
The Dilemma of Balance between Benefits and Losses for Chondromyxoid Fibroma-like Osteosarcoma in Thoracic Spine with Azygos Tumor Thrombosis: A Case Report
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
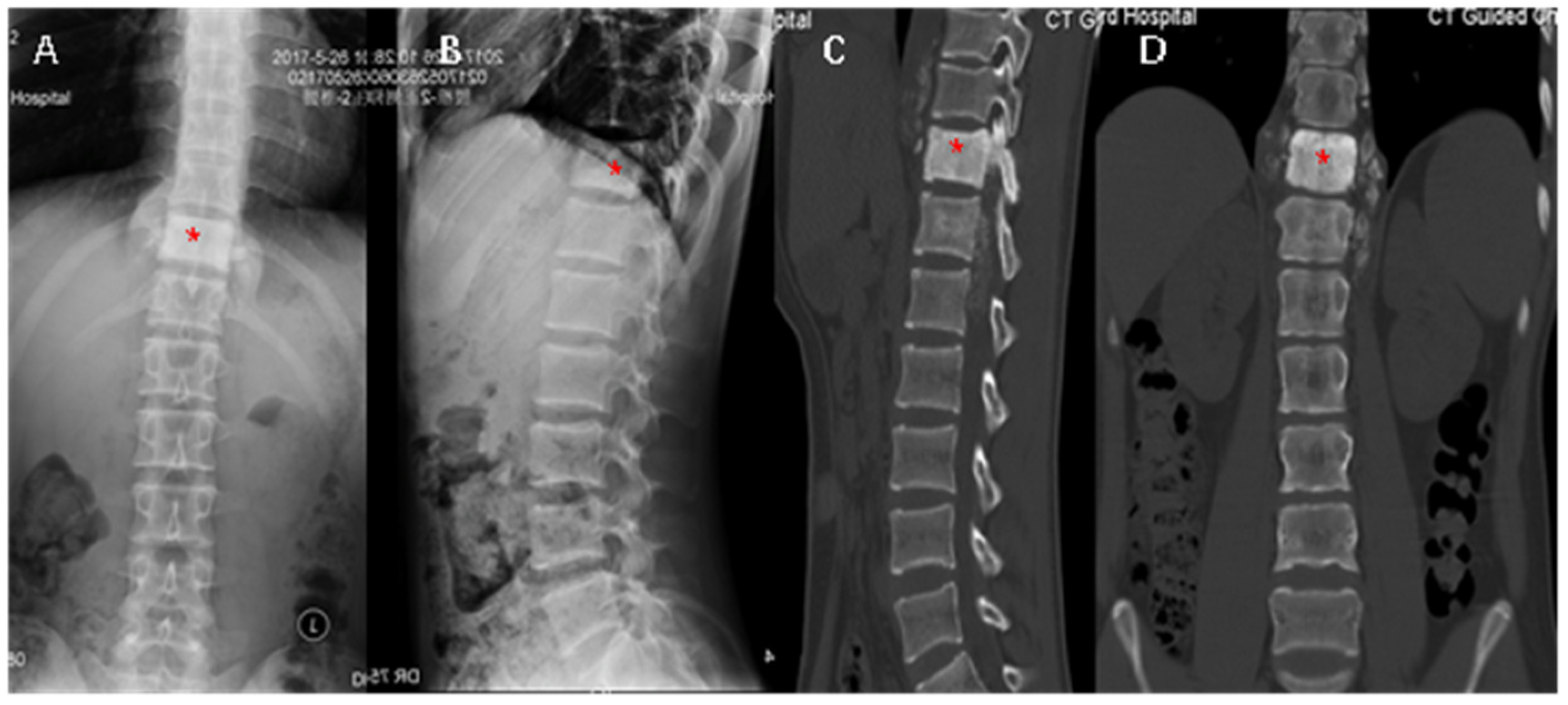
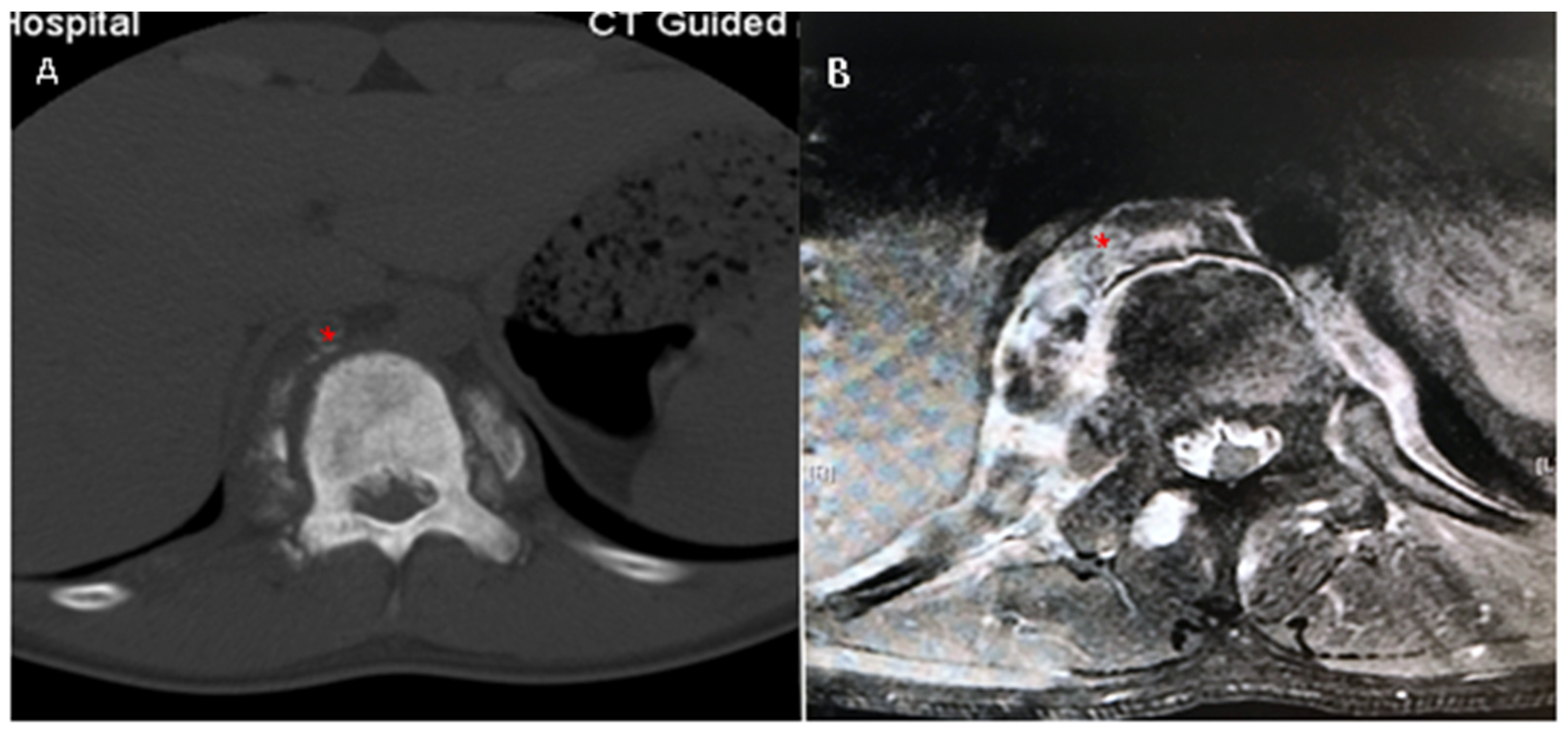
2. Case Report
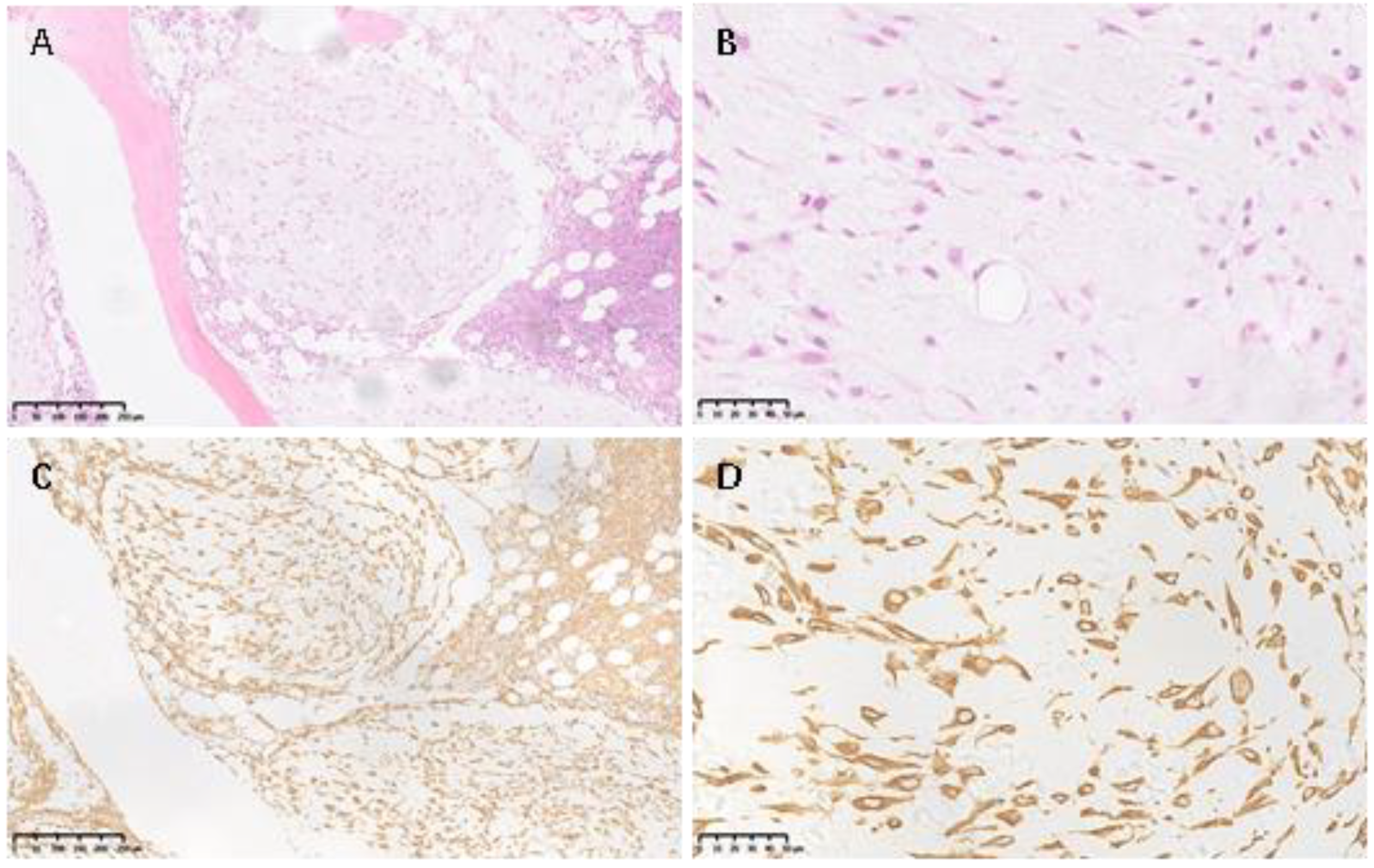
2.1. Pathology Report
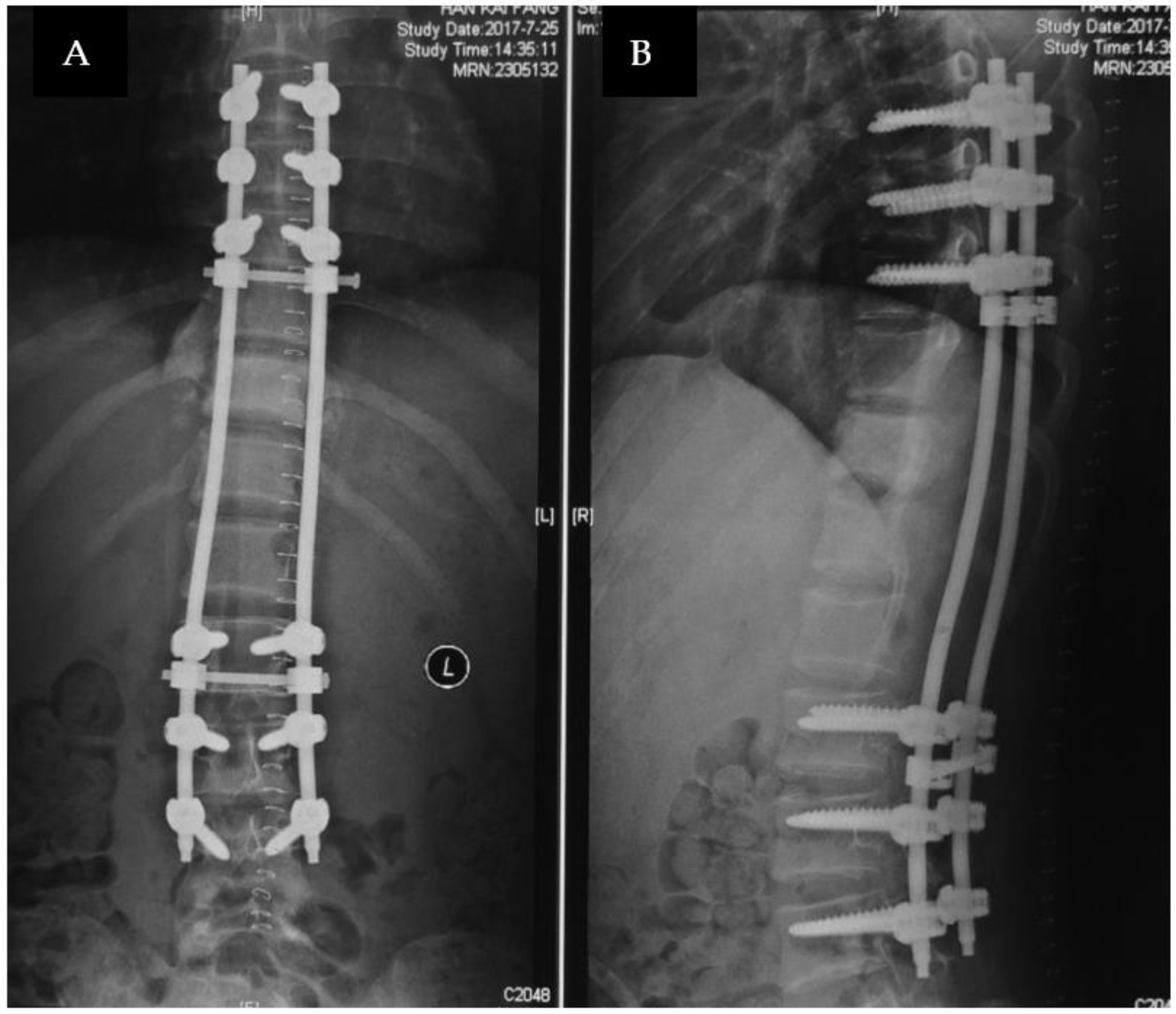
2.2. Treatment
3. Discussion
3.1. CMF-OS, Low-Grade, but Highly Aggressive
3.2. Proactive Treatments Are Suggested for Azygos Vein with Tumor Thrombosis
3.3. The Dilemma of Benefits and Loses
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chow, L.T.C.; Lin, J.; Yip, K.M.H.; Kumta, S.M.; Ahuja, A.T.; King, W.W.K.; Lee, J.C.K. Chondromyxoid fibroma-like osteosarcoma: A distinct variant of low-grade osteosarcoma. Histopathology 1996, 29, 429–436. [Google Scholar] [CrossRef] [PubMed]
