


Assessment of Labor Practices in Healthcare Using an Innovatory Framework for Sustainability



Abstract
:1. Introduction
2. Materials and Methods
- Designing the new reference framework according to the 4 quality cycle steps, by integrating sustainable development requirements, social responsibility standards, and ensuring compatibility with the applicable legislation and standards in the health sector;
- Exploring scientific medical literature and extracting scientifically confirmed evidence regarding the sustainability of medical practices;
- Designing the indicator matrix by connecting the quality cycle core activities with the social responsibility core subjects based on successful practices described in the scientific literature;
- Designing indicator content and evaluation grids based on the input of successful medical practices confirmed in scientific studies;
- Implementing a pilot frame of reference in a hospital for the practical validation of the theoretical studies.
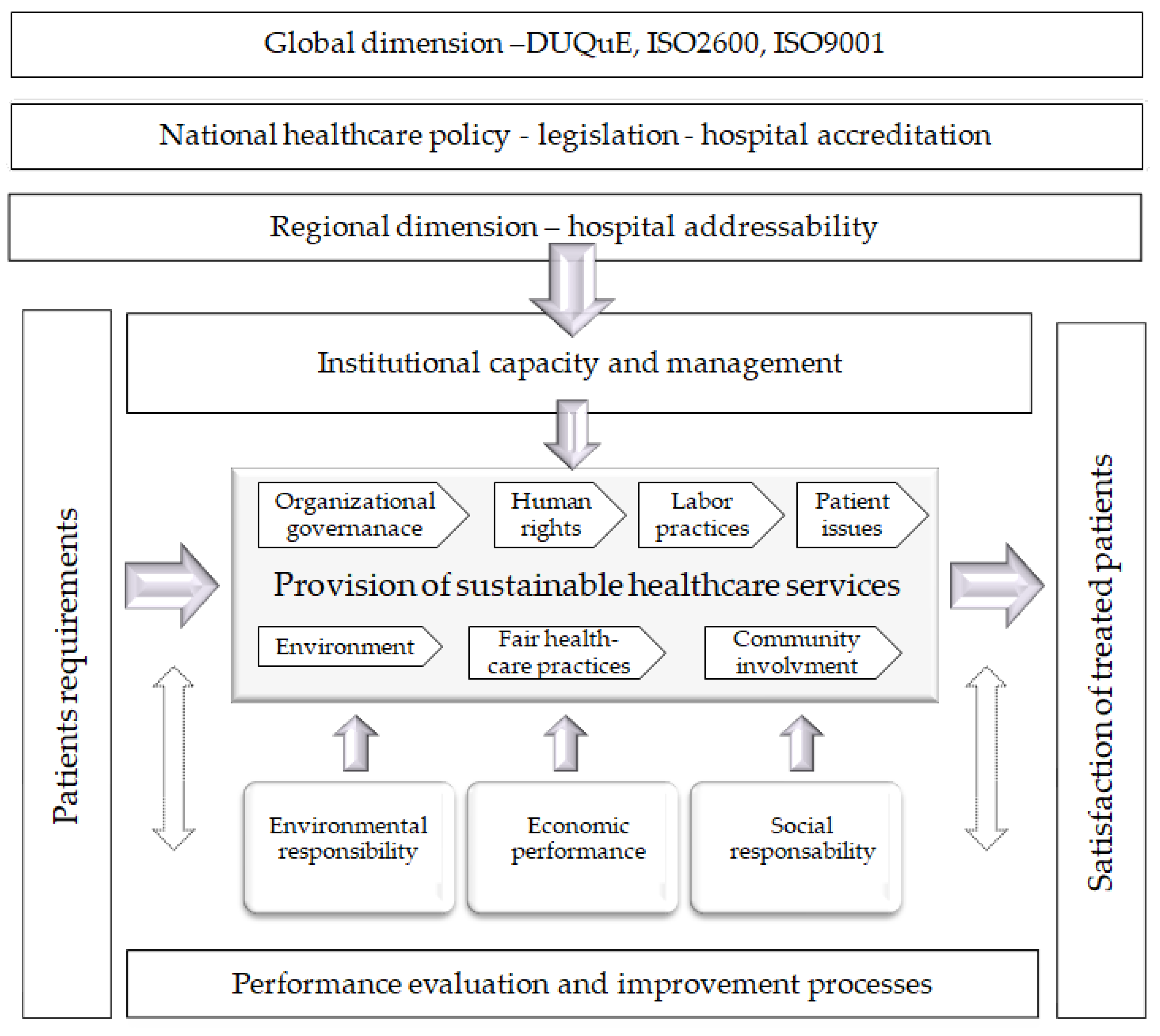
2.1. Areas of the New Reference Framework
2.2. Evidence of Sustainable Labor Practices
2.2.1. Indicators for the Design of Medical Service Provision
2.2.2. Indicators for Medical Service Provision
2.2.3. Indicators for Medical Service Evaluation
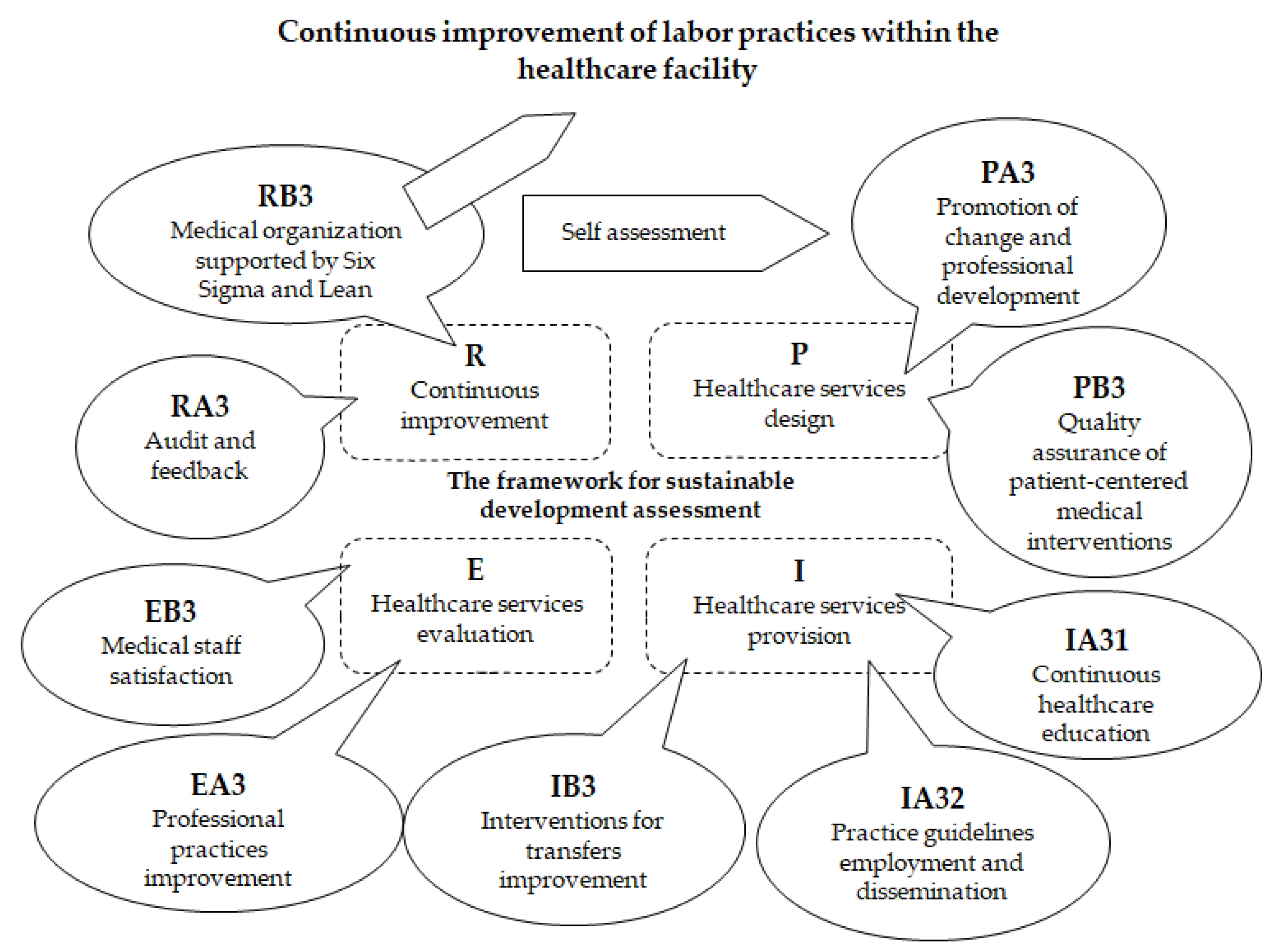
2.2.4. Continuous Improvement Indicators
2.3. Description of Indicators and Evaluation Grids
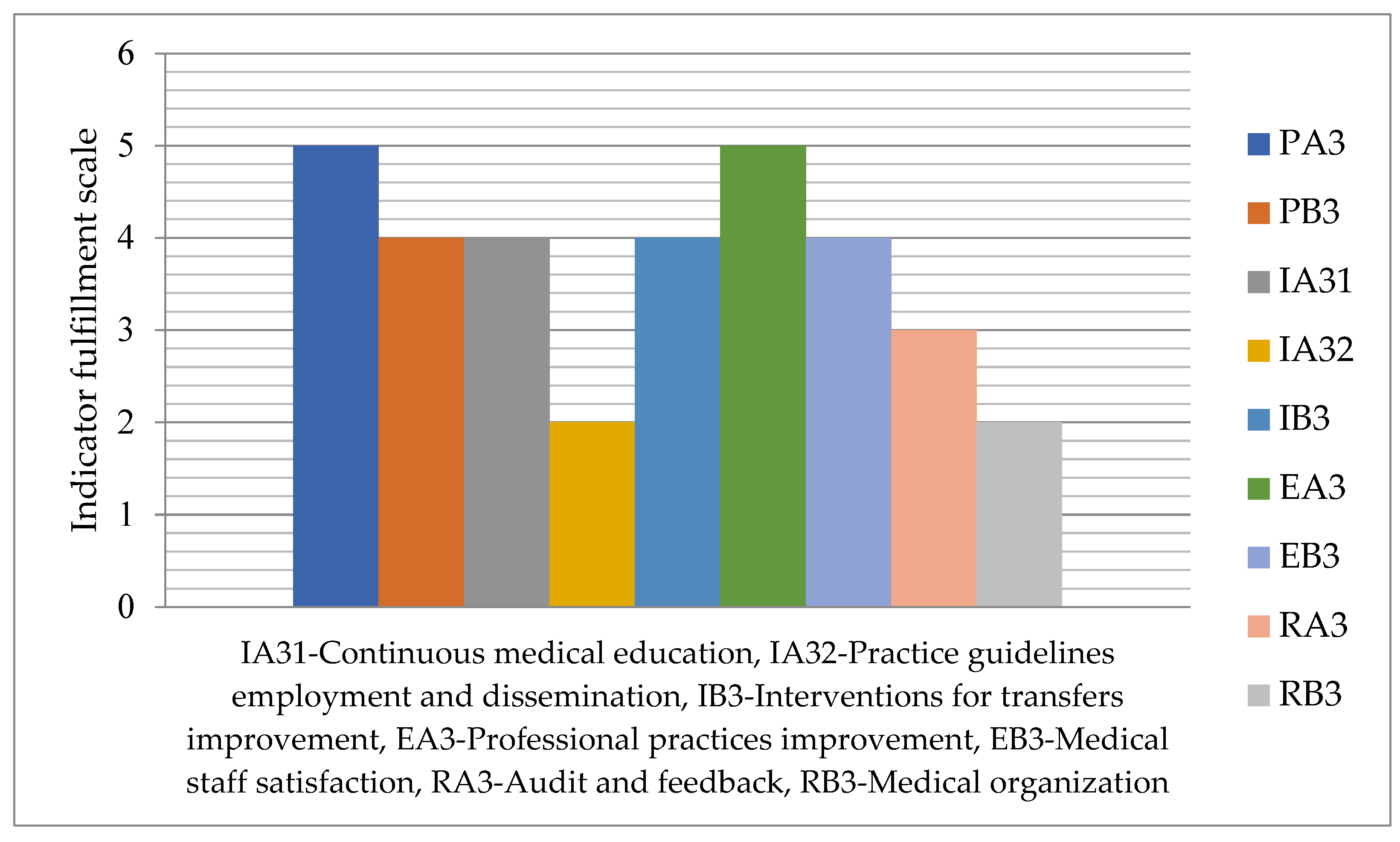
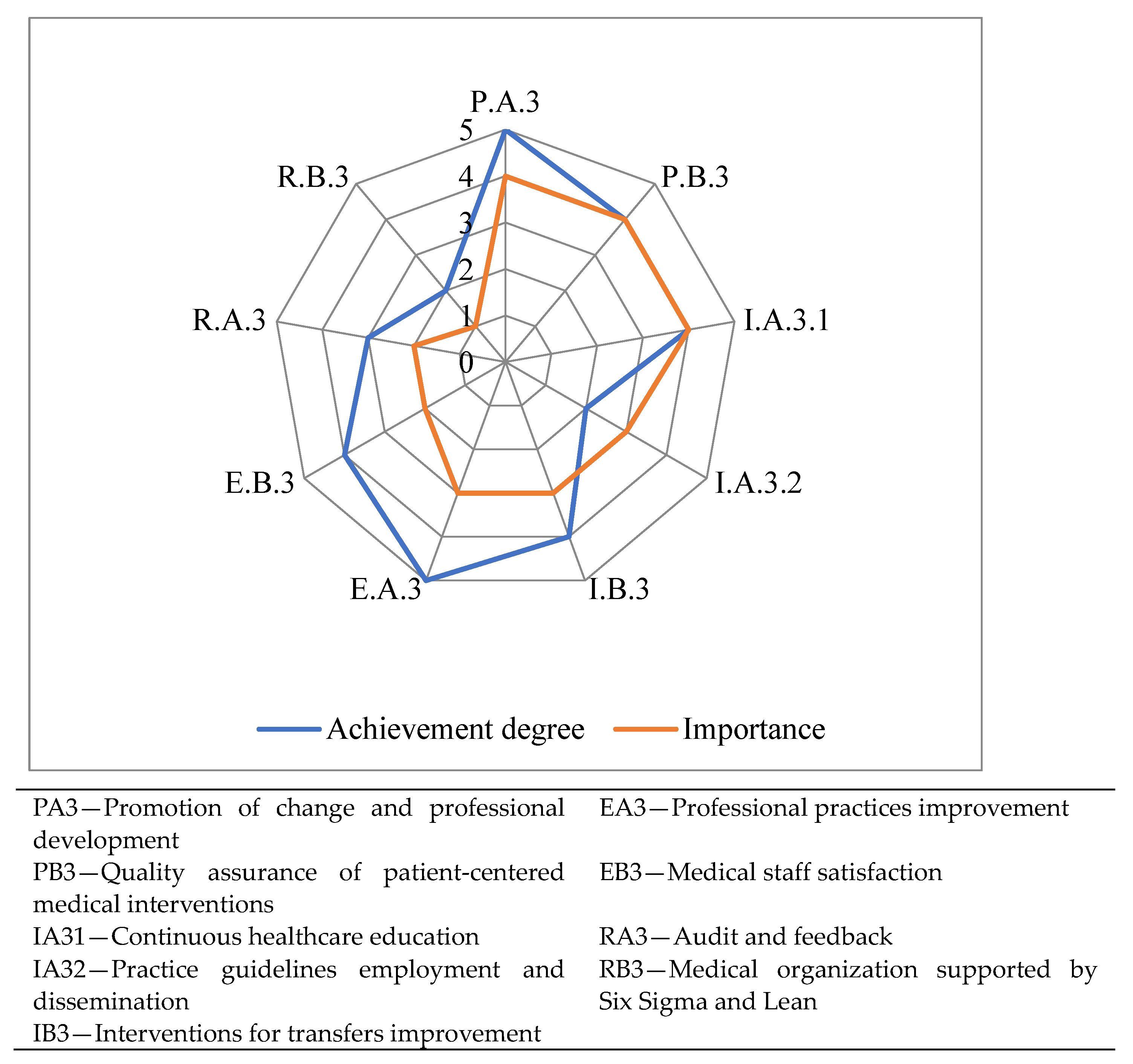
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Indicator | PA3—Promotion of Change and Professional Development |
|---|---|
| Description | Identification of actions to promote change and improvement of the organizational structures of healthcare facilities that facilitate the improvement of the care process provided by medical assistance services. Identification of actions to promote professional development. |
| Evaluation questions | Are the needs to change the organizational structures identified? Are opportunities to improve healthcare services identified? Are the professional development requirements and opportunities of the medical staff identified? Is staff consulted to identify actions to promote change and professional development? |
| Score [A] | Achievement | Content |
|---|---|---|
| 0 | Not relevant | – |
| 1 | Low | The promotion of change and professional development is a desire of the healthcare facility. |
| 2 | Satisfactory | Managerial analyses identify the needs to change the organizational structures. These changes are implemented according to the proposed action plans. |
| 3 | Good | Regular analysis of healthcare services, identification of improvement opportunities—implemented according to the proposed action plans. |
| 4 | Very good | Identification of the requirements and opportunities for professional development of the medical staff, design of professional development plans—implemented. |
| 5 | Excellent | The medical staff is regularly consulted to identify actions to promote change and professional development, and the results of the consultations are transposed into the action plans. |
| Indicator | PB3—Quality Assurance of Patient-Centered Medical Interventions |
|---|---|
| Description | Designing interventions supported by medical professionals:
|
| Evaluation questions | How are patient-centered medical interventions designed? Is training of medical staff on patient-centered care taking place? Are decision guidelines provided to improve clinical decision making? |
| Score [A] | Achievement | Content |
|---|---|---|
| 0 | Not relevant | – |
| 1 | Low | Some inputs can be used to design patient-centered medical interventions. |
| 2 | Satisfactory | There is an organizational framework that facilitates the design of patient-centered medical interventions. |
| 3 | Good | Patient-centered medical interventions are designed, and the designed services have output elements/specifications. |
| 4 | Very good | Regular staff training is conducted on patient-centered care and newly designed/improved services. Training includes the presentation of deliverables/specifications from the design stage. |
| 5 | Excellent | With the support of improved healthcare services, decision guidelines are developed and made available to medical staff to improve clinical decision-making. |
| Indicator | IA3—Continuous Healthcare Education |
|---|---|
| Description | Continuing medical education (CME) of health care professionals is intended to help professionals stay abreast of advances in patient care, adopt new, more beneficial care, and discontinue the use of costly diagnostic and therapeutic interventions that have limited benefit. CME tools and procedures include: vocational programs, collective education, professional information, clinical practice guidelines, reminders, opinion leaders’ interventions, audit and feedback. Continuing medical education improvement is supported by:
