

Benefits of Antimicrobial Photodynamic Therapy as an Adjunct to Non-Surgical Periodontal Treatment in Smokers with Periodontitis: A Systematic Review and Meta-Analysis
 ,
,  and
and 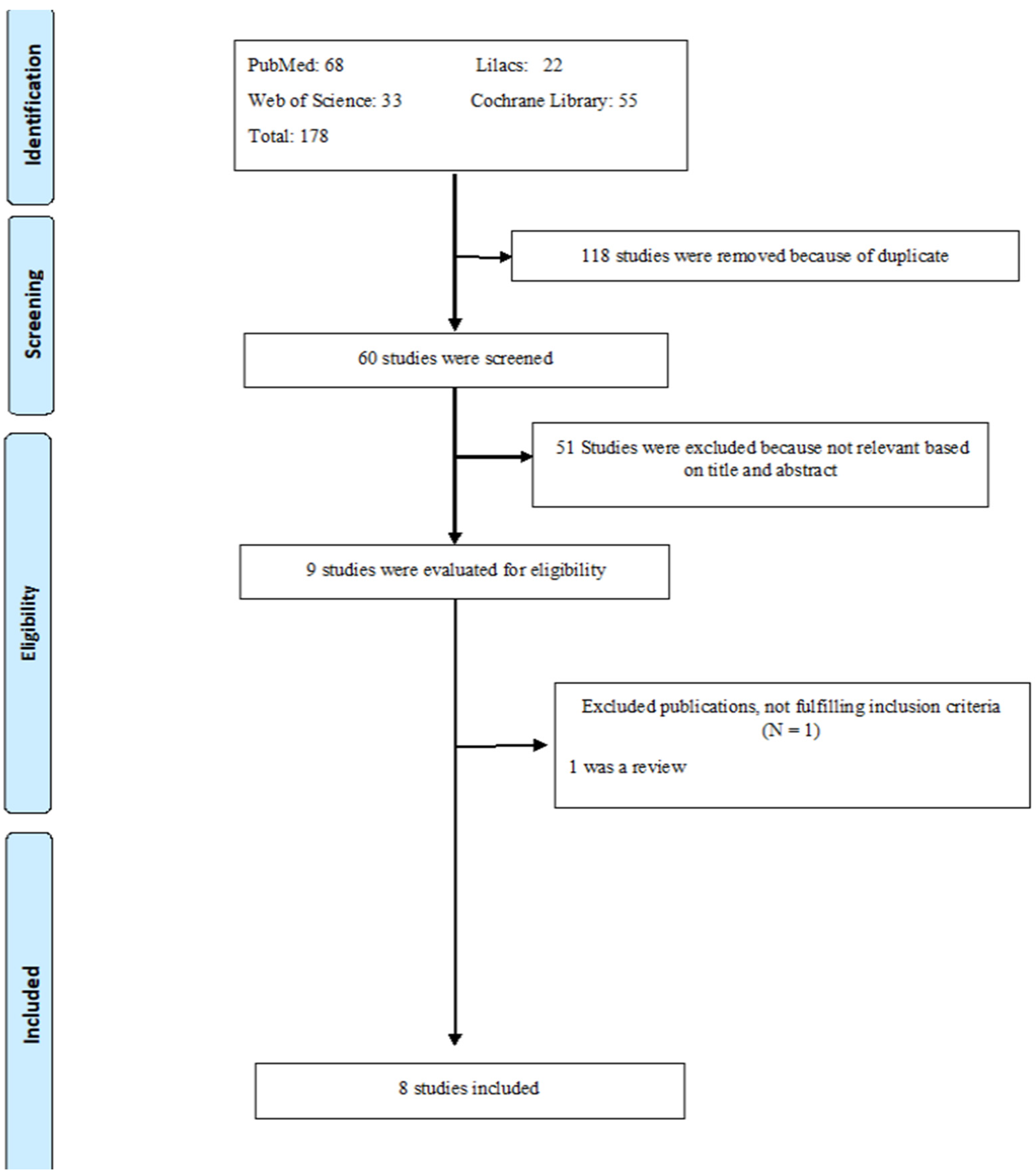{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Inclusion Criteria
- -
- Changes in periodontal clinical parameters (reduction in pocket depth (PD) and gain in clinical attachment level (CAL)).
