
Gingival Orofacial Granulomatosis Clinical and 2D/3D Microscopy Features after Orthodontic Therapy: A Pediatric Case Report
 ,
,  , , , and
, , , and 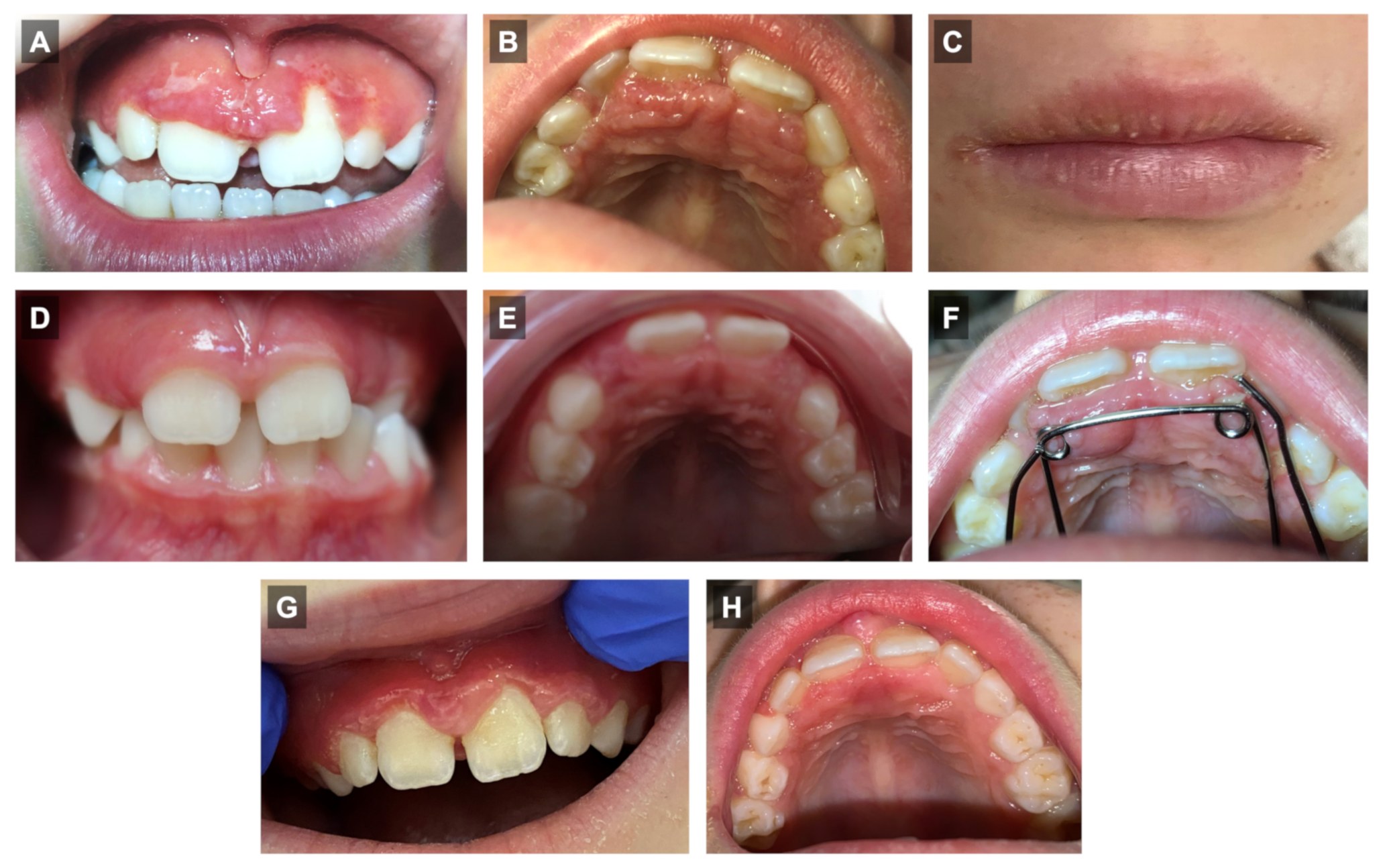{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Case Report
2.1. Clinical Features
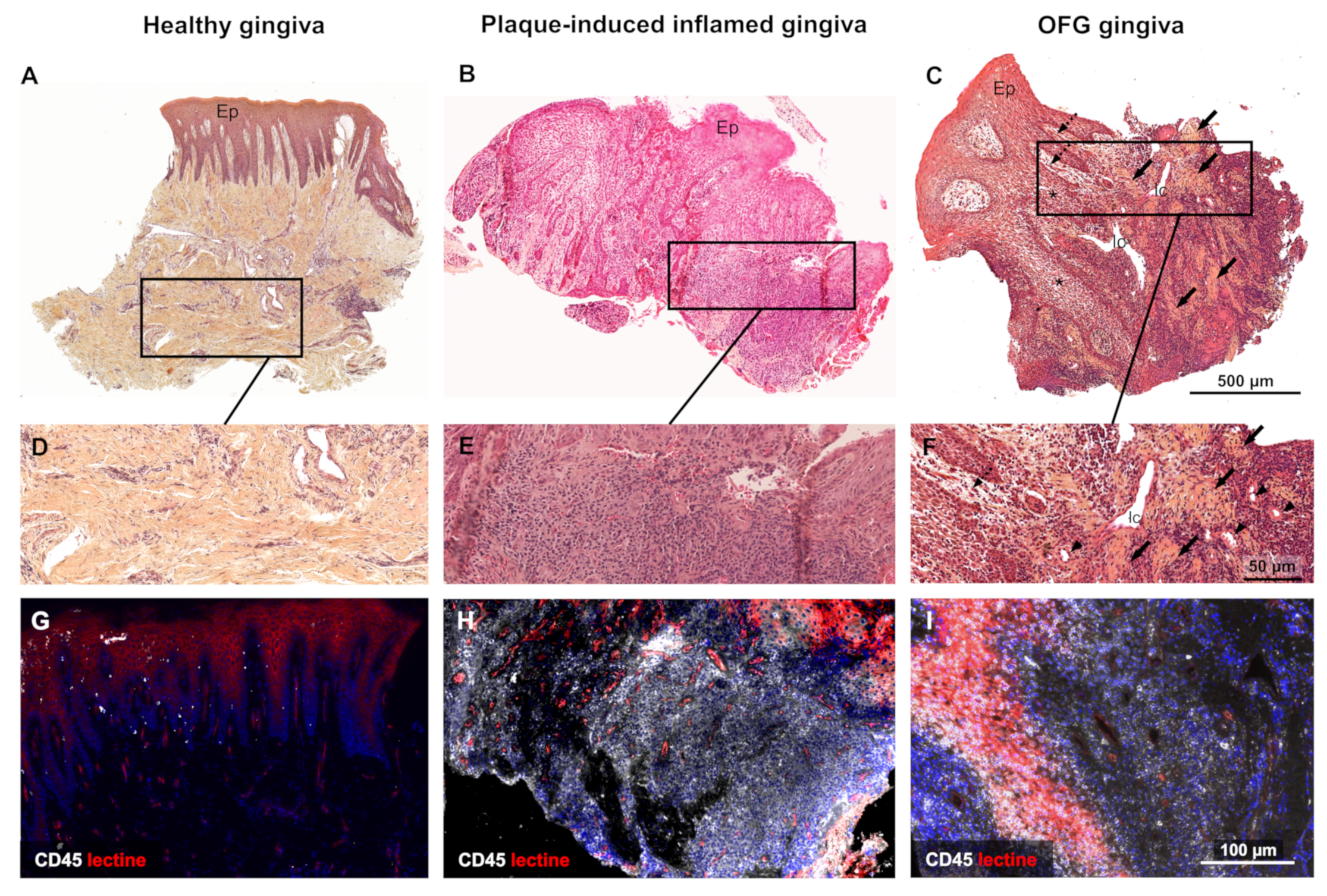
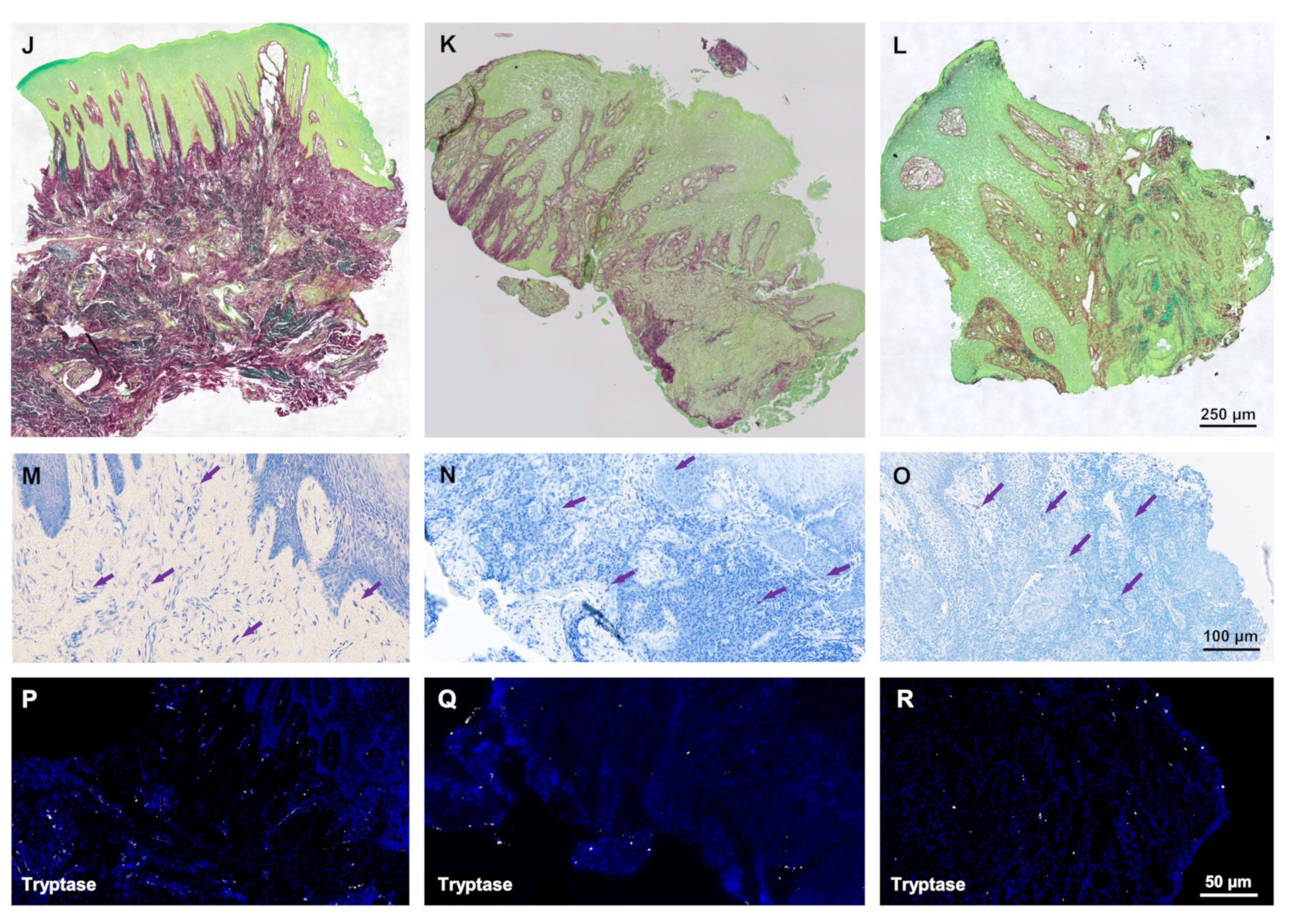
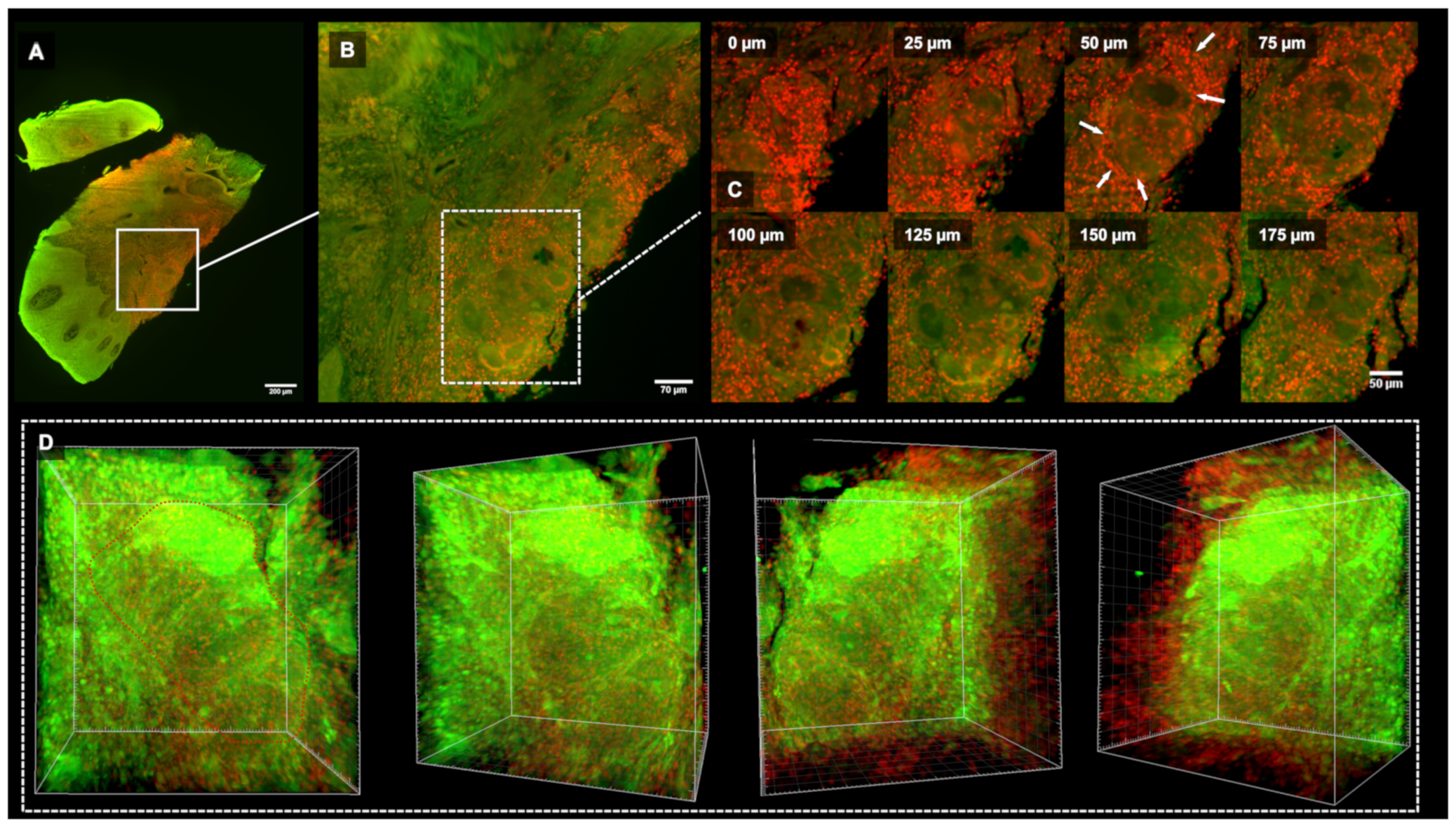
2.2. Histopathology and 3D Microscopy Analysis
3. Discussion
4. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ASCA | anti-Saccharomyces cerevicae IgG auto-antibody |
| CD | Crohn’s disease |
| ECM | Extra-Cellular Matrix |
| OFG | Orofacial granulomatosis |
References
- Atkin, P.A.; Simms, M.L. Orofacial granulomatosis: An unsuccessful response to weekly azithromycin pulse therapy. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 125, e83–e85. [Google Scholar] [CrossRef]
