
Effects of Topical or Intravitreal Application of Anti-Vascular Endothelial Growth Factor on Density of Intestinal Blood Vessels of Mice


Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of Mice for Experiments
2.2. Surgical Procedure for Mice Experiment
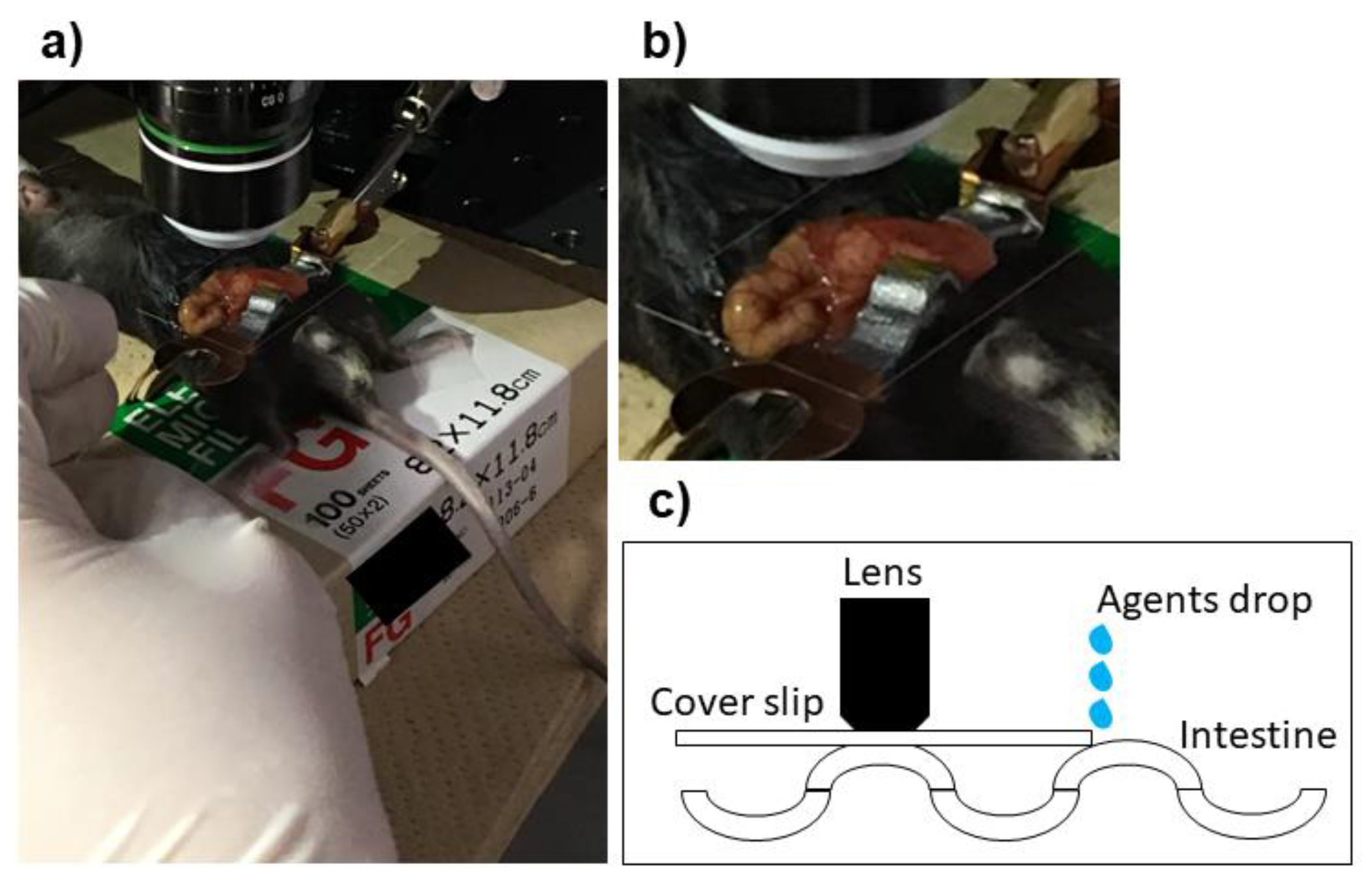
2.3. Preparation and Set Up of Microscope for Experiments
2.4. Administration of Anti-VEGF and Control Agents
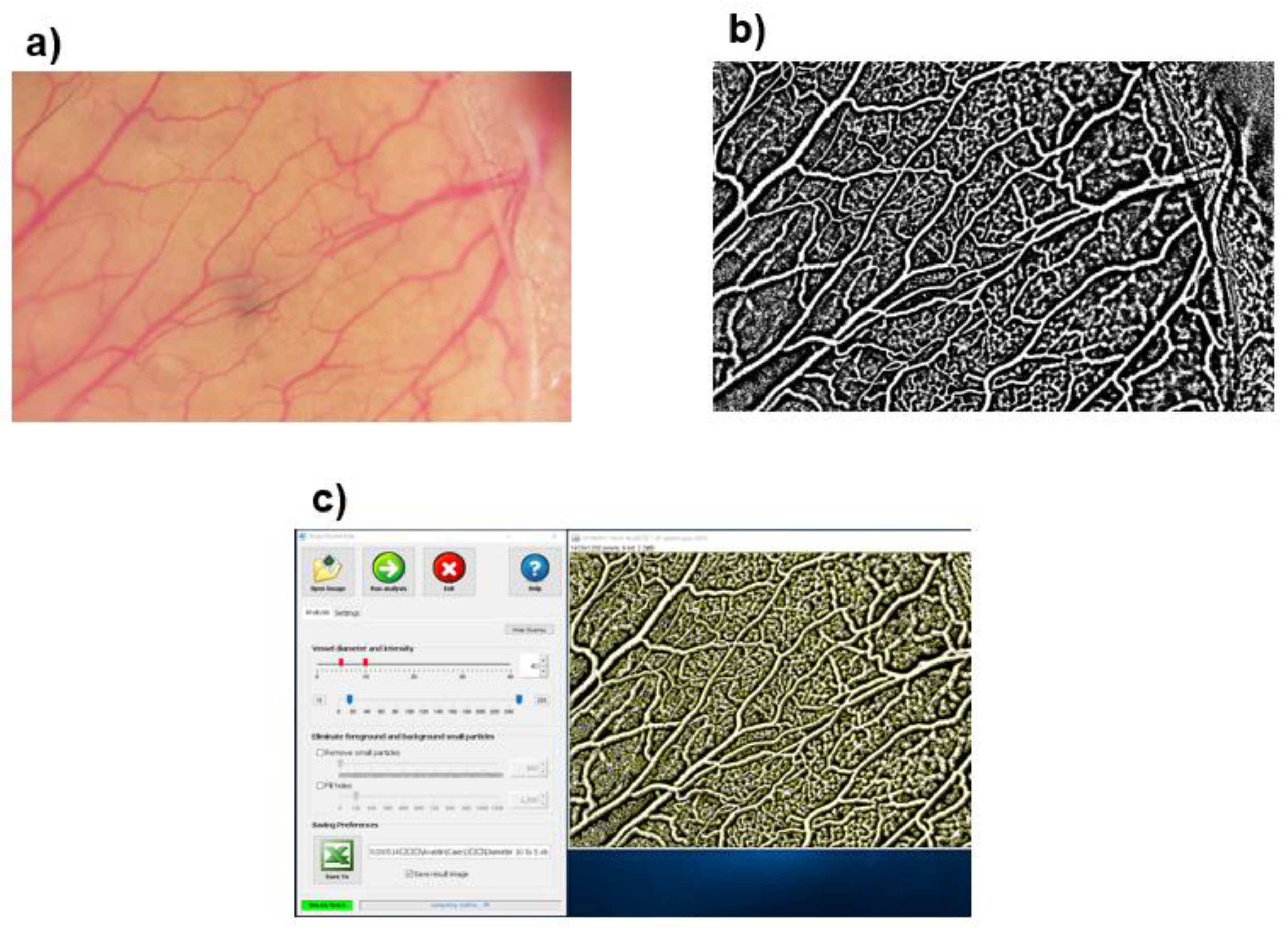
2.5. Evaluations of Vascular Density
Statistical Analyses
3. Results
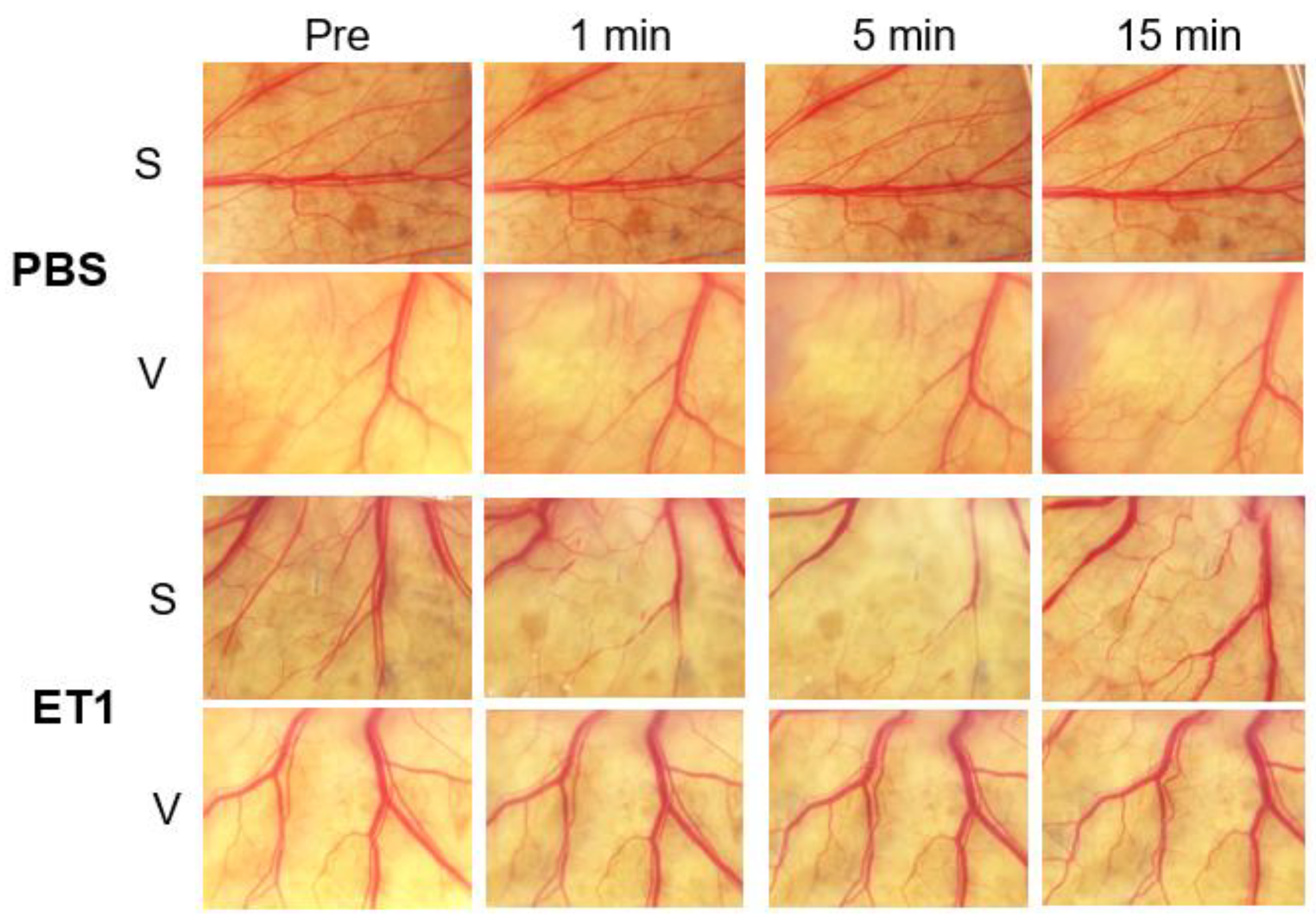
3.1. Vascular Density (VD) after Applications of Control Agents
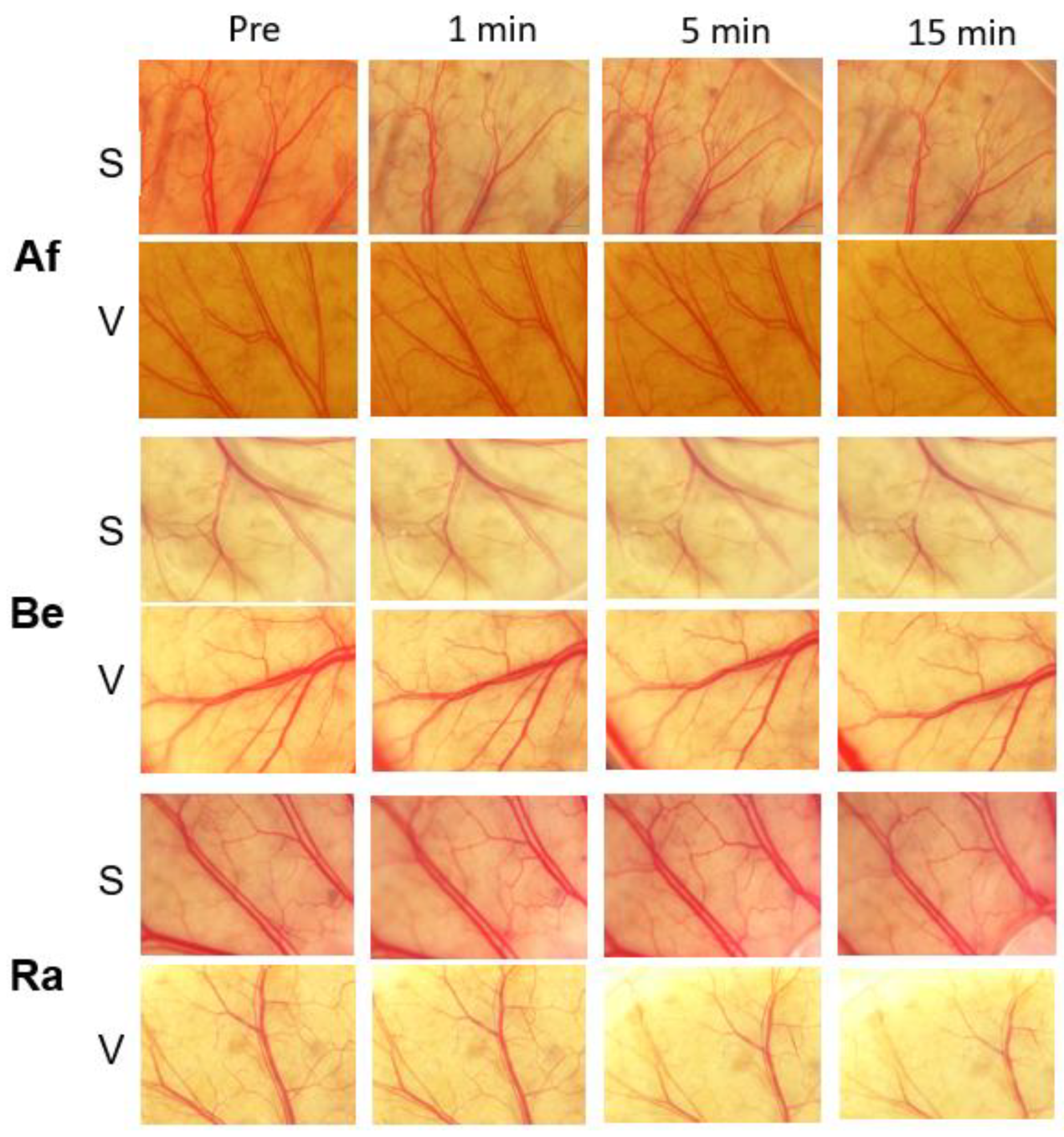
3.2. Evaluations of Vascular Density for Different Anti-VEGF Agents
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

References
- Nguyen, Q.D.; Brown, D.M.; Marcus, D.M.; Boyer, D.S.; Patel, S.; Feiner, L.; Gibson, A.; Sy, J.; Rundle, A.C.; Hopkins, J.J.; et al. Ranibizumab for diabetic macular edema: Results from 2 phase III randomized trials: RISE and RIDE. Ophthalmology 2012, 119, 789–801. [Google Scholar] [CrossRef]
- Brown, D.M.; Schmidt-Erfurth, U.; Do, D.V.; Holz, F.G.; Boyer, D.S.; Midena, E.; Heier, J.S.; Terasaki, H.; Kaiser, P.K.; Marcus, D.M.; et al. Intravitreal aflibercept for diabetic macular edema: 100-week results from the VISTA and VIVID studies. Ophthalmology 2015, 122, 2044–2052. [Google Scholar] [CrossRef] [PubMed]
