
Impact of Sarcopenia on Percutaneous Epidural Balloon Neuroplasty in Patients with Lumbar Spinal Stenosis: A Retrospective Analysis
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
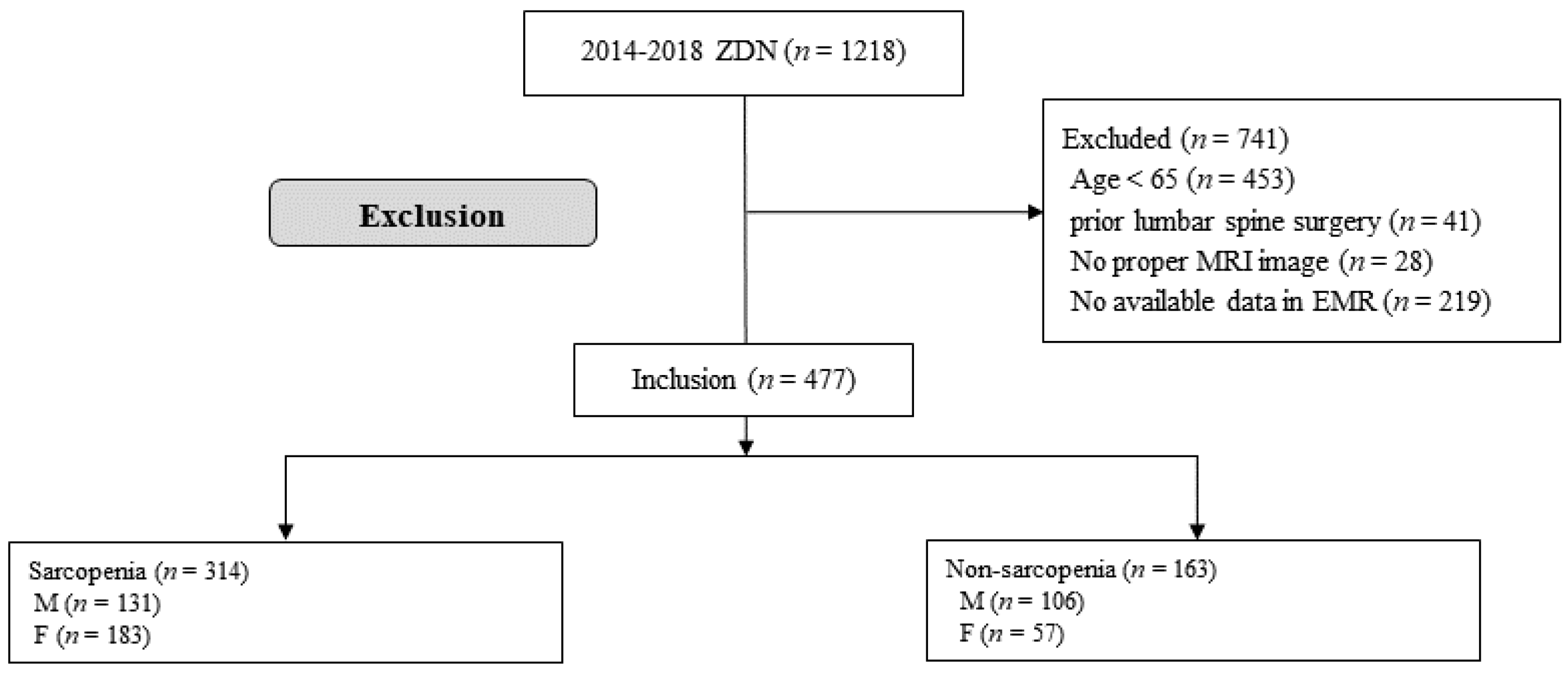
2.1. Study Design and Participants
2.2. Percutaneous Epidural Balloon Neuroplasty
2.3. Demographic Data and Outcome Assessments
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M. Sarcopenia: European consensus on definition and diagnosisReport of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed]
- Doherty, T.J. Invited review: Aging and sarcopenia. J. Appl. Physiol. 2003, 95, 1717–1727. [Google Scholar] [CrossRef]
- Bentov, I.; Kaplan, S.J.; Pham, T.N.; Reed, M.J. Frailty assessment: From clinical to radiological tools. Br. J. Anaesth. 2019, 123, 37–50. [Google Scholar] [CrossRef] [PubMed]
- Campins, L.; Camps, M.; Riera, A.; Pleguezuelos, E.; Yebenes, J.C.; Serra-Prat, M. Oral drugs related with muscle wasting and sarcopenia. A review. Pharmacology 2017, 99, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Alipour, O.; Lee, V.; Tejura, T.K.; Wilson, M.L.; Memel, Z.; Cho, J.; Cologne, K.; Hwang, C.; Shao, L. The assessment of sarcopenia using psoas muscle thickness per height is not predictive of post-operative complications in IBD. Scand. J. Gastroenterol. 2021, 56, 1175–1181. [Google Scholar] [CrossRef] [PubMed]
- Zager, Y.; Khalilieh, S.; Ganaiem, O.; Gorgov, E.; Horesh, N.; Anteby, R.; Kopylov, U.; Jacoby, H.; Dreznik, Y.; Dori, A. Low psoas muscle area is associated with postoperative complications in Crohn’s disease. Int. J. Colorectal Dis. 2021, 36, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Nakashima, Y.; Saeki, H.; Nakanishi, R.; Sugiyama, M.; Kurashige, J.; Oki, E.; Maehara, Y. Assessment of sarcopenia as a predictor of poor outcomes after esophagectomy in elderly patients with esophageal cancer. Annal. Sur. 2018, 267, 1100–1104. [Google Scholar] [CrossRef]
- Hsu, J.; Krishnan, A.; Lin, C.T.; Shah, P.D.; Broderick, S.R.; Higgins, R.S.; Merlo, C.A.; Bush, E.L. Sarcopenia of the psoas muscles is associated with poor outcomes following lung transplantation. Annal. Thorac. Sur. 2019, 107, 1082–1088. [Google Scholar] [CrossRef] [PubMed]
- Druckmann, I.; Yashar, H.; Schwartz, D.; Schwartz, I.F.; Goykhman, Y.; Ben-Bassat, O.K.; Baruch, R.; Tzadok, R.; Shashar, M.; Cohen-Hagai, K. Presence of Sarcopenia before Kidney Transplantation Is Associated with Poor Outcomes. Am. J. Nephrol. 2022, 53, 427–434. [Google Scholar] [CrossRef]
