
Guided Endodontic Surgery: A Narrative Review
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
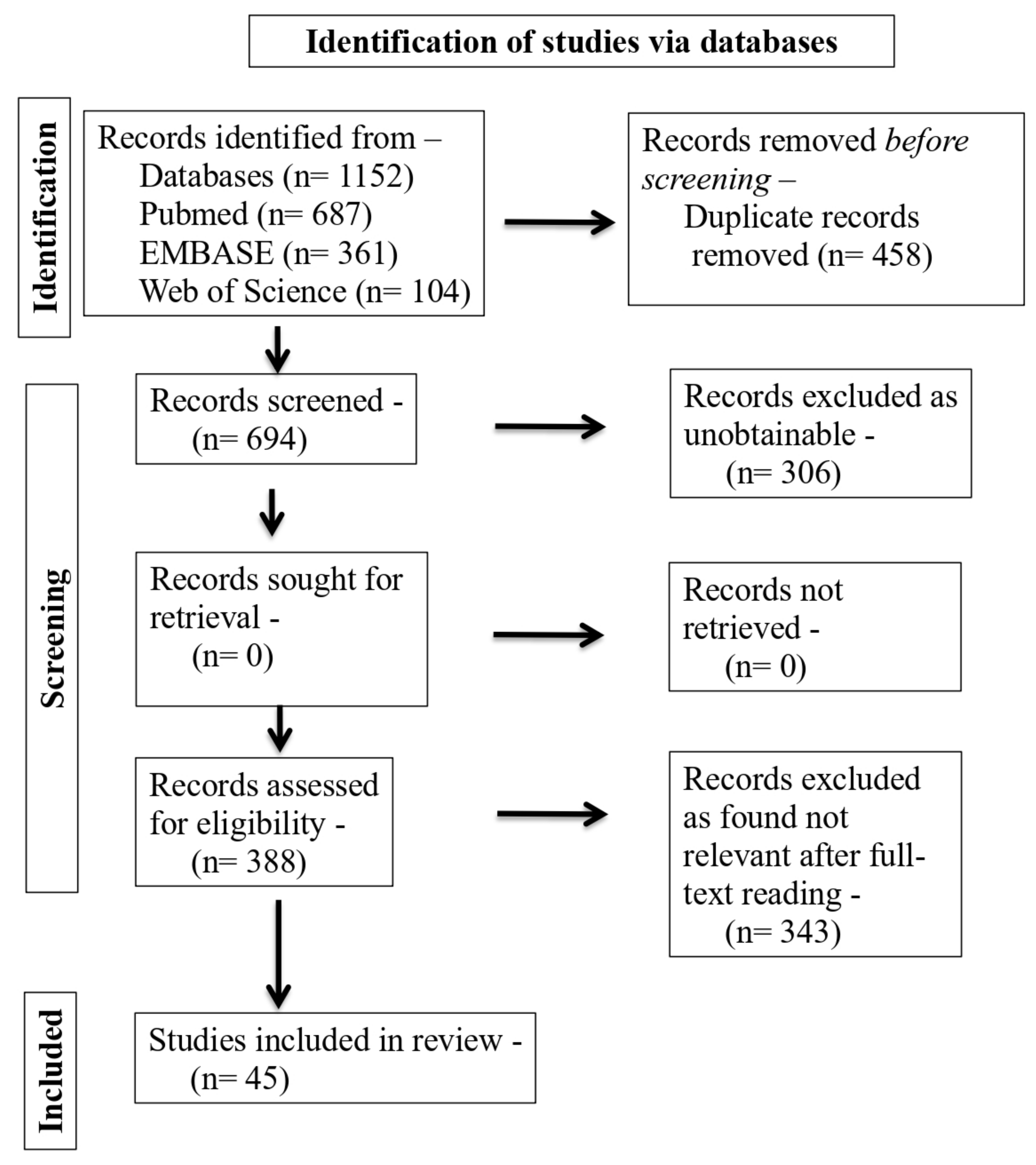
2. Materials and Methods
3. Results

{kind=link}
| Previous Work | GE Research Topic and Classification | Origins and Varieties of Teeth | Operator Characteristics and Skill | Conclusions |
|---|---|---|---|---|
| Gambarini, G., et al., 2020 [38] | Incredibly efficient DC gear from DGE against MAN for AC precision | Type 2.6 R3D Ray Tracing Rendering | Operators fluent in both groups | Less tissue is lost during DGE, decreasing the possibility of iatrogenic coronary weakness. |
| Jain, S.D., et al., 2020 [34] | Root canal attrition in PO teeth (DGE vs. MAN) | Modeled R3D with PO 2.1 and PO 4.1 | One EC (with a microscope for MAN access) | Compared to PO, DGE requires less tissue removal and provides more precise duct location. |
| Loureiro, M.A.Z., et al., 2020 [39] | California’s tooth extraction rate (SGE vs. MAN) | Molars in the mandibular midline and on the jaw’s sides are NAT I features (1st and 2nd jaws). | EC (with magnifying glasses) | SGE helps keep more molar tissue intact. When comparing the amount of tissue extracted from the incisors, there was no discernible difference. |
| Connert, T., et al., 2021 [13] | Root canal attrited teeth wearing down (miniaturized DGE vs. MAN) | Maxillae (both central and lateral) and cheekbones (R3D) in position C | One operator with 12 years of experience | Smaller DGE allows for more precise CA with minimal tissue sacrifice. There was no discernible difference in performance between inexperienced and experienced operators. |
| Koch, G.K., et al., 2022 [40] | Compare 3D printers (for SGE) | R3D All types | One EC |
|
| Buchgreitz, J. et al., 2019 [41] | DGE’s accuracy (teeth with apical periodontitis, teeth requiring post and with PO) |
| -- | DGE is accurate in identifying canals with PO |
| Torres, A., et al., 2021 [32] | Pinpoint accuracy and reliable outcomes (with DGE) |
|
| Incorporating a laser into DGE is a good idea for precisely slicing through sturdy dental tissues. |
| Strbac, G.D., et al., 2021 [42] | Preciseness in attrited canal, disturbances in linear and angular dimension during alternating current (with SGE) | NAT I, C, PM, and M. | -- | SGE accuracy acceptable in AC M has angular and linear dispersion. |
| Meda, R.G., et al., 2022 [43] | Two-AC-Program Accuracy and Effort | It is a R3D model with a simulated PO. | One operator | The milling guide might be quickly planned using any program. Predictability in SGE treatment. PO teeth can safely undergo root canal localization. |
| Choi, Y., et al., 2021 [44] | Guidelines for preventing tooth loss effectively in California (student-oriented) (with SGE) | NAT PM and M | One ES pre-doctoral | In PM, students who employed the AOG-3DP guide saw a 74.9 percent reduction in preparation time, and in M, an 81.1 percent reduction. Methods that follow such advice more conservatively. Design and production take time. Even in more complex situations, the handbook can be used as a resource. |