- -
- Changes in microbiological parameters (changes in the bacterial population—bacterial count).
- -
- PD and CAL in millimeters (mm).
- -
- Changes in microbiological proportion and/or percentage.
2.2. Secondary Outcomes
2.3. Extracted Data
2.4. Risk of Bias Assessment
2.5. Data Analysis
3. Results
3.1. Selection of Studies
3.2. Characteristics of the Included Studies
3.3. Definition of the Disease
3.4. Characteristics of Laser and Photosensitizer
3.5. Periodontal Therapy and Protocol for aPDT Administration
3.6. Clinical Parameter Results
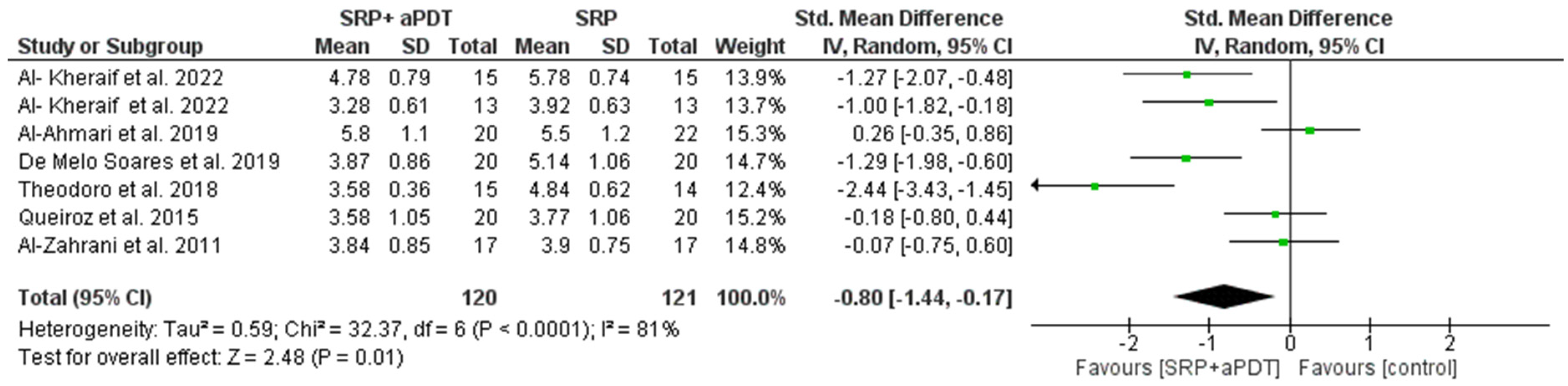
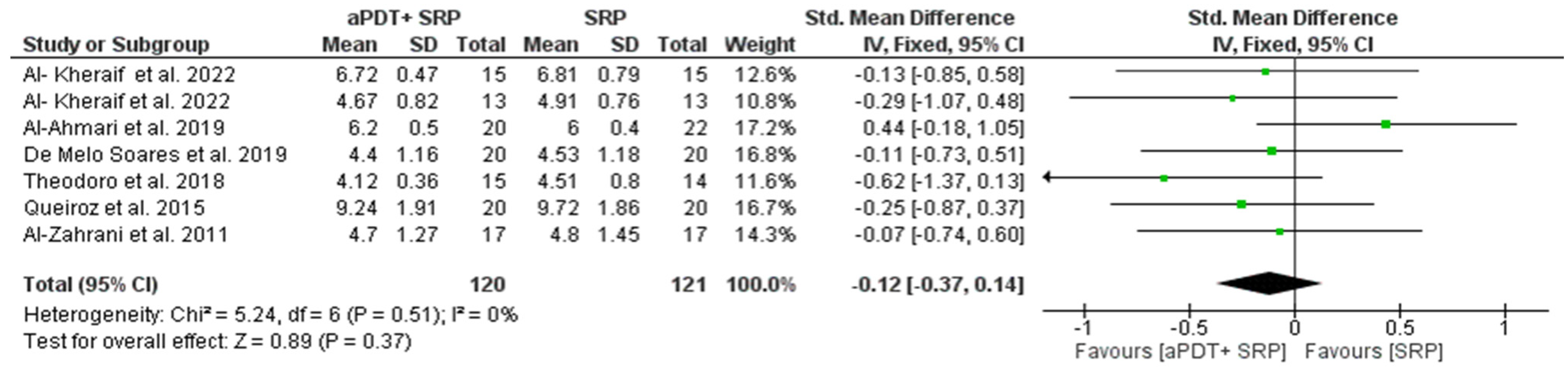
3.7. Results of the Quantitative Assessment of PD and CAL
3.8. Microbiological Parameters
3.8.1. Sample Collection Site
3.8.2. Microbiological Techniques Used
3.8.3. Microbiological Parameter Results
3.8.4. Secondary Results
3.8.5. Quality Assessment
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hajishengallis, G.; Lamont, R.J. Beyond the red complex and into more complexity: The polymicrobial synergy and dysbiosis (PSD) model of periodontal disease etiology. Mol. Oral Microbiol. 2012, 27, 409–419. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Williams, R.C.; Offenbacher, S. Periodontal medicine: The emergence of a new branch of periodontology. Periodontology 2000, 23, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Haber, J. Smoking is a major risk factor for periodontitis. Curr. Opin. Periodontol. 1994, 12–18. [Google Scholar] [PubMed]
- Ryder, M.I.; Couch, E.T.; Chaffee, B.W. Personalized periodontal treatment for the tobacco- and alcohol-using patient. Periodontology 2018, 78, 30–46. [Google Scholar] [CrossRef] [PubMed]
- Graves, D.; Corrêa, J.; Silva, T. The oral microbiota is modified by systemic diseases. J. Dent. Res. 2019, 98, 148–156. [Google Scholar] [CrossRef]
- Hajishengallis, G. Periodontitis: From microbial immune subversion to systemic inflammation. Nat. Rev. Immunol. 2015, 15, 30–44. [Google Scholar] [CrossRef] [Green Version]
- Curtis, M.A.; Diaz, P.I.; Van Dyke, T.E. The role of the microbiota in periodontal disease. Periodontology 2020, 83, 14–25. [Google Scholar] [CrossRef]
- de Cristhiam, J.H.M.; Villafuerte, K.R.V.; Luchiari, H.R.; de Juliana, O.C.; Sales, M.; Palioto, D.B.; Messora, M.R.; Souza, S.L.S.; Taba, M., Jr.; Ramos, E.S.; et al. Effect of smoking on the DNA methylation pattern of the SOCS1 promoter in epithelial cells from the saliva of patients with chronic periodontitis. J. Periodontol. 2019, 90, 1279–1286. [Google Scholar] [CrossRef]
