
Efficacy and Safety of Ethylene-Vinyl Alcohol (EVOH) Copolymer-Based Non-Adhesive Liquid Embolic Agents (NALEAs) in Transcatheter Arterial Embolization (TAE) of Acute Non-Neurovascular Bleeding: A Multicenter Retrospective Cohort Study
 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Treatment
2.3. Outcomes and Definitions
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
References
- Valek, V.; Husty, J. Quality Improvement Guidelines for Transcatheter Embolization for Acute Gastrointestinal Nonvariceal Hemorrhage. Cardiovasc. Interv. Radiol. 2012, 36, 608–612. [Google Scholar] [CrossRef] [Green Version]
- Chakraverty, S.; Flood, K.; Kessel, D.; McPherson, S.; Nicholson, T.; Ray, C.E.; Robertson, I.; Van Delden, O.M. CIRSE Guidelines: Quality Improvement Guidelines for Endovascular Treatment of Traumatic Hemorrhage. Cardiovasc. Interv. Radiol. 2012, 35, 472–482. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Angle, J.F.; Siddiqi, N.H.; Wallace, M.J.; Kundu, S.; Stokes, L.; Wojak, J.C.; Cardella, J.F. Quality Improvement Guidelines for Percutaneous Transcatheter Embolization: Society of Interventional Radiology Standards of Practice Committee. J. Vasc. Interv. Radiol. 2010, 21, 1479–1486. [Google Scholar] [CrossRef] [PubMed]
- Loffroy, R.; Guiu, B. Role of transcatheter arterial embolization for massivebleeding from gastroduodenal ulcers. World J. Gastroenterol. 2009, 15, 5889–5897. [Google Scholar] [CrossRef] [PubMed]
- Loffroy, R.; Guiu, B.; Mezzetta, L.; Minello, A.; Michiels, C.; Jouve, J.-L.; Cheynel, N.; Rat, P.; Cercueil, J.-P.; Krausé, D. Short- and long-term results of transcatheter embolization for massive arterial hemorrhage from gastroduodenal ulcers not controlled by endoscopic hemostasis. Can. J. Gastroenterol. 2009, 23, 115–120. [Google Scholar] [CrossRef]
- Sapoval, M.; Vidal, V.; Déan, C.; Del Giudice, C.; Tradi, F.; Chevallier, O.; Charles-Nelson, A.; Pellerin, O.; Loffroy, R. Safety and Efficacy of Peripheral Embolization with EASYX Liquid Embolic Agent: A Multicenter Prospective Study. J. Vasc. Interv. Radiol. 2021, 32, 1136–1143. [Google Scholar] [CrossRef]
- Augustin, A.M.; Fluck, F.; Bley, T.; Kickuth, R. Endovascular Therapy of Gastrointestinal Bleeding. In RöFo-Fortschritte auf dem Gebiet der Röntgenstrahlen und der Bildgebenden Verfahren; Georg Thieme Verlag KG: Stuttgart, Germany, 2019; Volume 191, pp. 1073–1082. [Google Scholar] [CrossRef] [Green Version]
- Valisena, S.; Abboud, A.-E.; Andereggen, E.; Ansorge, A.; Gamulin, A. Management of high-energy blunt pelvic ring injuries: A retrospective cohort study evaluating an institutional protocol. Injury 2022, 53, 4054–4061. [Google Scholar] [CrossRef]
- Di Pietro, S.; Tiralongo, F.; Desiderio, C.M.; Vacirca, F.; Palmucci, S.; Giurazza, F.; Venturini, M.; Basile, A. Efficacy of Percutaneous Transarterial Embolization in Patients with Spontaneous Abdominal Wall Hematoma and Comparison between Blind and Targeted Embolization Approaches. J. Clin. Med. 2022, 11, 1270. [Google Scholar] [CrossRef]
- Tiralongo, F.; Seminatore, S.; Di Pietro, S.; Distefano, G.; Galioto, F.; Vacirca, F.; Giurazza, F.; Palmucci, S.; Venturini, M.; Scaglione, M.; et al. Spontaneous Retroperitoneal Hematoma Treated with Percutaneous Transarterial Embolization in COVID-19 Era: Diagnostic Findings and Procedural Outcome. Tomography 2022, 8, 1228–1240. [Google Scholar] [CrossRef]
- Lucatelli, P.; Corona, M.; Teodoli, L.; Nardis, P.; Cannavale, A.; Rocco, B.; Trobiani, C.; Cipollari, S.; de Gyurgyokai, S.Z.; Bezzi, M.; et al. Use of Phil Embolic Agent for Bleeding in Non-Neurological Interventions. J. Clin. Med. 2021, 10, 701. [Google Scholar] [CrossRef]
- Ling, G.; Zhou, J.; Ding, X.; Long, Q. Emergency Transcatheter Arterial Embolization for Acute Mediastinal Hemorrhage. Thorac. Cardiovasc. Surg. 2021, 70, 652–657. [Google Scholar] [CrossRef]
- Kettenbach, J.; Ittrich, H.; Gaubert, J.Y.; Gebauer, B.; Vos, J.A. CIRSE Standards of Practice on Bronchial Artery Embolisation. Cardiovasc. Interv. Radiol. 2022, 45, 721–732. [Google Scholar] [CrossRef]
- Pecoraro, F.; Dinoto, E.; Bracale, U.M.; Badalamenti, G.; Farina, A.; Bajardi, G. Symptomatic Deep Femoral Artery Pseudoaneurysm Endovascular Exclusion. Case Report and Literature Review. Ann. Vasc. Surg. 2017, 42, 303.e5–303.e9. [Google Scholar] [CrossRef]