| Simon, J.C., et al., 2021 [45] | Variation in fracture strength due to method (SGE vs. MAN) SGE’s effectiveness in treating CA with MTAs | NAT PM mandibular | One operator (with magnifiers for MAN) | SGE makes the process of removing MTAs quicker and less prone to mistakes. Increased resistance to tooth breakage is maintained with SGE. |
| Mediavilla Guzmán, A., et al., 2019 [46] | Efficiency and precision while using PO to locate ducts (DGE vs. MAN) | PO with maxillary and mandibular NAT I, C, and PM | One EC One ES | To find ducts with PO, DGE is more precise and effective. |
| Fan, Y., et al., 2019 [47] | Simulated PO for minimally invasive localization of attrited canal and channels (in DGE) | R3D All types | One EC | The average 2D horizontal deviation with DGE and high-velocity drills for canal localization with OP is 0.9 mm, whereas the average 3D deviation is 1.3 mm, and the average 3D angle deviation is 1.7 mm. |
| Smith, B.G., et al., 2019 [48] |
| Using CBCT scans of patients’ first and second maxillary molar teeth | Two EC | A total of 47% of upper first molars and 52% of upper second molars with a 2 mm safety margin can have endodontic surgery. Half of the maxillary first and second molars can be reached without a palate flap. |
| Aldahmash, S.A., et al., 2022 [29] | For OT and AP, the efficacy and precision of DGE (DGE vs. MAN) | For all NATs | One EC (with a microscope for MAN) | DGE improves accuracy over the MAN method. The effectiveness and precision of the MAN method are diminished when the roots are further away from the cortical bone. |
| Authors | Tooth | Previously Used Therapy | Trauma | Problem | EG Subtype | Results |
|---|---|---|---|---|---|---|
| Todd, R., et al., 2021 [6] | 2.1 | No | No | PO | SGE | No symptoms after 24 h |
| Buchgreitz, J. 2019 [12] | 1.6 | Yes | No | PO | SGE | Asymptomatic after two years |
| Torres, A., et al., 2021 [35] | 1.4 | No | No | PO | SGE | Bone healing evident after 12 months |
| Sônia, T.d.O., et al., 2018 [36] | 2.7, 2.8 | No | No | PO | SGE | Complete healing after one year |
| Fonseca, F.O., et al., 2020 [49] | 1.1 | No | Yes | PO | SGE | No symptoms after 12 months. |
| Tavares, W.L.F., et al., 2020 [50] |
| No Yes | Yes | PO | SGE | No symptoms after 12 months. |
| Maia, L.M., et al., 2020 [51] | 4.6 | Yes | No | PO | SGE | No symptoms after 12 months. |
| Freire, B.B., et al., 2021 [52] | 1.1 | No | Yes | PO | SGE | Complete healing after 24 months. |
| Doranala, S., et al., 2020 [53] | 1.1 | No | Yes | PO | DGE | Complete recovery with no symptoms after 12 months |
| Casadei, B.d.A., et al., 2020 [54] | 1.5 | Yes | No | PO | SGE | Complete recovery with no symptoms after 3 months |
| Maia, L.M., et al., 2022 [55] | 2.1 | Yes | Yes | RT | SGE | Healing in 18 months |
| Perez, C. 2020 [56] | 1.6 | Yes | No | RP | SGE | Periapical healing region at 1 year. |
| Strbac, G.D., et al., 2017 [42] | 1.5 | Yes | No | OP | SGE | Healing of periapical tissues after 12 months |
| Giacomino, C.M. 2018 [57] | 1.7 | Yes | No | AP | SGE | Asymptomatic after 12 weeks |
| Popowicz, W. 2019 [58] | 2.5 | Yes | No | OP | SGE | Asymptomatic after 7 months |