It is recognized that there are no unique professional education routes for every situation, and educators must select the appropriate methods according to the professional, social and economic particularities of the target group. |
| Evaluation questions | Is there a continuing medical education strategy/programme? What continuing medical education tools and techniques are used? The following elements are evaluated: vocational programs, collective education, professional information, clinical practice guidelines, reminders, opinion leaders’ interventions, audit and feedback. Are interactive programs on optimal versus effective care provided to practitioners and educators? Are there best practice outreach programs? Is electronic continuing medical education used? Is the information transmitted based on plain text only? What are the key characteristics that ensure the success of the applied continuing medical education program? The following elements are evaluated: information transmitted by personalities; targeting the interests and motivations of the group; teamwork; adapting the interventions to the needs of the audience; collaborative learning; the participation of top managers; awareness of the health unit’s needs; evidence of suboptimal use of health care; convincing peers of the benefits of behavior change. Do educators use approaches that focus on social, political, and economic particularities of the team and organization? |
| Score [A] | Achievement | Content |
|---|---|---|
| 0 | Not relevant | – |
| 1 | Low | There is a strategy and plan for the implementation of continuing healthcare education programs. |
| 2 | Satisfactory | Continuing medical education programs are currently conducted with the support of continuing medical education tools and techniques, and the information conveyed is based on plain text only. These include vocational programs, collective education, professional information, clinical practice guidelines, reminders, opinion leaders’ interventions, audit and feedback. |
| 3 | Good | Information programs on best practices are conducted, and continuing medical education is supported electronically. Interactive programs on optimal versus effective care are offered to practitioners and educators. |
| 4 | Very good | The key characteristics that ensure the success of the continuous healthcare education program are identified, such as: the information transmitted by personalities; targeting the interests and motivations of the group; teamwork; adapting the interventions to the needs of the audience; collaborative learning; the participation of top managers; awareness of the needs of the healthcare facility; evidence of suboptimal use of health care; convincing peers of the benefits of practice change. |
| 5 | Excellent | In continuing medical education, educators use approaches that focus on social, political and economic particularities of the team and organization. |
| Indicator | IA32—Practice Guidelines Employment and Dissemination |
|---|---|
| Description | By promoting evidence-based interventions, clinical guidelines improve patient care. Clinical guideline dissemination and implementation interventions consist of:
Clinical practice guidelines are more effective if they are tailored to local needs. |
| Evaluation questions | Are evidence-based interventions promoted through clinical guidelines? What are the actions to disseminate and implement the clinical guidelines? The following elements are evaluated: reminders (in electronic format or on paper); dissemination of educational materials; educational meetings; patient-directed interventions. Are clinical guidelines presented in portable, easy-to-access formats? Are patient-specific reminders used? Are clinical practice guidelines adapted to local needs? |
| Score [A] | Achievement | Content |
|---|---|---|
| 0 | Not relevant | – |
| 1 | Low | Organization promotes evidence-based interventions with the support of clinical guidelines. |
| 2 | Satisfactory | Actions to disseminate and implement clinical guidelines aim at: reminders in electronic format or on paper; dissemination of educational materials; educational meetings; patient-directed interventions. |
| 3 | Good | Clinical guidelines are presented in portable, easy-to-access formats. |
| 4 | Very good | Patient-specific reminders are used. |
| 5 | Excellent | The clinical practice guidelines are adapted to local needs by covering the specific aspects identified. |
| Indicator | IB3—Interventions for Transfers’ Improvement |
|---|---|
| Description | Critical transition points in patient care during hospitalization and after discharge are called handoffs. They appear:
|