- Kim, J.; Park, S.K.; Chung, J. Role of Transarterial Embolization in the Treatment of Life-Threatening Hemorrhage in Patients With Maxillofacial Injury. Korean J. Neurotrauma 2022, 18, 178. [Google Scholar] [CrossRef]
- Pierot, L.; Wakhloo, A.K. Endovascular Treatment of Intracranial Aneurysms. Stroke 2013, 44, 2046–2054. [Google Scholar] [CrossRef]
- Vanninen, R.L.; Manninen, I. Onyx, a New Liquid Embolic Material for Peripheral Interventions: Preliminary Experience in Aneurysm, Pseudoaneurysm, and Pulmonary Arteriovenous Malformation Embolization. Cardiovasc. Interv. Radiol. 2007, 30, 196–200. [Google Scholar] [CrossRef]
- Piacentino, F.; Fontana, F.; Curti, M.; Macchi, E.; Coppola, A.; Ossola, C.; Giorgianni, A.; Marra, P.; Mosconi, C.; Ierardi, A.M.; et al. Non-Adhesive Liquid Embolic Agents in Extra-Cranial District: State of the Art and Review of the Literature. J. Clin. Med. 2021, 10, 4841. [Google Scholar] [CrossRef]
- Schmitt, N.; Floca, R.O.; Paech, D.; El Shafie, R.A.; Neuberger, U.; Bendszus, M.; Möhlenbruch, M.; Vollherbst, D.F. Imaging Artifacts of Nonadhesive Liquid Embolic Agents in Conventional and Cone-beam CT in a Novel in Vitro AVM Model. Clin. Neuroradiol. 2021, 31, 1141–1148. [Google Scholar] [CrossRef]
- van Rooij, W.J.; Sluzewski, M.; Beute, G.N. Brain AVM embolization with Onyx. AJNR Am. J. Neuroradiol. 2007, 28, 172–177, discussion 178. [Google Scholar]
- Weber, W.; Kis, B.; Siekmann, R.; Kuehne, D. Endovascular Treatment of Intracranial Arteriovenous Malformations with Onyx: Technical Aspects. Am. J. Neuroradiol. 2007, 28, 371–377. [Google Scholar]
- Elsenousi, A.; Aletich, V.A.; Alaraj, A. Neurological outcomes and cure rates of embolization of brain arteriovenous malformations with n-butyl cyanoacrylate or Onyx: A meta-analysis. J. Neurointerv. Surg. 2014, 8, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Ilkay, A.; Ergun, D.; Tunca, K.; Fatih, A.; Mert, S.; Ahmet, P.; Shehram, D.; Dogan, D.; Deniz, B.; Anil, A. Preliminary experience with squid: A new liquid embolizing agent for avm, av fistulas and tumors. Turk. Neurosurg. 2014, 24, 565–570. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alturki, A.Y.; Enriquez-Marulanda, A.; Schmalz, P.; Ogilvy, C.S.; Thomas, A.J. Transarterial Onyx Embolization of Bilateral Transverse–Sigmoid Dural Arteriovenous Malformation with Transvenous Balloon Assist—Initial U.S. Experience with Copernic RC Venous Remodeling Balloon. World Neurosurg. 2018, 109, 398–402. [Google Scholar] [CrossRef] [PubMed]
- Nerva, J.D.; Barber, J.; Levitt, M.R.; Rockhill, J.K.; Hallam, D.K.; Ghodke, B.V.; Sekhar, L.N.; Kim, L.J. Onyx embolization prior to stereotactic radiosurgery for brain arteriovenous malformations: A single-center treatment algorithm. J. Neurointerv. Surg. 2017, 10, 258–267. [Google Scholar] [CrossRef]
- Singfer, U.; Hemelsoet, D.; Vanlangenhove, P.; Martens, F.; Verbeke, L.; Van Roost, D.; Defreyne, L. Unruptured Brain Arteriovenous Malformations: Primary ONYX Embolization in ARUBA (A Randomized Trial of Unruptured Brain Arteriovenous Malformations)-Eligible Patients. Stroke 2017, 48, 3393–3396. [Google Scholar] [CrossRef]
- Cobb, R.J.; Patterson, B.; Karthikesalingam, A.; Morgan, R.; Thompson, M.; Loftus, I. Onyx: A Novel Solution for a Mycotic Aneurysm. Cardiovasc. Interv. Radiol. 2013, 37, 541–543. [Google Scholar] [CrossRef]
- Né, R.; Chevallier, O.; Falvo, N.; Facy, O.; Berthod, P.-E.; Galland, C.; Gehin, S.; Midulla, M.; Loffroy, R. Embolization with ethylene vinyl alcohol copolymer (Onyx®) for peripheral hemostatic and non-hemostatic applications: A feasibility and safety study. Quant. Imaging Med. Surg. 2018, 8, 280–290. [Google Scholar] [CrossRef] [Green Version]
- Izaaryene, J.; Vidal, V.; Bartoli, J.-M.; Gaubert, J.-Y. Multiple bronchial artery aneurysms: Successful treatment with ethylene-vinyl alcohol copolymer (Onyx®). Diagn. Interv. Imaging 2016, 97, 125–127. [Google Scholar] [CrossRef] [Green Version]
- Regine, R.; Palmieri, F.; Siero, M.; Rescigno, A.; Sica, V.; Cantarela, R.; Villari, V. Embolization of traumatic and non-traumatic peripheral vascular lesions with Onyx. Interv. Med. Appl. Sci. 2015, 7, 22–29. [Google Scholar] [CrossRef]
- Chevallier, O.; Gehin, S.; Foahom-Kamwa, A.; Pottecher, P.; Favelier, S.; Loffroy, R. Ethylene-vinyl alcohol copolymer (Onyx®) transarterial embolization for post-traumatic high-flow priapism. Quant. Imaging Med. Surg. 2016, 6, 323–327. [Google Scholar] [CrossRef] [Green Version]