| Benjamin, G., et al., 2021 [59] | 2.2 | Yes | No | OT | SGE | Asymptomatic after 10 days. |
| Meda, R.G., et al., 2022 [43] | 2.3 | No | No | AUT | SGE | Bone completely healed after 24 months |
| Gambarini, G., et al., 2019 [60] | 1.2 | Yes | No | AP | SGE | Healing visible at three months with complete healing at 6 months |
| Villa-Machado, P.A., et al., 2022 [61] | 3.1 | Yes | No | OP | SGE | Asymptomatic after 8 weeks |
| Connert, T., et al., 2018 [62] | 4.1 | Yes | No | OP | SGE | Asymptomatic after 12 weeks |
| Torres, A., et al., 2019 [63] | 2.3 | No | Yes | OP | SGE | Periapical healing at 6 months |
| Silva, A.S., et al., 2020 [64] | 2.2 | No | Yes | OP | SGE | Complete healing after one year |
| Santiago, M.C., et al., 2022 [65] | 4.5 | No | No | OP | SGE | Asymptomatic after 6 months |
| Krug, R., et al., 2020 [18] | 3.6 | No | Yes | OP | SGE | An average 3.6-fold reduction in lesion size as measured by optical coherence tomography after one year |
| Kaur, G. 2021 [66] | 2.4 | Yes | No | OP | SGE | Asymptomatic after 2 weeks. |
| Ali, A., et al., 2022 [26] | 2.2 | Yes | Yes | OP | SGE | Complete healing after a year. |
| Pujol, M.L., et al., 2021 [67] | 4.4 | No | Yes | OP | SGE | Asymptomatic after one year |
| Yan, Y.Q., et al., 2021 [68] | 2.1 | No | No | OP | SGE | Asymptomatic after two years |
| Mena-Álvarez, J., et al., 2017 [69] | 2.7 | Yes | No | OP | Dens evaginatus | Asymptomatic after one year |
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bastos, J.V.; Côrtes, M.I.d.S. Pulp canal obliteration after traumatic injuries in permanent teeth–scientific fact or fiction? Braz. Oral Res. 2018, 32, e75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spinas, E.; Deias, M.; Mameli, A.; Giannetti, L. Pulp canal obliteration after extrusive and lateral luxation in young permanent teeth: A scoping review. Eur. J. Paediatr. Dent. 2021, 22, 55–60. [Google Scholar] [PubMed]
- Kulinkovych-Levchuk, K.; Pecci-Lloret, M.P.; Castelo-Baz, P.; Pecci-Lloret, M.R.; Oñate-Sánchez, R.E. Guided Endodontics: A Literature Review. Int. J. Environ. Res. Public Health 2022, 19, 13900. [Google Scholar] [CrossRef] [PubMed]
- Ribeiro, D.; Reis, E.; Marques, J.A.; Falacho, R.I.; Palma, P.J. Guided Endodontics: Static vs. Dynamic Computer-Aided Techniques—A Literature Review. J. Pers. Med. 2022, 12, 1516. [Google Scholar] [CrossRef]
- Acevedo-Mascarúa, A.E.; Torres-Rosas, R.; Pérez-Cervera, Y.; Pérez-Cruz, D.; Ku-Valenzuela, L.Z.; Gijón-Soriano, A.L.; Argueta-Figueroa, L. External Apical Root Resorption in Orthodontic Patients Who Practice Combat Sports: A Case-Control Observational Pilot Study. Medicina 2022, 58, 1342. [Google Scholar] [CrossRef]
- Todd, R.; Resnick, S.; Zicarelli, T.; Linenberg, C.; Donelson, J.; Boyd, C. Template-guided endodontic access. J. Am. Dent. Assoc. 2021, 152, 65–70. [Google Scholar] [CrossRef]
- Vinagre, A.; Castanheira, C.; Messias, A.; Palma, P.J.; Ramos, J.C. Management of Pulp Canal Obliteration—Systematic Review of Case Reports. Medicina 2021, 57, 1237. [Google Scholar] [CrossRef]
