
Differences in Technical Aspects of Primary Sleeve Gastrectomy Prior to Redo Bariatric Surgery—A Multicenter Cohort Study (PROSS Study)
 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Surgical Technique and Perioperative Care
2.3. Statistical Analysis
2.4. Ethical Considerations
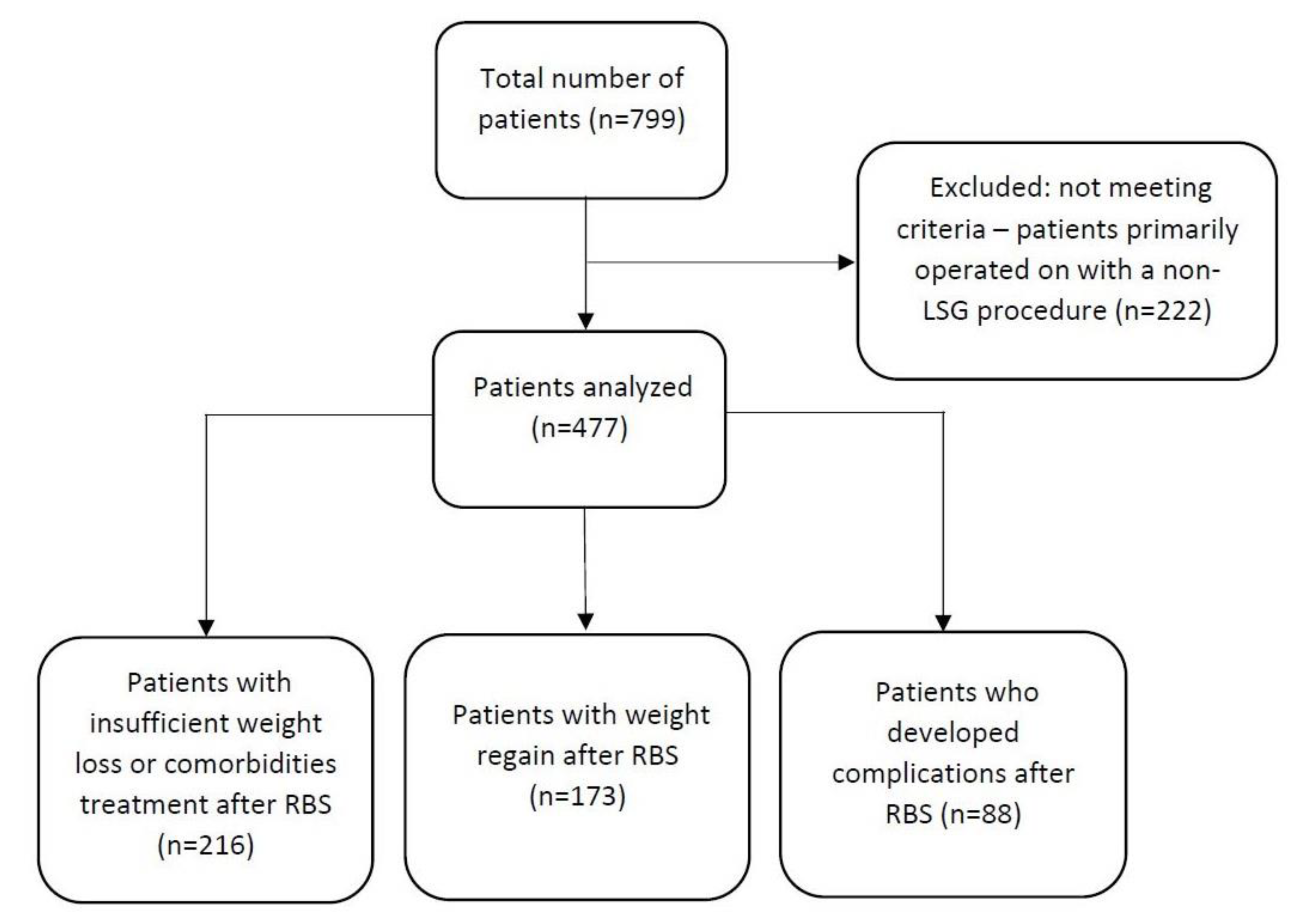
3. Results
3.1. Group Characteristics
3.2. Technical Aspects of Primary Sleeve Gastrectomy
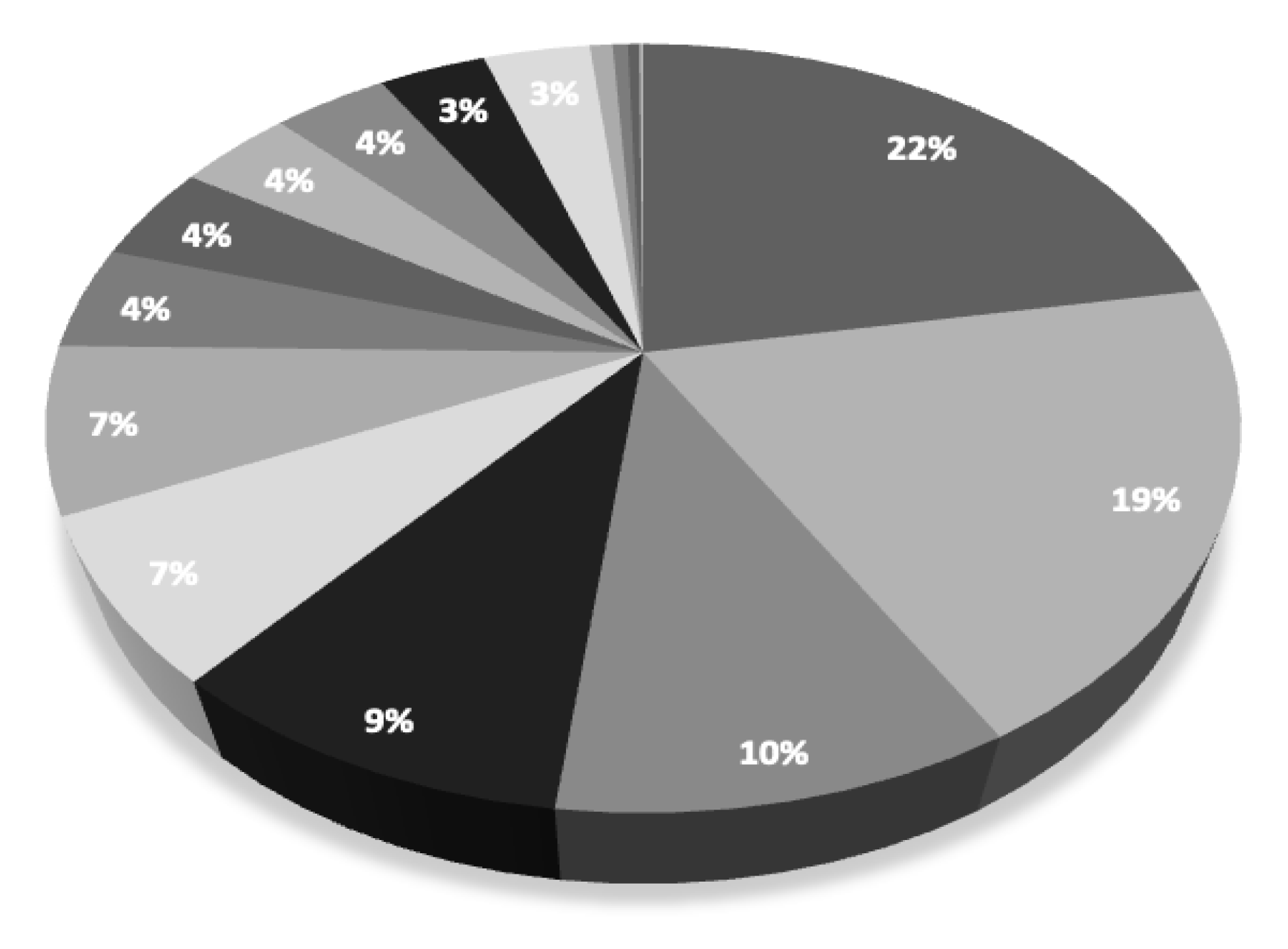
3.3. Revision Bariatric Procedures
4. Discussion
4.1. Technical Aspects of Using a Calibrating Bougie
4.2. Technical Aspects of the Distance from the Pylorus of the First Stapler
4.3. Technical Aspects of the Number of Stapler Firings
4.4. Technical Aspects of the Oversuturing the Staple Line
4.5. Technical Aspects of the Cruroplasty
4.6. Revisional Bariatric Surgery after Primary Sleeve Gastrectomy
4.7. Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Society for Metabolic and Bariatric Surgery. Estimate of Bariatric Surgery Numbers, 2011–2019. Available online: https://asmbs.org/resources/estimate-of-bariatric-surgery-numbers (accessed on 19 May 2022).