- Kodjikian, L.; Bellocq, D.; Bandello, F.; Loewenstein, A.; Chakravarthy, U.; Koh, A.; Augustin, A.; de Smet, M.D.; Chhablani, J.; Tufail, A.; et al. First-line treatment algorithm and guidelines in center-involving diabetic macular edema. Eur. J. Ophthalmol. 2019, 29, 573–584. [Google Scholar] [CrossRef]
- Zarbin, M.A. Anti-VEGF Agents and the Risk of Arteriothrombotic Events. Asia-Pac. J. Ophthalmol. 2018, 7, 63–67. [Google Scholar]
- Azzolini, C.; Pagani, I.S.; Pirrone, C.; Borroni, D.; Donati, S.; Al Oum, M.; Pigni, D.; Chiaravalli, A.M.; Vinciguerra, R.; Simonelli, F.; et al. Expression of VEGF-A, Otx homeobox and p53 family genes in proliferative vitreoretinopathy. Mediat. Inflamm. 2013, 2013, 857380. [Google Scholar] [CrossRef] [PubMed]
- Kamba, T.; McDonald, D.M. Mechanisms of adverse effects of anti-VEGF therapy for cancer. Br. J. Cancer 2007, 96, 1788–1795. [Google Scholar] [CrossRef]
- Sugimoto, M.; Nunome, T.; Sakamoto, R.; Kobayashi, M.; Kondo, M. Effect of intravitreal ranibizumab on the ocular circulation of the untreated fellow eye. Graefes Arch. Clin. Exp. Ophthalmol. 2017, 255, 1543–1550. [Google Scholar] [CrossRef] [PubMed]
- Avery, R.L.; A Castellarin, A.; Steinle, N.C.; Dhoot, D.S.; Pieramici, D.J.; See, R.; Couvillion, S.; A Nasir, M.; Rabena, M.D.; Le, K.; et al. Systemic pharmacokinetics following intravitreal injections of ranibizumab, bevacizumab or aflibercept in patients with neovascular AMD. Br. J. Ophthalmol. 2014, 98, 1636–1641. [Google Scholar] [CrossRef]