- Bergström, J.; Eliasson, S.; Preber, H. Cigarette smoking and periodontal bone loss. J. Periodontol. 1991, 62, 242–246. [Google Scholar] [CrossRef]
- Albandar, J.M.; Streckfus, C.F.; Adesanya, M.R.; Winn, D.M. Cigar, pipe, and cigarette smoking as risk factors for periodontal disease and tooth loss. J. Periodontol. 2000, 71, 1874–1881. [Google Scholar] [CrossRef]
- Camelo-Castillo, A.J.; Mira, A.; Pico, A.; Nibali, L.; Henderson, B.; Donos, N.; Tomás, I. Subgingival microbiota in health compared to periodontitis and the influence of smoking. Front. Microbiol. 2015, 6, 119. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suvan, J.; Leira, Y.; Moreno Sancho, F.M.; Graziani, F.; Derks, J.; Tomasi, C. Subgingival instrumentation for treatment of periodontitis. A systematic review. J. Clin. Periodontol. 2020, 47 (Suppl. S22), 155–175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- How, K.Y.; Song, K.P.; Chan, K.G. Porphyromonas gingivalis: An Overview of Periodontopathic Pathogen below the Gum Line. Front. Microbiol. 2016, 7, 53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azaripour, A.; Dittrich, S.; van Noorden, C.J.F.; Willershausen, B. Efficacy of photodynamic therapy as adjunct treatment of chronic periodontitis: A systematic review and meta-analysis. Lasers Med. Sci. 2018, 33, 407–423. [Google Scholar] [CrossRef]
- Rajesh, S.; Koshi, E.; Philip, K.; Mohan, A. Antimicrobial photodynamic therapy: An overview. J. Indian Soc. Periodontol. 2011, 15, 323. [Google Scholar] [CrossRef]
- Dolmans, D.E.; Fukumura, D.; Jain, R.K. Photodynamic therapy for cancer. Nat. Rev. Cancer 2003, 3, 380–387. [Google Scholar] [CrossRef]
- Braham, P.; Herron, C.; Street, C.; Darveau, R. Antimicrobial photodynamic therapy may promote periodontal healing through multiple mechanisms. J. Periodontol. 2009, 80, 1790–1798. [Google Scholar] [CrossRef]
- Fontana, C.R.; Abernethy, A.D.; Som, S.; Ruggiero, K.; Doucette, S.; Marcantonio, R.C.; Boussios, C.I.; Kent, R.; Goodson, J.M.; Tanner, A.C.; et al. The antibacterial effect of photodynamic therapy in dental plaque-derived biofilms. J. Periodontal. Res. 2009, 44, 751–759. [Google Scholar] [CrossRef]
- Goulart Rde, C.; Bolean, M.; Paulino Tde, P.; Thedei, G., Jr.; Souza, S.L.; Tedesco, A.C.; Ciancaglini, P. Photodynamic therapy in planktonic and biofilm cultures of Aggregatibacter actinomycetemcomitans. Photomed. Laser Surg. 2010, 28 (Suppl. S1), S53–S60. [Google Scholar] [CrossRef]
- Theodoro, L.H.; Assem, N.Z.; Longo, M.; Alves, M.L.F.; Duque, C.; Stipp, R.N.; Vizoto, N.L.; Garcia, V.G. Treatment of periodontitis in smokers with multiple sessions of antimicrobial photodynamic therapy or systemic antibiotics: A randomized clinical trial. Photodiagn. Photodyn. Ther. 2018, 22, 217–222. [Google Scholar] [CrossRef]