- Nakai, Y.; Makizako, H.; Kiyama, R.; Tomioka, K.; Taniguchi, Y.; Kubozono, T.; Takenaka, T.; Ohishi, M. Association between chronic pain and physical frailty in community-dwelling older adults. Int. J. Environ. Res. Public Health 2019, 16, 1330. [Google Scholar] [CrossRef]
- Deer, T.; Sayed, D.; Michels, J.; Josephson, Y.; Li, S.; Calodney, A.K. A review of lumbar spinal stenosis with intermittent neurogenic claudication: Disease and diagnosis. Pain Med. 2019, 20, S32–S44. [Google Scholar] [CrossRef] [PubMed]
- Lurie, J.; Tomkins-Lane, C. Management of lumbar spinal stenosis. BMJ 2016, 352, h6234. [Google Scholar] [CrossRef] [PubMed]
- Szpalski, M.; Gunzburg, R. Lumbar spinal stenosis in the elderly: An overview. Eur. Spine J. 2003, 12, S170–S175. [Google Scholar] [CrossRef] [PubMed]
- Kaptan, H.; Kasimcan, O.; Cakiroglu, K.; Ilhan, M.N.; Kilic, C. Lumbar spinal stenosis in elderly patients. Annal. N. Y. Acad. Sci. 2007, 1100, 173–178. [Google Scholar] [CrossRef]
- Park, S.; Kim, H.; Ko, B.; Chung, J.; Kim, S.; Park, S.; Lee, M.; Yeom, J. The prevalence and impact of sarcopenia on degenerative lumbar spinal stenosis. Bone Joint J. 2016, 98, 1093–1098. [Google Scholar] [CrossRef]
- Sakai, Y.; Matsui, H.; Ito, S.; Hida, T.; Ito, K.; Koshimizu, H.; Harada, A. Sarcopenia in elderly patients with chronic low back pain. Osteoporos. Sarcopenia 2017, 3, 195–200. [Google Scholar] [CrossRef]
- Karm, M.-H.; Kim, C.-S.; Kim, D.-H.; Lee, D.; Kim, Y.; Shin, J.-W.; Choi, S.-S. Effectiveness of percutaneous epidural neuroplasty using a balloon catheter in patients with chronic spinal stenosis accompanying mild spondylolisthesis: A longitudinal cohort study. Korean J. Pain 2023, 36, 184–194. [Google Scholar] [CrossRef]
- Karm, M.-H. Effectiveness of epidural balloon neuroplasty in patients with chronic spinal stenosis accompanied by redundant nerve roots: A longitudinal cohort study. Pain Physician 2022, 25, E841–E850. [Google Scholar]
- Kim, N.E.; Choi, J.B.; Kwon, H.R.; Chung, H.T.; Jang, E.S.; Moon, C.Y.; Kim, B.G. Comparison of the Effect of Balloon Catheter vs Nucleoplasty vs Balloon Catheter and Nucleoplasty in Patients With Lumbar Spinal Stenosis. Pain Physician 2022, 25, E1095–E1103. [Google Scholar]
- Gil, H.Y.; Jeong, S.; Cho, H.; Choi, E.; Nahm, F.S.; Lee, P.-B. Kambin’s triangle approach versus traditional safe triangle approach for percutaneous transforaminal epidural adhesiolysis using an inflatable balloon catheter: A pilot study. J. Clin. Med. 2019, 8, 1996. [Google Scholar] [CrossRef]
