
Positron Emission-Computed Tomography, Cryobiopsy versus Bronchoalveolar Lavage and Computed Tomography Findings for Interstitial Lung Disease: A Long-Term Follow-Up

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
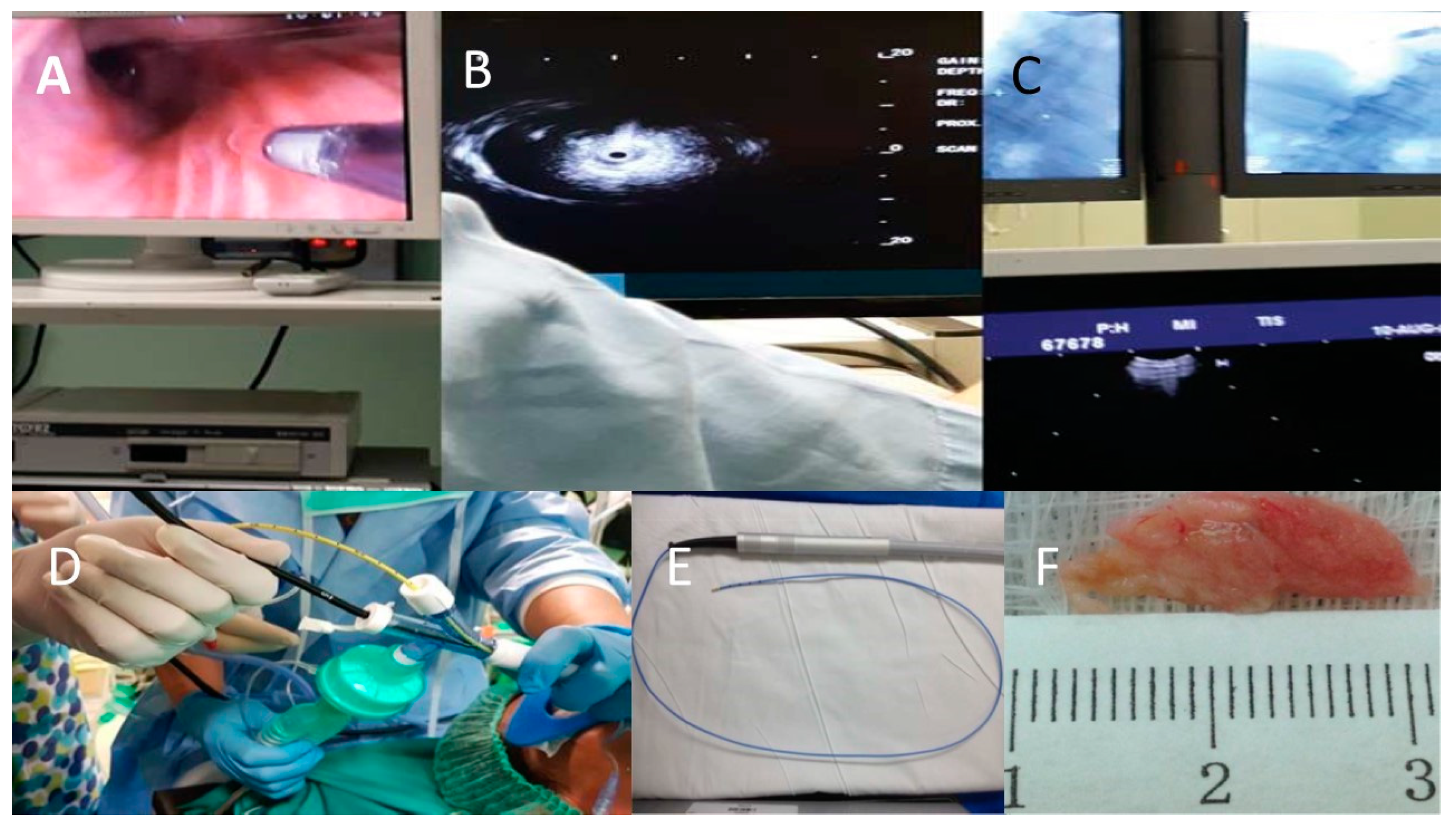
Biopsy Specimens
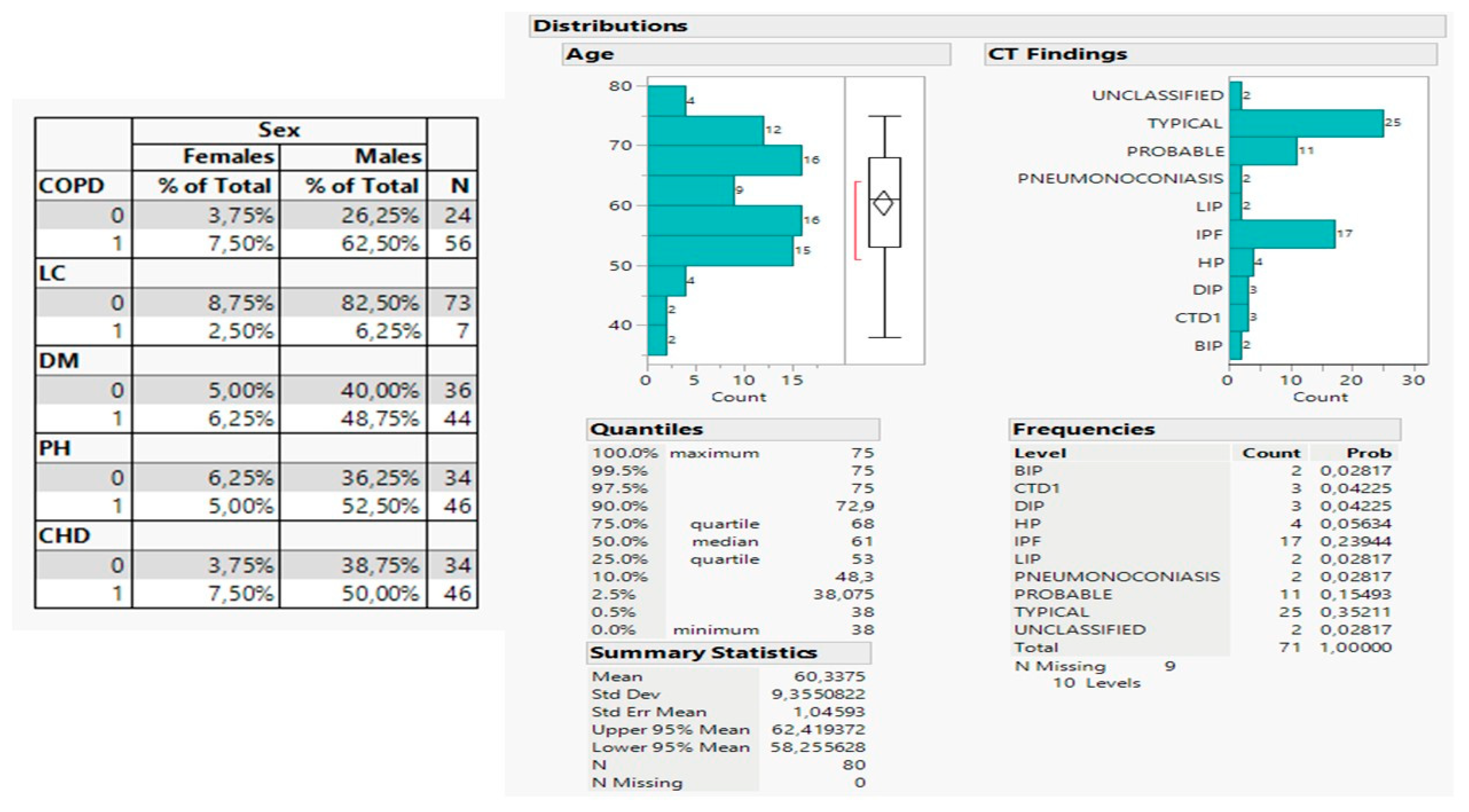
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Raghu, G.; Remy-Jardin, M.; Myers, J.L.; Richeldi, L.; Ryerson, C.J.; Lederer, D.J.; Behr, J.; Cottin, V.; Danoff, S.K.; Morell, F.; et al. Diagnosis of Idiopathic Pulmonary Fibrosis. An Official ATS/ERS/JRS/ALAT Clinical Practice Guideline. Am. J. Respir. Crit. Care Med. 2018, 198, e44–e68. [Google Scholar] [CrossRef]
- Hutchinson, J.P.; Fogarty, A.W.; McKeever, T.M.; Hubbard, R.B. In-Hospital Mortality after Surgical Lung Biopsy for Interstitial Lung Disease in the United States. 2000 to 2011. Am. J. Respir. Crit. Care Med. 2016, 193, 1161–1167. [Google Scholar] [CrossRef] [PubMed]
- Utz, J.P.; Ryu, J.H.; Douglas, W.W.; Hartman, T.E.; Tazelaar, H.D.; Myers, J.L.; Allen, M.S.; Schroeder, D.R. High short-term mortality following lung biopsy for usual interstitial pneumonia. Eur. Respir. J. 2001, 17, 175–179. [Google Scholar] [CrossRef]
- Guler, S.A.; Ellison, K.; Algamdi, M.; Collard, H.R.; Ryerson, C.J. Heterogeneity in Unclassifiable Interstitial Lung Disease. A Systematic Review and Meta-Analysis. Ann. Am. Thorac. Soc. 2018, 15, 854–863. [Google Scholar] [CrossRef] [PubMed]
- King, T.E., Jr.; Bradford, W.Z.; Castro-Bernardini, S.; Fagan, E.A.; Glaspole, I.; Glassberg, M.K.; Gorina, E.; Hopkins, P.M.; Kardatzke, D.; Lancaster, L.; et al. A phase 3 trial of pirfenidone in patients with idiopathic pulmonary fibrosis. N. Engl. J. Med. 2014, 370, 2083–2092. [Google Scholar] [CrossRef] [PubMed]
- Richeldi, L.; du Bois, R.M.; Raghu, G.; Azuma, A.; Brown, K.K.; Costabel, U.; Cottin, V.; Flaherty, K.R.; Hansell, D.M.; Inoue, Y.; et al. Efficacy and safety of nintedanib in idiopathic pulmonary fibrosis. N. Engl. J. Med. 2014, 370, 2071–2082. [Google Scholar] [CrossRef]