- Ierardi, A.M.; Franchin, M.; Fontana, F.; Piffaretti, G.; Crippa, M.; Angileri, S.A.; Biasina, A.M.; Piacentino, F.; Tozzi, M.; Pinto, A.; et al. The role of ethylene–vinyl alcohol copolymer in association with other embolic agents for the percutaneous and endovascular treatment of type Ia endoleak. La Radiol. Med. 2018, 123, 638–642. [Google Scholar] [CrossRef]
- Cheung, E.Y.H.; Ng, R.Y.T.; Yu, S.C.H.; Zhuang, J.T.F.; Wong, G.K.C. PHIL and Squid Embolization of Cerebral Arteriovenous Malformation: A Retrospective Case Series of 23 Patients. Neurointervention 2022, 17, 174–182. [Google Scholar] [CrossRef]
- Piacentino, F.; Fontana, F.; Curti, M.; Imperatori, A.; Venturini, M. Trancatheter embolization of pulmonary artery pseudoaneurysm with detachable coils in association with non-adhesive liquid embolizing agent (Squid). Acta Bio-Med. Atenei Parm. 2021, 92, e2021274. [Google Scholar] [CrossRef]
- Piacentino, F.; Fontana, F.; Curti, M.; Coppola, A.; Venturini, M. Bronchial artery embolization with an ethylene vinyl alcohol copolymer agent (Squid) and polyvinyl alcohol particles for treatment of hemoptysis. Diagn. Interv. Radiol. 2021, 27, 786–788. [Google Scholar] [CrossRef]
- Venturini, M.; Lanza, C.; Marra, P.; Colarieti, A.; Panzeri, M.; Augello, L.; Gusmini, S.; Salvioni, M.; De Cobelli, F.; Del Maschio, A. Transcatheter embolization with Squid, combined with other embolic agents or alone, in different abdominal diseases: A single-center experience in 30 patients. CVIR Endovasc. 2019, 2, 1–13. [Google Scholar] [CrossRef] [Green Version]
- Akbayir, O.; Gedikbaşı, A.; Akyol, A.; Ucar, A.; Saygi-Ozyurt, S.; Gulkilik, A. Cesarean scar pregnancy: A rare cause of uterine arteriovenous malformation. J. Clin. Ultrasound 2011, 39, 534–538. [Google Scholar] [CrossRef]
- Ao, M.; Guo, S.-L.; Zhang, X.-D.; Li, Y.-L.; Li, Y.; Li, Q. First case in China: Onyx for bronchial artery embolization in treatment of refractory massive hemoptysis in one case. J. Thorac. Dis. 2013, 5, E98–E102. [Google Scholar] [CrossRef]
- Bharadwaz, A.; Madhab, G. Liquid Embolization with Onyx in a Technically Challenging Case of Acute Upper GI Bleeding. Indian J. Surg. 2013, 75, 495–496. [Google Scholar] [CrossRef] [Green Version]
- Bommart, S.; Bourdin, A.; Giroux, M.F.; Klein, F.; Micheau, A.; Bares, V.M.; Kovacsik, H. Transarterial Ethylene Vinyl Alcohol Copolymer Visualization and Penetration After Embolization of Life-Threatening Hemoptysis: Technical and Clinical Outcomes. Cardiovasc. Interv. Radiol. 2011, 35, 668–675. [Google Scholar] [CrossRef]
- Jiménez, A.B.; Herráez, J.G.; Membrives, P.P.; Girelli, J.H.; Gómez, D.D.; Berta, J.E. Transcatheter Embolization of a Pancreatic Pseudoaneurysm Using a New Liquid Embolic Agent, Ethylene Vinyl Alcohol Copolymer (Onyx). Pancreas 2009, 38, 110–112. [Google Scholar] [CrossRef]
- Cantasdemir, M.; Kantarci, F.; Mihmanli, I.; Numan, F. Embolization of Profunda Femoris Artery Branch Pseudoaneurysms with Ethylene Vinyl Alcohol Copolymer (Onyx). J. Vasc. Interv. Radiol. 2002, 13, 725–728. [Google Scholar] [CrossRef] [PubMed]
- Carberry, G.; Dalvie, P.; Ozkan, O. 4:18 PM Abstract No. 222—Onyx as a second-line embolic agent in peripheral applications. J. Vasc. Interv. Radiol. 2013, 24, S103. [Google Scholar] [CrossRef]
- Hörer, T.; Toivola, A.; Larzon, T. Embolization with Onyx in Iatrogenic Bleeding of the Gluteal Region. Innov. Technol. Tech. Cardiothorac. Vasc. Surg. 2011, 6, 267–270. [Google Scholar] [CrossRef] [PubMed]
- Khalil, A.; Fartoukh, M.; Bazot, M.; Parrot, A.; Marsault, C.; Carette, M.-F. Systemic Arterial Embolization in Patients With Hemoptysis: Initial Experience With Ethylene Vinyl Alcohol Copolymer in 15 Cases. Am. J. Roentgenol. 2010, 194, W104–W110. [Google Scholar] [CrossRef]
- Khalil, A.; Parrot, A.; Fartoukh, M.; Djibre, M.; Tassart, M.; Carette, M.-F. Pulmonary Artery Occlusion With Ethylene Vinyl Alcohol Copolymer in Patients With Hemoptysis: Initial Experience in 12 Cases. Am. J. Roentgenol. 2012, 198, 207–212. [Google Scholar] [CrossRef]
- Larzon, T.; Mathisen, S.R. Internal Sealing of Acute Aortic Bleeding with a Catheter-Delivered Liquid to Solid Embolic Agent (Onyx). Vascular 2010, 18, 106–110. [Google Scholar] [CrossRef]