| Evaluation questions | Are transfers properly identified as critical transition points in patient care during and after hospitalization? Intra-hospital transfers, admissions and discharges of patients are evaluated. Is there a nurse liaison in intensive care units? Are transfer protocols used? They can be assessed using the Formula (1) pit stop analogy and aviation expertise. Is voicemail-based semi-structured sign-off used for patients picked up by the emergency department? During the transfer of the patient from the oncology and hematology unit to critical care is the presence of an accompanying pharmacist ensured? Are technological solutions used? For example, the existence of electronic templates that download information from electronic medical records is evaluated. Is verbal information supplemented by written information? Are educational interventions used for information management, error recognition, teamwork and communication? (using role play, observation, evaluation and feedback). |
| Score [A] | Achievement | Content |
|---|---|---|
| 0 | Not relevant | – |
| 1 | Low | Intra-hospital transfers, admissions and discharges of patients are appropriately identified and treated as critical transition points in patient care during and after hospitalization. |
| 2 | Satisfactory | In intensive care units there is a liaison nurse. Transfer protocols exist and are enforced. Transfer protocols are evaluated by analogy with Formula 1 pit stops and aviation expertise. |
| 3 | Good | After discharge, continuity of care is planned to be achieved until the case is resolved. In the case of patients taken over by the emergency department, semi-structured disconnection based on voicemail is used. A pharmacist accompanies the transfer of the patient from the oncology and hematology unit to critical care. |
| 4 | Very good | Verbal information related to the transfer is supplemented with written information and technological solutions supported by IT systems are used to obtain information from electronic medical records. |
| 5 | Excellent | Transfers are improved through communication, teamwork, error recognition. Transfers are supported by information management training, using observation, role play, etc. |
| Indicator | EA3—Professional Practices Improvement |
|---|---|
| Description | The practice of health professionals and their results are positively influenced by opinion leaders. Due to their status within the community and the credibility gained, they constitute a support for quality improvement strategies through:
|
| Evaluation questions | Do local opinion leaders positively influence the practice of health professionals and their results? Are norms transmitted through the interventions of local opinion leaders? Do local opinion leaders contribute to modeling appropriate behavior? Is the use of new technologies disseminated among colleagues? |
| Score [A] | Achievement | Content |
|---|---|---|
| 0 | Not relevant | – |
| 1 | Low | The organization includes local opinion leaders that are recognized for their professionalism. |
| 2 | Satisfactory | Professional practice and health outcomes are positively influenced by local opinion leaders. |
| 3 | Good | Through the interventions of local opinion leaders, norms are transmitted and healthcare services are improved. |
| 4 | Very good | Local opinion leaders help shape appropriate behavior that results in improved healthcare services. |
| 5 | Excellent | The employment of innovative healthcare interventions is disseminated following the intervention of local opinion leaders, among professional colleagues. |
| Indicator | EB3—Medical Staff Satisfaction |
|---|---|
| Description | The degree of satisfaction of the medical staff regarding the working conditions and the delivery of medical services. |
| Evaluation questions | Is the satisfaction of medical staff measured in terms of working conditions and medical service delivery? Compared to the previous assessment, how did the degree of satisfaction of the medical staff evolve? |
| Score [A] | Achievement | Content |
|---|---|---|
| 0 | Not relevant | – |
| 1 | Low | There are updated questionnaires for evaluating medical staff satisfaction. |
| 2 | Satisfactory | Based on a procedure, questionnaires are periodically distributed to evaluate medical staff satisfaction. |
| 3 | Good | Periodically, the degree of medical staff satisfaction is measured in terms of working conditions and medical service delivery. |
| 4 | Very good | Compared to previous evaluation, there is an improved degree of satisfaction. |
| 5 | Excellent | Improvement measures are established to increase the satisfaction of the medical staff. |
| Indicator | RA3—Audit and Feedback |
|---|---|
| Description | Audit and feedback are essential quality improvement tools that can be used individually or in combination with other methods. Professionals are expected to improve activities when poor care outcomes and process deficiencies are highlighted. Audit and feedback processes are characterized by:
|
| Evaluation questions | Is there a body of designated auditors? What is the frequency of audits? Is it performed repetitively? What performance level does the audit report to? Are the audit results documented? Do the conclusions contain the necessary direction of change? Do the conclusions contain explicit objectives and an action plan? In what format and how is feedback delivered? Does it consider the profession of the audited/feedback recipient? Is the context in which the audit is carried out considered? Is the behavior of the audit participants analyzed? |