- Chaves, G.S.; Capeletti, L.R.; Miguel, J.G.; Loureiro, M.A.Z.; Silva, E.J.; Decurcio, D.A. A Novel Simplified Workflow for Guided Endodontic Surgery in Mandibular Molars with a Thick Buccal Bone Plate: A Case Report. J. Endod. 2022, 48, 930–935. [Google Scholar] [CrossRef]
- Maia, L.M.; de Carvalho Machado, V.; da Silva, N.R.F.A.; Brito, M., Jr.; da Silveira, R.R.; Moreira, G., Jr.; Sobrinho, A.P.R. Case reports in maxillary posterior teeth by guided endodontic access. J. Endod. 2019, 45, 214–218. [Google Scholar] [CrossRef]
- Tavares, W.L.F.; Pedrosa, N.d.O.M.; Moreira, R.A.; Braga, T.; de Carvalho Machado, V.; Sobrinho, A.P.R.; Amaral, R.R. Limitations and management of static-guided endodontics failure. J. Endod. 2022, 48, 273–279. [Google Scholar] [CrossRef]
- Ishak, G.; Habib, M.; Tohme, H.; Patel, S.; Bordone, A.; Perez, C.; Zogheib, C. Guided endodontic treatment of calcified lower incisors: A case report. Dent. J. 2020, 8, 74. [Google Scholar] [CrossRef]
- Buchgreitz, J.; Buchgreitz, M.; Bjørndal, L. Guided endodontics modified for treating molars by using an intracoronal guide technique. J. Endod. 2019, 45, 818–823. [Google Scholar] [CrossRef]
- Connert, T.; Leontiev, W.; Dagassan-Berndt, D.; Kühl, S.; ElAyouti, A.; Krug, R.; Krastl, G.; Weiger, R. Real-time guided endodontics with a miniaturized dynamic navigation system versus conventional freehand endodontic access cavity preparation: Substance loss and procedure time. J. Endod. 2021, 47, 1651–1656. [Google Scholar] [CrossRef]
- Leontiev, W.; Bieri, O.; Madörin, P.; Dagassan-Berndt, D.; Kühl, S.; Krastl, G.; Krug, R.; Weiger, R.; Connert, T. Suitability of magnetic resonance imaging for guided endodontics: Proof of principle. J. Endod. 2021, 47, 954–960. [Google Scholar] [CrossRef]
- Decurcio, D.A.; Bueno, M.R.; Silva, J.A.; Loureiro, M.A.Z.; Damião Sousa-Neto, M.; Estrela, C. Digital Planning on Guided Endodontics Technology. Braz. Dent. J. 2021, 32, 23–33. [Google Scholar] [CrossRef]
- Connert, T.; Krug, R.; Eggmann, F.; Emsermann, I.; ElAyouti, A.; Weiger, R.; Kühl, S.; Krastl, G. Guided endodontics versus conventional access cavity preparation: A comparative study on substance loss using 3-dimensional–printed teeth. J. Endod. 2019, 45, 327–331. [Google Scholar] [CrossRef]
- Connert, T.; Weiger, R.; Krastl, G. Present status and future directions-Guided endodontics. Int. Endod. J. 2022, 10, 995–1002. [Google Scholar] [CrossRef]
- Krug, R.; Volland, J.; Reich, S.; Soliman, S.; Connert, T.; Krastl, G. Guided endodontic treatment of multiple teeth with dentin dysplasia: A case report. Head Face Med. 2020, 16, 27. [Google Scholar] [CrossRef]
- Ackerman, S.; Aguilera, F.C.; Buie, J.M.; Glickman, G.N.; Umorin, M.; Wang, Q.; Jalali, P. Accuracy of 3-dimensional–printed endodontic surgical guide: A human cadaver study. J. Endod. 2019, 45, 615–618. [Google Scholar] [CrossRef]
- Alzate Guerrero, M.A.; Rodriguez Granados, L.X. Descripción de la cirugía endodóntica guiada con navegación estática. Available online: https://repository.usta.edu.co/bitstream/handle/11634/44873/2022AlzateMonica.pdf?sequence=8 (accessed on 13 February 2023).