- Yoshida, I.; Shiba, T.; Taniguchi, H.; Takahashi, M.; Murano, T.; Hiruta, N.; Hori, Y.; Bujo, H.; Maeno, T. Evaluation of plasma vascular endothelial growth factor levels after intravitreal injection of ranibizumab and aflibercept for exudative age-related macular degeneration. Graefes Arch. Clin. Exp. Ophthalmol. 2014, 252, 1483–1489. [Google Scholar] [CrossRef]
- Wang, X.; Sawada, T.; Sawada, O.; Saishin, Y.; Liu, P.; Ohji, M. Serum and Plasma Vascular Endothelial Growth Factor Concentrations Before and After Intravitreal Injection of Aflibercept or Ranibizumab for Age-Related Macular Degeneration. Am. J. Ophthalmol. 2014, 158, 738–744. [Google Scholar] [CrossRef]
- Avery, R.L.; Castellarin, A.A.; Steinle, N.C.; Dhoot, D.S.; Pieramici, D.J.; See, R.; Couvillion, S.; Nasir, M.A.; Rabena, M.D.; Maia, M.; et al. Systemic pharmacokinetics and pharmacodynamics of intravitreal aflibercept, bevacizumab abd ranibizumab. Retina 2017, 37, 1847–1858. [Google Scholar] [CrossRef] [PubMed]
- Avery, R.L.; Gordon, G.M. Systemic safety of prolonged monthly anti-vascular endothelial growth factor therapy for diabetic macular edema: A systematic review and meta-analysis. JAMA Ophthalmol. 2016, 134, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Thulliez, M.; Angoulvant, D.; Pisella, P.-J.; Bejan-Angoulvant, T. Overview of systematic reviews and meta-analyses on systemic adverse events associated with intravitreal anti-vascular endothelial growth factor medication use. JAMA Ophthalmol. 2018, 136, 557–566. [Google Scholar] [CrossRef]
