
Safety, Pharmacokinetic and Pharmacodynamic Evaluation of Teverelix for the Treatment of Hormone-Sensitive Advanced Prostate Cancer: Phase 2 Loading-Dose-Finding Studies
Abstract
:1. Introduction
2. Materials and Methods
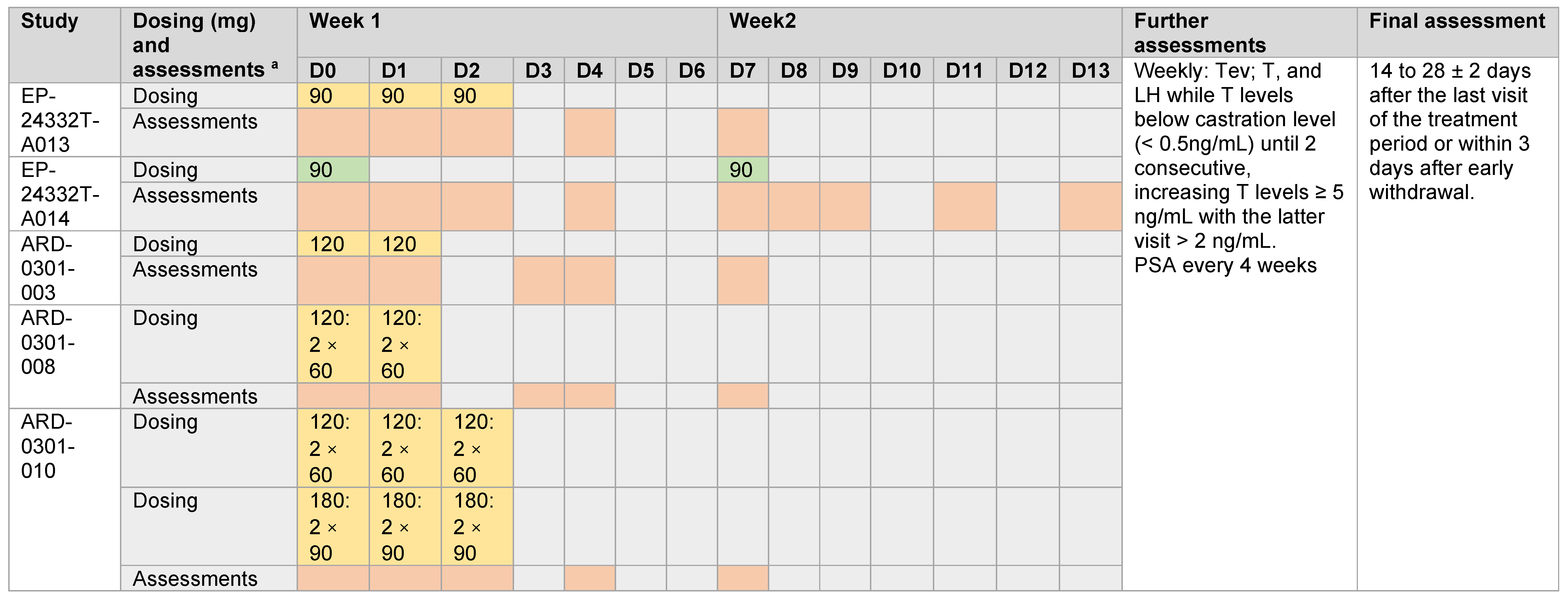
2.1. Study Design, Conduct and Treatment
2.2. Patients
- Histologically proven adenocarcinoma of the prostate;
- Androgen deprivation therapy suitable (advanced prostate cancer, i.e., with local invasion or/and metastasis);
- Signed written informed consent.
- Liver or renal function tests (ASAT/SGOT, ALAT/SGPT, total bilirubin, creatinine) exceeding twice the upper limit of the normal range, unless the elevation is attributed to hepatic metastasis;
- Any contraindication to the use of Teverelix DP;
- Life expectancy of less than 1 year;
- Baseline testosterone value below 2.31 ng/mL;
- Bilateral orchidectomy;
- Pre-existing hormone therapy or planned concomitant use of androgen deprivation therapy with any agent other than the investigational drug;
- Neurological, psychiatric disease, drug or alcohol abuse which could interfere with the subject’s proper compliance;
- Evidence of concurrent malignancy;
- Exposure to another investigational agent within the last month;
- Lack of ability or willingness to give informed consent;
- Anticipated non-availability for study visits/procedures.