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [Green Version]
- Torres, P.R.; Madroño, E.C.; Zubizarreta-Macho, Á.; Pérez, M.B.; Catalán, A.G.; de la Vega Buró, S.; Deglow, E.R.; Montero, S.H. Impact of Augmented Reality Technology on Osteotomy Site Preparation for Apical Location: An In Vitro Study. Res. Sq. 2022. [Google Scholar] [CrossRef]
- Jonaityte, E.M.; Bilvinaite, G.; Drukteinis, S.; Torres, A. Accuracy of Dynamic Navigation for Non-Surgical Endodontic Treatment: A Systematic Review. J. Clin. Med. 2022, 11, 3441. [Google Scholar] [CrossRef]
- Gregory, D.F. Computer-guided.endodontics advantages compared to free hand. CBCT (Cone Beam Comput. Tomogr.) 2022, 8. [Google Scholar]
- Chaves, G.S.; Silva, J.A.; Capeletti, L.R.; Silva, E.J.; Estrela, C.; Decurcio, D.A. Guided access cavity preparation using a new simplified digital workflow. J. Endod. 2023, 49, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Ali, A.; Ishaq, A.; Jain, P.; Ali, S. Management of pulp canal obliteration using static-guided endodontic technique: Case series. Saudi Endod. J. 2022, 12, 120. [Google Scholar] [CrossRef]
- Dianat, O.; Nosrat, A.; Tordik, P.A.; Aldahmash, S.A.; Romberg, E.; Price, J.B.; Mostoufi, B. Accuracy and efficiency of a dynamic navigation system for locating calcified canals. J. Endod. 2020, 46, 1719–1725. [Google Scholar] [CrossRef]
- Kostunov, J.; Rammelsberg, P.; Klotz, A.-L.; Zenthöfer, A.; Schwindling, F.S. Minimization of tooth substance removal in normally calcified teeth using guided endodontics: An in vitro pilot study. J. Endod. 2021, 47, 286–290. [Google Scholar] [CrossRef]
- Aldahmash, S.A.; Price, J.B.; Mostoufi, B.; Griffin, I.L.; Dianat, O.; Tordik, P.A.; Martinho, F.C. Real-time 3-dimensional Dynamic Navigation System in Endodontic Microsurgery: A Cadaver Study. J. Endod. 2022, 48, 922–929. [Google Scholar] [CrossRef]
- Janabi, A.; Tordik, P.A.; Griffin, I.L.; Mostoufi, B.; Price, J.B.; Chand, P.; Martinho, F.C. Accuracy and Efficiency of 3-dimensional Dynamic Navigation System for Removal of Fiber Post from Root Canal–Treated Teeth. J. Endod. 2021, 47, 1453–1460. [Google Scholar] [CrossRef]
- Chaudhary, F.A.; Ahmad, B.; Sinor, M.Z. The severity of facial burns, dental caries, periodontal disease, and oral hygiene impact oral health-related quality of life of burns victims in Pakistan: A cross-sectional study. BMC Oral Health 2021, 21, 570. [Google Scholar] [CrossRef]
- Torres, A.; Boelen, G.J.; Lambrechts, P.; Pedano, M.S.; Jacobs, R. Dynamic navigation: A laboratory study on the accuracy and potential use of guided root canal treatment. Int. Endod. J. 2021, 54, 1659–1667. [Google Scholar] [CrossRef]
- Krug, R.; Reich, S.; Connert, T.; Kess, S.; Soliman, S.; Reymus, M.; Krastl, G. Guided endodontics: A comparative in vitro study on the accuracy and effort of two different planning workflows. Int. J. Comput. Dent 2020, 23, 119–128. [Google Scholar]
- Jain, S.D.; Carrico, C.K.; Bermanis, I. 3-Dimensional accuracy of dynamic navigation technology in locating calcified canals. J. Endod. 2020, 46, 839–845. [Google Scholar] [CrossRef]
- Torres, A.; Lerut, K.; Lambrechts, P.; Jacobs, R. Guided endodontics: Use of a sleeveless guide system on an upper premolar with pulp canal obliteration and apical periodontitis. J. Endod. 2021, 47, 133–139. [Google Scholar] [CrossRef]
- Sônia, T.d.O.; Camila de Freitas, M.B.; Santa-Rosa, C.C.; Machado, V.C. Guided endodontic access in maxillary molars using cone-beam computed tomography and computer-aided design/computer-aided manufacturing system: A case report. J. Endod. 2018, 44, 875–879. [Google Scholar]
- Lara-Mendes, S.T.; Camila de Freitas, M.B.; Machado, V.C.; Santa-Rosa, C.C. A new approach for minimally invasive access to severely calcified anterior teeth using the guided endodontics technique. J. Endod. 2018, 44, 1578–1582. [Google Scholar] [CrossRef]