- Sugimoto, M.; Handa, C.; Hirano, K.; Sunaya, T.; Kondo, M. Intravitreal aflibercept for diabetic macular edema in real-world clinical practice in Japan: 24-month outcomes. Graefes Arch. Clin. Exp. Ophthalmol. 2022, 260, 3489–3498. [Google Scholar] [CrossRef] [PubMed]
- Koike, Y.; Li, B.; Chen, Y.; Miyake, H.; Lee, C.; Chi, L.; Wu, R.; Inoue, M.; Uchida, K.; Kusunoki, M.; et al. Live imaging of fetal intra-abdominal organs using Two-photon laser-scanning microscopy. Methods Mol. Biol. 2018, 1752, 63–69. [Google Scholar]
- Fukuda, Y.; Hirata, Y.; Yoshimi, H.; Kojima, T.; Kobayashi, Y.; Yanagisawa, M.; Masaki, T. Endothelin is a potent secretagogue for atrial natriuretic peptide in cultured rat atrial myocytes. Biochem. Biophys. Res. Commun. 1988, 155, 167–172. [Google Scholar] [CrossRef]
- Zudaire, E.; Gambardella, L.; Kurcz, C.; Vermeren, S. A computational tool for quantitative analysis of vascular networks. PLoS ONE 2011, 6, e27385. [Google Scholar]
- Thulliez, M.; Angoulvant, D.; Le Lez, M.L.; Jonville-Bera, A.P.; Pisella, P.J.; Gueyffier, F.; Bejan-Angoulvant, T. Cardiovascular events and bleeding risk associated with intravitreal antivascular endothelial growth factor monoclonal antibodies: Systematic review and meta-analysis. JAMA Ophthalmol. 2014, 132, 1317–1326. [Google Scholar] [CrossRef]
- Kitchens, J.W.; Do, D.V.; Boyer, D.S.; Thompson, D.; Gibson, A.; Saroj, N.; Vitti, R.; Berliner, A.J.; Kaiser, P.K. Comprehensive review of ocular and systemic safety events with intravitreal aflibercept injection in randomized controlled trials. Ophthalmology 2016, 123, 1511–1520. [Google Scholar] [CrossRef]
