
Longitudinal Change in Brain Functional Connectivity with Herpes Zoster Patients: Neuroimaging Case Series

Abstract
:1. Introduction
2. Case Report
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Denk, F.; McMahon, S.B.; Tracey, I. Pain vulnerability: A neurobiological perspective. Nat. Neurosci. 2014, 17, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.H.; Son, J.H.; Kim, Y.C. Neuroimaging studies of chronic pain. Korean J. Pain 2010, 23, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Gu, L.; Huang, Q.; Hong, S.; Zeng, X.; Zhang, D.; Zhou, F.; Jiang, J. Altered gray matter volume in patients with herpes zoster and postherpetic neuralgia. J. Pain Res. 2019, 12, 605–616. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Huang, X.; Sang, K.; Bodner, M.; Ma, K.; Dong, X.W. Modulation of prefrontal connectivity in postherpetic neuralgia patients with chronic pain: A resting-state functional magnetic resonance-imaging study. J. Pain Res. 2018, 11, 2131–2144. [Google Scholar] [CrossRef] [PubMed]
- Tzourio-Mazoyer, N.; Landeau, B.; Papathanassiou, D.; Crivello, F.; Etard, O.; Delcroix, N.; Mazoyer, B.; Joliot, M. Automated anatomical labeling of activations in SPM using a macroscopic anatomical parcellation of the MNI MRI single-subject brain. Neuroimage 2002, 15, 273–289. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.; Gu, L.; Bao, D.; Hong, S.; He, W.; Tan, Y.; Zeng, X.; Gong, H.; Zhang, D.; Zhou, F. Altered homotopic connectivity in postherpetic neuralgia: A resting state fMRI study. J. Pain Res. 2016, 9, 877–886. [Google Scholar] [CrossRef] [PubMed]
- Fu, W.-L.; Tao, W.; Chen, F.-Y. Altered Functional Connectivity of The Amygdala in Postherpetic Neuralgia. Prog. Biochem. Biophys. 2018, 45, 841–852. [Google Scholar]
- Hong, S.; Gu, L.; Zhou, F.; Liu, J.; Huang, M.; Jiang, J.; He, L.; Gong, H.; Zeng, X. Altered functional connectivity density in patients with herpes zoster and postherpetic neuralgia. J. Pain Res. 2018, 11, 881–888. [Google Scholar] [CrossRef] [PubMed]
- Kouneiher, F.; Charron, S.; Koechlin, E. Motivation and cognitive control in the human prefrontal cortex. Nat. Neurosci. 2009, 12, 939–945. [Google Scholar] [CrossRef]
