
Short-Term Effect of Conventional Versus Accelerated Corneal Cross-Linking Protocol on Corneal Geography and Stability
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Methods
2.1. Ethics
2.2. Subjects and Study Details
2.3. Statistical Analyses
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hersh, P.S.; Stulting, R.D.; Muller, D.; Durrie, D.S.; Rajpal, R.K.; United States Crosslinking Study Group. United States multicenter clinical trial of corneal collagen crosslinking for keratoconus treatment. Ophthalmology 2017, 124, 1259–1270. [Google Scholar] [CrossRef] [PubMed]
- Krachmer, J.H.; Feder, R.S.; Belin, M.W. Keratoconus and related noninflammatory corneal thinning disorders. Surv. Ophthalmol. 1984, 28, 293–322. [Google Scholar] [CrossRef] [PubMed]
- Rabinowitz, Y.S. Keratoconus. Surv. Ophthalmol. 1998, 42, 297–319. [Google Scholar] [CrossRef] [PubMed]
- Wollensak, G.; Spoerl, E.; Seiler, T. Riboflavin/Ultraviolet-Ainduced Collagen Crosslinking for the Treatment of Keratoconus. Am. J. Ophthalmol. 2003, 135, 620–627. [Google Scholar] [CrossRef]
- Beckman, K.A.; Gupta, P.K.; Farid, M.; Berdahl, J.P.; Yeu, E.; Ayres, B.; Chan, C.C.; Gomes, J.A.P.; Holland, E.J.; Kim, T.; et al. ASCRS Cornea Clinical Committee. Corneal crosslinking: Current protocols and clinical approach. J. Cataract Refract. Surg. 2019, 45, 1670–1679. [Google Scholar] [CrossRef]
- Wang, Y.M.; Chan, T.C.; Yu, M.C.Y.; Jhanji, V. Comparative evaluation of progression rate in keratoconus before and after collagen crosslinking. Br. J. Ophthalmol. 2018, 102, 1109–1113. [Google Scholar] [CrossRef]
- Koller, T.; Iseli, H.P.; Hafezi, F.; Vinciguerra, P.; Seiler, T. Scheimpflug imaging of corneas after collagen cross-linking. Cornea 2009, 28, 510–515. [Google Scholar] [CrossRef] [PubMed]
- Danesh, Z.; Sedaghat, M.R.; Momeni-Moghaddam, H.; Yekta, A.A.; Belin, M.W. Corneal Stability and Visual Acuity 1 Year After Corneal Cross-linking Assessed Using the ABCD Keratoconus Staging System. J. Refract. Surg. 2021, 37, 700–706. [Google Scholar] [CrossRef] [PubMed]
- Cınar, Y.; Cingü, A.K.; Türkcü, F.M.; Çınar, T.; Yüksel, H.; Özkurt, Z.G.; Çaçaet, I. Comparison of accelerated and conventional corneal collagen cross-linking for progressive keratoconus. Cutan. Ocul. Toxicol. 2014, 33, 218–222. [Google Scholar] [CrossRef]