- Lenhart, M.; Paetzel, C.; Sackmann, M.; Schneider, H.; Jung, E.M.; Schreyer, A.G.; Feuerbach, S.; Zorger, N. Superselective arterial embolisation with a liquid polyvinyl alcohol copolymer in patients with acute gastrointestinal haemorrhage. Eur. Radiol. 2010, 20, 1994–1999. [Google Scholar] [CrossRef]
- Müller-Wille, R.; Heiss, P.; Herold, T.; Jung, E.M.; Schreyer, A.G.; Hamer, O.W.; Rennert, J.; Hoffstetter, P.; Stroszczynski, C.; Zorger, N. Endovascular Treatment of Acute Arterial Hemorrhage in Trauma Patients Using Ethylene Vinyl Alcohol Copolymer (Onyx). Cardiovasc. Interv. Radiol. 2011, 35, 65–75. [Google Scholar] [CrossRef]
- Ahuja, C.; Chadha, M.; Pierce, G. Case report: Complex internal mammary to pulmonary artery fistula as a cause of hemoptysis in tuberculosis: Diagnosis and endovascular management using ethylene vinyl alcohol copolymer (Onyx). Indian J. Radiol. Imaging 2011, 21, 10–12. [Google Scholar] [CrossRef]
- Rennert, J.; Herold, T.; Schreyer, A.G.; Banas, B.; Jung, E.M.; Feuerbach, S.; Lenhart, M.; Mueller-Wille, R.; Zorger, N. Evaluation of a Liquid Embolization Agent (Onyx) for Transcatheter Embolization for Renal Vascular Lesions. In RöFo-Fortschritte auf dem Gebiet der Röntgenstrahlen und der Bildgebenden Verfahren; Georg Thieme Verlag KG Stuttgart: New York, NY, USA, 2009; Volume 181, pp. 996–1001. [Google Scholar] [CrossRef]
- Urbano, J.; Cabrera, J.M.; Franco, A.; Alonso-Burgos, A. Selective Arterial Embolization with Ethylene–Vinyl Alcohol Copolymer for Control of Massive Lower Gastrointestinal Bleeding: Feasibility and Initial Experience. J. Vasc. Interv. Radiol. 2014, 25, 839–846. [Google Scholar] [CrossRef]
- Zeleňák, K.; Sopilko, I.; Svihra, J.; Kliment, J. Successful Embolization of a Renal Artery Pseudoaneurysm with Arteriovenous Fistula and Extravasations Using Onyx After Partial Nephrectomy for Renal Cell Carcinoma. Cardiovasc. Interv. Radiol. 2008, 32, 163–165. [Google Scholar] [CrossRef]
- Zelenák, S.; Janík, L.; Talapková, L. Bleeding in acute pancreatitis treated by transcatheter arterial embolization with ethylene-vinyl alcohol copolymer (Onyx). Vasa 2012, 41, 380–382. [Google Scholar] [CrossRef]
- López-Martínez, L.; Molina-Nuevo, J.D.; Pedrosa-Jiménez, M.J.; Juliá-Mollá, E. Spontaneous Haematomas in Anticoagulated COVID-19 Patients: Diagnosis and Treatment by Embolization. Cardiovasc. Interv. Radiol. 2022, 45, 1001–1006. [Google Scholar] [CrossRef]
- Fontana, F.; Piacentino, F.; Ossola, C.; Coppola, A.; Curti, M.; Macchi, E.; De Marchi, G.; Floridi, C.; Ierardi, A.M.; Carrafiello, G.; et al. Transcatheter Arterial Embolization in Acute Non-Variceal Gastrointestinal Bleedings: A Ten-Year Single-Center Experience in 91 Patients and Review of the Literature. J. Clin. Med. 2021, 10, 4979. [Google Scholar] [CrossRef]
- Loffroy, R.; Desmyttere, A.-S.; Mouillot, T.; Pellegrinelli, J.; Facy, O.; Drouilllard, A.; Falvo, N.; Charles, P.-E.; Bardou, M.; Midulla, M.; et al. Ten-year experience with arterial embolization for peptic ulcer bleeding: N-butyl cyanoacrylate glue versus other embolic agents. Eur. Radiol. 2020, 31, 3015–3026. [Google Scholar] [CrossRef]
- Mattay, R.R.; Shlansky-Goldberg, R.; Pukenas, B.A. Recurrent massive hemoptysis in a patient with cystic fibrosis: Balloon assisted Onyx embolization after bronchial artery coil recanalization. CVIR Endovasc. 2021, 4, 1–6. [Google Scholar] [CrossRef]
- Venturini, M.; Augello, L.; Lanza, C.; Curti, M.; Coppola, A.; Piacentino, F.; De Cobelli, F. Emergency tips recanalisation and gastroesophageal varices embolisation with an ethylene vinyl alcohol copolymer agent (Squid) and detachable coils. Eur. Radiol. Exp. 2020, 4, 1–5. [Google Scholar] [CrossRef]
- Mahdjoub, E.; Serhal, A.; Males, L.; Tligui, M.; Hermieu, J.-F.; Khalil, A. Ethylene Vinyl Alcohol Copolymer Embolization for Acute Renal Hemorrhage: Initial Experience in 24 Cases. Am. J. Roentgenol. 2020, 214, 465–471. [Google Scholar] [CrossRef]
- Urbano, J.; Paul, L.; Cabrera, M.; Alonso-Burgos, A.; Gómez, D. Elective and Emergency Renal Angiomyolipoma Embolization with Ethylene Vinyl Alcohol Copolymer: Feasibility and Initial Experience. J. Vasc. Interv. Radiol. 2017, 28, 832–839. [Google Scholar] [CrossRef]
- Ierardi, A.M.; Xhepa, G.; Duka, E.; Laganà, D.; Ianniello, A.; Floridi, C.; Bacuzzi, A.; Reginelli, A.; Squillaci, E.; Brunese, L.; et al. Ethylene-vinyl alcohol polymer trans-arterial embolization in emergency peripheral active bleeding: Initial experience. Int. Angiol. 2015, 34, 28–35. [Google Scholar]