- Ozsoy, Z.; Demir, E. Which Bariatric Procedure Is the Most Popular in the World? A Bibliometric Comparison. Obes. Surg. 2018, 28, 2339–2352. [Google Scholar] [CrossRef] [PubMed]
- Cornejo-Pareja, I.; Clemente-Postigo, M.; Tinahones, F.J. Metabolic and Endocrine Consequences of Bariatric Surgery. Front. Endocrinol. 2019, 10, 626. [Google Scholar] [CrossRef]
- Park, J.Y.; Song, D.; Kim, Y.J. Causes and outcomes of revisional bariatric surgery: Initial experience at a single center. Ann. Surg. Treat. Res. 2014, 86, 295–301. [Google Scholar] [CrossRef] [PubMed]
- Qiu, J.; Lundberg, P.W.; Birriel, T.J.; Claros, L.; Stoltzfus, J.; El Chaar, M. Revisional Bariatric Surgery for Weight Regain and Refractory Complications in a Single MBSAQIP Accredited Center: What Are We Dealing with? Obes. Surg. 2018, 28, 2789–2795. [Google Scholar] [CrossRef] [PubMed]
- Gupta, M.; Singla, V.; Kumar, A.; Chekuri, R.; Kaustubh, Y.S.; Aggarwal, S. Banded Sleeve Gastrectomy vs Non-banded Sleeve Gastrectomy: A Systematic review and Meta-analysis. Obes. Surg. 2022, 32, 2744–2752. [Google Scholar] [CrossRef]
- Filho, A.M.; Silva, L.B.; Godoy, E.; Falcão, A.M.; de Quadros, L.G.; Filho, I.J.Z.; Campos, J.M.; Filho, L.V.R. Omentopexy in Sleeve Gastrectomy Reduces Early Gastroesophageal Reflux Symptoms. Surg. Laparosc. Endosc. Percutaneous Tech. 2019, 29, 155–161. [Google Scholar] [CrossRef]
- Andersson, D.P.; Eriksson-Hogling, D.; Bäckdahl, J.; Thorell, A.; Löfgren, P.; Rydén, M.; Arner, P.; Hoffstedt, J. Omentectomy in Addition to Bariatric Surgery—A 5-Year Follow-up. Obes. Surg. 2017, 27, 1115–1118. [Google Scholar] [CrossRef]
- Hady, H.R.; Olszewska, M.; Czerniawski, M.; Groth, D.; Diemieszczyk, I.; Pawluszewicz, P.; Kretowski, A.; Ladny, J.R.; Dadan, J. Different surgical approaches in laparoscopic sleeve gastrectomy and their influence on metabolic syndrome: A retrospective study. Medicine 2018, 97, e9699. [Google Scholar] [CrossRef]
- Von Elm, E.; Altman, D.G.; Egger, M.; Pocock, S.J.; Gøtzsche, P.C.; Vandenbroucke, J.P.; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: Guidelines for reporting observational studies. J. Clin. Epidemiol. 2008, 61, 344–349. [Google Scholar] [CrossRef]
- Lee, J.H.; Park, D.J. Sleeve Gastrectomy. In Bariatric and Metabolic Surgery; Springer: Berlin/Heidelberg, Germany, 2013; pp. 45–53. [Google Scholar] [CrossRef]
- Chang, P.-C.; Chen, K.-H.; Jhou, H.-J.; Chen, P.-H.; Huang, C.-K.; Lee, C.-H.; Chang, T.-W. Promising effects of 33 to 36 Fr. bougie calibration for laparoscopic sleeve gastrectomy: A systematic review and network meta-analysis. Sci. Rep. 2021, 11, 15217. [Google Scholar] [CrossRef]
- Ramos, A.C.; Bastos, E.L.D.S.; Ramos, M.G.; Bertin, N.T.S.; Galvão, T.D.; de Lucena, R.T.F.; Campos, J.M. TECHNICAL ASPECTS OF LAPAROSCOPIC SLEEVE GASTRECTOMY. Arq. Bras. Cir. Dig. ABCD 2015, 28, 65–68. [Google Scholar] [CrossRef]