2.3. Outcomes and Assessments
2.4. Statistical Analysis
3. Results
3.1. Patients
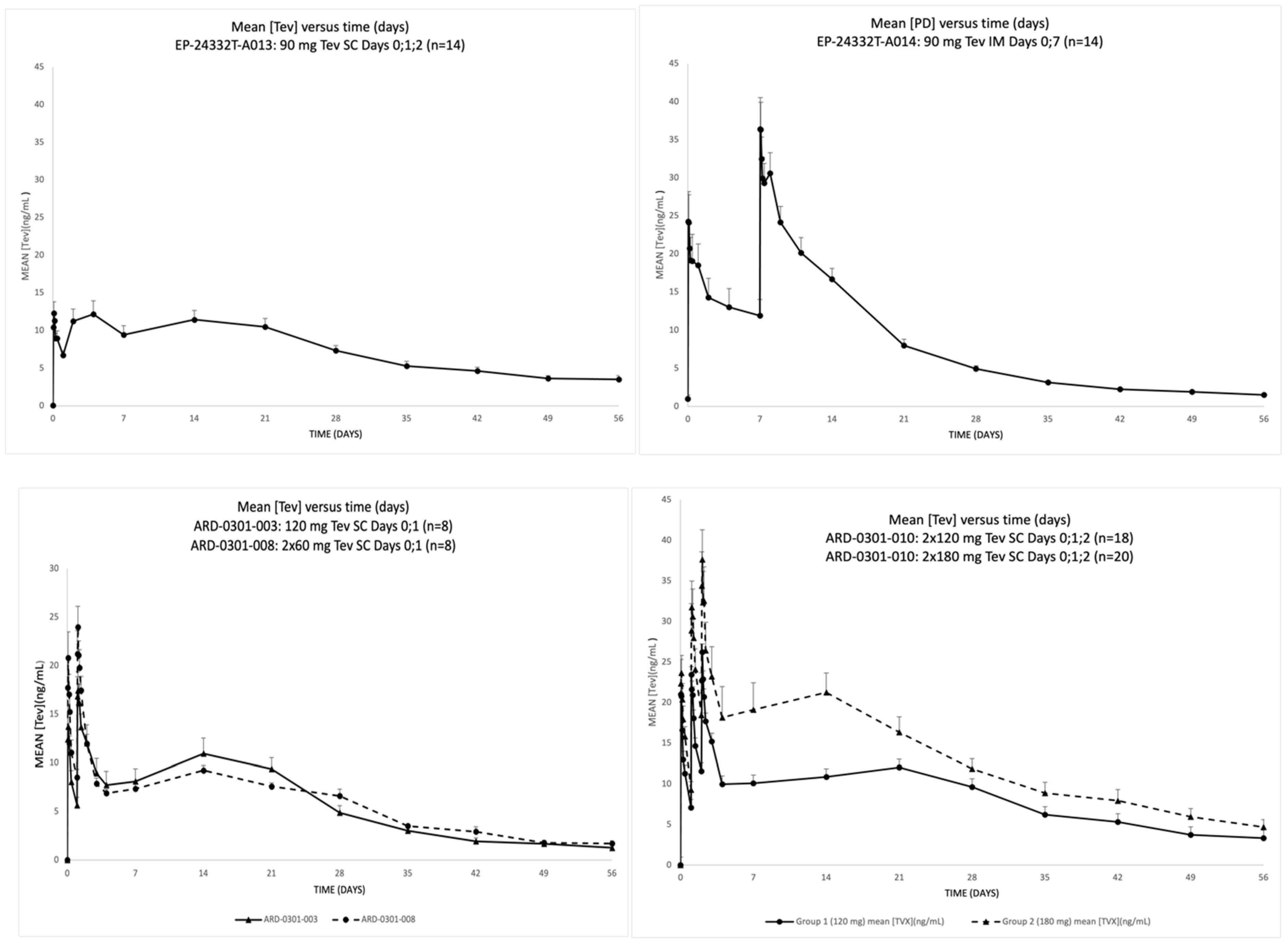
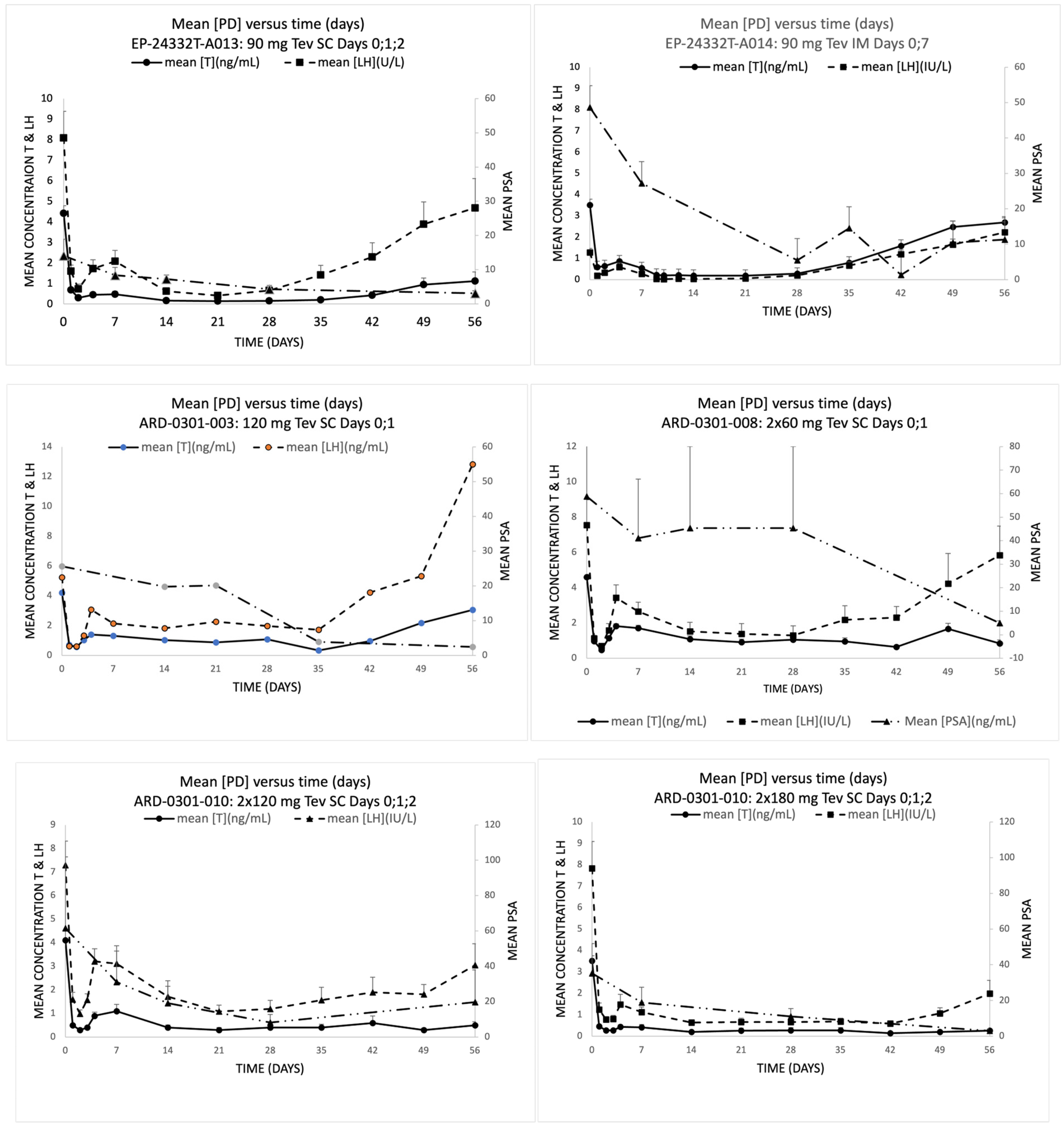
3.2. Efficacy, Pharmacokinetic and Pharmacodynamic Evaluations
3.3. Safety and Tolerability
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Parker, C.; Castro, E.; Fizazi, K.; Heidenreich, A.; Ost, P.; Procopio, G.; Tombal, B.; Gillessen, S. Prostate cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2020, 31, 1119–1134. [Google Scholar] [CrossRef]
- Mohler, J.L.; Antonarakis, E.S.; Armstrong, A.J.; D’Amico, A.V.; Davis, B.J.; Dorff, T.; Eastham, J.A.; Enke, C.A.; Farrington, T.A.; Higano, C.S.; et al. Prostate Cancer, Version 2.2019, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2019, 17, 479–505. [Google Scholar] [CrossRef] [Green Version]
- Van Poppel, H.; Abrahamsson, P.-A. Considerations for the use of gonadotropin-releasing hormone agonists and antagonists in patients with prostate cancer. Int. J. Urol. 2020, 27, 830–837. [Google Scholar] [CrossRef]
- Keating, N.L.; O’Malley, A.J.; Freedland, S.J.; Smith, M.R. Diabetes and Cardiovascular Disease During Androgen Deprivation Therapy: Observational Study of Veterans With Prostate Cancer. JNCI J. Natl. Cancer Inst. 2010, 102, 39–46. [Google Scholar] [CrossRef] [Green Version]
- Keating, N.L.; O’Malley, A.J.; Smith, M.R. Diabetes and cardiovascular disease during androgen deprivation therapy for prostate cancer. J. Clin. Oncol. 2006, 24, 4448–4456. [Google Scholar] [CrossRef]
- Okwuosa, T.M.; Morgans, A.; Rhee, J.-W.; Reding, K.W.; Maliski, S.; Plana, J.-C.; Volgman, A.S.; Moseley, K.F.; Porter, C.B.; Ismail-Khan, R.; et al. Impact of Hormonal Therapies for Treatment of Hormone-Dependent Cancers (Breast and Prostate) on the Cardiovascular System: Effects and Modifications: A Scientific Statement From the American Heart Association. Circ. Genom. Precis. Med. 2021, 14, e000082. [Google Scholar] [CrossRef] [PubMed]
- McLeod, D.; Zinner, N.; Tomera, K.; Gleason, D.; Fotheringham, N.; Campion, M.; Garnick, M.B. A phase 3, multicenter, open-label, randomized study of abarelix versus leuprolide acetate in men with prostate cancer. Urology 2001, 58, 756–761. [Google Scholar] [CrossRef]