- Sun, C.; Wang, C.; Wang, Y.; Xie, L.; Liu, T.; Ren, W. Transcatheter arterial embolization of acute gastrointestinal tumor hemorrhage with Onyx. Indian J. Cancer 2014, 51, 56–59. [Google Scholar] [CrossRef] [PubMed]
- Tipaldi, M.A.; Orgera, G.; Krokidis, M.; Rebonato, A.; Maiettini, D.; Vagnarelli, S.; Ambrogi, C.; Rossi, M. Trans Arterial Embolization of Non-variceal Upper Gastrointestinal Bleeding: Is the Use of Ethylene–Vinyl Alcohol Copolymer as Safe as Coils? Cardiovasc. Interv. Radiol. 2018, 41, 1340–1345. [Google Scholar] [CrossRef] [PubMed]
- Patel, I.J.; Rahim, S.; Davidson, J.C.; Hanks, S.E.; Tam, A.L.; Walker, T.G.; Wilkins, L.R.; Sarode, R.; Weinberg, I. Society of Interventional Radiology Consensus Guidelines for the Periprocedural Management of Thrombotic and Bleeding Risk in Patients Undergoing Percutaneous Image-Guided Interventions—Part II: Recommendations: Endorsed by the Canadian Association for Interventional Radiology and the Cardiovascular and Interventional Radiological Society of Europe. J. Vasc. Interv. Radiol. 2019, 30, 1168–1184.e1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coccolini, F.; Stahel, P.F.; Montori, G.; Biffl, W.; Horer, T.M.; Catena, F.; Kluger, Y.; Moore, E.E.; Peitzman, A.B.; Ivatury, R.; et al. Pelvic trauma: WSES classification and guidelines. World J. Emerg. Surg. 2017, 12, 1–18. [Google Scholar] [CrossRef] [Green Version]
- Sacks, D.; McClenny, T.E.; Cardella, J.F.; Lewis, C.A. Society of Interventional Radiology Clinical Practice Guidelines. J. Vasc. Interv. Radiol. 2003, 14, S199–S202. [Google Scholar] [CrossRef] [Green Version]
- Dariushnia, S.R.; Redstone, E.A.; Heran, M.K.; Cramer, H.R.; Ganguli, S.; Gomes, A.S.; Hogan, M.J.; Himes, E.A.; Patel, S.; Schiro, B.J.; et al. Society of Interventional Radiology Quality Improvement Standards for Percutaneous Transcatheter Embolization. J. Vasc. Interv. Radiol. 2021, 32, 476.e1–476.e33. [Google Scholar] [CrossRef]
- Loffroy, R.; Guiu, B.; D’Athis, P.; Mezzetta, L.; Gagnaire, A.; Jouve, J.; Ortega-Deballon, P.; Cheynel, N.; Cercueil, J.P.; Krausé, D. Arterial Embolotherapy for Endoscopically Unmanageable Acute Gastroduodenal Hemorrhage: Predictors of Early Rebleeding. Clin. Gastroenterol. Hepatol. 2009, 7, 515–523. [Google Scholar] [CrossRef]
- Khalilzadeh, O.; Baerlocher, M.O.; Shyn, P.B.; Connolly, B.L.; Devane, A.M.; Morris, C.S.; Cohen, A.M.; Midia, M.; Thornton, R.H.; Gross, K.; et al. Proposal of a New Adverse Event Classification by the Society of Interventional Radiology Standards of Practice Committee. J. Vasc. Interv. Radiol. 2017, 28, 1432–1437.e3. [Google Scholar] [CrossRef] [Green Version]
- Filippiadis, D.K.; Binkert, C.; Pellerin, O.; Hoffmann, R.T.; Krajina, A.; Pereira, P.L. Cirse Quality Assurance Document and Standards for Classification of Complications: The Cirse Classification System. Cardiovasc. Interv. Radiol. 2017, 40, 1141–1146. [Google Scholar] [CrossRef]
- Minici, R.; Ammendola, M.; Manti, F.; Siciliano, M.A.; Giglio, E.; Minici, M.; Melina, M.; Currò, G.; Laganà, D. Safety and Efficacy of Degradable Starch Microspheres Transcatheter Arterial Chemoembolization as a Bridging Therapy in Patients with Early Stage Hepatocellular Carcinoma and Child-Pugh Stage B Eligible for Liver Transplant. Front. Pharmacol. 2021, 12, 634084. [Google Scholar] [CrossRef]
- Minici, R.; Ammendola, M.; Manti, F.; Siciliano, M.A.; Minici, M.; Komaei, I.; Currò, G.; Laganà, D. Safety and Efficacy of Degradable Starch Microspheres Transcatheter Arterial Chemoembolization (DSM-TACE) in the Downstaging of Intermediate-Stage Hepatocellular Carcinoma (HCC) in Patients With a Child-Pugh Score of 8-9. Front. Pharmacol. 2021, 12, 634087. [Google Scholar] [CrossRef]
- Kolber, M.K.; Shukla, P.A.; Kumar, A.; Silberzweig, J.E. Ethylene Vinyl Alcohol Copolymer (Onyx) Embolization for Acute Hemorrhage: A Systematic Review of Peripheral Applications. J. Vasc. Interv. Radiol. 2015, 26, 809–815. [Google Scholar] [CrossRef]
- Van Vugt, R.; Van Munster, I.P.; De Jager, C.P.; Rutten, M.J.; Bosscha, K. Embolization as Treatment of Choice for Bleeding Peptic Ulcers in High-Risk Patients. Dig. Surg. 2009, 26, 37–42. [Google Scholar] [CrossRef]
- Aina, R.; Oliva, V.L.; Therasse, E.; Perreault, P.; Bui, B.T.; Dufresne, M.-P.; Soulez, G. Arterial Embolotherapy for Upper Gastrointestinal Hemorrhage: Outcome Assessment. J. Vasc. Interv. Radiol. 2001, 12, 195–200. [Google Scholar] [CrossRef]