- Caruso, C.; Costagliola, C.; Troisi, S.; Epstein, R.L. Compaction of very thin corneas from ultraviolet A riboflavin-vitamin E transepithelial cross-linking. Exp. Eye Res. 2021, 205, 108484. [Google Scholar] [CrossRef] [PubMed]
- Randleman, J.B.; Khandelwal, S.S.; Hafezi, F. Corneal cross-linking. Surv. Ophthalmol. 2015, 60, 509–523. [Google Scholar] [CrossRef] [PubMed]
- Wollensak, G.; Spoerl, E.; Seiler, T. Stress-strain measurements of human and porcine corneas after riboflavin-ultraviolet-A-induced cross-linking. J. Cataract Refract. Surg. 2003, 29, 1780–1785. [Google Scholar] [CrossRef] [PubMed]
- Hagem, A.M.; Thorsrud, A.; Sandvik, G.F.; Drolsum, L. Randomized Study of Collagen Cross-Linking with Conventional Versus Accelerated UVA Irradiation Using Riboflavin with Hydroxypropyl Methylcellulose: Two-Year Results. Cornea 2019, 38, 203–209. [Google Scholar] [CrossRef] [PubMed]
- Hagem, A.M.; Thorsrud, A.; Sandvik, G.F.; Råen, M.; Drolsum, L. Collagen crosslinking with conventional and accelerated ultraviolet-A irradiation using riboflavin with hydroxypropyl methylcellulose. J. Cataract Refract. Surg. 2017, 43, 511–517. [Google Scholar] [CrossRef] [PubMed]
- Kobashi, H.; Tsubota, K. Accelerated Versus Standard Corneal Cross-Linking for Progressive Keratoconus: A Meta-Analysis of Randomized Controlled Trials. Cornea 2020, 39, 172–180. [Google Scholar] [CrossRef]
- Lang, P.Z.; Hafezi, N.L.; Khandelwal, S.S.; Torres-Netto, E.A.; Hafezi, F.; Randleman, J.B. Comparative Functional Outcomes After Corneal Crosslinking Using Standard, Accelerated, and Accelerated With Higher Total Fluence Protocols. Cornea 2019, 38, 433–441. [Google Scholar] [CrossRef] [PubMed]
- Shajari, M.; Kolb, C.M.; Agha, B.; Steinwender, G.; Müller, M.; Herrmann, E.; Schmack, I.; Mayer, W.J.; Kohnen, T. Comparison of standard and accelerated corneal cross-linking for the treatment of keratoconus: A meta-analysis. Acta Ophthalmol. 2019, 97, 22–35. [Google Scholar] [CrossRef]
- Cummings, A.B.; McQuaid, R.; Naughton, S.; Brennan, E.; Mrochen, M. Optimizing Corneal Cross-Linking in the Treatment of Keratoconus: A Comparison of Outcomes After Standard- and High-Intensity Protocols. Cornea 2016, 35, 814–822. [Google Scholar] [CrossRef]
- Shetty, R.; Pahuja, N.K.; Nuijts, R.M.; Ajani, A.; Jayadev, C.; Sharma, C.; Nagaraja, H. Current Protocols of Corneal Collagen Cross-Linking: Visual, Refractive, and Tomographic Outcomes. Am. J. Ophthalmol. 2015, 160, 243–249. [Google Scholar] [CrossRef]