- Baliki, M.N.; Chang, P.C.; Baria, A.T.; Centeno, M.V.; Apkarian, A.V. CORRIGENDUM: Resting-state functional reorganization of the rat limbic system following neuropathic injury. Sci. Rep. 2015, 5, 7603. [Google Scholar] [CrossRef]
- Bilbao, A.; Falfan-Melgoza, C.; Leixner, S.; Becker, R.; Singaravelu, S.K.; Sack, M.; Sartorius, A.; Spanagel, R.; Weber-Fahr, W. Longitudinal Structural and Functional Brain Network Alterations in a Mouse Model of Neuropathic Pain. Neuroscience 2018, 387, 104–115. [Google Scholar] [CrossRef] [PubMed]
- Mutso, A.A.; Petre, B.; Huang, L.; Baliki, M.N.; Torbey, S.; Herrmann, K.M.; Schnitzer, T.J.; Apkarian, A.V. Reorganization of hippocampal functional connectivity with transition to chronic back pain. J. Neurophysiol. 2014, 111, 1065–1076. [Google Scholar] [CrossRef] [PubMed]
- du Boisgueheneuc, F.; Levy, R.; Volle, E.; Seassau, M.; Duffau, H.; Kinkingnehun, S.; Samson, Y.; Zhang, S.; Dubois, B. Functions of the left superior frontal gyrus in humans: A lesion study. Brain 2006, 129, 3315–3328. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Li, W.; Zhang, T.; Zhang, J.; Jin, Z.; Li, L. Probing the role of the right inferior frontal gyrus during Pain-Related empathy processing: Evidence from fMRI and TMS. Hum. Brain Mapp. 2021, 42, 1518–1531. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, J.T.; Seminowicz, D.A. Neuroimaging of pain in animal models: A review of recent literature. Pain Rep. 2019, 4, e732. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Case 1 | Case 2 | Case 3 | Case 4 | Case 5 | ||
|---|---|---|---|---|---|---|
| Age, yr | 54 | 71 | 44 | 65 | 54 | |
| Sex, M/F | M | F | F | F | M | |
| Location of lesion | Right T4 | Right T5 | Right T4 | Right T6 | Right T10 | |
| NRS | 0-month | 8 | 7 | 8 | 6 | 10 |
| 3-month | 0 | 0 | 2 | 2 | 3 | |
| DN4 | 0-month | 5 | 5 | 9 | 8 | 7 |
| 3-month | 2 | 2 | 3 | 2 | 2 | |
| BDI | 0-month | 32 | 33 | 40 | 25 | 36 |
| 3-month | 31 | 29 | 39 | 23 | 36 | |
| SF-MPQ | 0-month | 44 | 51 | 61 | 44 | 56 |
| 3-month | 23 | 20 | 31 | 24 | 29 | |
| CPT, µA | 0-month | 13.6 | 22.1 | 14.8 | 16.0 | 20.8 |
| 3-month | 12.4 | 21.6 | 11.8 | 10.0 | 10.6 | |
| Development of PHN, Y/S | N | N | Y | Y | Y | |
| Regions | ROIs | |
|---|---|---|
| Central region | ||
| Postcentral gyrus | ||
| Frontal lobe | ||
| Lateral surface | Superior frontal gyrus, dorsolateral (SFG_dors) | |