- Sugimoto, M.; Wakamatsu, Y.; Miyata, R.; Nunome, T.; Tenma, Y.; Matsubara, H.; Kondo, M.; Wada, H.; Nakatani, K. Expression of vascular infarction-related molecules after anti-vascular endothelium growth factor treatment for diabetic macular edema. Sci. Rep. 2019, 9, 12373. [Google Scholar] [CrossRef]
- Shweiki, D.; Itin, A.; Neufeld, G.; Gitay-Goren, H.; Keshet, E. Patterns of expression of vascular endothelial growth factor (VEGF) and VEGF receptors in mice suggest a role in hormonally regulated angiogenesis. J. Clin. Investig. 1993, 91, 2235–2243. [Google Scholar] [CrossRef]
- Ropert, S.; Vignaux, O.; Mir, O.; Goldwasser, F. VEGF pathway inhibition by anticancer agent sunitinib and susceptibility to atherosclerosis plaque disruption. Investig. New Drugs 2011, 29, 1497–1499. [Google Scholar] [CrossRef] [PubMed]
- Boswell, C.A.; Ferl, G.Z.; Mundo, E.E.; Bumbaca, D.; Schweiger, M.G.; Theil, F.-P.; Fielder, P.J.; Khawli, L.A. Effects of anti-VEGF on predicted antibody biodistribution: Roles of vascular volume, interstitial volume, and blood flow. PLoS ONE 2011, 6, e17874. [Google Scholar] [CrossRef] [PubMed]
- Yu, L.; Wu, X.; Cheng, Z.; Lee, C.V.; LeCouter, J.; Campa, C.; Fuh, G.; Lowman, H.; Ferrara, N. Interaction between bevacizumab and murine VEGF-A: A reassessment. Investig. Ophthalmol. Vis. Sci. 2008, 49, 522–527. [Google Scholar] [CrossRef] [PubMed]