- de Melo Soares, M.S.; D’Almeida Borges, C.; de Mendonça Invernici, M.; Frantz, F.G.; de Figueiredo, L.C.; de Souza, S.L.S.; Taba, M., Jr.; Messora, M.R.; Novaes, A.B., Jr. Antimicrobial photodynamic therapy as adjunct to non-surgical periodontal treatment in smokers: A randomized clinical trial. Clin. Oral Investig. 2019, 23, 3173–3182. [Google Scholar] [CrossRef] [PubMed]
- Li, S.M.; Ji, Y.Z.; Wu, S.S.; Zhan, S.Y.; Wang, B.; Liu, L.R.; Li, S.Y.; Wang, N.L.; Wang, J.J. Multifocal versus single vision lenses intervention to slow progression of myopia in school-age children: A meta-analysis. Surv. Ophthalmol. 2011, 56, 451–460. [Google Scholar] [CrossRef]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- AlAhmari, F.; Ahmed, H.B.; Al-Kheraif, A.A.; Javed, F.; Akram, Z. Effectiveness of scaling and root planning with and without adjunct antimicrobial photodynamic therapy in the treatment of chronic periodontitis among cigarette-smokers and never-smokers: A randomized controlled clinical trial. Photodiagn. Photodyn. Ther. 2019, 25, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Al-Kheraif, A.A.; Alshahrani, O.A.; Al-Shehri, A.M.; Khan, A.A. Chloro-aluminum phthalocyanine-mediated photodynamic therapy in the treatment of stage-II chronic periodontitis among smokers. Photodermatol. Photoimmunol. Photomed. 2022, 38, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Al-Kheraif, A.A.; Alshahrani, O.A.; Al-Shehri, A.M.; Khan, A.A. Antimicrobial photodynamic therapy using chloro-aluminum phthalocyanine for treating advanced stage-III periodontitis in smoking patients. Photodermatol. Photoimmunol. Photomed. 2022, 38, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Queiroz, A.C.; Suaid, F.A.; de Andrade, P.F.; Oliveira, F.S.; Novaes, A.B., Jr.; Taba, M., Jr.; Palioto, D.B.; Grisi, M.F.; Souza, S.L. Adjunctive effect of antimicrobial photodynamic therapy to nonsurgical periodontal treatment in smokers: A randomized clinical trial. Lasers Med. Sci. 2015, 30, 617–625. [Google Scholar] [CrossRef]
- Queiroz, A.C.; Suaid, F.A.; de Andrade, P.F.; Novaes, A.B., Jr.; Taba, M., Jr.; Palioto, D.B.; Grisi, M.F.; Souza, S.L. Antimicrobial photodynamic therapy associated to nonsurgical periodontal treatment in smokers: Microbiological results. J. Photochem. Photobiology B Biol. 2014, 141, 170–175. [Google Scholar] [CrossRef]
- Al-Zahrani, M.S.; Austah, O.N. Photodynamic therapy as an adjunctive to scaling and root planing in treatment of chronic periodontitis in smokers. Saudi Med. J. 2011, 32, 1183–1188. [Google Scholar]