- Ostacolo, C.; Caruso, C.; Tronino, D.; Troisi, S.; Laneri, S.; Pacente, L.; Del Prete, A.; Sacchi, A. Enhancement of corneal permeation of riboflavin-5’-phosphate through vitamin E TPGS: A promising approach in corneal trans-epithelial cross linking treatment. Int. J. Pharm. 2013, 440, 148–153. [Google Scholar] [CrossRef]
- Caruso, C.; Ostacolo, C.; Epstein, R.L.; Barbaro, G.; Troisi, S.; Capobianco, D. Transepithelial Corneal Cross-Linking With Vitamin E-Enhanced Riboflavin Solution and Abbreviated, Low-Dose UV-A: 24-Month Clinical Outcomes. Cornea 2016, 35, 145–150. [Google Scholar] [CrossRef]
- Caruso, C.; Barbaro, G.; Epstein, R.L.; Tronino, D.; Ostacolo, C.; Sacchi, A.; Pacente, L.; Del Prete, A.; Sala, M.; Troisi, S. Corneal Cross-Linking: Evaluating the Potential for a Lower Power, Shorter Duration Treatment. Cornea 2016, 35, 659–662. [Google Scholar] [CrossRef]
- Caruso, C.; Epstein, R.L.; Ostacolo, C.; Pacente, L.; Troisi, S.; Barbaro, G. Customized Corneal Cross-Linking-A Mathematical Model. Cornea 2017, 36, 600–604. [Google Scholar] [CrossRef]
- Rubinfeld, R.S.; Caruso, C.; Ostacolo, C. Corneal Cross-Linking: The Science Beyond the Myths and Misconceptions. Cornea 2019, 38, 780–790. [Google Scholar] [CrossRef]
- Rubinfeld, R.S.; Caruso, C.; Ostacolo, C. Reassessing transepithelial corneal crosslinking. J. Cataract Refract. Surg. 2019, 45, 535–536. [Google Scholar] [CrossRef] [PubMed]
- Caruso, C.; Epstein, R.L.; Troiano, P.; Ostacolo, C.; Barbaro, G.; Pacente, L.; Bartollino, S.; Costagliola, C. Topography and Pachymetry Guided, Rapid Epi-on Corneal Cross-Linking for Keratoconus: 7-year Study Results. Cornea 2020, 39, 56–62. [Google Scholar] [CrossRef]
- Caruso, C.; Epstein, R.L.; Troiano, P.; Napolitano, F.; Scarinci, F.; Costagliola, C. Topo-Pachimetric Accelerated Epi-On Cross-Linking Compared to the Dresden Protocol Using Riboflavin with Vitamin E TPGS: Results of a 2-Year Randomized Study. J. Clin. Med. 2021, 10, 3799. [Google Scholar] [CrossRef] [PubMed]
- Brittingham, S.; Tappeiner, C.; Frueh, B.E. Corneal cross-linking in keratoconus using the standard and rapid treatment protocol: Differences in demarcation line and 12-month outcomes. Investig. Ophthalmol. Vis. Sci. 2014, 55, 8371–8376. [Google Scholar] [CrossRef]
- Ng, A.L.; Chan, T.C.; Cheng, A.C. Conventional versus accelerated corneal collagen cross-linking in the treatment of keratoconus. Clin. Exp. Ophthalmol. 2016, 44, 8–14. [Google Scholar] [CrossRef]