- Huang, Y.-S.; Chang, C.-C.; Liou, J.-M.; Jaw, F.-S.; Liu, K.-L. Transcatheter Arterial Embolization with N-Butyl Cyanoacrylate for Nonvariceal Upper Gastrointestinal Bleeding in Hemodynamically Unstable Patients: Results and Predictors of Clinical Outcomes. J. Vasc. Interv. Radiol. 2014, 25, 1850–1857. [Google Scholar] [CrossRef]
- Yonemitsu, T.; Kawai, N.; Sato, M.; Sonomura, T.; Takasaka, I.; Nakai, M.; Minamiguchi, H.; Sahara, S.; Iwasaki, Y.; Naka, T.; et al. Comparison of Hemostatic Durability between N-Butyl Cyanoacrylate and Gelatin Sponge Particles in Transcatheter Arterial Embolization for Acute Arterial Hemorrhage in a Coagulopathic Condition in a Swine Model. Cardiovasc. Interv. Radiol. 2010, 33, 1192–1197. [Google Scholar] [CrossRef]
- Yonemitsu, T.; Kawai, N.; Sato, M.; Tanihata, H.; Takasaka, I.; Nakai, M.; Minamiguchi, H.; Sahara, S.; Iwasaki, Y.; Shima, Y.; et al. Evaluation of Transcatheter Arterial Embolization with Gelatin Sponge Particles, Microcoils, and N-butyl Cyanoacrylate for Acute Arterial Bleeding in a Coagulopathic Condition. J. Vasc. Interv. Radiol. 2009, 20, 1176–1187. [Google Scholar] [CrossRef]
- Abdulmalak, G.; Chevallier, O.; Falvo, N.; Di Marco, L.; Bertaut, A.; Moulin, B.; Abi-Khalil, C.; Gehin, S.; Charles, P.-E.; Latournerie, M.; et al. Safety and efficacy of transcatheter embolization with Glubran®2 cyanoacrylate glue for acute arterial bleeding: A single-center experience with 104 patients. Abdom. Imaging 2017, 43, 723–733. [Google Scholar] [CrossRef]
- Hayakawa, M. Pathophysiology of trauma-induced coagulopathy: Disseminated intravascular coagulation with the fibrinolytic phenotype. J. Intensiv. Care 2017, 5, 14. [Google Scholar] [CrossRef] [Green Version]
- Kim, P.H.; Tsauo, J.; Shin, J.H.; Yun, S.-C. Transcatheter Arterial Embolization of Gastrointestinal Bleeding with N-Butyl Cyanoacrylate: A Systematic Review and Meta-Analysis of Safety and Efficacy. J. Vasc. Interv. Radiol. 2017, 28, 522–531.e5. [Google Scholar] [CrossRef]
- Minici, R.; Paone, S.; Talarico, M.; Zappia, L.; Abdalla, K.; Petullà, M.; Laganà, D. Percutaneous treatment of vascular access-site complications: A ten years’ experience in two centres. CVIR Endovasc. 2020, 3, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Minici, R.; Ammendola, M.; Talarico, M.; Luposella, M.; Minici, M.; Ciranni, S.; Guzzardi, G.; Laganà, D. Endovascular recanalization of chronic total occlusions of the native superficial femoral artery after failed femoropopliteal bypass in patients with critical limb ischemia. CVIR Endovasc. 2021, 4, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Minici, R.; Serra, R.; Ierardi, A.M.; Petullà, M.; Bracale, U.M.; Carrafiello, G.; Laganà, D. Thoracic endovascular repair for blunt traumatic thoracic aortic injury: Long-term results. Vascular 2022. [Google Scholar] [CrossRef] [PubMed]
- Bracale, U.M.; Peluso, A.; Panagrosso, M.; Cecere, F.; DEL Guercio, L.; Minici, R.; Giannotta, N.; Ielapi, N.; Licastro, N.; Serraino, G.F.; et al. Ankle-Brachial Index evaluation in totally percutaneous approach vs. femoral artery cutdown for endovascular aortic repair of abdominal aortic aneurysms. Chirurgia 2022, 35, 349–354. [Google Scholar] [CrossRef]
- Minici, R.; Serra, R.; De Rosi, N.; Ciranni, S.; Talarico, M.; Petullà, M.; Guzzardi, G.; Fontana, F.; Laganà, D. Endovascular treatment of femoro-popliteal occlusions with retrograde tibial access after failure of the antegrade approach. Catheter. Cardiovasc. Interv. 2023, in press. [Google Scholar] [CrossRef]
- Minici, R.; Serra, R.; Giurdanella, M.; Talarico, M.; Siciliano, M.A.; Carrafiello, G.; Laganà, D. Efficacy and Safety of Distal Radial Access for Transcatheter Arterial Chemoembolization (TACE) of the Liver. J. Pers. Med. 2023, in press. [Google Scholar]
- Guimaraes, M.; Wooster, M. Onyx (Ethylene-vinyl Alcohol Copolymer) in Peripheral Applications. Semin. Interv. Radiol. 2011, 28, 350–356. [Google Scholar] [CrossRef] [Green Version]
- Capriotti, K.; Capriotti, J.A. Dimethyl sulfoxide: History, chemistry, and clinical utility in dermatology. J. Clin. Aesthetic. Dermatol. 2012, 5, 24–26. [Google Scholar]
- Vaidya, S.; Tozer, K.R.; Chen, J. An Overview of Embolic Agents. Semin. Interv. Radiol. 2008, 25, 204–215. [Google Scholar] [CrossRef] [Green Version]