- Zhong, J.; Si, L.; Geng, J.; Xing, Y.; Hu, Y.; Jiao, Q.; Zhang, H.; Yao, W. Chondromyxoid fibroma-like osteosarcoma: A case series and literature review. BMC Musculoskelet Disord. 2020, 21, 53–55. [Google Scholar] [CrossRef] [PubMed]
- Lu, Q.; Shi, B.; Hong, J.; Chen, H.; Li, C. Removal of tumor thrombus from the azygos vein in an esophageal squamous cell carcinoma patient. J. Cardiothorac. Surg. 2020, 15, 52–54. [Google Scholar] [CrossRef] [PubMed]
- Roberts, T.T.; Leonard, G.R.; Cepela, D.J. Classifications in Brief: American Spinal Injury Association (ASIA) Impairment Scale. Clin. Orthop. Relat. Res. 2017, 475, 1499–1504. [Google Scholar] [CrossRef] [PubMed]
- Han, X.; Wang, W.; He, J.; Jiang, L.; Li, X. Osteopontin as a biomarker for osteosarcoma therapy and prognosis. Oncol. Lett. 2019, 17, 2592–2598. [Google Scholar] [CrossRef] [PubMed]
- Serra, M.; Morini, M.C.; Scotlandi, K.; Fisher, L.W.; Zini, N.; Colombo, M.P.; Campanacci, M.; Maraldi, N.M.; Olivari, S.; Baldini, N. Evaluation of osteonectin as a diagnostic marker of osteogenic bone tumors. Hum. Pathol. 1992, 23, 1326–1331. [Google Scholar] [CrossRef] [PubMed]
- Casali, P.G.; Bielack, S.; Abecassis, N.; Aro, H.; Bauer, S.; Biagini, R.; Bonvalot, S.; Boukovinas, I.; Bovee, J.V.M.G.; Brennan, B.; et al. Bone sarcomas: ESMO-PaedCan-EURACAN Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 29 (Suppl. 4), iv79–iv95. [Google Scholar] [CrossRef] [PubMed]
- Comandone, A.; Passera, R.; Boglione, A.; Tagini, V.; Ferrari, S.; Cattel, L. High dose methotrexate in adult patients with osteosarcoma: Clinical and pharmacokinetic results. Acta Oncol. 2005, 44, 406–411. [Google Scholar] [CrossRef] [PubMed]
- Gigant, B.; Wang, C.; Ravelli, R.B.; Roussi, F.; Steinmetz, M.O.; Curmi, P.A.; Sobel, A.; Knossow, M. Structural basis for the regulation of tubulin by vinblastine. Nature 2005, 435, 519–522. [Google Scholar] [CrossRef] [PubMed]