| Score [A] | Achievement | Content |
|---|---|---|
| 0 | Not relevant | – |
| 1 | Low | In the healthcare facility there is a body of designated auditors, who have the necessary level of training to carry out audits. |
| 2 | Satisfactory | There is an annual audit plan that establishes the frequency of audits in each compartment. The audit plan establishes the performance level to which the audit reports. |
| 3 | Good | The audit results are documented, and the audit conclusions contain proposals for improving the activity in the audited department. |
| 4 | Very good | Based on the proposals made to improve the activity, an action plan is drawn up with explicit objectives, activities, responsibilities and allocated resources. |
| 5 | Excellent | The behavior of the participants in the audit and the context in which the audit is carried out are analyzed. The format and mode of transmission of audit feedback takes into account the profession of the audited/recipient. |
| Indicator | RB3—Medical Organization Supported by Six Sigma and Lean |
|---|---|
| Description | Continuous improvement in the quality of healthcare can be achieved with the help of data provided by Six Sigma and Lean. Both tools use data and quantitative methods to improve quality and ensure progress towards an assumed goal. Combined use provides processes focused on measuring and eliminating errors (Six Sigma) and ensuring an efficient and value-added workflow (Lean). They facilitate improved care processes and clinical outcomes, as well as the economic efficiency of healthcare organizations. |
| Evaluation questions | Is the Lean method used to continuously improve the quality of healthcare? Is the Six Sigma method used to continuously improve the quality of healthcare? What are the errors measured and eliminated using the Six Sigma method? Can you describe the extent to which the efficiency and added value of the work flow has increased by applying the Lean method? |
| Score [A] | Achievement | Content |
|---|---|---|
| 0 | Not relevant | – |
| 1 | Low | Data are collected and quantitative methods are used to improve quality and ensure progress towards the stated goal. |
| 2 | Satisfactory | The healthcare facility uses Six Sigma and Lean methods in a cycle of continuous improvement of the medical care quality. |
| 3 | Good | The combined use of the two methods provides processes focused on measuring and eliminating errors (Six Sigma) and ensuring an efficient and value-added workflow (Lean). |
| 4 | Very good | The use of Six Sigma and Lean in the medical organization results in improved clinical outcomes, care processes and financial performance of the healthcare facility. |
| 5 | Excellent | Data are collected and quantitative methods are used to improve quality and ensure progress towards the stated goal. |
References
- Enriquez-Puga, A.; Baker, R.; Paul, S.; Villoro-Valdes, R. Effect of educational outreach on general practice prescribing of antibiotics and antidepressants: A two-year randomised controlled trial. Scand. J. Prim. Health Care 2009, 27, 195–201. [Google Scholar] [CrossRef] [PubMed]
- Forsetlund, L.; Bjørndal, A.; Rashidian, A.; Jamtvedt, G.; O’Brien, M.A.; Wolf, F.; Davis, D.; Odgaard-Jensen, J.; Oxman, A.D. Continuing education meetings and workshops: Effects on professional practice and health care outcomes. Cochrane Database Syst. Rev. 2009, 2, CD003030. [Google Scholar] [CrossRef] [PubMed]
- Yang, A.; Farmer, P.; McGahan, A. ‘Sustainability’ in global health. Glob. Public Health 2010, 5, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Moldovan, F. New Approaches and Trends in Health Care. Procedia Manuf. 2018, 22, 947–951. [Google Scholar] [CrossRef]
- Moldovan, F. Recent trends in bioprinting. Procedia Manuf. 2019, 32, 95–101. [Google Scholar] [CrossRef]
- Edwards, R.L.; Markaki, A.; Shirey, M.R.; Patrician, P.A. A Model Operationalizing Sustainability in Global Nursing. Nurs. Outlook 2020, 68, 345–354. [Google Scholar] [CrossRef]
- Coiera, E. Putting the technical back into socio-technical systems research. Int. J. Med. Inform. 2007, 76, S98–S103. [Google Scholar] [CrossRef]
- Pavlovskaia, E. Sustainability criteria: Their indicators, control, and monitoring (with examples from the biofuel sector). Environ. Sci. Eur. 2014, 26, 17. [Google Scholar] [CrossRef]
- Isaksson, R. Total quality management for sustainable development: Process based system models. Bus. Process Manag. J. 2006, 12, 632–645. [Google Scholar] [CrossRef]
- Zdravkovic, D.; Radukic, S. Institutional framework for sustainable development in Serbia. Monten. J. Econ. 2012, 8, 27–36. [Google Scholar]
- Groene, O.; Kringos, D.; Sunol, R. On behalf of the DUQuE Project. Seven Ways to Improve Quality and Safety in Hospitals. An Evidence-Based Guide. DUQuE Collaboration. 2014. Available online: www.duque.eu (accessed on 7 January 2023).