- Loffroy, R.; Favelier, S.; Genson, P.-Y.; Guiu, B. Onyx for Embolization of Life-Threatening Hemoptysis: A Promising but Luxury Embolic Agent! Cardiovasc. Interv. Radiol. 2011, 35, 221. [Google Scholar] [CrossRef] [Green Version]
- Lv, X.; Li, Y.; Jiang, C.; Wu, Z. The Incidence of Trigeminocardiac Reflex in Endovascular Treatment of Dural Arteriovenous Fistula with Onyx. Interv. Neuroradiol. 2010, 16, 59–63. [Google Scholar] [CrossRef]
- Simon, S.D.; Reig, A.S.; Archer, K.J.; A Mericle, R. Biomechanical attributes of microcatheters used in liquid embolization of intracranial aneurysms. J. Neurointerv. Surg. 2011, 4, 211–214. [Google Scholar] [CrossRef]
- Asouhidou, I.; Katsaridis, V.; Meng, L.; Zilianaki, D.; Vaidis, G.; Ioannou, P.; Georgiadis, G. Desaturation during Onyx embolization. Br. J. Anaesth. 2010, 105, 385–386. [Google Scholar] [CrossRef] [Green Version]
- Murugesan, C.; Saravanan, S.; Rajkumar, J.; Prasad, J.; Banakal, S.; Muralidhar, K. Severe pulmonary oedema following therapeutic embolization with Onyx for cerebral arteriovenous malformation. Neuroradiology 2008, 50, 439–442. [Google Scholar] [CrossRef]
- Loffroy, R.; Midulla, M.; Falvo, N.; Chevallier, O. Ethylene Vinyl Alcohol Copolymer as First Hemostatic Liquid Embolic Agent for Non-variceal Upper Gastrointestinal Bleeding Patients: Pros and Cons. Cardiovasc. Interv. Radiol. 2018, 41, 1808–1809. [Google Scholar] [CrossRef]
- Pop, R.; Mertz, L.; Ilyes, A.; Mihoc, D.; Richter, J.S.; Manisor, M.; Kremer, S.; Beaujeux, R. Beam hardening artifacts of liquid embolic agents: Comparison between Squid and Onyx. J. Neurointerv. Surg. 2018, 11, 706–709. [Google Scholar] [CrossRef]
- Nogueira, R.G.; Bayrlee, A.; Hirsch, J.A.; Yoo, A.J.; Copen, W.A. Dynamic Contrast-Enhanced MRA at 1.5 T for Detection of Arteriovenous Shunting Before and After Onyx Embolization of Cerebral Arteriovenous Malformations. J. Neuroimaging 2013, 23, 514–517. [Google Scholar] [CrossRef]
- Jankowitz, B.T.; Vora, N.; Jovin, T.; Horowitz, M. Ear Necrosis Resulting from the Endovascular Onyx-18 Embolization of a Dural Arteriovenous Fistula Fed by the Posterior Auricular Artery. J. Neuroimaging 2009, 19, 259–262. [Google Scholar] [CrossRef]
- Walcott, B.P.; Gerrard, J.; Nogueira, R.G.; Nahed, B.V.; Terry, A.R.; Ogilvy, C.S. Microsurgical retrieval of an endovascular microcatheter trapped during Onyx embolization of a cerebral arteriovenous malformation. J. Neurointerv. Surg. 2010, 3, 77–79. [Google Scholar] [CrossRef]
- Kilani, M.S.; Izaaryene, J.; Cohen, F.; Varoquaux, A.; Gaubert, J.; Louis, G.; Jacquier, A.; Bartoli, J.; Moulin, G.; Vidal, V. Ethylene vinyl alcohol copolymer (Onyx®) in peripheral interventional radiology: Indications, advantages and limitations. Diagn. Interv. Imaging 2015, 96, 319–326. [Google Scholar] [CrossRef]
- Chemelli, A.P.; Thauerer, M.; Wiedermann, F.J.; Strasak, A.; Klocker, J.; Chemelli-Steingruber, I.E. Transcatheter arterial embolization for the management of iatrogenic and blunt traumatic intercostal artery injuries. J. Vasc. Surg. 2009, 49, 1505–1513. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lai, H.-Y.; Wu, K.-T.; Liu, Y.; Zeng, Z.-F.; Zhang, B. Angiography and transcatheter arterial embolization for non-variceal gastrointestinal bleeding. Scand. J. Gastroenterol. 2020, 55, 931–940. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.F.; Lai, K.W.; Yung, A.W.; Luk, W.H.; Cheng, L.F.; Ma, J.K. Transcatheter arterial embolisation can be the standard treatment for non-variceal upper gastrointestinal bleeding refractory to endoscopy. Hong Kong Med. J. Xianggang Yi Xue Za Zhi 2019, 25, 164–166. [Google Scholar] [CrossRef] [PubMed] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | All Patients (n = 53) |
|---|---|
| Age (years) | 66.2 (±15) |
| Sex (M/F) | 34 (64.2%)/19 (35.8%) |
| COVID-19 | 10 (18.9%) |
| eGFR (mL/min) | 68 (±25) |
| CKD Stage | 2 (1–3) |
| INR | 1.2 (±0.3) |
| aPTT | 35.8 (±4.8) |
| Platelet count (No. ×103/μL) | 386.1 (±73.4) |
| Coagulopathy | 8 (15.1%) |
| Hemoglobin (g/dL) | 7.7 (±0.7) |
| CT angiography execution | 47 (88.7%) |
| Bleeding on CT angiography | 47 (88.7%) |
| Hematoma volume (mL) | 231.3 (±298.6) |
| Antiplatelet therapy - Single list - Dual | 21 (39.6%) 15 (28.3%) 6 (11.3%) |
| Anticoagulant therapy | 13 (24.5%) |
| Antiplatelet AND anticoagulant therapy | 2 (3.8%) |