- Gaillard, M.; Lainas, P.; Agostini, H.; Dagher, I.; Tranchart, H. Impact of the calibration bougie diametre during laparoscopic sleeve gastrectomy on the rate of postoperative staple-line leak (BOUST): Study protocol for a multicentre randomized prospective trial. Trials 2021, 22, 806. [Google Scholar] [CrossRef] [PubMed]
- Ellatif, M.A.; Abdallah, E.; Askar, W.; Thabet, W.; Aboushady, M.; Abbas, A.; El Hadidi, A.; Elezaby, A.; Salama, A.; Dawoud, I.; et al. Long term predictors of success after laparoscopic sleeve gastrectomy. Int. J. Surg. 2014, 12, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Hussein, A.H.; Khaled, I.; Faisal, M. The role of the surgical resection distance from the pylorus after laparoscopic sleeve gastrectomy: A prospective cohort study from an academic medical center in Egypt. Patient Saf. Surg. 2020, 14, 42. [Google Scholar] [CrossRef]
- Maklad, A.A.; Rizk, A.G.; Ahmed, M.Y.; Elamaary, M.K. Laparoscopic Sleeve Gastrectomy: 2 cm versus 6 cm Distance from the Pylorus. SVU-Int. J. Med. Sci. 2021, 4, 30–40. [Google Scholar] [CrossRef]
- Avlanmis, O.; Isil, R.G.; Burcu, B. Effect of Resection Distance from Pylorus on Weight Loss Outcomes in Laparoscopic Sleeve Gastrectomy. Obes. Surg. 2019, 29, 2731–2738. [Google Scholar] [CrossRef] [PubMed]
- Major, P.; Wysocki, M.; Pędziwiatr, M.; Pisarska, M.; Małczak, P.; Wierdak, M.; Dembiński, M.; Migaczewski, M.; Rubinkiewicz, M.; Budzyński, A. More stapler firings increase the risk of perioperative morbidity after laparoscopic sleeve gastrectomy. Videosurg. Other Miniinvasive Tech. 2018, 13, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Aiolfi, A.; Gagner, M.; Zappa, M.A.; Lastraioli, C.; Lombardo, F.; Panizzo, V.; Bonitta, G.; Cavalli, M.; Campanelli, G.; Bona, D. Staple Line Reinforcement During Laparoscopic Sleeve Gastrectomy: Systematic Review and Network Meta-analysis of Randomized Controlled Trials. Obes. Surg. 2022, 32, 1466–1478. [Google Scholar] [CrossRef]
- Sroka, G.; Milevski, D.; Shteinberg, D.; Mady, H.; Matter, I. Minimizing Hemorrhagic Complications in Laparoscopic Sleeve Gastrectomy—A Randomized Controlled Trial. Obes. Surg. 2015, 25, 1577–1583. [Google Scholar] [CrossRef]
- D’ugo, S.; Gentileschi, P.; Benavoli, D.; Cerci, M.; Gaspari, A.; Berta, R.D.; Moretto, C.; Bellini, R.; Basso, N.; Casella, G.; et al. Comparative use of different techniques for leak and bleeding prevention during laparoscopic sleeve gastrectomy: A multicenter study. Surg. Obes. Relat. Dis. 2014, 10, 450–454. [Google Scholar] [CrossRef]
- Aggarwal, S.; Sharma, A.P.; Ramaswamy, N. Outcome of Laparoscopic Sleeve Gastrectomy with and without Staple Line Oversewing in Morbidly Obese Patients: A Randomized Study. J. Laparoendosc. Adv. Surg. Tech. 2013, 23, 895–899. [Google Scholar] [CrossRef] [PubMed]