- ANMCS. Manualul Standardelor de Acreditare a Unitatilor Sanitare cu Paturi (Manual of Accreditation Standards for Sanitary Units with Beds). 2020. Available online: https://anmcs.gov.ro/web/wp-content/uploads/2021/02/Manualul-standardelor-de-acreditare-2020.pdf (accessed on 7 January 2023).
- ANMCS. Standardele Autoritatii Nationale de Management al Calitatii in Sanatate Pentru Serviciile de Sanatate Acordate in Regim Ambulatoriu (Standards of the National Authority for Quality Management in Health for Outpatient Health Services). Available online: https://anmcs.gov.ro/web/standarde-ambulatoriu/ (accessed on 7 January 2023).
- Moldovan, F.; Blaga, P.; Moldovan, L.; Bataga, T. An Innovative Framework for Sustainable Development in Healthcare: The Human Rights Assessment. Int. J. Environ. Res. Public Health 2022, 19, 2222. [Google Scholar] [CrossRef] [PubMed]
- Moukhafi, S.; Benabdelhadi, A. Hospital quality management: A historical foundation. Rev. Econ. Gest. Soc. 2021, 1, 1–14. [Google Scholar]
- Sack, C.; Lütkes, P.; Günther, W.; Erbel, R.; Jöckel, K.H.; Holtmann, G.J. Challenging the holy grail of hospital accreditation: A cross sectional study of inpatient satisfaction in the field of cardiology. BMC Health Serv. Res. 2010, 10, 120. [Google Scholar] [CrossRef] [PubMed]
- Alaraki, M.S. The impact of critical total quality management practices on hospital performance in the Ministry of Health hospitals in Saudi Arabia. Qual. Manag. Health Care 2014, 23, 59–63. [Google Scholar] [CrossRef]
- Greenfield, D.; Braithwaite, J. Health sector accreditation research: A systematic review. Int. J. Qual. Health 2008, 20, 172–183. [Google Scholar] [CrossRef]
- Flodgren, G.; Pomey, M.P.; Taber, S.A.; Eccles, M.P. Effectiveness of external inspection of compliance with standards in improving healthcare organization behaviour, healthcare professional behaviour or patient outcomes. Cochrane Database Syst. Rev. 2011, 11, CD008992. [Google Scholar]
- Alkhenizan, A.; Shaw, C. Impact of accreditation on the quality of healthcare services: A systematic review of the literature. Ann. Saudi Med. 2011, 31, 407–416. [Google Scholar] [CrossRef]
- Lam, M.B.; Figueroa, J.F.; Feyman, Y.; Reimold, K.E.; Orav, E.J.; Jha, A.K. Association between patient outcomes and accreditation in US hospitals: Observational study. BMJ 2018, 363, k4011. [Google Scholar] [CrossRef]
- Mansour, W.; Boyd, A.; Walshe, K. The development of hospital accreditation in low-and middle-income countries: A literature review. Health Policy Plan. 2020, 35, 684–700. [Google Scholar] [CrossRef]
- Hilty, D.M.; Liu, H.Y.; Stubbe, D.; Teshima, J. Defining Professional Development in Medicine, Psychiatry, and Allied Fields. Psychiatr. Clin. N. Am. 2019, 42, 337–356. [Google Scholar] [CrossRef]
- James, A.H.; Stacey-Emile, G. Action learning: Staff development, implementing change, interdisciplinary working and leadership. Nurs. Manag. 2019, 26, 36–41. [Google Scholar]
- Hunt, J.; Brannan, E.; Sexson, S. Lifelong Learning for Professional Development in Psychiatry: Pedagogy, Innovations, and Maintenance of Certification. Psychiatr. Clin. N. Am. 2019, 42, 425–437. [Google Scholar] [CrossRef] [PubMed]
- Chidharla, A.; Utengen, A.; Attai, D.J.; Drake, E.K.; van Londen, G.J.; Subbiah, I.M.; Henry, E.; Murphy, M.; Barry, M.M.; Manochakian, R.; et al. Social Media and Professional Development for Oncology Professionals. JCO Oncol. Pract. 2022, 18, 566–571. [Google Scholar] [CrossRef] [PubMed]
- Cowley, S. Professional development and change in a learning organization. J. Adv. Nurs. 1995, 21, 965–974. [Google Scholar] [CrossRef] [PubMed]
- Rohrbasser, A.; Wong, G.; Mickan, S.; Harris, J. Understanding how and why quality circles improve standards of practice, enhance professional development and increase psychological well-being of general practitioners: A realist synthesis. BMJ Open 2022, 12, e058453. [Google Scholar] [CrossRef]
- Nelson, K.M.; Helfrich, C.; Sun, H.; Hebert, P.L.; Liu, C.F.; Dolan, E.; Taylor, L.; Wong, E.; Maynard, C.; Hernandez, S.E.; et al. Implementation of the Patient-Centered Medical Home in the Veterans Health Administration: Associations with Patient Satisfaction, Quality of Care, Staff Burnout, and Hospital and Emergency Department Use. JAMA Intern. Med. 2014, 174, 1350–1358. [Google Scholar] [CrossRef]
- Pham, J.C.; Trueger, N.S.; Hilton, J.; Khare, R.K.; Smith, J.P.; Bernstein, S.L. Interventions to improve patient-centered care during times of emergency department crowding. Acad. Emerg. Med. 2011, 18, 1289–1294. [Google Scholar] [CrossRef]
- Constand, M.K.; MacDermid, J.C.; DalBello-Haas, V.; Law, M. Scoping review of patient-centered care approaches in healthcare. BMC Health Serv. Res. 2014, 14, 271. [Google Scholar] [CrossRef]
- Groene, O.; Sunol, R.; Klazinga, N.S.; Wang, A.; Dersarkissian, M.; Thompson, C.A.; Thompson, A.; Arah, O.A.; Kringos, D.; Lombarts, M.; et al. Involvement of patients or their representatives in quality management functions in EU hospitals: Implementation and impact on patient-centred care strategies. Int. J. Qual. Health Care 2014, 26, 81–91. [Google Scholar] [CrossRef]
- Tapuria, A.; Porat, T.; Kalra, D.; Dsouza, G.; Xiaohui, S.; Curcin, V. Impact of patient access to their electronic health record: Systematic review. Inform. Health Soc. Care 2021, 46, 192–204. [Google Scholar] [CrossRef]
- Asmat, K.; Dhamani, K.; Gul, R.; Froelicher, E.S. The effectiveness of patient-centered care vs. usual care in type 2 diabetes self-management: A systematic review and meta-analysis. Front. Public Health 2022, 10, 994766. [Google Scholar] [CrossRef] [PubMed]
- Fossey, J.; Masson, S.; Stafford, J.; Lawrence, V.; Corbett, A.; Ballard, C. The disconnect between evidence and practice: A systematic review of person-centred interventions and training manuals for care home staff working with people with dementia. Int. J. Geriatr. Psychiatry 2014, 29, 797–807. [Google Scholar] [CrossRef] [PubMed]
- Ding, X.; Zhu, L.; Zhang, R.; Wang, L.; Wang, T.T.; Latour, J.M. Effects of family-centred care interventions on preterm infants and parents in neonatal intensive care units: A systematic review and meta-analysis of randomised controlled trials. Aust. Crit. Care 2019, 32, 63–75. [Google Scholar] [CrossRef] [PubMed]