- Hullah, E.A.; Escudier, M.P. The mouth in inflammatory bowel disease and aspects of orofacial granulomatosis. Periodontology 2000 2019, 80, 61–76. [Google Scholar] [CrossRef] [PubMed]
- Honigman, A.D.; Kim, M.; Chow, C.; Robertson, S.J. Orofacial Granulomatosis Presenting With Acquired Lymphangiectasia. JAMA Dermatol. 2019, 155, 1320. [Google Scholar] [CrossRef] [PubMed]
- Razdan, R.; Newby, M.D.; Carr, M.M. Orofacial Granulomatosis in a Child. Case Rep. Pediatr. 2019, 2019, 7519267. [Google Scholar] [CrossRef] [Green Version]
- Espinoza, I.; Navarrete, J.; Benedetto, J.; Borzutzky, A.; Roessler, P.; Ortega-Pinto, A. Orofacial granulomatosis and diet therapy: A review of the literature and two clinical cases. An. Bras. Dermatol. 2018, 93, 80–85. [Google Scholar] [CrossRef] [PubMed]
- Georgesen, C.; Huang, J.; Avarbock, A.; Harp, J.; Magro, C. Orofacial granulomatosis and erythema multiforme in an adolescent with Crohn’s disease. Pediatr. Dermatol. 2018, 35, e294–e297. [Google Scholar] [CrossRef]
- Gavioli, C.F.B.; Florezi, G.P.; Dabronzo, M.L.D.; Jiménez, M.R.; Nico, M.M.S.; Lourenço, S.V. Orofacial Granulomatosis and Crohn Disease: Coincidence or Pattern? A Systematic Review. Dermatology 2021, 237, 635–640. [Google Scholar] [CrossRef]
- McCartan, B.E.; Healy, C.M.; McCreary, C.E.; Flint, S.R.; Rogers, S.; Toner, M.E. Characteristics of patients with orofacial granulomatosis. Oral Dis. 2011, 17, 696–704. [Google Scholar] [CrossRef]
- Gavioli, C.F.B.; Florezi, G.P.; Lourenço, S.V.; Nico, M.M.S. Clinical Profile of Melkersson-Rosenthal Syndrome/Orofacial Granulomatosis: A Review of 51 Patients. J. Cutan. Med. Surg. 2021, 25, 390–396. [Google Scholar] [CrossRef]