- Gambarini, G.; Galli, M.; Morese, A.; Stefanelli, L.V.; Abduljabbar, F.; Giovarruscio, M.; Di Nardo, D.; Seracchiani, M.; Testarelli, L. Precision of dynamic navigation to perform endodontic ultraconservative access cavities: A preliminary in vitro analysis. J. Endod. 2020, 46, 1286–1290. [Google Scholar] [CrossRef]
- Loureiro, M.A.Z.; Elias, M.R.; Capeletti, L.R.; Silva, J.A.; Siqueira, P.C.; Chaves, G.S.; Decurcio, D.A. Guided Endodontics: Volume of Dental Tissue Removed by Guided Access Cavity Preparation—An Ex Vivo Study. J. Endod. 2020, 46, 1907–1912. [Google Scholar] [CrossRef]
- Koch, G.K.; Gharib, H.; Liao, P.; Liu, H. Guided Access Cavity Preparation Using Cost-Effective 3D Printers. J. Endod. 2022, 48, 909–913. [Google Scholar] [CrossRef]
- Buchgreitz, J.; Buchgreitz, M.; Bjørndal, L. Guided root canal preparation using cone beam computed tomography and optical surface scans–an observational study of pulp space obliteration and drill path depth in 50 patients. Int. Endod. J. 2019, 52, 559–568. [Google Scholar] [CrossRef]
- Strbac, G.D.; Schnappauf, A.; Giannis, K.; Moritz, A.; Ulm, C. Guided modern endodontic surgery: A novel approach for guided osteotomy and root resection. J. Endod. 2017, 43, 496–501. [Google Scholar] [CrossRef] [PubMed]
- Meda, R.G.; Sans, F.A.; Esquivel, J.; Zufía, J. Impacted maxillary canine with curved apex: Three-dimensional guided protocol for autotransplantation. J. Endod. 2022, 48, 379–387. [Google Scholar] [CrossRef]
- Choi, Y.; Jeon, W.S.; Cho, J.M.; Jeong, H.G.; Shin, Y.; Park, W. Access opening guide produced using a 3D printer (AOG-3DP) as an effective tool in difficult cases for dental students. J. Dent. Educ. 2021, 85, 1640–1645. [Google Scholar] [CrossRef] [PubMed]
- Simon, J.C.; Kwok, J.W.; Vinculado, F.; Fried, D. Computer-Controlled CO2 Laser Ablation System for Cone-beam Computed Tomography and Digital Image Guided Endodontic Access: A Pilot Study. J. Endod. 2021, 47, 1445–1452. [Google Scholar] [CrossRef] [PubMed]
- Mediavilla Guzmán, A.; Riad Deglow, E.; Zubizarreta-Macho, Á.; Agustín-Panadero, R.; Hernández Montero, S. Accuracy of computer-aided dynamic navigation compared to computer-aided static navigation for dental implant placement: An in vitro study. J. Clin. Med. 2019, 8, 2123. [Google Scholar] [CrossRef] [Green Version]
- Fan, Y.; Glickman, G.N.; Umorin, M.; Nair, M.K.; Jalali, P. A novel prefabricated grid for guided endodontic microsurgery. J. Endod. 2019, 45, 606–610. [Google Scholar] [CrossRef]
- Smith, B.G.; Pratt, A.M.; Anderson, J.A.; Ray, J.J. Targeted endodontic microsurgery: Implications of the greater palatine artery. J. Endod. 2021, 47, 19–27. [Google Scholar] [CrossRef]
- Fonseca, F.O.; Vasconcellos, B.d.L.C.; Costa, M.M.; Sobrinho, A.P.R.; Tavares, W.L.F. Combined endodontic and surgical therapy for resolution of type III dens invaginatus. Iran. Endod. J. 2020, 15, 117–123. [Google Scholar]
- Tavares, W.L.F.; Fonseca, F.O.; Machado, V.; Vasconcellos, B.d.L.C.; Guimarães, L.C.; Viana, A.C.D.; Henriques, L.C.F. Guided endodontics in complex scenarios of calcified molars. Iran. Endod. J. 2020, 15, 50–56. [Google Scholar]
- Maia, L.M.; Toubes, K.M.; Moreira, G., Jr.; Tonelli, S.Q.; de Carvalho Machado, V.; Silveira, F.F.; Nunes, E. Guided endodontics in nonsurgical retreatment of a mandibular first molar: A new approach and case report. Iran. Endod. J. 2020, 15, 111–116. [Google Scholar]
- Freire, B.B.; Vianna, S.; Nascimento, E.H.L.; Freire, M.; Chilvarquer, I. Guided Endodontic Access in a Calcified Central Incisor: A Conservative Alternative for Endodontic Therapy. Iran. Endod. J. 2021, 16, 56–59. [Google Scholar]