- VanNieuwenborg, L.; Goossens, M.; DeLepeleire, J.; Schoenmakers, B. Continuing medical education for general practitioners: A practice format. Postgrad. Med. J. 2016, 92, 217–222. [Google Scholar] [CrossRef] [PubMed]
- François, P.; Vinck, D.; Labarère, J.; Reverdy, T.B.; Peyrin, J.C. Assessment of an intervention to train teaching hospital care providers in quality management. Qual. Saf. Health Care 2005, 14, 234–239. [Google Scholar] [CrossRef]
- Farmer, A.P.; Légaré, F.; Turcot, L.; Grimshaw, J.; Harvey, E.; McGowan, J.; Wolf, F.M. Printed educational materials: Effects on professional practice and health care outcomes. Cochrane Database Syst. Rev. 2008, 3, CD004398. [Google Scholar]
- Pantoja, T.; Grimshaw, J.M.; Colomer, N.; Castañon, C.; Martelli, J.L. Manually-generated reminders delivered on paper: Effects on professional practice and patient outcomes. Cochrane Database Syst. Rev. 2019, 12, CD001174. [Google Scholar] [CrossRef]
- Grimshaw, J.; Eccles, M.; Thomas, R.; MacLennan, G.; Ramsay, C.; Fraser, C.; Vale, L. Toward evidence-based quality improvement: Evidence (and its limitations) of the effectiveness of guideline dissemination and implementation strategies 1966–1998. J. Gen. Intern. Med. 2006, 21 (Suppl. S2), S14–S20. [Google Scholar]
- Ivers, N.; Jamtvedt, G.; Flottorp, S.; Young, J.M.; Odgaard-Jensen, J.; French, S.; O’Brien, M.A.; Johansen, M.; Grimshaw, J.; Oxman, A.D. Audit and feedback: Effects on professional practice and healthcare outcomes. Cochrane Database Syst. Rev. 2012, 6, CD000259. [Google Scholar] [CrossRef]
- Morello, R.T.; Lowthian, J.A.; Barker, A.L.; McGinnes, R.; Dunt, D.; Brand, C. Strategies for improving patient safety culture in hospitals: A systematic review. BMJ Qual. Saf. 2013, 22, 11–18. [Google Scholar] [CrossRef]
- Scott, T.; Mannion, R.; Marshall, M.; Davies, H. Does organisational culture influence health care performance? A review of the evidence. J. Health Serv. Res. Policy 2003, 8, 105–117. [Google Scholar] [CrossRef] [PubMed]
- Curry, L.A.; Brault, M.; Linnander, E.L.; McNatt, Z.; Brewster, A.L.; Cherlin, E.; Flieger, S.P.; Ting, H.H.; Bradley, E.H. Influencing organisational culture to improve hospital performance in care of patients with acute myocardial infarction: A mixed-methods intervention study. BMJ Qual. Saf. 2018, 27, 207–217. [Google Scholar] [CrossRef] [PubMed]
- Parmelli, E.; Flodgren, G.; Beyer, F.; Baillie, N.; Schaafsma, M.E.; Eccles, M.O. The effectiveness of strategies to change organisational culture to improve healthcare performance: A systematic review. Implement. Sci. 2011, 6, 33. [Google Scholar] [CrossRef]
- Rosenberg, M.E. An Outcomes-Based Approach across the Medical Education Continuum. Trans. Am. Clin. Climatol. Assoc. 2018, 129, 325–340. [Google Scholar] [PubMed]
- Fischer, W.W.; Reel, L.B. Total quality management (TQM) in a hospital library: Identifying service benchmarks. Bull. Med. Libr. Assoc. 1992, 80, 347–352. [Google Scholar]
- Fervers, B.; Carretier, J.; Bataillard, A. Clinical practice guidelines. J. Visc. Surg. 2010, 147, e341–e349. [Google Scholar] [CrossRef]
- Grimshaw, J.M.; Thomas, R.E.; MacLennan, G.; Fraser, C.; Ramsay, C.R.; Vale, L.; Whitty, P.; Eccles, M.P.; Matowe, L.; Shirran, L.; et al. Effectiveness and efficiency of guideline dissemination and implementation strategies. Health Technol. Assess. 2004, 8, 1–72. [Google Scholar] [CrossRef]
- Murad, M.H. Clinical Practice Guidelines: A Primer on Development and Dissemination. Mayo Clin. Proc. 2017, 92, 423–433. [Google Scholar] [CrossRef]
- Arora, V.M.; Manjarrez, E.; Dressler, D.D.; Basaviah, P.; Halasyamani, L.; Kripalani, S. Hospitalist handoffs: A systematic review and task force recommendations. J. Hosp. Med. 2009, 4, 433–440. [Google Scholar] [CrossRef]
- Braet, A.; Weltens, C.; Sermeus, W. Effectiveness of discharge interventions from hospital to home on hospital readmissions: A systematic review. JBI Database Syst. Rev. Implement. Rep. 2016, 14, 106–173. [Google Scholar] [CrossRef]
- Roukis, T.S. White Papers, Position Papers, Clinical Consensus Statements, and Clinical Practice Guidelines: Future Directions for ACFAS. J. Foot Ankle Surg. 2015, 54, 151–152. [Google Scholar] [CrossRef] [PubMed]
- Gordon, M.; Hill, E.; Stojan, J.N.; Daniel, M. Educational Interventions to Improve Handover in Health Care: An Updated Systematic Review. Acad. Med. 2018, 93, 1234–1244. [Google Scholar] [CrossRef] [PubMed]
- Shepperd, S.; Lannin, N.A.; Clemson, L.M.; McCluskey, A.; Cameron, I.D.; Barras, S.L. Discharge planning from hospital to home. Cochrane Database Syst. Rev. 2013, 1, CD000313. [Google Scholar]
- Emes, M.; Smith, S.; Ward, S.; Smith, A. Improving the patient discharge process: Implementing actions derived from a soft systems methodology study. Health Syst. 2018, 8, 117–133. [Google Scholar] [CrossRef] [PubMed]
- Mas, M.A.; Inzitari, M.; Sabaté, S.; Santaeugènia, S.J.; Miralles, R. Hospital-at-home Integrated Care Programme for the management of disabling health crises in older patients: Comparison with bed-based Intermediate Care. Age Ageing 2017, 46, 925–931. [Google Scholar] [CrossRef]
- Allen, D.; Rixson, L. How has the impact of ‘care pathway technologies’ on service integration in stroke care been measured and what is the strength of the evidence to support their effectiveness in this respect? Int. J. Evid. Based Healthc. 2008, 6, 78–110. [Google Scholar]
- Roy, J.; Adhikary, K.; Kar, S.; Pamučar, D. A rough strength relational DEMATEL model for analysing the key success factors of hospital service quality. Decis. Mak. Appl. Manag. Eng. 2018, 1, 121–142. [Google Scholar] [CrossRef]
- Carpenter, C.R.; Sherbino, J. How does an “opinion leader” influence my practice? CJEM 2010, 12, 431–434. [Google Scholar] [CrossRef]
- Holliday, J.; Audrey, S.; Campbell, R.; Moore, L. Identifying Well-Connected Opinion Leaders for Informal Health Promotion: The Example of the ASSIST Smoking Prevention Program. Health Commun. 2016, 31, 946–953. [Google Scholar] [CrossRef]