- Bokshan, S.L.; Han, A.L.; DePasse, J.M.; Eltorai, A.E.; Marcaccio, S.E.; Palumbo, M.A.; Daniels, A.H. Effect of sarcopenia on postoperative morbidity and mortality after thoracolumbar spine surgery. Orthopedics 2016, 39, e1159–e1164. [Google Scholar] [CrossRef] [PubMed]
- Hirase, T.; Haghshenas, V.; Bratescu, R.; Dong, D.; Kuo, P.H.; Rashid, A.; Kavuri, V.; Hanson, D.S.; Meyer, B.C.; Marco, R.A. Sarcopenia predicts perioperative adverse events following complex revision surgery for the thoracolumbar spine. Spine J. 2021, 21, 1001–1009. [Google Scholar] [CrossRef] [PubMed]
- Inose, H.; Yamada, T.; Hirai, T.; Yoshii, T.; Abe, Y.; Okawa, A. The impact of sarcopenia on the results of lumbar spinal surgery. Osteoporos. Sarcopenia 2018, 4, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Rho, M.; Yoon, K.B.; Jo, M.; Lee, D.W.; Kim, S.H. Influence of cross-sectional area and fat infiltration of paraspinal muscles on analgesic efficacy of epidural steroid injection in elderly patients. Pain Pract. 2022, 22, 621–630. [Google Scholar] [CrossRef]
- Amini, N.; Spolverato, G.; Gupta, R.; Margonis, G.A.; Kim, Y.; Wagner, D.; Rezaee, N.; Weiss, M.J.; Wolfgang, C.L.; Makary, M.M. Impact total psoas volume on short-and long-term outcomes in patients undergoing curative resection for pancreatic adenocarcinoma: A new tool to assess sarcopenia. J. Gastrointest. Sur. 2015, 19, 1593–1602. [Google Scholar] [CrossRef]
- Gallizzi, M.; Gagnon, C.; Harden, R.N.; Stanos, S.; Khan, A. Medication Quantification Scale Version III: Internal validation of detriment weights using a chronic pain population. Pain Pract. 2008, 8, 1–4. [Google Scholar] [CrossRef]
- Schizas, C.; Theumann, N.; Burn, A.; Tansey, R.; Wardlaw, D.; Smith, F.W.; Kulik, G. Qualitative grading of severity of lumbar spinal stenosis based on the morphology of the dural sac on magnetic resonance images. Spine 2010, 35, 1919–1924. [Google Scholar] [CrossRef]
- Lee, S.; Lee, J.W.; Yeom, J.S.; Kim, K.-J.; Kim, H.-J.; Chung, S.K.; Kang, H.S. A practical MRI grading system for lumbar foraminal stenosis. Am. J. Roentgenol. 2010, 194, 1095–1098. [Google Scholar] [CrossRef]
- Naruishi, K.; Yumoto, H.; Kido, J.-i. Clinical effects of low body mass index on geriatric status in elderly patients. Exp. Gerontol. 2018, 110, 86–91. [Google Scholar] [CrossRef]
- Rosenberg, I.H. Sarcopenia: Origins and clinical relevance. J. Nutr. 1997, 127, 990S–991S. [Google Scholar] [CrossRef]
