein, P.G. KSHV/HHV8-mediated hematologic diseases. Blood 2022, 139, 1013–1025. [Google Scholar] [CrossRef]
- Narkhede, M.; Arora, S.; Ujjani, C. Primary effusion lymphoma: Current perspectives. OncoTargets Ther. 2018, 11, 3747–3754. [Google Scholar] [CrossRef]
- Castillo, J.J.; Bibas, M.; Miranda, R.N. The biology and treatment of plasmablastic lymphoma. Blood 2015, 125, 2323–2330. [Google Scholar] [CrossRef]
- Chen, B.-J.; Chuang, S.-S. Lymphoid Neoplasms with Plasmablastic Differentiation: A Comprehensive Review and Diagnostic Approaches. Adv. Anat. Pathol. 2020, 27, 61–74. [Google Scholar] [CrossRef]
- Won, J.-H.; Han, S.-H.; Bae, S.-B.; Kim, C.-K.; Lee, N.-S.; Lee, K.-T.; Park, S.-K.; Hong, D.-S.; Lee, D.-W.; Park, H.-S. Successful eradication of relapsed primary effusion lymphoma with high-dose chemotherapy and autologous stem cell transplantation in a patient seronegative for human immunodeficiency virus. Int. J. Hematol. 2006, 83, 328–330. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.; Liang, S.; Quan, X.; Guo, B.; Huang, D.; Li, J.; Liu, Y. HIV-associated Burkitt lymphoma in the combination antiretroviral therapy era: Real-world outcomes and prognostication. EJHaem 2022, 4, 100–107. [Google Scholar] [CrossRef]
- Lim, K.J.C.; Di Ciaccio, P.; Polizzotto, M.N.; Milliken, S.; Cochrane, T.; Goh, Z.; Shaw, B.; Perry, E.; Gilbertson, M.; Kermode, W.; et al. Outcomes of human immunodeficiency virus-associated Burkitt lymphoma and diffuse large B-cell lymphoma treated in Australia: A report from the Australasian Lymphoma Alliance. Br. J. Haematol. 2023, 201, 865–873. [Google Scholar] [CrossRef] [PubMed]
- Lurain, K.; Ramaswami, R.; Mangusan, R.; Widell, A.; Ekwede, I.; George, J.; Ambinder, R.; Cheever, M.; Gulley, J.L.; Goncalves, P.H.; et al. Use of pembrolizumab with or without pomalidomide in HIV-associated non-Hodgkin’s lymphoma. J. Immunother. Cancer 2021, 9, e002097. [Google Scholar] [CrossRef] [PubMed]
- Gathers, D.A.; Galloway, E.; Kelemen, K.; Rosenthal, A.; Gibson, S.E.; Munoz, J. Primary Effusion Lymphoma: A Clinicopathologic Perspective. Cancers 2022, 14, 722. [Google Scholar] [CrossRef] [PubMed]
- Uldrick, T.S.; Polizzotto, M.N.; Aleman, K.; Wyvill, K.M.; Marshall, V.; Whitby, D.; Wang, V.; Pittaluga, S.; O’Mahony, D.; Steinberg, S.M.; et al. Rituximab plus liposomal doxorubicin in HIV-infected patients with KSHV-associated multicentric Castleman disease. Blood 2014, 124, 3544–3552. [Google Scholar] [CrossRef]
- Shah, N.N.; Singavi, A.K.; Harrington, A. Daratumumab in Primary Effusion Lymphoma. N. Engl. J. Med. 2018, 379, 689–690. [Google Scholar] [CrossRef]
- Tan, C.R.; Barta, S.K.; Lensing, S.Y.; Noy, A. A Multicenter, Open-Label Feasibility Study of Daratumumab with Dose-Adjusted EPOCH in Newly Diagnosed Plasmablastic Lymphoma: AIDS Malignancy Consortium 105. Blood 2019, 134, 1595. [Google Scholar] [CrossRef]
- Ricker, E.C.; Ryu, Y.K.; Amengual, J.E. Daratumumab Plus Chemotherapy Induces Complete Responses in a Consecutive Series of Four Patients with Plasmablastic Lymphoma. Blood 2021, 138, 4573. [Google Scholar] [CrossRef]
- Casper, C.; Krantz, E.M.; Corey, L.; Kuntz, S.R.; Wang, J.; Selke, S.; Hamilton, S.; Huang, M.-L.; Wald, A. Valganciclovir for suppression of human herpesvirus-8 replication: A randomized, double-blind, placebo-controlled, crossover trial. J. Infect. Dis. 2008, 198, 23–30. [Google Scholar] [CrossRef]
- Casper, C.; Nichols, W.G.; Huang, M.-L.; Corey, L.; Wald, A. Remission of HHV-8 and HIV-associated multicentric Castleman disease with ganciclovir treatment. Blood 2004, 103, 1632–1634. [Google Scholar] [CrossRef]
- Plachouri, K.-M.; Oikonomou, C.; Sarantopoulos, A.; Koumoundourou, D.; Georgiou, S.; Spiliopoulos, T. Successful treatment and durable remission of human herpesvirus-8-induced Kaposi sarcoma and multicentric Castleman’s disease under valganciclovir in an HIV-negative patient. Dermatol. Ther. 2020, 33, e13419. [Google Scholar] [CrossRef]
- Bower, M. How I treat HIV-associated multicentric Castleman disease. Blood 2010, 116, 4415–4421. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Disease Distribution | Extranodal |
|---|---|
| Viral infection | HIV, HHV-8 |
| Positive markers | CD-138 |
| Negative markers | CD20, CD3, EBER |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Caballero, J.C.; Pardo, L.; Rodriguez-Pinilla, M.S.; Piris, M.A.; Alvarez, B.; Solan, L.; Cornago, J.; Lopez-Lorenzo, J.L.; Llamas, P.; Cordoba, R.; et al. Primary Effusion Lymphoma, Multicentric Castleman’s Disease, and Kaposi’s Sarcoma in an HHV-8 and HIV-Positive Patient: A Case Report. Medicina 2023, 59, 1049. https://doi.org/10.3390/medicina59061049
Caballero JC, Pardo L, Rodriguez-Pinilla MS, Piris MA, Alvarez B, Solan L, Cornago J, Lopez-Lorenzo JL, Llamas P, Cordoba R, et al. Primary Effusion Lymphoma, Multicentric Castleman’s Disease, and Kaposi’s Sarcoma in an HHV-8 and HIV-Positive Patient: A Case Report. Medicina. 2023; 59(6):1049. https://doi.org/10.3390/medicina59061049
Chicago/Turabian StyleCaballero, Juan Carlos, Laura Pardo, Maria Socorro Rodriguez-Pinilla, Miguel Angel Piris, Beatriz Alvarez, Laura Solan, Javier Cornago, Jose Luis Lopez-Lorenzo, Pilar Llamas, Raul Cordoba, and et al. 2023. "Primary Effusion Lymphoma, Multicentric Castleman’s Disease, and Kaposi’s Sarcoma in an HHV-8 and HIV-Positive Patient: A Case Report" Medicina 59, no. 6: 1049. https://doi.org/10.3390/medicina59061049