- Parand, A.; Dopson, S.; Renz, A.; Vincent, C.A. The role of hospital managers in quality and patient safety: A systematic review. BMJ Open 2014, 4, e005055. [Google Scholar] [CrossRef]
- Thomson O’Brien, M.A.; Oxman, A.D.; Haynes, R.B.; Davis, D.A.; Freemantle, N.; Harvey, E.L. Local opinion leaders: Effects on professional practice and health care outcomes. Cochrane Database Syst. Rev. 2000, 2, CD000125. [Google Scholar]
- Flodgren, G.; Parmelli, E.; Doumit, G.; Gattellari, M.; O’Brien, M.A.; Grimshaw, J.; Eccles, M.P. Local opinion leaders: Effects on professional practice and health care outcomes. Cochrane Database Syst. Rev. 2011, (8):CD000125. [Google Scholar] [CrossRef] [PubMed]
- Flodgren, G.; O’Brien, M.A.; Parmelli, E.; Grimshaw, J.M. Local opinion leaders: Effects on professional practice and healthcare outcomes. Cochrane Database Syst. Rev. 2019, (6):CD000125. [Google Scholar] [CrossRef] [PubMed]
- Doumit, G.; Gattellari, M.; Grimshaw, J.; O’Brien, M.A. Local opinion leaders: Effects on professional practice and health care outcomes. Cochrane Database Syst. Rev. 2007, (1):CD000125. [Google Scholar]
- Elliott, T.E.; Murray, D.M.; Oken, M.M.; Johnson, K.M.; Braun, B.L.; Elliott, B.A.; Post-White, J. Improving cancer pain management in communities: Main results from a randomized controlled trial. J. Pain Symptom Manag. 1997, 13, 191–203. [Google Scholar] [CrossRef]
- Rangachari, P. The Strategic Management of Organizational Knowledge Exchange Related to Hospital Quality Measurement and Reporting. Qual. Manag. Health Care 2008, 17, 252–269. [Google Scholar] [CrossRef] [PubMed]
- Rangachari, P. Knowledge sharing networks related to hospital quality measurement and reporting. Health Care Manag. Rev. 2008, 33, 253–263. [Google Scholar] [CrossRef]
- Locock, L.; Dopson, S.; Chambers, D.A.; Gabbay, J. Understanding the Role of Opinion Leaders in Improving Clinical Effectiveness. Soc. Sci. Med. 2001, 53, 745–757. [Google Scholar] [CrossRef]
- Rotar, A.M.; Botje, D.; Klazinga, N.S.; Lombarts, K.M.; Groene, O.; Sunol, R.; Plochg, T. The involvement of medical doctors in hospital governance and implications for quality management: A quick scan in 19 and an in depth study in 7 OECD countries. BMC Health Serv. Res. 2016, 16, 160. [Google Scholar] [CrossRef]
- Mosadeghrad, A. Strategic Collaborative Quality Management and Employee Job Satisfaction. Int. J. Health Policy Manag. 2014, 2, 167–174. [Google Scholar] [CrossRef]
- Hammer, A.; Arah, O.A.; Dersarkissian, M.; Thompson, C.A.; Mannion, R.; Wagner, C.; Ommen, O.; Sunol, R.; Pfaff, H.; DUQuE Project Consortium. The Relationship between Social Capital and Quality Management Systems in European Hospitals: A Quantitative Study. PLoS ONE 2013, 8, e85662. [Google Scholar] [CrossRef] [PubMed]
- Shin, J.; Lee, E. The effect of social capital on job satisfaction and quality of care among hospital nurses in South Korea. J. Nurs. Manag. 2016, 24, 934–942. [Google Scholar] [CrossRef] [PubMed]
- Kelly, L.A.; Lefton, C.; Fischer, S.A. Nurse Leader Burnout, Satisfaction, and Work-Life Balance. J. Nurs. Adm. 2019, 49, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Ulianov, Y.A.; Mingazova, E.N. Professional satisfaction of the medical staff of the scientific and practical dental complex. Probl. Sotsial’noi Gig. Zdravookhranenniiai Istor. Med. 2020, 28, 817–821. [Google Scholar]
- Meng, R.; Li, J.; Zhang, Y.; Yu, Y.; Luo, Y.; Liu, X.; Zhao, Y.; Hao, Y.; Hu, Y.; Yu, C. Evaluation of Patient and Medical Staff Satisfaction regarding Healthcare Services in Wuhan Public Hospitals. Int. J. Environ. Res. Public Health 2018, 15, 769. [Google Scholar] [CrossRef]
- McCay, R.; Lyles, A.A.; Larkey, L. Nurse Leadership Style, Nurse Satisfaction, and Patient Satisfaction: A Systematic Review. J. Nurs. Care Qual. 2018, 33, 361–367. [Google Scholar] [CrossRef]
- Hysong, S.J. Meta-analysis: Audit and feedback features impact effectiveness on care quality. Med. Care 2009, 47, 356–363. [Google Scholar] [CrossRef]
- Hurst, D. Audit and feedback had small but potentially important improvements in professional practice. Evid. Based Dent. 2013, 14, 8–9. [Google Scholar] [CrossRef]
- Hysong, S.J.; Kell, H.J.; Petersen, L.A.; Campbell, B.A.; Trautner, B.W. Theory-based and evidence-based design of audit and feedback programmes: Examples from two clinical intervention studies. BMJ Qual. Saf. 2017, 26, 323–334. [Google Scholar] [CrossRef]
- Brown, B.; Gude, W.T.; Blakeman, T.; van der Veer, S.N.; Ivers, N.; Francis, J.J.; Lorencatto, F.; Presseau, J.; Peek, N.; Daker-White, G. Clinical Performance Feedback Intervention Theory (CP-FIT): A new theory for designing, implementing, and evaluating feedback in health care based on a systematic review and meta-synthesis of qualitative research. Implement. Sci. 2019, 14, 40. [Google Scholar] [CrossRef]
- Vansteenkiste, N.; Rademakers, F.E.; Kips, J.C. Hospital quality management: The perspective of a Belgian academic medical center. World Hosp. Health Serv. Off. J. Int. Hosp. Fed. 2012, 48, 14–16. [Google Scholar]
- Shukla, P.J.; Barreto, S.G.; Nadkarni, M.S. Application of Six Sigma towards improving surgical outcomes. Hepato-Gastroenterol. 2008, 55, 311–314. [Google Scholar]
- Nicolay, C.R.; Purkayastha, S.; Greenhalgh, A.; Benn, J.; Chaturvedi, S.; Phillips, N.; Darzi, A. Systematic review of the application of quality improvement methodologies from the manufacturing industry to surgical healthcare. Br. J. Surg. 2012, 99, 324–335. [Google Scholar] [CrossRef] [PubMed]
- Amaratunga, T.; Dobranowski, J. Systematic Review of the Application of Lean and Six Sigma Quality Improvement Methodologies in Radiology. J. Am. Coll. Radiol. 2016, 13, 1088–1095.e7. [Google Scholar] [CrossRef] [PubMed]
- DelliFraine, J.L.; Langabeer, J.R., 2nd; Nembhard, I.M. Assessing the evidence of Six Sigma and Lean in the health care industry. Qual. Manag. Health Care 2010, 19, 211–225. [Google Scholar] [CrossRef]
- Mason, S.E.; Nicolay, C.R.; Darzi, A. The use of Lean and Six Sigma methodologies in surgery: A systematic review. Surgeon 2015, 13, 91–100. [Google Scholar] [CrossRef]
- County Emergency Clinical Hospital of Targu Mures. Available online: https://www.spitalmures.ro/en/ (accessed on 7 January 2023).