- Bradley, B.; Branley, H.M.; Egan, J.J.; Greaves, M.S.; Hansell, D.M.; Harrison, N.K.; Hirani, N.; Hubbard, R.; Lake, F.; Millar, A.B.; et al. Interstitial lung disease guideline: The British Thoracic Society in collaboration with the Thoracic Society of Australia and New Zealand and the Irish Thoracic Society. Thorax 2008, 63, v1–v58. [Google Scholar] [CrossRef]
- MacJannette, R.; Fiddes, J.; Kerr, K.; Dempsey, O. Is bronchoscopic lung biopsy helpful in the management of patients with diffuse lung disease? Eur. Respir. J. 2007, 29, 1064. [Google Scholar] [CrossRef]
- Tomassetti, S.; Cavazza, A.; Colby, T.V.; Ryu, J.H.; Nanni, O.; Scarpi, E.; Tantalocco, P.; Buccioli, M.; Dubini, A.; Piciucchi, S.; et al. Transbronchial biopsy is useful in predicting UIP pattern. Respir. Res. 2012, 13, 96. [Google Scholar] [CrossRef]
- Sheth, J.S.; Belperio, J.A.; Fishbein, M.C.; Kazerooni, E.A.; Lagstein, A.; Murray, S.; Myers, J.L.; Simon, R.H.; Sisson, T.H.; Sundaram, B.; et al. Utility of Transbronchial vs Surgical Lung Biopsy in the Diagnosis of Suspected Fibrotic Interstitial Lung Disease. Chest 2017, 151, 389–399. [Google Scholar] [CrossRef]
- Griff, S.; Schonfeld, N.; Ammenwerth, W.; Blum, T.G.; Grah, C.; Bauer, T.T.; Gruning, W.; Mairinger, T.; Wurps, H. Diagnostic yield of transbronchial cryobiopsy in non-neoplastic lung disease: A retrospective case series. BMC Pulm. Med. 2014, 14, 171. [Google Scholar] [CrossRef] [PubMed]
- Berbescu, E.A.; Katzenstein, A.L.; Snow, J.L.; Zisman, D.A. Transbronchial biopsy in usual interstitial pneumonia. Chest 2006, 129, 1126–1131. [Google Scholar] [CrossRef]
- Leslie, K.O.; Gruden, J.F.; Parish, J.M.; Scholand, M.B. Transbronchial biopsy interpretation in the patient with diffuse parenchymal lung disease. Arch. Pathol. Lab. Med. 2007, 131, 407–423. [Google Scholar] [CrossRef] [PubMed]
- Bianchi, R.; Dubini, A.; Asioli, S.; Ravaglia, C.; Tomassetti, S.; Puglisi, S.; Piciucchi, S.; Gurioli, C.; Gurioli, C.; Fiocca, R.; et al. Transbronchial cryobiopsy: An effective tool in the diagnosis of lymphoproliferative disorders of the lung. ERJ Open Res. 2020, 6, 00260–02019. [Google Scholar] [CrossRef] [PubMed]