| Antiplatelet OR anticoagulant therapy | 30 (56.6%) |
| Variables | All Patients (n = 53) |
|---|---|
| Bleeding on XA | 50 (94.3%) |
| Blind embolization | 3 (5.7%) |
| Site of bleeding - Pelvic - Upper GI - Lower GI - Abdomen - Thorax - Neck - Limbs | 15 (28.4%) 4 (7.5%) 2 (3.8%) 18 (34%) 8 (15%) 2 (3.8%) 4 (7.5%) |
| Number of embolized vessels | 1.4 (±0.8) |
| Cause of bleeding - Trauma - Spontaneous - Others (tumors, diverticula, ulcers, etc.) | 31 (58.5%) 5 (9.4%) 16 (32.1%) |
| Embolic agent concentration - 12 - 18 - 20 - 34 | 4 (7.5%) 6 (11.3%) 20 (37.7%) 23 (43.5%) |
| Embolic agent dose (mL) | 0.5 (±0.3) |
| Use of an additional embolic agent | 0 (0%) |
| Intraoperative unfractionated heparin (IU) | 528.3 (±952.8) |
| Intraoperative contrast medium (mL) | 35.2 (±9.4) |
| Volume of contrast to creatinine clearance ratio | 0.7 (±0.6) |
| Vascular access site - Femoral - Radial - Brachial | 40 (75.5%) 11 (20.7%) 2 (3.8%) |
| Sheath diameter, 4F/5F/6F/≥7F | 6 (11.3%)/44 (83.0%)/3 (5.7%)/0 (0%) |
| Angiography injection technique, manual/powered | 29 (54.7%)/24 (45.3%) |
| CT-to-groin time (min) | 22.9 (±12.4) |
| Procedure time (min) | 27.5 (±7) |
| CT-to-embolization time (min) | 50.3 (±13.1) |
| Fluoroscopy time (min) | 7.5 (±2.8) |
| Cumulative air kerma (mGy) | 160 (±58.3) |
| Dose area product (DAP) (Gy/cm2) | 25.1 (±9.3) |
| Variables | All Patients (n = 53) |
|---|---|
| Technical success | 53 (100%) |
| Clinical success | 51 (96.2%) |
| Vascular access site hemostasis - Manual compression - Vascular closure device | 50 (94.3%) 3 (5.7%) |
| Units of packed red blood cells transfused per patient | 1 (±0.6) |
| Rebleeding | 2 (3.8%) |
| Nontarget embolization | 1 (1.9%) |
| Complications | 6 (11.3%) |
| Vascular access site complications (VASCs) | 2 (3.8%) |
| Complications, according to SIR classifications - None - Minor (grade 1–2) - Major (grade 3–5) | 47 (88.7%) 4 (7.5%) 2 (3.8%) |
| Complications, according to CIRSE classification - Grade 0 - Grade 3 - Grade 6 | 47 (88.7%) 5 (9.4%) 1 (1.9%) |
| Treatment required for complications - None - Medical - Interventional - Surgical | 47 (88.7%) 5 (9.4%) 1 (1.9%) 0 (0%) |
| 30-day mortality | 1 (1.9%) |
| Variables | Group 1 (n° = 8) Patients with Coagulopathy | Group 2 (n° = 45) Patients without Coagulopathy | p Value |
|---|---|---|---|
| COVID-19 | 2 (25%) | 8 (17.8%) | 0.6364 |
| INR | 1.6 (1.5–1.8) | 1.1 (1–1.2) | 0.0002 |
| Platelet count (No. ×103/μL) | 393 (254–423) | 394 (378–421) | 0.4709 |
| Antiplatelet OR anticoagulant therapy | 4 (50%) | 26 (57.8%) | 0.7153 |
| Embolic agent dose (mL) | 0.5 (0.4–1) | 0.4 (0.3–0.6) | 0.3719 |
| Procedure time (min) | 30 (26–31) | 27 (22–32) | 0.4182 |
| Fluoroscopy time (min) | 7 (7–10) | 7 (6–9) | 0.2635 |
| Technical success | 8 (100%) | 45 (100%) | 1 |
| Clinical success | 7 (87.5%) | 44 (97.8%) | 0.2816 |
| Rebleeding | 7 (87.5%) | 44 (97.8%) | 0.2816 |
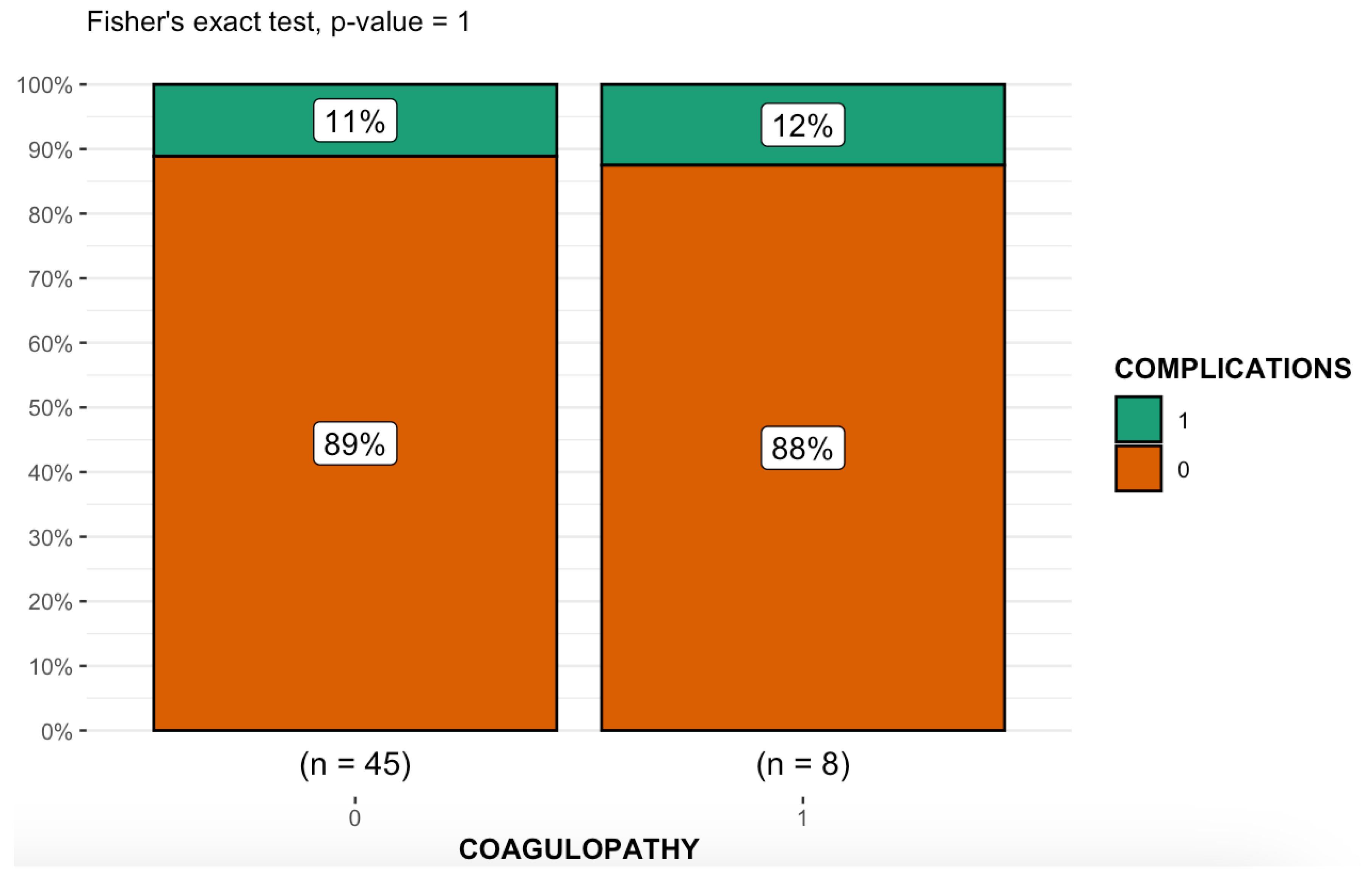
| Complications | 1 (12.5%) | 5 (11.1%) | 1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minici, R.; Venturini, M.; Fontana, F.; Guzzardi, G.; Pingitore, A.; Piacentino, F.; Serra, R.; Coppola, A.; Santoro, R.; Laganà, D. Efficacy and Safety of Ethylene-Vinyl Alcohol (EVOH) Copolymer-Based Non-Adhesive Liquid Embolic Agents (NALEAs) in Transcatheter Arterial Embolization (TAE) of Acute Non-Neurovascular Bleeding: A Multicenter Retrospective Cohort Study. Medicina 2023, 59, 710. https://doi.org/10.3390/medicina59040710
Minici R, Venturini M, Fontana F, Guzzardi G, Pingitore A, Piacentino F, Serra R, Coppola A, Santoro R, Laganà D. Efficacy and Safety of Ethylene-Vinyl Alcohol (EVOH) Copolymer-Based Non-Adhesive Liquid Embolic Agents (NALEAs) in Transcatheter Arterial Embolization (TAE) of Acute Non-Neurovascular Bleeding: A Multicenter Retrospective Cohort Study. Medicina. 2023; 59(4):710. https://doi.org/10.3390/medicina59040710
Chicago/Turabian StyleMinici, Roberto, Massimo Venturini, Federico Fontana, Giuseppe Guzzardi, Armando Pingitore, Filippo Piacentino, Raffaele Serra, Andrea Coppola, Rita Santoro, and Domenico Laganà. 2023. "Efficacy and Safety of Ethylene-Vinyl Alcohol (EVOH) Copolymer-Based Non-Adhesive Liquid Embolic Agents (NALEAs) in Transcatheter Arterial Embolization (TAE) of Acute Non-Neurovascular Bleeding: A Multicenter Retrospective Cohort Study" Medicina 59, no. 4: 710. https://doi.org/10.3390/medicina59040710