- Kymionis, G.D.; Tsoulnaras, K.I.; Grentzelos, M.A.; Plaka, A.D.; Mikropoulos, D.G.; Liakopoulos, D.A.; Tsakalis, N.G.; Pallikaris, I.G. Corneal stroma demarcation line after standard and high-intensity collagen crosslinking determined with anterior segment optical coherence tomography. J. Cataract Refract. Surg. 2014, 40, 736–740. [Google Scholar] [CrossRef] [PubMed]
- Tomita, M.; Mita, M.; Huseynova, T. Accelerated versus conventional corneal collagen crosslinking. J. Cataract Refract. Surg. 2014, 40, 1013–1020. [Google Scholar] [CrossRef]
- Belin, M.W.; Duncan, J.K. Keratoconus: The ABCD Grading System. Klin. Monbl. Surg. 2012, 28, 645–649. [Google Scholar] [CrossRef] [PubMed]
- Toprak, I.; Yaylali, V.; Yildirim, C. A combination of topographic and pachymetric parameters in keratoconus diagnosis. Contact Lens Anterior Eye 2015, 38, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Kránitz, K.; Kovács, I.; Miháltz, K.; Sándor, G.L.; Knorz, M.C.; Németh, J.; Nagy, Z.Z. Corneal changes in progressive keratoconus after cross-linking assessed by Scheimpflug camera. J. Refract. Surg. 2012, 28, 645–649. [Google Scholar] [CrossRef]
- Flockerzi, E.; Xanthopoulou, K.; Goebels, S.C.; Zemova, E.; Razafimino, S.; Hamon, L.; Jullien, T.; Klühspies, U.; Eppig, T.; Langenbucher, A.; et al. Keratoconus staging by decades: A baseline ABCD classification of 1000 patients in the Homburg Keratoconus Center. Br. J. Ophthalmol. 2021, 105, 1069–1075. [Google Scholar] [CrossRef] [PubMed]
- Soeters, N.; van der Valk, R.; Tahzib, N.G. Corneal cross-linking for treatment of progressive keratoconus in various age groups. J. Refract. Surg. 2014, 30, 454–460. [Google Scholar] [CrossRef] [PubMed]
- Tian, M.; Ma, P.; Zhou, W.; Feng, J.; Mu, G. Outcomes of corneal crosslinking for central and paracentral keratoconus. Medicine 2017, 96, e6247. [Google Scholar] [CrossRef]
- Gomes, J.A.; Tan, D.; Rapuano, C.J.; Belin, M.W.; Ambrósio, R., Jr.; Guell, J.L.; Malecaze, F.; Nishida, K.; Sangwan, V.S.; Group of Panelists for the Global Delphi Panel of Keratoconus and Ectatic Diseases. Global consensus on keratoconus and ectatic diseases. Cornea 2015, 34, 359–369. [Google Scholar] [CrossRef]
- Saglik, A.; Isik, M.U. Progression Analysis with ABCD Grading System following Corneal Collagen Cross-Linking in Keratoconus. Beyoglu Eye J. 2019, 4, 156–162. [Google Scholar] [CrossRef]