- Debruyne, F.; Bhat, G.; Garnick, M.B. Abarelix for injectable suspension: First-in-class gonadotropin-releasing hormone antagonist for prostate cancer. Future Oncol. 2006, 2, 677–696. [Google Scholar] [CrossRef]
- Van Poppel, H.; Klotz, L. Gonadotropin-releasing hormone: An update review of the antagonists versus agonists. Int. J. Urol. 2012, 19, 594–601. [Google Scholar] [CrossRef]
- Klotz, L.; Boccon-Gibod, L.; Shore, N.D.; Andreou, C.; Persson, B.E.; Cantor, P.; Jensen, J.K.; Olesen, T.K.; Schröder, F.H. The efficacy and safety of degarelix: A 12-month, comparative, randomized, open-label, parallel-group phase III study in patients with prostate cancer. BJU Int. 2008, 102, 1531–1538. [Google Scholar] [CrossRef]
- Shore, N.D.; Saad, F.; Cookson, M.S.; George, D.J.; Saltzstein, D.R.; Tutrone, R.; Akaza, H.; Bossi, A.; van Veenhuyzen, D.F.; Selby, B.; et al. Oral Relugolix for Androgen-Deprivation Therapy in Advanced Prostate Cancer. N. Engl. J. Med. 2020, 382, 2187–2196. [Google Scholar] [CrossRef] [PubMed]
- Cirne, F.; Aghel, N.; Petropoulos, J.A.; Klotz, L.; Lenihan, D.J.; Saad, F.; Pinthus, J.; Leong, D.P. The cardiovascular effects of gonadotropin-releasing hormone antagonists in men with prostate cancer. Eur. Heart J. Cardiovasc. Pharmacother. 2022, 8, 253–262. [Google Scholar] [CrossRef]
- Abufaraj, M.; Iwata, T.; Kimura, S.; Haddad, A.; Al-Ani, H.; Abusubaih, L.; Moschini, M.; Briganti, A.; Karakiewicz, P.I.; Shariat, S.F. Differential Impact of Gonadotropin-releasing Hormone Antagonist Versus Agonist on Clinical Safety and Oncologic Outcomes on Patients with Metastatic Prostate Cancer: A Meta-analysis of Randomized Controlled Trials. Eur. Urol. 2021, 79, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Margel, D.; Peer, A.; Ber, Y.; Shavit-Grievink, L.; Tabachnik, T.; Sela, S.; Witberg, G.; Baniel, J.; Kedar, D.; Duivenvoorden, W.C.M.; et al. Cardiovascular Morbidity in a Randomized Trial Comparing GnRH Agonist and GnRH Antagonist among Patients with Advanced Prostate Cancer and Preexisting Cardiovascular Disease. J. Urol. 2019, 202, 1199–1208. [Google Scholar] [CrossRef] [PubMed]