- Lentz, R.J.; Argento, A.C.; Colby, T.V.; Rickman, O.B.; Maldonado, F. Transbronchial cryobiopsy for diffuse parenchymal lung disease: A state-of-the-art review of procedural techniques, current evidence, and future challenges. J. Thorac. Dis. 2017, 9, 2186–2203. [Google Scholar] [CrossRef]
- Colella, S.; Haentschel, M.; Shah, P.; Poletti, V.; Hetzel, J. Transbronchial Lung Cryobiopsy in Interstitial Lung Diseases: Best Practice. Respir. Int. Rev. Thorac. Dis. 2018, 95, 383–391. [Google Scholar] [CrossRef]
- Tomassetti, S.; Wells, A.U.; Costabel, U.; Cavazza, A.; Colby, T.V.; Rossi, G.; Sverzellati, N.; Carloni, A.; Carretta, E.; Buccioli, M.; et al. Bronchoscopic Lung Cryobiopsy Increases Diagnostic Confidence in the Multidisciplinary Diagnosis of Idiopathic Pulmonary Fibrosis. Am. J. Respir. Crit. Care Med. 2016, 193, 745–752. [Google Scholar] [CrossRef]
- Ravaglia, C.; Wells, A.U.; Tomassetti, S.; Gurioli, C.; Gurioli, C.; Dubini, A.; Cavazza, A.; Colby, T.V.; Piciucchi, S.; Puglisi, S.; et al. Diagnostic yield and risk/benefit analysis of trans-bronchial lung cryobiopsy in diffuse parenchymal lung diseases: A large cohort of 699 patients. BMC Pulm. Med. 2019, 19, 16. [Google Scholar] [CrossRef]
- Walscher, J.; Gross, B.; Eberhardt, R.; Heussel, C.P.; Eichinger, M.; Warth, A.; Lasitschka, F.; Herth, F.J.F.; Kreuter, M. Transbronchial Cryobiopsies for Diagnosing Interstitial Lung Disease: Real-Life Experience from a Tertiary Referral Center for Interstitial Lung Disease. Respir. Int. Rev. Thorac. Dis. 2019, 97, 348–354. [Google Scholar] [CrossRef]
- Ussavarungsi, K.; Kern, R.M.; Roden, A.C.; Ryu, J.H.; Edell, E.S. Transbronchial Cryobiopsy in Diffuse Parenchymal Lung Disease: Retrospective Analysis of 74 Cases. Chest 2017, 151, 400–408. [Google Scholar] [CrossRef]
- Rodrigues, I.; Estevao Gomes, R.; Coutinho, L.M.; Rego, M.T.; Machado, F.; Morais, A.; Novais Bastos, H. Diagnostic yield and safety of transbronchial lung cryobiopsy and surgical lung biopsy in interstitial lung diseases: A systematic review and meta-analysis. Eur. Respir. Rev. 2022, 31, 210280. [Google Scholar] [CrossRef] [PubMed]