- Bardan, A.S.; Kubrak-Kisza, M.; Kisza, K.J.; Nanavaty, M.A. Impact of classifying keratoconus location based on keratometry or pachymetry on progression parameters. Clin. Exp. Optom. 2020, 103, 312–319. [Google Scholar] [CrossRef]
- Krolo, I.; Kasumović, A.; Matoc, I.; Sabol, I.; Radman, I.; Ratković, M. The ABCD grading system in assessment of corneal cross-linking effect in keratoconus with different cone locations. J. Optom. 2023, 16, 74–80. [Google Scholar] [CrossRef] [PubMed]
- Kasumović, A.; Matoc, I.; Kasumović, A.; Sabol, I.; Radman, I.; Krolo, I. Assessment of the postoperative effect of corneal cross-linking on keratoconus using the ABCD grading system. Indian. J. Ophthalmol. 2022, 70, 79–84. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Shen, D.; Wang, H.Y.; Liang, D.F.; Zeng, Q.Y. Independent-effect comparison of five crosslinking procedures for Progressive Keratoconus based on Keratometry and the ABCD Grading System using Generalized Estimating Equations (GEE). BMC Ophthalmol. 2023, 23, 16. [Google Scholar] [CrossRef] [PubMed]
- Greenstein, S.A.; Hersh, P.S. Characteristics influencing outcomes of corneal collagen crosslinking for keratoconus and ectasia: Implications for patient selection. J. Cataract Refract. Surg. 2013, 39, 1133–1140. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| CXL30 (n = 15) | CXL10 (n = 13) | t a χ2 b Z c | p | |
|---|---|---|---|---|
| Age (years) * | 22.58 ± 4.48 | 28.08 ± 5.27 | −2.797 a | 0.010 |
| Gender (m/f) ** | 9/3 | 12/1 | 1.391 b | 0.238 |
| Eye (right/left) ** | 8/7 | 7/6 | 0.001 b | 0.978 |
| Kmax ≥ 55, BCVA ≤ 0.5/Kmax < 55, BCVA > 0.5 ** | 12/3 | 13/0 | 2.912 b | 0.088 |
| Kmax † | 57.2 (47–77) | 60 (53–90) | −1.750 c | 0.080 |
| UDVA (decimal) † | 0.2 (0.05–0.8) | 0.1 (0.01–0.5) | 1.727 c | 0.084 |
| Sphere (dptr) † | −1.00 (0.00, −7.00) | −1.50 (0.50, −14.00) | 0.668 c | 0.504 |
| Cylinder (dptr) † | −1.25 (0.00, −5.00) | −2.50 (0.00, −6.00) | 1.543 c | 0.123 |
| BCVA (decimal) † | 0.4 (0.15–0.8) | 0.2 (0.08–0.7) | 1.589 c | 0.112 |
| UDVA † | ||||||
| V0 | V1 | V2 | V3 | χ2 d | p | |
| CXL30 | 0.2 (0.05–0.8) | 0.3 (0.05–0.7) | 0.4 (0.05–0.7) | 0.5 (0.05–1.0) | 17.388 | <0.001 |
| CXL10 | 0.1 (0.01–0.5) | 0.1 (0.03–0.3) | 0.2 (0.08–0.5) | 0.2 (0.10–0.6) | 16.885 | <0.001 |
| BCVA † | ||||||
| V0 | V1 | V2 | V3 | χ2 d | p | |
| CXL30 | 0.4 (0.15–0.8) | 0.3 (0.10–0.8) | 0.6 (0.20–0.8) | 0.6 (0.15–1.0) | 24.529 | <0.001 |