- Moldovan, F.; Bataga, T. Torque Control during Bone Insertion of Cortical Screws. Procedia Manuf. 2020, 46, 484–490. [Google Scholar] [CrossRef]
- Moldovan, L. Sustainability assessment framework for VET organizations. Sustainability 2015, 7, 7156–7174. [Google Scholar] [CrossRef]
- Jarvis, B.A.; Johnson, T.; Butler, P.; O’Shaughnessy, K.; Fullam, F.A.; Tran, L.; Gupta, R. Assessing the impact of electronic health records as an enabler of hospital quality and patient satisfaction. Acad. Med. 2013, 88, 1471–1477. [Google Scholar] [CrossRef]
- Eberlein-Gonska, M.; Petzold, T.; Helaß, G.; Albrecht, D.M.; Schmitt, J. The incidence and determinants of decubitus ulcers in hospital care: An analysis of routine quality management data at a university hospital. Dtsch. Arztebl. Int. 2013, 110, 550–556. [Google Scholar]
- DePaula, D.A.G.; Piatti, N.C.T.P.; Costa, L.M.; Chiavegato, L.D. Satisfaction levels with physical therapy in hospitalized patients. Braz. J. Phys. Thera. 2020, 24, 118–123. [Google Scholar] [CrossRef] [PubMed]






| Social Responsibility Quality Cycle | 1−Organizational Governance | 2−Human Rights | 3−Labor Practices | 4−Environment | 5−Fair Healthcare Practices | 6−Patient Issues | 7−Community Involvement and Development | |
|---|---|---|---|---|---|---|---|---|
| (P) Healthcare services design | PA−Healthcare services accreditation | PA1−Decision structures and processes | PA21−Health care services accessibility PA22−Medical care services for disadvantaged groups | PA3−Promotion of change and professional development | PA4−Plan for environmental impact | PA5−Attitudes of the profession towards accreditation | PA6−Performance information | PA7−Community involvement activities |
| PB−Patient-centered care interventions design | PB1−Quality assurance processes design | PB2−Interventions with positive effects on patient satisfaction | PB3−Quality assurance of patient- centered medical interventions | PB4−Environmental criteria for the selection of materials used in interventions | PB5−Effective interventions implementation | PB6−Patient self-care design and self-management | PB7−Content of the interventions adapted to the community | |
| (I) Healthcare services provision | IA−Health care provision | IA1−Computerized support systems for clinical decisions | IA2−Specific medical approaches | IA31−Continuous healthcare education IA32−Practice guidelines employment and dissemination | IA41−Usability of recycled materials IA42−Recycling of waste | IA5−Promotion of the patient safety culture | IA6−Critical features for improving the surveillance of patients with chronic conditions | IA71−Networking and partnership IA72−Involvement of volunteers and training networks |
| IB−Transfer assurance | IB1−Transfer evaluation mechanisms | IB2−Fair transfer interventions | IB3−Interventions for transfers improvement | IB4−Environmentally friendly transfer interventions | IB5−Features that affect transfer effectiveness | IB6−Interventions to reduce problems in outpatients | IB7−Involvement and participation of professional associations | |
| (E) Healthcare services evaluation | EA−Evaluation and involvement of local opinion leaders | EA1−Existence and recognition of local opinion leaders | EA2−Evaluation of current medical practices | EA3−Professional practices improvement | EA4−Environmental consumption improvement | EA5−Effective work practices | EA6−Patient-specific issues management | EA7−Local opinion leaders involved in the community |
| EB−Satisfaction assessment | EB1−Monitoring mechanisms assignment | EB2−Patient satisfaction degree | EB3−Medical staff satisfaction | Not relevant | Not relevant | EB6−Patient satisfaction degree regarding therapeutic benefits | EB7−Satisfaction regarding partnerships | |
| (R) Continuous improvement | RA-Self assessment | RA1−Self-assessment tools | RA2−Freedom of expression assurance | RA3−Audit and feedback | RA4−Waste generation and energy consumption surveillance tools | RA5−Feedback to medical staff | RA6−Complaints management | RA7−Communitarian initiatives |
| RB−Healthcare services innovation | RB1−Changes to healthcare services | Not relevant | RB3−Medical organization supported by Six sigma and Lean | RB4−Measures applied to the environment | RB5−Safety checklists | RB6−Incident report | RB7−Educational visits | |
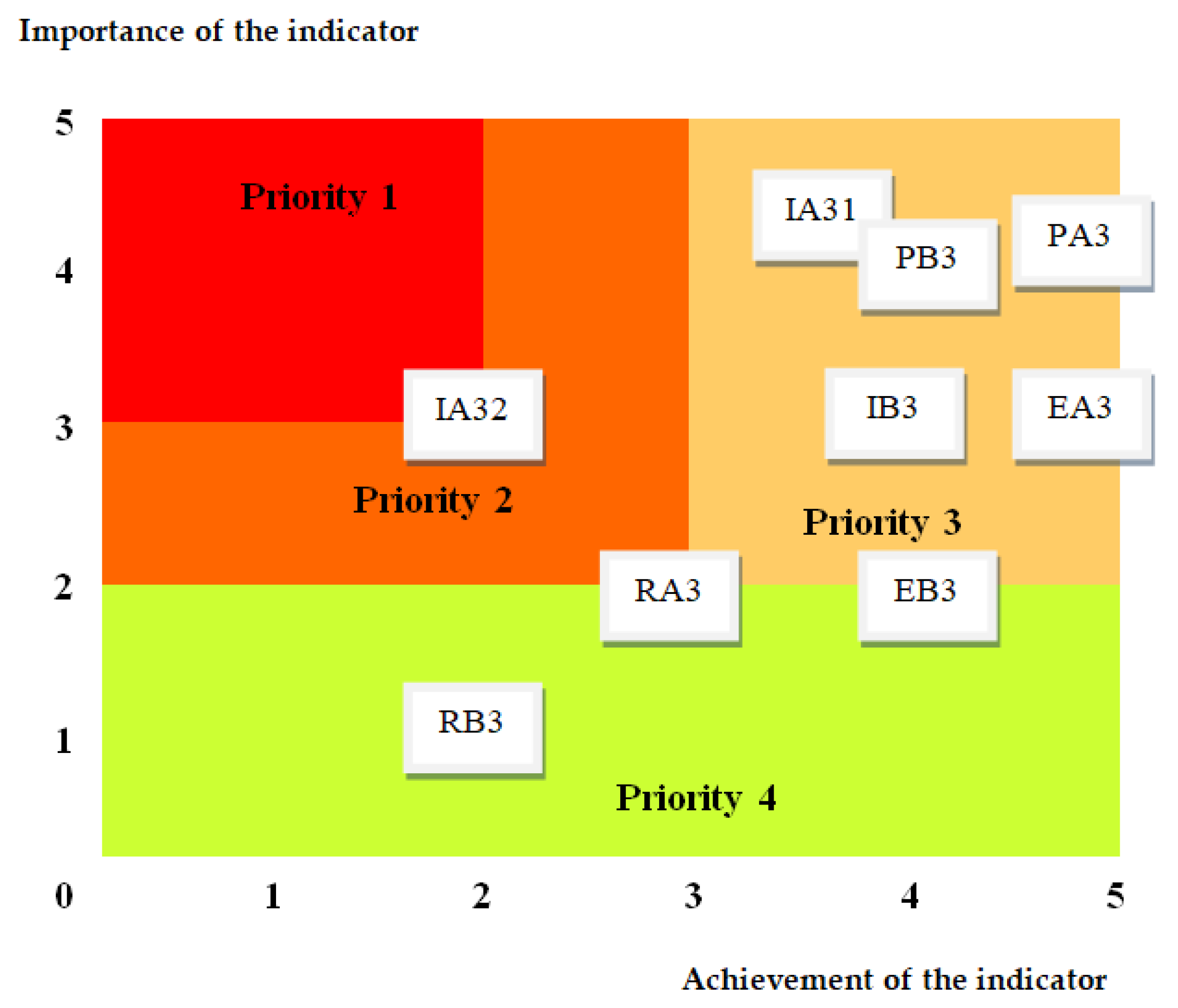
| No. | Indicator identifier | Importance Ii | Achievement Ai | Sustainability Indicator Si = Ii × Ai |
|---|---|---|---|---|
| 1 | PA3—Promotion of change and professional development | 4 | 5 | 20 |
| 2 | PB3—Quality assurance of patient-centered medical interventions | 4 | 4 | 16 |
| 3 | IA31—Continuous healthcare education | 4 | 4 | 16 |
| 4 | IA32—Practice guidelines employment and dissemination | 3 | 2 | 6 |
| 5 | IB3—Interventions for transfer improvement | 3 | 4 | 12 |
| 6 | EA3—Professional practices improvement | 3 | 5 | 15 |
| 7 | EB3—Medical staff satisfaction | 2 | 4 | 8 |
| 8 | RA3—Audit and feedback | 2 | 3 | 6 |
| 9 | RB3—Medical organization supported by Six sima and Lean | 1 | 2 | 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Moldovan, F.; Moldovan, L.; Bataga, T. Assessment of Labor Practices in Healthcare Using an Innovatory Framework for Sustainability. Medicina 2023, 59, 796. https://doi.org/10.3390/medicina59040796
Moldovan F, Moldovan L, Bataga T. Assessment of Labor Practices in Healthcare Using an Innovatory Framework for Sustainability. Medicina. 2023; 59(4):796. https://doi.org/10.3390/medicina59040796
Chicago/Turabian StyleMoldovan, Flaviu, Liviu Moldovan, and Tiberiu Bataga. 2023. "Assessment of Labor Practices in Healthcare Using an Innovatory Framework for Sustainability" Medicina 59, no. 4: 796. https://doi.org/10.3390/medicina59040796