- Friedman, J.; Lussiez, A.; Sullivan, J.; Wang, S.; Englesbe, M. Implications of sarcopenia in major surgery. Nutr. Clin. Pract. 2015, 30, 175–179. [Google Scholar] [CrossRef] [PubMed]
- Beaudart, C.; Zaaria, M.; Pasleau, F.; Reginster, J.-Y.; Bruyère, O. Health outcomes of sarcopenia: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0169548. [Google Scholar] [CrossRef] [PubMed]
- Kaplan, S.J.; Pham, T.N.; Arbabi, S.; Gross, J.A.; Damodarasamy, M.; Bentov, I.; Taitsman, L.A.; Mitchell, S.H.; Reed, M.J. Association of radiologic indicators of frailty with 1-year mortality in older trauma patients: Opportunistic screening for sarcopenia and osteopenia. JAMA Surg. 2017, 152, e164604. [Google Scholar] [CrossRef]
- Moisey, L.L.; Mourtzakis, M.; Cotton, B.A.; Premji, T.; Heyland, D.K.; Wade, C.E.; Bulger, E.; Kozar, R.A. Skeletal muscle predicts ventilator-free days, ICU-free days, and mortality in elderly ICU patients. Crit. Care 2013, 17, R206. [Google Scholar] [CrossRef] [PubMed]
- Hawkins, R.B.; Mehaffey, J.H.; Charles, E.J.; Kern, J.A.; Lim, D.S.; Teman, N.R.; Ailawadi, G. Psoas muscle size predicts risk-adjusted outcomes after surgical aortic valve replacement. Annal. Thorac. Sur. 2018, 106, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, J.N.; Tosteson, T.D.; Lurie, J.D.; Tosteson, A.N.; Blood, E.; Hanscom, B.; Herkowitz, H.; Cammisa, F.; Albert, T.; Boden, S.D. Surgical versus nonsurgical therapy for lumbar spinal stenosis. N. Engl. J. Med. 2008, 358, 794–810. [Google Scholar] [CrossRef]
- Kobayashi, S.; Takeno, K.; Miyazaki, T.; Kubota, M.; Shimada, S.; Yayama, T.; Uchida, K.; Normura, E.; Mwaka, E.; Baba, H. Effects of arterial ischemia and venous congestion on the lumbar nerve root in dogs. J. Orthop. Res. 2008, 26, 1533–1540. [Google Scholar] [CrossRef]
- Chen, J.; Wang, J.; Wang, B.; Xu, H.; Lin, S.; Zhang, H. Post-surgical functional recovery, lumbar lordosis, and range of motion associated with MR-detectable redundant nerve roots in lumbar spinal stenosis. Clin. Neurol. Neurosur. 2016, 140, 79–84. [Google Scholar] [CrossRef]
- Moon, D.E.; Park, H.J.; Kim, Y.H. Assessment of clinical outcomes of cervical epidural neuroplasty using a Racz-catheter and predictive factors of efficacy in patients with cervical spinal pain. Pain Physician 2015, 18, E163. [Google Scholar]
- World Health Organization. Physical Status: The Use of and Interpretation of Anthropometry, Report of a WHO Expert Committee; World Health Organization: Geneva, Switzerland, 1995.