- Kronborg-White, S.; Folkersen, B.; Rasmussen, T.R.; Voldby, N.; Madsen, L.B.; Rasmussen, F.; Poletti, V.; Bendstrup, E. Introduction of cryobiopsies in the diagnostics of interstitial lung diseases–experiences in a referral center. Eur. Clin. Respir. J. 2017, 4, 1274099. [Google Scholar] [CrossRef] [PubMed]
- Meyer, K.C.; Raghu, G.; Baughman, R.P.; Brown, K.K.; Costabel, U.; du Bois, R.M.; Drent, M.; Haslam, P.L.; Kim, D.S.; Nagai, S.; et al. An official American Thoracic Society clinical practice guideline: The clinical utility of bronchoalveolar lavage cellular analysis in interstitial lung disease. Am. J. Respir. Crit. Care Med. 2012, 185, 1004–1014. [Google Scholar] [CrossRef] [PubMed]
- Lederer, C.; Buschulte, K.; Hellmich, B.; Heussel, C.P.; Kriegsmann, M.; Polke, M.; Kreuter, M. Interstitial lung diseases: Classification, differential diagnosis and treatment approaches in a heterogeneous group of chronic lung disorders. Inn. Med. 2023, 64, 247–259. [Google Scholar] [CrossRef]
- Kronborg-White, S.; Sritharan, S.S.; Madsen, L.B.; Folkersen, B.; Voldby, N.; Poletti, V.; Rasmussen, T.R.; Bendstrup, E. Integration of cryobiopsies for interstitial lung disease diagnosis is a valid and safe diagnostic strategy-experiences based on 250 biopsy procedures. J. Thorac. Dis. 2021, 13, 1455–1465. [Google Scholar] [CrossRef] [PubMed]
- Harari, S.; Cereda, F.; Pane, F.; Cavazza, A.; Papanikolaou, N.; Pelosi, G.; Scarioni, M.; Uslenghi, E.; Zompatori, M.; Caminati, A. Lung Cryobiopsy for the Diagnosis of Interstitial Lung Diseases: A Series Contribution to a Debated Procedure. Medicina 2019, 55, 606. [Google Scholar] [CrossRef] [PubMed]
- Berim, I.G.; Saeed, A.I.; Awab, A.; Highley, A.; Colanta, A.; Chaudry, F. Radial Probe Ultrasound-Guided Cryobiopsy. J. Bronchol. Interv. Pulmonol. 2017, 24, 170–173. [Google Scholar] [CrossRef]