| Middle frontal gyrus, lateral (MFG_lat) | ||
| Inferior frontal gyrus, opercular part (IFG_oper) | ||
| Inferior frontal gyrus, triangular part (IFG_tri) | ||
| Orbital surface | Superior frontal gyrus, orbital part (SFG_orb) | |
| Middle frontal gyrus, orbital part (MFG_orb) | ||
| Inferior frontal gyrus, orbital part (IFG_orb) | ||
| Temporal lobe | ||
| Lateral surface | Inferior temporal gyrus (ITG) | |
| Parietal lobe | ||
| Medial surface | Precuneus | |
| Limbic lobe | ||
| Hippocampus | ||
| Parahippocampal gyrus | ||
| Insula | ||
| Insula | ||
| Subcortical gray nuclei | ||
| Amygdala | ||
| Caudate nucleus | ||
| Putamen | ||
| Globus pallidus | ||
| Thalamus | ||
| Cases | Suppression | No Change | Activation |
|---|---|---|---|
| Recovery group (1, 2) | N/A | SFG(L)_orb–MFG(L)_orb Precuneus(L)–Precuneus(R) SFG(R)_dors–MFG(R)_lat | Postcentral gyrus(L)–Postcentral gyrus(R) IFG(R)_oper–IFG(R)_tri |
| PHN group (3, 4, 5) | N/A | SFG(L)_dors–SFG(R)_dors MFG(L)_lat–IFG(L)_tri Precuneus(L)–Precuneus(R) SFG(R)_dors–MFG(R)_lat | SFG(L)_orb–IFG(R)_orb |
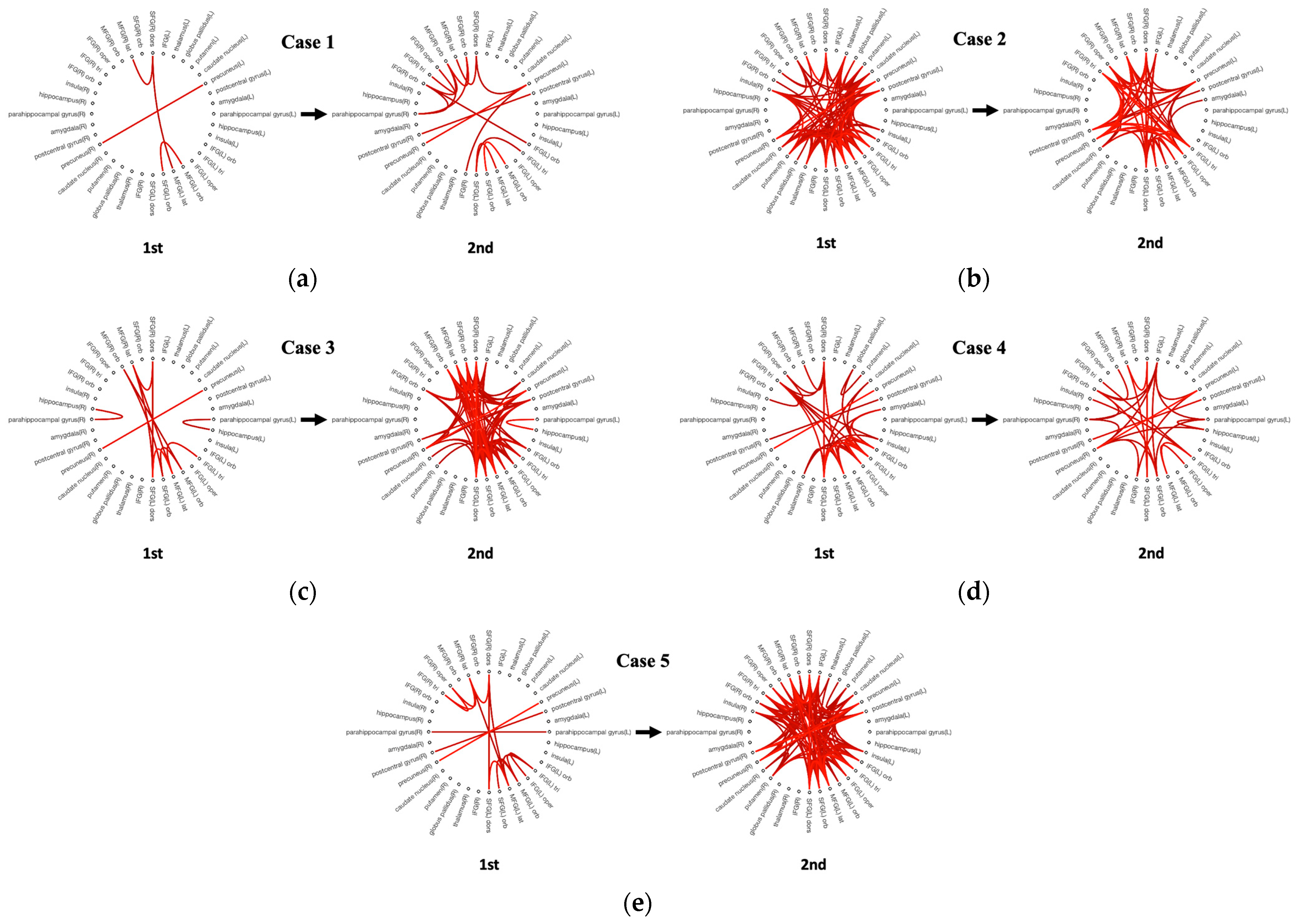
| Case 1 | Case 2 | Case 3 | Case 4 | Case 5 | |
|---|---|---|---|---|---|
| Intra-hemispheric connectivity | |||||
| 0-month, n | 2 | 47 | 6 | 22 | 10 |
| 3-month, n | 10 | 31 | 41 | 12 | 59 |
| 3-month–0-month, n | 8 | −16 | 35 | −10 | 49 |
| Inter-hemispheric connectivity | |||||
| 0-month, n | 2 | 43 | 6 | 13 | 7 |
| 3-month, n | 5 | 24 | 37 | 13 | 48 |
| 3-month–0-month, n | 3 | −9 | 31 | 0 | 41 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, C.; Kim, J.; Chang, H.; Hong, D.; Hong, S.; Moon, H. Longitudinal Change in Brain Functional Connectivity with Herpes Zoster Patients: Neuroimaging Case Series. Medicina 2023, 59, 1045. https://doi.org/10.3390/medicina59061045
Kim C, Kim J, Chang H, Hong D, Hong S, Moon H. Longitudinal Change in Brain Functional Connectivity with Herpes Zoster Patients: Neuroimaging Case Series. Medicina. 2023; 59(6):1045. https://doi.org/10.3390/medicina59061045
Chicago/Turabian StyleKim, Changjae, Joongbaek Kim, Hyunjae Chang, Dakyung Hong, Sanghyun Hong, and Hosik Moon. 2023. "Longitudinal Change in Brain Functional Connectivity with Herpes Zoster Patients: Neuroimaging Case Series" Medicina 59, no. 6: 1045. https://doi.org/10.3390/medicina59061045