- Miki, K.; Miki, A.; Matsuoka, M.; Muramatsu, D.; Hackett, S.F.; Campochiaro, P.A. Effects of intraocular ranibizumab and bevacizumab in transgenic mice expressing human vascular endothelial growth factor. Ophthalmology 2009, 116, 1748–1754. [Google Scholar] [CrossRef]
- Irani, Y.; Scotney, P.; Nash, A.; Williams, K.A. Species cross-reactivity of antibodies used to treat ophthalmic conditions. Investig. Ophthalmol. Vis. Sci. 2016, 57, 586–591. [Google Scholar] [CrossRef]
- Feng, F.; Cheng, Y.; Liu, Q.-H. Bevacizumab treatment reduces retinal neovascularization in a mouse model of retinopathy of prematurity. Int. J. Ophthalmol. 2014, 7, 608–613. [Google Scholar]
- Akkoyun, I.; Karabay, G.; Haberal, N.; Dagdeviren, A.; Yilmaz, G.; Oto, S.; Erkanli, L.; Akova, Y.A. Structural consequences after intravitreal bevacizumab injection without increasing apoptotic cell death in a retinopathy of prematurity mouse model. Acta Ophthalmol. 2012, 90, 564–570. [Google Scholar] [CrossRef]
- Koike, Y.; Li, B.; Chen, Y.; Ganji, N.; Alganabi, M.; Miyake, H.; Lee, C.; Hock, A.; Wu, R.; Uchida, K.; et al. Live intravital intestine with blood flow visualization in neonatal mice using Two-photon laser scanning microscopy. Bio-Protocol 2021, 11, e3937. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pre (%) | 1 min (%) | 5 min (%) | 15 min (%) | ||
|---|---|---|---|---|---|
| PBS | S | 46.3 ± 1.1 | 44.5 ± 0.8 | 44.8 ± 0.4 | 43.2 ± 1.4 |
| V | 44.8 ± 0.4 | 45.2 ± 0.6 | 45.4 ± 0.3 | 45.7 ± 0.1 | |