- Akram, Z.; Raffat, M.A.; Saad Shafqat, S.; Mirza, S.; Ikram, S. Clinical efficacy of photodynamic therapy as an adjunct to scaling and root planing in the treatment of chronic periodontitis among cigarette smokers: A systematic review and meta-analysis. Photodiagn. Photodyn. Ther. 2019, 26, 334–341. [Google Scholar] [CrossRef]
- Papapanou, P.N.; Sanz, M.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemmig, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89 (Suppl. S1), S173–S182. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Socransky, S.S.; Haffajee, A.D.; Cugini, M.A.; Smith, C.; Kent, R.L., Jr. Microbial complexes in subgingival plaque. J. Clin. Periodontol. 1998, 25, 134–144. [Google Scholar] [CrossRef] [PubMed]
- Zeller, I.; Hutcherson, J.A.; Lamont, R.J.; Demuth, D.R.; Gumus, P.; Nizam, N.; Buduneli, N.; Scott, D.A. Altered antigenic profiling and infectivity of Porphyromonas gingivalis in smokers and non-smokers with periodontitis. J. Periodontol. 2014, 85, 837–844. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chambrone, L.; Wang, H.L.; Romanos, G.E. Antimicrobial photodynamic therapy for the treatment of periodontitis and peri-implantitis: An American Academy of Periodontology best evidence review. J. Periodontol. 2018, 89, 783–803. [Google Scholar] [CrossRef]
- Ramanauskaite, E.; Moraschini, V.; Machiulskiene, V.; Sculean, A. Clinical efficacy of single and multiple applications of antimicrobial photodynamic therapy in periodontal maintenance: A systematic review and network meta-analysis. Photodiagn. Photodyn. Ther. 2021, 36, 102435. [Google Scholar] [CrossRef]
- Franco, T.P.M.; Dos Santos, A.P.P.; Canabarro, A. The effects of repeated applications of antimicrobial photodynamic therapy in the treatment of residual periodontal pockets: A systematic review. Lasers Med. Sci. 2019, 34, 855–863. [Google Scholar] [CrossRef]
- Derikvand, N.; Ghasemi, S.S.; Safiaghdam, H.; Piriaei, H.; Chiniforush, N. Antimicrobial Photodynamic Therapy with Diode laser and Methylene blue as an adjunct to scaling and root planning: A clinical trial. Photodiagn. Photodyn. Ther. 2020, 31, 101818. [Google Scholar] [CrossRef]
- Nuernberg, M.A.A.; Wainwright, M.; Miessi, D.M.J.; Scalet, V.; Olivo, M.B.; Ervolino, E.; Garcia, V.G.; Theodoro, L.H. Effects of butyl toluidine blue photosensitizer on antimicrobial photodynamic therapy for experimental periodontitis treatment in rats. Photodiagn. Photodyn. Ther. 2020, 31, 101868. [Google Scholar] [CrossRef]