- Abe, T.; Kearns, C.; Fukunaga, T. Sex differences in whole body skeletal muscle mass measured by magnetic resonance imaging and its distribution in young Japanese adults. Br. J. Sports Med. 2003, 37, 436–440. [Google Scholar] [CrossRef]
- Schorr, M.; Dichtel, L.E.; Gerweck, A.V.; Valera, R.D.; Torriani, M.; Miller, K.K.; Bredella, M.A. Sex differences in body composition and association with cardiometabolic risk. Biol. Sex Differ. 2018, 9, 28. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Total (n = 477) | Sarcopenia | p-Value | |
|---|---|---|---|---|
| No (n = 163) | Yes (n = 314) | |||
| Age, year | 72.0 (69.0–77.0) | 71.0 (68.0–77.0) | 73.0 (69.0–78.0) | 0.031 |
| Sex, male | 237 (49.7) | 106 (65.0) | 131 (41.7) | 0.001 |
| BMI, kg/m2 | 24.8 (22.9–26.6) | 25.8 (23.9–28.0) | 24.1 (22.5–26.0) | 0.001 |
| Diabetes | 113 (23.7) | 35 (21.5) | 78 (24.8) | 0.480 |
| Hypertension | 240 (50.3) | 82 (50.3) | 158 (50.3) | 0.999 |
| Pain duration, months | 24.0 (12.0–48.0) | 26.0 (12.0–62.0) | 24.0 (12.0–48.0) | 0.058 |
| Pain location | ||||
| Back/leg/both | 42 (8.8)/141 (29.6)/294 (61.6) | 10 (6.1)/48 (29.4)/105 (64.4) | 32 (10.2)/93 (29.6)/189 (60.2) | 0.314 |
| Pain intensity (NRS) | ||||
| Back pain | 7.0 (6.0–8.0) | 7.0 (6.0–8.0) | 7.0 (6.0–8.0) | 0.844 |
| Leg pain | 7.0 (6.0–8.0) | 7.0 (6.0–8.0) | 7.0 (6.0–8.0) | 0.565 |
| MQS | 8.2 (4.2–12.4) | 9.6 (4.6–13.8) | 6.8 (4.2–11.6) | 0.002 |
| Central stenosis grading | ||||
| Mild/Moderate/ Severe | 117 (25.0)/98 (20.9)/253 (53.8) | 31 (19.5)/30 (18.9)/ 98 (61.6) | 86 (27.8)/68 (22.0)/155 (50.3) | 0.093 |
| Foraminal stenosis grading | ||||
| Mild/Moderate /Severe | 139 (33.4)/123 (29.6)/154 (37.0) | 55 (37.9)/44 (30.3)/ 46 (31.7) | 84 (31.0)/79 (29.2)/108 (39.9) | 0.213 |
| Target level | 0.179 | |||
| 1 level | 208 (43.6) | 69 (42.3) | 139 (44.3) | |
| 2 levels | 191 (40.0) | 65 (39.9) | 126 (40.1) | |
| 3 levels | 67 (14.0) | 28 (17.2) | 39 (12.4) | |
| >4 levels | 11 (2.3) | 1 (0.6) | 10 (3.2) | |
| Variables | Time | Estimated Pain Score (95% CI) | Estimated Difference (95% CI) * | p-Value | |
|---|---|---|---|---|---|
| Non-Sarcopenia (n = 163) | Sarcopenia (n = 314) | ||||
| Back pain (NRS) | Baseline | 6.7 (6.3–7.1) | 6.7 (6.5–7.0) | 0.0 (−0.5–0.5) | 0.912 |
| 1 month | 4.9 (4.5–5.3) † | 4.7 (4.4–5.0) † | −0.2 (−0.7–0.3) | 0.463 | |
| 3 months | 4.9 (4.4–5.5) † | 4.6 (4.2–4.9) † | −0.4 (−1.0–0.3) | 0.262 | |
| 6 months | 4.8 (4.2–5.5) † | 4.4 (4.0–4.9) † | −0.4 (−1.2–0.4) | 0.343 | |
| Leg pain (NRS) | Baseline | 7.0 (6.7–7.4) | 7.2 (6.9–7.4) | 0.2 (−0.3–0.6) | 0.456 |