- Doranala, S.; Vemisetty, H.; Punna, R.; Alwala, A.M. Endodontic management of canal calcification in maxillary central incisor using 3d prototyping technique: A case report. J. Adv. Oral Res. 2020, 11, 93–96. [Google Scholar] [CrossRef]
- Casadei, B.d.A.; Lara-Mendes, S.T.d.O.; Barbosa, C.d.F.M.; Araújo, C.V.; de Freitas, C.A.; Machado, V.C.; Santa-Rosa, C.C. Access to original canal trajectory after deviation and perforation with guided endodontic assistance. Aust. Endod. J. 2020, 46, 101–106. [Google Scholar] [CrossRef]
- Maia, L.M.; Bambirra, W., Jr.; Toubes, K.M.; Moreira, G., Jr.; de Carvalho Machado, V.; Parpinelli, B.C.; Sobrinho, A.P.R. Endodontic guide for the conservative removal of a fiber-reinforced composite resin post. J. Prosthet. Dent. 2022, 128, 4–7. [Google Scholar] [CrossRef]
- Perez, C.; Finelle, G.; Couvrechel, C. Optimisation of a guided endodontics protocol for removal of fibre-reinforced posts. Aust. Endod. J. 2020, 46, 107–114. [Google Scholar] [CrossRef]
- Giacomino, C.M.; Ray, J.J.; Wealleans, J.A. Targeted endodontic microsurgery: A novel approach to anatomically challenging scenarios using 3-dimensional–printed guides and trephine burs—A report of 3 cases. J. Endod. 2018, 44, 671–677. [Google Scholar] [CrossRef] [Green Version]
- Popowicz, W.; Palatyńska-Ulatowska, A.; Kohli, M.R. Targeted endodontic microsurgery: Computed tomography–based guided stent approach with platelet-rich fibrin graft: A report of 2 cases. J. Endod. 2019, 45, 1535–1542. [Google Scholar] [CrossRef]
- Benjamin, G.; Ather, A.; Bueno, M.R.; Estrela, C.; Diogenes, A. Preserving the neurovascular bundle in targeted endodontic microsurgery: A case series. J. Endod. 2021, 47, 509–519. [Google Scholar] [CrossRef]
- Gambarini, G.; Galli, M.; Stefanelli, L.V.; Di Nardo, D.; Morese, A.; Seracchiani, M.; De Angelis, F.; Di Carlo, S.; Testarelli, L. Endodontic microsurgery using dynamic navigation system: A case report. J. Endod. 2019, 45, 1397–1402.e1396. [Google Scholar] [CrossRef]
- Villa-Machado, P.A.; Restrepo-Restrepo, F.A.; Sousa-Dias, H.; Tobón-Arroyave, S.I. Application of computer-assisted dynamic navigation in complex root canal treatments: Report of two cases of calcified canals. Aust. Endod. J. 2022, 48, 187–196. [Google Scholar] [CrossRef]
- Connert, T.; Zehnder, M.; Amato, M.; Weiger, R.; Kühl, S.; Krastl, G. Microguided Endodontics: A method to achieve minimally invasive access cavity preparation and root canal location in mandibular incisors using a novel computer-guided technique. Int. Endod. J. 2018, 51, 247–255. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Shaheen, E.; Lambrechts, P.; Politis, C.; Jacobs, R. Microguided Endodontics: A case report of a maxillary lateral incisor with pulp canal obliteration and apical periodontitis. Int. Endod. J. 2019, 52, 540–549. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.S.; Carvalho Santos, A.C.; de Sousa Caneschi, C.; Machado, V.C.; Moreira, A.N.; dos Santos Alves Morgan, L.F.; Tavares, W.L.F. Adaptable fiberglass post after 3D guided endodontic treatment: Novel approaches in restorative dentistry. J. Esthet. Restor. Dent. 2020, 32, 364–370. [Google Scholar] [CrossRef] [PubMed]
- Santiago, M.C.; Altoe, M.M.; de Azevedo Mohamed, C.P.; de Oliveira, L.A.; Salles, L.P. Guided endodontic treatment in a region of limited mouth opening: A case report of mandibular molar mesial root canals with dystrophic calcification. BMC Oral Health 2022, 22, 37. [Google Scholar] [CrossRef]
- Kaur, G.; Venkatesh, K.V.; Sihivahanan, D. Microguided endodontics: A case report of conservative approach for the management of calcified maxillary lateral incisors. Saudi Endod. J. 2021, 11, 266. [Google Scholar]
- Pujol, M.L.; Vidal, C.; Mercadé, M.; Muñoz, M.; Ortolani-Seltenerich, S. Guided endodontics for managing severely calcified canals. J. Endod. 2021, 47, 315–321. [Google Scholar] [CrossRef]