- Davey, P.; Kirby, M.G. Cardiovascular risk profiles of GnRH agonists and antagonists: Real-world analysis from UK general practice. World J. Urol. 2021, 39, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Sturgeon, K.M.; Deng, L.; Bluethmann, S.M.; Zhou, S.; Trifiletti, D.M.; Jiang, C.; Kelly, S.P.; Zaorsky, N.G. A population-based study of cardiovascular disease mortality risk in US cancer patients. Eur. Heart J. 2019, 40, 3889–3897. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Epstein, M.M.; Edgren, G.; Rider, J.R.; Mucci, L.A.; Adami, H.O. Temporal trends in cause of death among Swedish and US men with prostate cancer. J. Natl. Cancer Inst. 2012, 104, 1335–1342. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- MacLean, C.M.; Godsafe, Z.; Soto-Forte, P.; Larsen, F. Pharmacokinetic, Safety, and Pharmacodynamic Properties of Teverelix Trifluoroacetate, a Novel Gonadotropin-Releasing Hormone Antagonist, in Healthy Adult Subjects. Clin. Pharmacol. Drug. Dev. 2022, 11, 257–269. [Google Scholar] [CrossRef] [PubMed]
- MacLean, C.; Larsen, F.; Drewe, J.; Ulys, A.; Kaniušas, D. 257 Efficacy and safety of teverelix LA, a new GNRH antagonist in patients with advanced prostate cancer. Results from a Phase II multi-centre, open-label, pilot study investigating an initial. Eur. Urol. Suppl. 2007, 6, 87. [Google Scholar] [CrossRef]
- MacLean, C.; Ulys, A.; Jankevičius, F.; Kaniušas, D.; Drewe, J.; Larsen, F. Efficacy and safety of teverelix, a new gonadotrophin releasing hormone antagonist in patients with advanced prostate cancer. Results from a phase 2 multicentre, open-label, pilot study investigating an initial intramuscular loading dose regimen of teverelix. Eur. Urol. Suppl. 2006, 5, 251. [Google Scholar] [CrossRef]
- MacLean, C.M.; Larsen, F.; Beglinger, C.; Piechatzek, R.; Drewe, J. Safety, Tolerability, Pharmacodynamics and Pharmacokinetics of Teverelix Following Single or Repeated Doses Administered Subcutaneously To Healthy Female Volunteers. Fertil. Steril. 2005, 84, S352–S353. [Google Scholar] [CrossRef]
- Behre, H.M.; Kliesch, S.; Pühse, G.; Reissmann, T.; Nieschlag, E. High loading and low maintenance doses of a gonadotropin-releasing hormone antagonist effectively suppress serum luteinizing hormone, follicle-stimulating hormone, and testosterone in normal men. J. Clin. Endocrinol. Metab. 1997, 82, 1403–1408. [Google Scholar] [CrossRef] [PubMed]