- Biermann, J.S.; Chow, W.; Reed, D.; Lucas, D.; Adkins, D.R.; Agulnik, M.; Benjamin, R.S.; Brigman, B.; Budd, G.T.; Curry, W.T.; et al. NCCN Guidelines Insights: Bone Cancer, Version 2.2017. J. Natl. Compr. Cancer Netw. 2017, 15, 155–167. [Google Scholar] [CrossRef] [PubMed]
- Gao, F.; Zhao, X.; Sun, W.; Abhinav, P.; Li, Z. Course of major paravertebral vessels and the positional relationship to the vertebral bodies in healthy Chinese subjects: A CT-based study. Chin. Med. J. 2014, 127, 3887–3893. [Google Scholar] [PubMed]
- Galeano-Valle, F.; Ordieres-Ortega, L.; Demelo-Rodriguez, P. Acute thrombosis of the azygos vein and severe post-thrombotic syndrome of superior vena cava. Med. Clin. Barc. 2019, 152, e61–e62. [Google Scholar] [CrossRef] [PubMed]
- Van Vuuren, T.M.; Doganci, S.; Toonder, I.M.; Graaf, R.; Wittens, C.H. Venous stent patency may be affected by collateral vein lumen size. Phlebology 2019, 34, 32–39. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Du, C.; Liu, X.; Liu, Z.; Wei, F. The Dilemma of Balance between Benefits and Losses for Chondromyxoid Fibroma-like Osteosarcoma in Thoracic Spine with Azygos Tumor Thrombosis: A Case Report. Medicina 2023, 59, 792. https://doi.org/10.3390/medicina59040792
Du C, Liu X, Liu Z, Wei F. The Dilemma of Balance between Benefits and Losses for Chondromyxoid Fibroma-like Osteosarcoma in Thoracic Spine with Azygos Tumor Thrombosis: A Case Report. Medicina. 2023; 59(4):792. https://doi.org/10.3390/medicina59040792
Chicago/Turabian StyleDu, Chuanchao, Xiaoguang Liu, Zhongjun Liu, and Feng Wei. 2023. "The Dilemma of Balance between Benefits and Losses for Chondromyxoid Fibroma-like Osteosarcoma in Thoracic Spine with Azygos Tumor Thrombosis: A Case Report" Medicina 59, no. 4: 792. https://doi.org/10.3390/medicina59040792