| 1 month | 5.2 (4.8–5.5) † | 4.9 (4.6–5.2) † | −0.3 (−0.7–0.2) | 0.241 | |
| 3 months | 4.6 (4.1–5.0) † | 4.7 (4.3–5.0) † | 0.1 (−0.5–0.6) | 0.758 | |
| 6 months | 4.5 (4.0–5.0) † | 4.7 (4.3–5.1) † | 0.2 (−0.5–0.9) | 0.540 | |
| MQS | Baseline | 9.6 (8.6–10.6) | 7.6 (6.8–8.4) | −2.0 (−3.2–0.7) | 0.003 |
| 1 month | 9.7 (8.6–10.7) | 8.2 (7.4–8.9) | −1.5 (−2.8–0.3) | 0.015 | |
| 3 months | 9.7 (8.6–10.9) | 8.2 (7.4–9.0) | −1.6 (−2.9–0.2) | 0.028 | |
| 6 months | 8.7 (7.4–9.9) | 7.4 (6.5–8.3) | −1.3 (−2.8–0.3) | 0.111 | |
| Variables | Time | Estimated Pain Score (95% CI) | Estimated Difference (95% CI) * | p-Value | |
|---|---|---|---|---|---|
| Non-Sarcopenia (n = 163) | Sarcopenia (n = 314) | ||||
| Back pain (NRS) | Baseline | 7.1 (6.6–7.6) | 6.9 (6.6–7.3) | −0.1 (−0.8–0.5) | 0.685 |
| 1 month | 5.2 (4.5–5.7) † | 4.8 (4.4–5.2) † | −0.4 (−1.0–0.3) | 0.257 | |
| 3 months | 5.3 (4.5–6.0) † | 4.8 (4.3–5.2) † | −0.5 (−1.4–0.4) | 0.268 | |
| 6 months | 5.1 (4.2–6.0) † | 4.6 (3.9–5.3) † | −0.5 (−1.7–0.6) | 0.347 | |
| Leg pain (NRS) | Baseline | 7.3 (6.9–7.7) | 7.4 (7.0–7.7) | 0.1 (−0.5–0.6) | 0.846 |
| 1 month | 5.4 (5.0–5.8) † | 5.0 (4.7–5.3) † | −0.4 (−1.0–0.1) | 0.145 | |
| 3 months | 4.5 (3.8–5.1) † | 4.8 (4.4–5.2) † | 0.3 (−0.4–1.1) | 0.407 | |
| 6 months | 4.9 (4.1–5.6) † | 5.1 (4.4–5.7) † | 0.2 (−0.8–1.2) | 0.684 | |
| MQS | Baseline | 10.1 (8.9–11.3) | 7.8 (6.9–8.7) | −2.3 (−3.8–0.8) | 0.003 |
| 1 month | 9.7 (8.6–10.9) | 8.4 (7.6–9.2) | −1.3 (−2.8–0.1) | 0.071 | |
| 3 months | 9.7 (8.4–10.9) | 8.4 (7.5–9.3) | −1.3 (−2.9–0.3) | 0.112 | |
| 6 months | 9.1 (7.6–10.5) | 7.6 (6.6–8.6) | −1.4 (−3.2–0.3) | 0.114 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Han, Y.-A.; Kwon, H.-J.; Lee, K.; Son, M.-G.; Kim, H.; Choi, S.-S.; Shin, J.-W.; Kim, D.-H. Impact of Sarcopenia on Percutaneous Epidural Balloon Neuroplasty in Patients with Lumbar Spinal Stenosis: A Retrospective Analysis. Medicina 2023, 59, 847. https://doi.org/10.3390/medicina59050847
Han Y-A, Kwon H-J, Lee K, Son M-G, Kim H, Choi S-S, Shin J-W, Kim D-H. Impact of Sarcopenia on Percutaneous Epidural Balloon Neuroplasty in Patients with Lumbar Spinal Stenosis: A Retrospective Analysis. Medicina. 2023; 59(5):847. https://doi.org/10.3390/medicina59050847
Chicago/Turabian StyleHan, Yun-A, Hyun-Jung Kwon, Kunhee Lee, Min-Gi Son, Hotaek Kim, Seong-Soo Choi, Jin-Woo Shin, and Doo-Hwan Kim. 2023. "Impact of Sarcopenia on Percutaneous Epidural Balloon Neuroplasty in Patients with Lumbar Spinal Stenosis: A Retrospective Analysis" Medicina 59, no. 5: 847. https://doi.org/10.3390/medicina59050847