- Tomabal, B.; Raghunath, S.K.; Srivatsa, N.; Nagaraj, V.H. GnRH Antagonist: A New and an Effective Way of Treatment of Advanced Prostate Cancer. Indian J. Surg. Oncol. 2017, 8, 385–388. [Google Scholar] [CrossRef] [PubMed]
- Shore, N.D. Experience with degarelix in the treatment of prostate cancer. Ther. Adv. Urol. 2012, 5, 11–24. [Google Scholar] [CrossRef] [Green Version]
- Klotz, L.; Miller, K.; Crawford, E.D.; Shore, N.; Tombal, B.; Karup, C.; Malmberg, A.; Persson, B.-E. Disease control outcomes from analysis of pooled individual patient data from five comparative randomised clinical trials of Degarelix versus luteinising hormone-releasing hormone agonists. Eur. Urol. 2014, 66, 1101–1108. [Google Scholar] [CrossRef]
- Ye, Y.; Zheng, Y.; Miao, Q.; Ruan, H.; Zhang, X. Causes of death among prostate cancer patients aged 40 years and older in the United States. Front. Oncol. 2022, 12, 914875. [Google Scholar] [CrossRef] [PubMed]
- Gupta, D.; Lee Chuy, K.; Yang, J.C.; Bates, M.; Lombardo, M.; Steingart, R.M. Cardiovascular and metabolic effects of androgen-deprivation therapy for prostate cancer. J. Oncol. Pract. 2018, 14, 580–587. [Google Scholar] [CrossRef] [Green Version]
- Knutsson, A.; Hsiung, S.; Celik, S.; Rattik, S.; Mattisson, I.Y.; Wigren, M.; Scher, H.I.; Nilsson, J.; Hultgårdh-Nilsson, A. Treatment with a gnrh receptor agonist, but not the gnrh receptor antagonist degarelix, induces atherosclerotic plaque instability in ApoE−/− Mice. Sci. Rep. 2016, 6, 26220. [Google Scholar] [CrossRef] [Green Version]
- Zareba, P.; Duivenvoorden, W.; Leong, D.P.; Pinthus, J.H. Androgen deprivation therapy and cardiovascular disease: What is the linking mechanism? Ther. Adv. Urol. 2015, 8, 118–129. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristic | EP-24332T-A013 | EP-24332T-A014 | ARD-0301-003 | ARD-0301-008 | ARD-0301-010 | |
|---|---|---|---|---|---|---|
| Administration (dose, route, schedule); n | 90 mg SC; D0, D1, D2 n = 14 | 90 mg IM; D0, D7; n = 14 | 120 mg SC; D0, D1; n = 8 | 120 (2 × 60) mg SC; D0, D1; n = 8 | 120 (2 × 60) mg SC; D0, D1, D2; n = 18 | 180 (2 × 90) mg SC; D0, D1, D2; n = 20 |
| Age (year), median (range) | 71.5 (62–78) | 74.0 (66–81) | 69.0 (54–74) | 63.5 (58–84) | 70.5 (51–79) | 70.5 (53–78) |