| ET1 | S | 46.7 ± 5.7 | 28.1 ± 8.6 ** | 32.1 ± 15.2 * | 34.0 ± 3.8 |
| V | 45.4 ± 5.7 | 43.5 ± 4.2 | 38.7 ± 8.2 | 40.7 ± 6.7 | |
| Pre (%) | 1 min (%) | 5 min (%) | 15 min (%) | ||
|---|---|---|---|---|---|
| Bevacizumab | S | 46.1 ± 0.4 | 46.7 ± 0.4 | 46.7 ± 0.4 | 46.3 ± 0.6 |
| V | 45.0 ± 0.5 | 45.4 ± 0.6 | 44.7 ± 0.6 | 45.6 ± 0.4 | |
| Ranibizumab | S | 44.7 ± 1.3 | 45.0 ± 2.1 | 44.7 ± 2.1 | 44.6 ± 2.6 |
| V | 45.8 ± 0.5 | 46.2 ± 0.4 | 45.2 ± 1.3 | 45.6 ± 0.3 | |
| Aflibercept | S | 46.5 ± 1.2 | 46.2 ± 0.9 | 45.9 ± 1.1 | 46.1 ± 1.3 |
| V | 47.0 ± 0.2 | 46.9 ± 0.1 | 46.6 ± 0.7 | 46.9 ± 0.1 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ichio, A.; Sugimoto, M.; Koike, Y.; Toiyama, Y.; Kondo, M. Effects of Topical or Intravitreal Application of Anti-Vascular Endothelial Growth Factor on Density of Intestinal Blood Vessels of Mice. Medicina 2023, 59, 809. https://doi.org/10.3390/medicina59040809
Ichio A, Sugimoto M, Koike Y, Toiyama Y, Kondo M. Effects of Topical or Intravitreal Application of Anti-Vascular Endothelial Growth Factor on Density of Intestinal Blood Vessels of Mice. Medicina. 2023; 59(4):809. https://doi.org/10.3390/medicina59040809
Chicago/Turabian StyleIchio, Atsushi, Masahiko Sugimoto, Yuhki Koike, Yuji Toiyama, and Mineo Kondo. 2023. "Effects of Topical or Intravitreal Application of Anti-Vascular Endothelial Growth Factor on Density of Intestinal Blood Vessels of Mice" Medicina 59, no. 4: 809. https://doi.org/10.3390/medicina59040809