| CXL10 | 0.2 (0.08–0.7) | 0.3 (0.05–0.5) | 0.4 (0.20–0.6) | 0.4 (0.30–0.7) | 18.031 | <0.001 |
| Kmax † | ||||||
| V0 | V1 | V2 | V3 | χ2 d | p | |
| CXL30 | 57.2 (47–77) | 57.9 (48–80) | 57.6 (46–76) | 55.4 (46–76) | 15.919 | 0.001 |
| CXL10 | 60 (53–90) | 63 (55–87) | 60 (54–87) | 60 (54–89) | 8.615 | 0.035 |
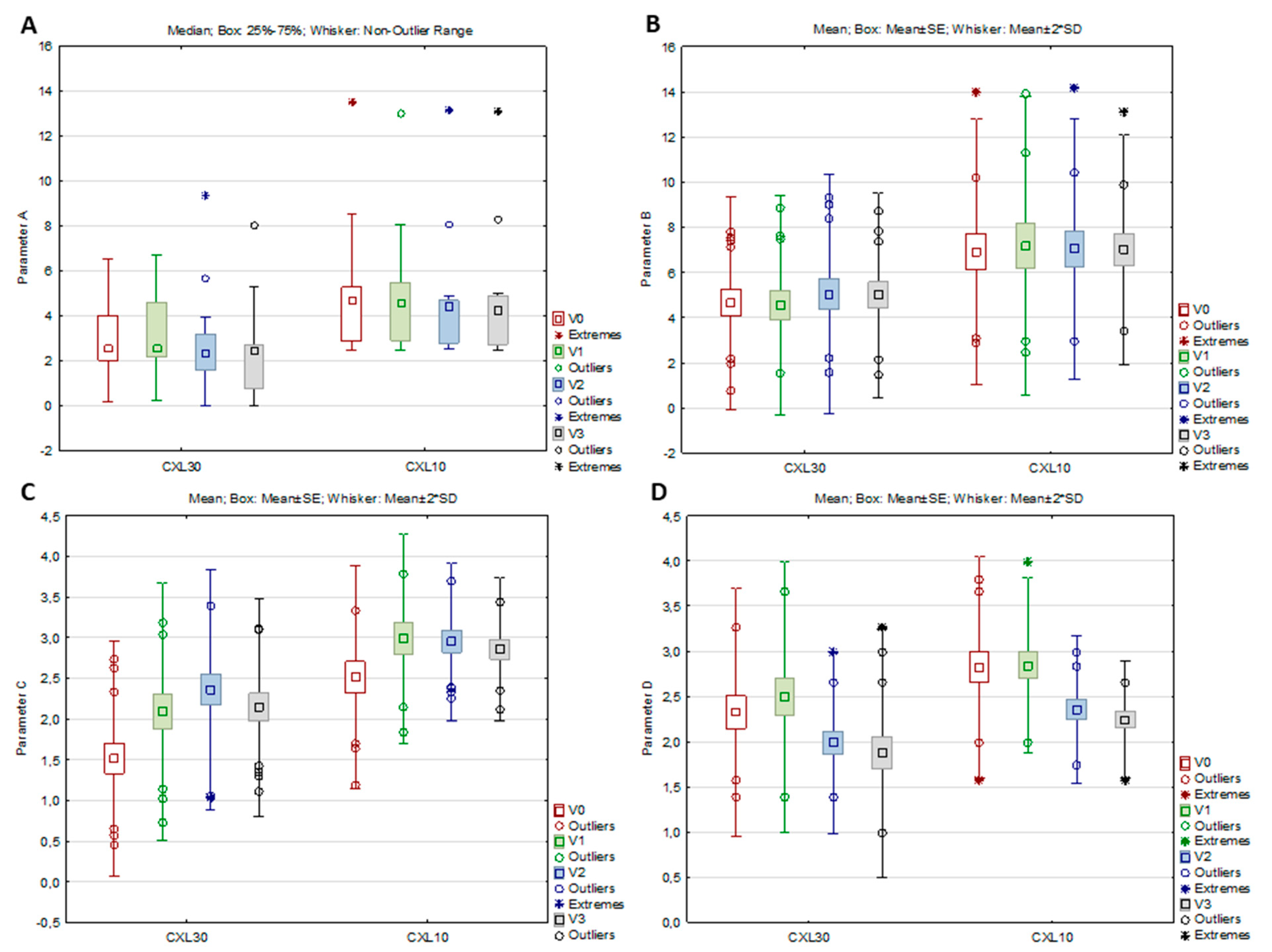
| Parameter A † | ||||||
| V0 | V1 | V2 | V3 | χ2 d | p | |
| CXL30 | 2.6 (0.2–6.5) | 2.6 (0.3–6.7) | 2.4 (0–9.4) | 2.5 (0.2–8.0) | 7.905 | 0.048 |
| CXL10 | 4.7 (2.5–13.5) | 4.6 (2.5–13.0) | 4.4 (2.5–13.2) | 4.3 (2.5–13.1) | 4.139 | 0.247 |
| Parameter B * | ||||||
| V0 | V1 | V2 | V3 | F e | p | |
| CXL30 | 4.66 ± 2.34 | 4.54 ± 2.43 | 5.03 ± 2.65 | 4.99 ± 2.26 | 4.292 | 0.010 |
| CXL10 | 6.92 ± 2.94 | 7.18 ± 3.31 | 7.05 ± 2.89 | 7.01 ± 2.55 | 0.144 | 0.933 |
| Parameter C * | ||||||
| V0 | V1 | V2 | V3 | F e | p | |
| CXL30 | 1.52 ± 0.72 | 2.09 ± 0.79 | 2.36 ± 0.74 | 2.14 ± 0.67 | 25.776 | <0.001 |
| CXL10 | 2.51 ± 0.69 | 2.98 ± 0.64 | 2.95 ± 0.48 | 2.86 ± 0.44 | 6.847 | 0.001 |
| Parameter D * | ||||||
| V0 | V1 | V2 | V3 | F e | p | |
| CXL30 | 2.33 ± 0.69 | 2.49 ± 0.75 | 1.99 ± 0.50 | 1.87 ± 0.69 | 17.629 | <0.001 |
| CXL10 | 2.82 ± 0.61 | 2.84 ± 0.48 | 2.35 ± 0.41 | 2.24 ± 0.32 | 12.839 | <0.001 |
| ARC * | ||||||
| V0 | V1 | V2 | V3 | F e | p | |
| CXL30 | 6.62 ± 0.54 | 6.59 ± 0.54 | 6.73 ± 0.73 | 6.85 ± 0.54 | 3.995 | 0.014 |
| CXL10 | 5.97 ± 0.66 | 5.96 ± 0.66 | 6.05 ± 0.62 | 6.06 ± 0.64 | 1.859 | 0.158 |
| PRC * | ||||||
| V0 | V1 | V2 | V3 | F e | p | |
| CXL30 | 4.89 ± 0.58 | 4.92 ± 0.58 | 4.81 ± 0.62 | 4.64 ± 0.84 | 4.056 | 0.013 |
| CXL10 | 4.37 ± 0.59 | 4.33 ± 0.69 | 4.34 ± 0.58 | 4.34 ± 0.51 | 0.058 | 0.982 |
| TP * | ||||||
| V0 | V1 | V2 | V3 | F e | p | |
| CXL30 | 470.60 ± 34.82 | 442.00 ± 37.93 | 428.33 ± 36.95 | 439.47 ± 32.13 | 21.936 | <0.001 |
| CXL10 | 419.00 ± 31.20 | 396.82 ± 55.58 | 393.38 ± 33.57 | 402.15 ± 27.37 | 3.590 | 0.025 |
| BAD-D † | ||||||
| V0 | V1 | V2 | V3 | χ2 d | p | |
| CXL30 | 9 (1.5–15.5) | 8.6 (1.6–18.6) | 9.3 (2.2–20.9) | 9.6 (4.1–18.3) | 16.200 | 0.001 |
| CXL10 | 13.0 (8–33.7) | 13.2 (8–34.3) | 13.5 (9–33.0) | 13.1 (8–31.6) | 2.119 | 0.548 |
| PI * | ||||||
| V0 | V1 | V2 | V3 | F e | p | |
| CXL30 | 2.15 ± 0.62 | 2.46 ± 0.78 | 2.78 ± 0.83 | 2.81 ± 0.66 | 9.161 | <0.001 |
| CXL10 | 2.92 ± 0.85 | 3.57 ± 1.58 | 3.43 ± 1.17 | 3.25 ± 0.79 | 2.483 | 0.079 |