| Weight (kg), mean (SD) | 80.93 (13.27) | 76.14 (12.13) | 86.38 (15.21) | 88.4 (16.7) | 85.7 (14.39) | 82.1 (13.7) |
| BMI (kg/m2), mean (SD) | 27.91 (4.41) | 25.17 (3.60) | 27.96 (3.28) | 28.60 (4.80) | 28.89 (3.69) | 28.13 (4.79) |
| TNM grading, n (%) | ||||||
| T (tumor) | ||||||
| T2 | 1 (7.1) | 1 (7.1) | 0 | 0 | 3 (16.7) | 4 (20) |
| T3 | 13 (92.9) | 13 (92.9) | 8 (100) | 8 (100) | 15 (83.3) | 15 (75) |
| T4 | 0 | 0 | 0 | 0 | 0 | 1 (5) |
| N (nodes) | ||||||
| N0 | 11 (78.6) | 7 (50) | 7 (87.5) | 8 (100) | 12 (66.7) | 12 (60.0) |
| N1 or 2 | 0 | 0 | 1 (12.5) | 0 | 1 (5.6) | 2 (10) |
| Nx | 3 (21.4) | 7 (50) | 0 | 0 | 5 (27.8) | 6 (30) |
| M (metastases) | ||||||
| M0 | 14 (100) | 12 (85.7) | 6 (75.0) | 7 (87.5) | 18 (100) | 14 (70) |
| M1 | 0 | 2 (14.3) | 2 (25.0) | 1 (12.5) | 0 | 4 (20.0) |
| Mx | 0 | 0 | 0 | 0 | 0 | 2 (10.0) |
| Gleason score | ||||||
| <6 | 0 | 0 | 0 | 0 | 5 (27.8) | 6 (30) |
| 6 | 11 (78.6) | 8 (57.1) | 6 (75.0) | 4 (50.0) | 8 (44.4) | 9 (45) |
| 7 | 2 (14.3) | 3 (21.4) | 1 (12.5) | 3 (37.5) | 3 (16.7) | 2 (10) |
| 8 | 1 (7.1) | 2 (14.3) | 1 12.5) | 1 12.5) | 0 | 1 (5) |
| 9 | 0 | 1 (7.1) | 0 | 0 | 2 (11.1) | 2 (10) |
| Outcome | EP-24332T-A013 | EP-24332T-A014 | ARD-0301-003 | ARD-0301-008 | ARD-0301-010 | |
|---|---|---|---|---|---|---|
| Administration (dose, route, schedule); n | 90 mg SC; D0, D1, D2 n = 14 | 90 mg IM; D0, D7; n = 14 | 120 mg SC; D0, D1; n = 8 | 120 (2 × 60) mg SC; D0, D1; n = 8 | 120 (2 × 60) mg SC; D0, D1, D2; n = 18 | 180 (2 × 90) mg SC; D0, D1, D2; n = 20 |
| Mean onset of castration (days) | 1.77 | 2.40 | 1.10 | 1.44 | 1.47 a | 1.42 |
| Mean sustained castration period (days) | 55.32 | 34.77 | 32.45 | 45.85 | 60.00 a | 68.95 |
| Castration period, range (min–max) (weeks) | 4–14 | 3–8 | 0–6 | 0 b–17 | 0–17 | 5–≥21 |
| Castration rate at Day 28: patients with T levels <0.5 ng/mL at Day 28, n (%) | 14 (100%) | 12 (86%) | 5 (63%) | 4 (50%) | 16 (89%) | 19 (95%) |
| Testosterone plasma concentration at Day 28, median (range) (ng/mL) | 0.09 (0.00, 0.47) | 0.14 (0.00, 1.25) | 0.16 (0.09, 0.26) | 0.24 (0.1, 3.48) | 0.20 (0.1, 3.1) | 0.10 (0.1, 2.6) |
| Adverse Event | EP-24332T-A013 | EP-24332T-A014 | ARD-0301-003 | ARD-0301-008 | ARD-0301-010 | Total n = 82 | |