- Gnass, M.; Filarecka, A.; Pankowski, J.; Soja, J.; Bugalho, A.; Szlubowski, A. Transbronchial lung cryobiopsy guided by endobronchial ultrasound radial miniprobe in interstitial lung diseases: Preliminary results of a prospective study. Pol. Arch. Intern. Med. 2018, 128, 259–262. [Google Scholar] [CrossRef]
- Bastos, A.L.; Ferreira, G.A.; Mamede, M.; Mancuzo, E.V.; Teixeira, M.M.; Santos, F.; Ferreira, C.S.; Correa, R.A. PET/CT and inflammatory mediators in systemic sclerosis-associated interstitial lung disease. J. Bras. Pneumol. 2022, 48, e20210329. [Google Scholar] [CrossRef]
- Broens, B.; Duitman, J.W.; Zwezerijnen, G.J.C.; Nossent, E.J.; van der Laken, C.J.; Voskuyl, A.E. Novel tracers for molecular imaging of interstitial lung disease: A state of the art review. Autoimmun. Rev. 2022, 21, 103202. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| 1 | Sarcoidosis |
| 2 | Langerhans cell histiocytosis |
| 3 | Vasculitis |
| 4 | Systemic lupus erythematosus |
| 5 | Lymphangitis carcinomatosis |
| 6 | Rheumatoid arthritis |
| 7 | Progressive systemic sclerosis |
| 8 | Anti-Jo-1 antibody positive interstitial lung disease |
| 9 | Anti-SRP autoantibody associated interstitial lung disease |
| 10 | Ankylosing spondylitis |
| 11 | Sjögren syndrome |
| 12 | Mixed connective tissue disease |
| 13 | Psoriasis—pulmonary manifestations of psoriasis |
| 14 | Interstitial pneumonia with autoimmune features |
| 15 | HIV associated interstitial lung diseases |
| 16 | Amyloidosis |
| 17 | Alveolar proteinosis |
| 18 | Idiopathic pulmonary fibrosis |
| 19 | Cryptogenic organizing pneumonia |
| 20 | Respiratory bronchiolitis-interstitial lung disease |
| 21 | Desquamative interstitial pneumonia |
| 22 | Lymphoid interstitial pneumonia |
| 23 | Acute interstitial pneumonitis |
| 24 | Combined pulmonary fibrosis and emphysema |
| 25 | Idiopathic pleuroparenchymal fibroelastosis |
| Disease | Old | Prob | New | Prob |
|---|---|---|---|---|
| 1 | 10 | 0.125 | 5 | 0.0625 |
| 2 | 3 | 0.0375 | 9 | 0.1125 |
| 3 | 5 | 0.0625 | 7 | 0.0875 |
| 4 | 4 | 0.05 | 3 | 0.0375 |
| 5 | 4 | 0.05 | 4 | 0.05 |