- Zarzycki, P.; Kulawik, J.; Małczak, P.; Rubinkiewicz, M.; Wierdak, M.; Major, P. Laparoscopic Sleeve Gastrectomy with Omentopexy: Is It Really a Promising Method?—A Systematic Review with Meta-analysis. Obes. Surg. 2021, 31, 2709–2716. [Google Scholar] [CrossRef] [PubMed]
- El-Serag, H.B.; Graham, D.Y.; Satia, J.A.; Rabeneck, L. Obesity Is an Independent Risk Factor for GERD Symptoms and Erosive Esophagitis. Am. J. Gastroenterol. 2005, 100, 1243–1250. [Google Scholar] [CrossRef] [PubMed]
- Shahraki, M.S.; Dehkordi, M.M.; Heydari, M.; Shahmiri, S.S.; Soheilipour, M.; Hajian, A. Cruroplasty added to laparoscopic sleeve gastrectomy; does it decrease postoperative incidence of de-novo acid reflux?: A randomised controlled trial. Ann. Med. Surg. 2021, 66, 102415. [Google Scholar] [CrossRef] [PubMed]
- Sabry, A.A.; Shafik, Y.S.; Sabry, A.M.; Wanees, A.N.F. Efficiency of Cruroplasty as a Treatment of Gastro-Esophageal Reflux Disease in Morbid Obese Patients with Hiatus Hernia during SleeveGastrectomy. Qjm Int. J. Med. 2021, 114, hcab097.015. [Google Scholar] [CrossRef]
- Boru, C.E.; Coluzzi, M.G.; de Angelis, F.; Silecchia, G. Long-Term Results After Laparoscopic Sleeve Gastrectomy with Concomitant Posterior Cruroplasty: 5-Year Follow-up. J. Gastrointest. Surg. 2019, 24, 1962–1968. [Google Scholar] [CrossRef]
- Małczak, P.; Pisarska-Adamczyk, M.; Zarzycki, P.; Wysocki, M.; Major, P. Hiatal hernia repair during laparoscopic sleeve gastrectomy: Systematic review and meta-analysis on gastroesophageal reflux disease symptoms changes. Ann. Surg. 2021, 93, 1–6. [Google Scholar] [CrossRef]
- Chen, W.; Feng, J.; Wang, C.; Wang, Y.; Yang, W.; Dong, Z. Effect of Concomitant Laparoscopic Sleeve Gastrectomy and Hiatal Hernia Repair on Gastroesophageal Reflux Disease in Patients with Obesity: A Systematic Review and Meta-analysis. Obes. Surg. 2021, 31, 3905–3918. [Google Scholar] [CrossRef]
- Li, S.; Jiao, S.; Zhang, S.; Zhou, J. Revisional Surgeries of Laparoscopic Sleeve Gastrectomy. Diabetes Metab. Syndr. Obes. Targets Ther. 2021, 14, 575–588. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Group 1 216 (45.28%) | Group 2 173 (36.27%) | Group 3 88 (18.45%) | |
|---|---|---|---|
| Age | 42.06 ± 11.09 | 38.42 ± 9.62 | 38.85 ± 10.75 |
| Sex | |||
| —women, n (%) | 215 (99.54%) | 129 (74.57%) | 20 (22.73%) |
| —men, n (%) | 1 (0.46%) | 44 (25.43%) | 68 (77.27%) |
| BMI max, median (range) | 50 (44.5–55.7) | 48.1 (43.3–53.3) | 43.8 (41.5–48) |
| BMI before primary SG, median (range) | 46.9 (42.4–52.5) | 46.8 (41.9–52.7) | 41.8 (38.3–47.3) |
| BMI after primary surgery, median (range) | 37.1 (33.5–41.7) | 31.8 (28–36.7) | 29.4 (17–32.6) |
| BMI before secondary (revisional) surgery, median (range) | 39.7 (35.1–45.2) | 40.9 (36.5–45.4) | 33.2 (29.4–36.6) |