|---|---|---|---|---|---|---|---|
| 90 mg SC; D0, D1, D2 n = 14 | 90 mg IM; D0, D7; n = 14 | 120 mg SC; D0, D1; n = 8 | 120 (2 × 60) mg SC; D0, D1; n = 8 | 120 (2 × 60) mg SC; D0, D1, D2; n = 18 | 180 (2 × 90) mg SC; D0, D1, D2; n = 20 | ||
| # subjects (%) | |||||||
| Any adverse event | 9 (64.3) | 0 | 8 (100) | 8 (100) | 13 (72.2) | 15 (75.0) | 53 (64.6) |
| Serious adverse event | 0 | 0 | 0 | 0 | 1 (5.6) | 0 | 1 (1.2) |
| Adverse events with severe intensity | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Drug-related adverse events | 7 (50.0) | 0 | 8 (100) | 8 (100) | 10 (55.6) | 13 (65.0) | 46 (56.1) |
| Deaths | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| Adverse events in >1 patient in each group in the individual trials | |||||||
| Injection site reaction a | 1 (7.1) | 0 | 8 (100) | 8 (100) | 9 (50) | 12 (60) | 38 (46.3) |
| Flushing/hot flush | 2 (14.3) | 0 | 2 (25.0) | 2 (25.0) | 6 (33.3) | 6 (30.0) | 18 (22.0) |
| Cystitis | 4 (28.6) | 0 | 0 | 0 | 0 | 1 (5.0) | 5 (6.1) |
| Influenza | 0 | 0 | 0 | 0 | 3 (16.7) | 1 (5.0) | 4 (4.9) |
| Urinary retention | 0 | 0 | 0 | 0 | 1 (5.6) | 2 (10) | 3 (3.7) |
| Dysuria | 0 | 0 | 2 (25.0) | 0 | 0 | 0 | 2 (2.4) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MacLean, C.M.; Ulys, A.; Jankevičius, F.; Saladžinskas, Ž.; van Os, S.; Larsen, F. Safety, Pharmacokinetic and Pharmacodynamic Evaluation of Teverelix for the Treatment of Hormone-Sensitive Advanced Prostate Cancer: Phase 2 Loading-Dose-Finding Studies. Medicina 2023, 59, 681. https://doi.org/10.3390/medicina59040681
MacLean CM, Ulys A, Jankevičius F, Saladžinskas Ž, van Os S, Larsen F. Safety, Pharmacokinetic and Pharmacodynamic Evaluation of Teverelix for the Treatment of Hormone-Sensitive Advanced Prostate Cancer: Phase 2 Loading-Dose-Finding Studies. Medicina. 2023; 59(4):681. https://doi.org/10.3390/medicina59040681
Chicago/Turabian StyleMacLean, Carol M., Albertas Ulys, Feliksas Jankevičius, Žilvinas Saladžinskas, Steve van Os, and Finn Larsen. 2023. "Safety, Pharmacokinetic and Pharmacodynamic Evaluation of Teverelix for the Treatment of Hormone-Sensitive Advanced Prostate Cancer: Phase 2 Loading-Dose-Finding Studies" Medicina 59, no. 4: 681. https://doi.org/10.3390/medicina59040681