| 6 | 3 | 0.0375 | 1 | 0.0125 |
| 7 | 4 | 0.05 | 1 | 0.0125 |
| 8 | 3 | 0.0375 | 2 | 0.025 |
| 9 | 3 | 0.0375 | ||
| 10 | 3 | 0.0375 | 6 | 0.075 |
| 11 | 2 | 0.025 | 2 | 0.025 |
| 12 | 2 | 0.025 | 5 | 0.0625 |
| 13 | 1 | 0.0125 | 4 | 0.05 |
| 14 | 2 | 0.025 | 2 | 0.025 |
| 15 | 1 | 0.0125 | 1 | 0.0125 |
| 16 | 2 | 0.025 | 2 | 0.025 |
| 17 | 2 | 0.025 | 2 | 0.025 |
| 18 | 1 | 0.0125 | 3 | 0.0375 |
| 19 | 3 | 0.0375 | 1 | 0.0125 |
| 20 | 2 | 0.025 | 2 | 0.025 |
| 21 | 3 | 0.0375 | 3 | 0.0375 |
| 22 | 4 | 0.05 | 6 | 0.075 |
| 23 | 5 | 0.0625 | 3 | 0.0375 |
| 24 | 4 | 0.05 | 3 | 0.0375 |
| 25 | 4 | 0.05 | 3 | 0.0375 |
| Total | 80 | 1 | 80 | 1 |
| Change in Diagnosis | Cryobiopsy | % of Total | n |
|---|---|---|---|
| 0 | 0 | 30 | 24 |
| 1 | 15 | 12 | |
| 1 | 0 | 20 | 16 |
| 1 | 35 | 28 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zarogoulidis, P.; Matthaios, D.; Huang, H.; Bai, C.; Hohenforst-Schmidt, W.; Porpodis, K.; Petridis, D.; Pigakis, K.; Kougkas, N.; Oikonomou, P.; et al. Positron Emission-Computed Tomography, Cryobiopsy versus Bronchoalveolar Lavage and Computed Tomography Findings for Interstitial Lung Disease: A Long-Term Follow-Up. Medicina 2023, 59, 787. https://doi.org/10.3390/medicina59040787
Zarogoulidis P, Matthaios D, Huang H, Bai C, Hohenforst-Schmidt W, Porpodis K, Petridis D, Pigakis K, Kougkas N, Oikonomou P, et al. Positron Emission-Computed Tomography, Cryobiopsy versus Bronchoalveolar Lavage and Computed Tomography Findings for Interstitial Lung Disease: A Long-Term Follow-Up. Medicina. 2023; 59(4):787. https://doi.org/10.3390/medicina59040787
Chicago/Turabian StyleZarogoulidis, Paul, Dimitris Matthaios, Haidong Huang, Chong Bai, Wolfgang Hohenforst-Schmidt, Konstantinos Porpodis, Dimitris Petridis, Konstantinos Pigakis, Nikolaos Kougkas, Panagoula Oikonomou, and et al. 2023. "Positron Emission-Computed Tomography, Cryobiopsy versus Bronchoalveolar Lavage and Computed Tomography Findings for Interstitial Lung Disease: A Long-Term Follow-Up" Medicina 59, no. 4: 787. https://doi.org/10.3390/medicina59040787