| ARTmax * | ||||||
| V0 | V1 | V2 | V3 | F e | p | |
| CXL30 | 156.0 ± 50.8 | 125.8 ± 50.9 | 119.6 ± 40.7 | 124.0 ± 38.9 | 4.531 | 0.008 |
| CXL10 | 110.4 ± 46.0 | 86.7 ± 50.0 | 90.8 ± 30.6 | 92.7 ± 28.3 | 3.829 | 0.019 |
| F Km * | ||||||
| V0 | V1 | V2 | V3 | F e | p | |
| CXL30 | 48.12 ± 3.38 | 48.90 ± −3.96 | 47.84 ± 4.25 | 46.97 ± 4.01 | 6.703 | <0.001 |
| CXL10 | 48.56 ± 15.48 | 53.43 ± 6.49 | 52.16 ± 6.22 | 51.95 ± 6.54 | 0.958 | 0.425 |
| B Km * | ||||||
| V0 | V1 | V2 | V3 | F e | p | |
| CXL30 | −7.21 ± 0.75 | −7.09 ± 0.75 | −7,36 ± 0.79 | −7.38 ± 0.76 | 9.249 | <0.001 |
| CXL10 | −8.00 ± 1.26 | −8.13 ± 1.46 | −8.08 ± 1.35 | −8.01 ± 1.17 | 1.058 | 0.382 |
| PA * | ||||||
| V0 | V1 | V2 | V3 | F e | p | |
| CXL30 | 482.80 ± 35.29 | 459.07 ± 32.14 | 446.00 ± 30.58 | 451.73 ± 27.49 | 22.345 | <0.001 |
| CXL10 | 432.92 ± 32.44 | 402.45 ± 44.64 | 405.77 ± 35.35 | 416.08 ± 30.24 | 7.386 | <0.001 |
| El. F * | ||||||
| V0 | V1 | V2 | V3 | F e | p | |
| CXL30 | 24.87 ± 11.47 | 26.43 ± 9.38 | 23.87 ± 15.09 | 21.33 ± 15.45 | 1.243 | 0.307 |
| CXL10 | 36.38 ± 17.75 | 36.00 ± 18.55 | 34.23 ± 16.80 | 34.54 ± 17.38 | 0.395 | 0.758 |
| El. B * | ||||||
| V0 | V1 | V2 | V3 | F e | p | |
| CXL30 | 55.67 ± 24.90 | 55.86 ± 22.62 | 58.13 ± 25.35 | 60.27 ± 23.86 | 2.991 | 0.042 |
| CXL10 | 77.15 ± 33.37 | 77.73 ± 40.06 | 77.08 ± 35.63 | 78.54 ± 31.14 | 0.143 | 0.933 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vidas Pauk, S.; Jandroković, S.; Lešin Gaćina, D.; Tomić, M.; Bulum, T.; Pupić Bakrač, A.; Kuzman, T.; Knežević, J.; Kalauz, M. Short-Term Effect of Conventional Versus Accelerated Corneal Cross-Linking Protocol on Corneal Geography and Stability. Medicina 2023, 59, 1043. https://doi.org/10.3390/medicina59061043
Vidas Pauk S, Jandroković S, Lešin Gaćina D, Tomić M, Bulum T, Pupić Bakrač A, Kuzman T, Knežević J, Kalauz M. Short-Term Effect of Conventional Versus Accelerated Corneal Cross-Linking Protocol on Corneal Geography and Stability. Medicina. 2023; 59(6):1043. https://doi.org/10.3390/medicina59061043
Chicago/Turabian StyleVidas Pauk, Sania, Sonja Jandroković, Dina Lešin Gaćina, Martina Tomić, Tomislav Bulum, Ana Pupić Bakrač, Tomislav Kuzman, Josip Knežević, and Miro Kalauz. 2023. "Short-Term Effect of Conventional Versus Accelerated Corneal Cross-Linking Protocol on Corneal Geography and Stability" Medicina 59, no. 6: 1043. https://doi.org/10.3390/medicina59061043