| LOS primary SG, mean (SD) | 3.12 ± 2.68 | 3.77 ± 1.5 | 3.74 ± 2.77 |
| LOS revisional surgery, median (min-max) | 3.17 (1–36) | 3.49 (2–23) | 3.40 (2–25) |
| T2D, n (%) | 78 (36.11%) | 35 (20.23%) | 19 (21.59%) |
| HTN, n (%) | 119 (55.09%) | 66 (38.15%) | 32 (36.36%) |
| Post-SG GERD, n (%) | 16 (7.14%) | 10 (5.78%) | 72 (81.82%) |
| Group 1 | Group 2 | Group 3 | p-Value | |
|---|---|---|---|---|
| Bougie size | 36 (34–36) | 35 (34–36) | 36 (34–36) | 0.04 |
| Length from the pylorus of the first stapler: | 0.065 | |||
| 2 cm | 2 (0.99%) | 1 (0.58%) | 1 (1.14%) | |
| 4 cm | 99 (45.83%) | 98 (56.65%) | 49 (55.68%) | |
| 6 cm | 70 (32.41%) | 33 (19.08%) | 18 (20.45%) | |
| >6 cm | 18 (8.33%) | 9 (5.20%) | 8 (9.09%) | |
| no data | 27 (12.50%) | 32 (18.50%) | 12 (13.64%) | |
| Number of stapler firings. mean (median) | 5.53 (5) | 5.13 (5) | 5.55 (6) | 0.529 |
| Oversuturing the staple line n (%): | 0.002 | |||
| Yes | 64 (29.63%) | 28 (16.18%) | 14 (15.91%) | |
| No | 152 (70.37%) | 145 (83.82%) | 74 (84.09%) | |
| Cruroplasty n (%): | 0.549 | |||
| Yes | 6 (2.78%) | 6 (3.47%) | 1 (1.14%) | |
| No | 210 (99.22%) | 167 (96.53%) | 87 (98.86%) | |
| All Patients (477) | Group A (216) | Group B (173) | Group C (88) | |
|---|---|---|---|---|
| OAGB | 270 (56.6%) | 148 (68.52%) | 81 (46.82%) | 41 (46.59%) |
| RYGB | 150 (31.45%) | 37 (17.13%) | 70 (40.76%) | 43 (48.86%) |
| ReSG | 37 (7.76%) | 20 (9.26%) | 14 (8.09%) | 3 (3.41%) |
| SADI-S | 8 (1.68%) | 6 (2.78%) | 2 (1.16%) | 0 |
| SASI | 7 (1.47%) | 3 (1.39%) | 4 (2.31%) | 0 |
| other | 5 (1.05%) | 2 (0.93%) | 2 (1.16%) | 1 (1.14%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zarzycki, P.; Rymarowicz, J.; Małczak, P.; Pisarska-Adamczyk, M.; Mulek, R.; Binda, A.; Dowgiałło-Gornowicz, N.; Major, P.; PROSS Collaborative Study Group. Differences in Technical Aspects of Primary Sleeve Gastrectomy Prior to Redo Bariatric Surgery—A Multicenter Cohort Study (PROSS Study). Medicina 2023, 59, 799. https://doi.org/10.3390/medicina59040799
Zarzycki P, Rymarowicz J, Małczak P, Pisarska-Adamczyk M, Mulek R, Binda A, Dowgiałło-Gornowicz N, Major P, PROSS Collaborative Study Group. Differences in Technical Aspects of Primary Sleeve Gastrectomy Prior to Redo Bariatric Surgery—A Multicenter Cohort Study (PROSS Study). Medicina. 2023; 59(4):799. https://doi.org/10.3390/medicina59040799
Chicago/Turabian StyleZarzycki, Piotr, Justyna Rymarowicz, Piotr Małczak, Magdalena Pisarska-Adamczyk, Rafał Mulek, Artur Binda, Natalia Dowgiałło-Gornowicz, Piotr Major, and PROSS Collaborative Study Group. 2023. "Differences in Technical Aspects of Primary Sleeve Gastrectomy Prior to Redo Bariatric Surgery—A Multicenter Cohort Study (PROSS Study)" Medicina 59, no. 4: 799. https://doi.org/10.3390/medicina59040799