- Yan, Y.-Q.; Wang, H.-L.; Liu, Y.; Zheng, T.-J.; Tang, Y.-P.; Liu, R. Three-dimensional inlay-guided endodontics applied in variant root canals: A case report and review of literature. World J. Clin. Cases 2021, 9, 11425. [Google Scholar] [CrossRef]
- Mena-Álvarez, J.; Rico-Romano, C.; Lobo-Galindo, A.B.; Zubizarreta-Macho, Á. Endodontic treatment of dens evaginatus by performing a splint guided access cavity. J. Esthet. Restor. Dent. 2017, 29, 396–402. [Google Scholar] [CrossRef]
- Ali, A.; Arslan, H.; Jethani, B. Conservative management of Type II dens invaginatus with guided endodontic approach: A case series. J. Conserv. Dent. JCD 2019, 22, 503. [Google Scholar] [CrossRef]
- Jain, S.D.; Saunders, M.W.; Carrico, C.K.; Jadhav, A.; Deeb, J.G.; Myers, G.L. Dynamically navigated versus freehand access cavity preparation: A comparative study on substance loss using simulated calcified canals. J. Endod. 2020, 46, 1745–1751. [Google Scholar] [CrossRef]
- Chaudhary, F.A.; Ahmad, B.; Butt, D.Q.; Hameed, S.; Bashir, U. Normal range of maximum mouth opening in pakistani population: A cross-sectional study. J. Int. Oral Health 2019, 11, 353. [Google Scholar] [CrossRef]
- Reeh, E.S.; Messer, H.H.; Douglas, W.H. Reduction in tooth stiffness as a result of endodontic and restorative procedures. J. Endod. 1989, 15, 512–516. [Google Scholar] [CrossRef]
- Shabbir, J.; Zehra, T.; Najmi, N.; Hasan, A.; Naz, M.; Piasecki, L.; Azim, A.A. Access cavity preparations: Classification and literature review of traditional and minimally invasive endodontic access cavity designs. J. Endod. 2021, 47, 1229–1244. [Google Scholar] [CrossRef]
- Ballester, B.; Giraud, T.; Ahmed, H.M.A.; Nabhan, M.S.; Bukiet, F.; Guivarc’h, M. Current strategies for conservative endodontic access cavity preparation techniques—Systematic review, meta-analysis, and decision-making protocol. Clin. Oral Investig. 2021, 25, 6027–6044. [Google Scholar] [CrossRef]
- Chaudhary, F.A.; Ahmad, B.; Javed, M.Q.; Yakub, S.S.; Arjumand, B.; Khan, A.M.; Mustafa, S. The Relationship of Orofacial Pain and Dental Health Status and Oral Health Behaviours in Facial Burn Patients. Pain Res. Manag. 2021, 2021, 5512755. [Google Scholar] [CrossRef]
- Gaffuri, S.; Audino, E.; Salvadori, M.; Garo, M.L.; Salgarello, S. Accuracy of a minimally invasive surgical guide in microsurgical endodontics: A human cadaver study. G. Ital. Di Endod. 2021, 35, 30–36. [Google Scholar]
- Buniag, A.G.; Pratt, A.M.; Ray, J.J. Targeted endodontic microsurgery: A retrospective outcomes assessment of 24 cases. J. Endod. 2021, 47, 762–769. [Google Scholar] [CrossRef]
- Jayaraj, A.; Jayakrishnan, S.; Shetty, K.P.; Nillan, K.; Shetty, R.R.; Govind, S. 3D printing in dentistry: A new dimension of vision. Int. J. Appl. Dent. Sci. 2019, 5, 165–169. [Google Scholar]
- Bergenholtz, G.; Spångberg, L. Controversies in endodontics. Crit. Rev. Oral Biol. Med. 2004, 15, 99–114. [Google Scholar] [CrossRef] [Green Version]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iqbal, A.; Sharari, T.A.; Khattak, O.; Chaudhry, F.A.; Bader, A.K.; Saleem, M.M.; Issrani, R.; Almaktoom, I.T.; Albalawi, R.F.H.; Alserhani, E.D.M. Guided Endodontic Surgery: A Narrative Review. Medicina 2023, 59, 678. https://doi.org/10.3390/medicina59040678
Iqbal A, Sharari TA, Khattak O, Chaudhry FA, Bader AK, Saleem MM, Issrani R, Almaktoom IT, Albalawi RFH, Alserhani EDM. Guided Endodontic Surgery: A Narrative Review. Medicina. 2023; 59(4):678. https://doi.org/10.3390/medicina59040678
Chicago/Turabian StyleIqbal, Azhar, Thani Al Sharari, Osama Khattak, Farooq Ahmad Chaudhry, Alzarea K. Bader, Muhammad Mudassar Saleem, Rakhi Issrani, Ibrahem T. Almaktoom, Raghad Fayez H. Albalawi, and Ebtehal Dhyab M. Alserhani. 2023. "Guided Endodontic Surgery: A Narrative Review" Medicina 59, no. 4: 678. https://doi.org/10.3390/medicina59040678