- de Almeida, J.M.; Matheus, H.R.; Sendão Alves, B.E.; Rodrigues Gusman, D.J.; Nagata, M.J.H.; de Abreu Furquim, E.M.; Ervolino, E. Evaluation of antimicrobial photodynamic therapy with acidic methylene blue for the treatment of experimental periodontitis. PLoS ONE 2022, 17, e0263103. [Google Scholar] [CrossRef]
- Ahmed, A.R.; Kamran, M.A.; Suleman, G.; Sharif, R.A.; Alamrey, A.A.M.; Sulaiman, S.A. Novel use of chloro-aluminum phthalocyanine assisted photodynamic therapy helps in periimplant healing among smoking patients. Photodiagn. Photodyn. Ther. 2022, 41, 103193. [Google Scholar] [CrossRef]
- Palmer, R.M.; Wilson, R.F.; Hasan, A.S.; Scott, D.A. Mechanisms of action of environmental factors—Tobacco smoking. J. Clin. Periodontol. 2005, 32 (Suppl. S6), 180–195. [Google Scholar] [CrossRef] [PubMed]
- Boström, L.; Linder, L.E.; Bergström, J. Smoking and GCF levels of IL-1beta and IL-1ra in periodontal disease. J. Clin. Periodontol. 2000, 27, 250–255. [Google Scholar] [CrossRef] [PubMed]
- Boström, L.; Linder, L.E.; Bergström, J. Smoking and crevicular fluid levels of IL-6 and TNF-alpha in periodontal disease. J. Clin. Periodontol. 1999, 26, 352–357. [Google Scholar] [CrossRef]
- Izakovicova Holla, L.; Hrdlickova, B.; Vokurka, J.; Fassmann, A. Matrix metalloproteinase 8 (MMP8) gene polymorphisms in chronic periodontitis. Arch. Oral Biol. 2012, 57, 188–196. [Google Scholar] [CrossRef] [PubMed]
- Beck, J.D.; Papapanou, P.N.; Philips, K.H.; Offenbacher, S. Periodontal Medicine: 100 Years of Progress. J. Dent. Res. 2019, 98, 1053–1062. [Google Scholar] [CrossRef] [PubMed]





Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Villafuerte, K.R.V.; Martinez, C.J.H.; Palucci Vieira, L.H.; Nobre, A.V. Benefits of Antimicrobial Photodynamic Therapy as an Adjunct to Non-Surgical Periodontal Treatment in Smokers with Periodontitis: A Systematic Review and Meta-Analysis. Medicina 2023, 59, 684. https://doi.org/10.3390/medicina59040684
Villafuerte KRV, Martinez CJH, Palucci Vieira LH, Nobre AV. Benefits of Antimicrobial Photodynamic Therapy as an Adjunct to Non-Surgical Periodontal Treatment in Smokers with Periodontitis: A Systematic Review and Meta-Analysis. Medicina. 2023; 59(4):684. https://doi.org/10.3390/medicina59040684
Chicago/Turabian StyleVillafuerte, Kelly R. V., Cristhiam Jesus H. Martinez, Luiz H. Palucci Vieira, and Atila V. Nobre. 2023. "Benefits of Antimicrobial Photodynamic Therapy as an Adjunct to Non-Surgical Periodontal Treatment in Smokers with Periodontitis: A Systematic Review and Meta-Analysis" Medicina 59, no. 4: 684. https://doi.org/10.3390/medicina59040684