- Al-Hamad, A.; Porter, S.; Fedele, S. Orofacial Granulomatosis. Dermatol. Clin. 2015, 33, 433–446. [Google Scholar] [CrossRef]
- Patel, P.; Brostoff, J.; Campbell, H.; Goel, R.M.; Taylor, K.; Ray, S.; Lomer, M.; Escudier, M.; Challacombe, S.; Spencer, J.; et al. Clinical evidence for allergy in orofacial granulomatosis and inflammatory bowel disease. Clin. Transl. Allergy 2013, 3, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Thomas, T.K.; Neelakandan, R.S.; Bhargava, D.; Deshpande, A. Orofacial granulomatosis: A clinicopathologic correlation. Head Neck Pathol. 2011, 5, 133–136. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shetty, N.; Subramanyam, R.V.; Srikanth, G.; Solomon, M.C. Orofacial granulomatosis: A case report and a proposal of a diagnostic algorithm for oral granulomatous lesions. J. Oral Maxillofac. Pathol. 2021, 25, 5. [Google Scholar]
- Sciubba, J.J.; Said-Al-Naief, N. Orofacial granulomatosis: Presentation, pathology and management of 13 cases: Orofacial granulomatosis. J. Oral Pathol. Med. 2003, 32, 576–585. [Google Scholar] [CrossRef] [PubMed]
- Wehl, G.; Rauchenzauner, M. A Systematic Review of the Literature of the Three Related Disease Entities Cheilitis Granulomatosa, Orofacial Granulomatosis and Melkersson–Rosenthal Syndrome. Curr. Pediatr. Rev. 2018, 14, 196–203. [Google Scholar] [CrossRef]
- Courtney, A.; Holmes, Z.; Sharma, S.; Brand, R. Orofacial granulomatosis: Challenges in diagnosis and treatment. J. Paediatr. Child Health 2022. [Google Scholar] [CrossRef]
- Goel, R.M.; Prosdocimi, E.M.; Amar, A.; Omar, Y.; Escudier, M.P.; Sanderson, J.D.; Wade, W.G.; Prescott, N.J. Streptococcus Salivarius: A Potential Salivary Biomarker for Orofacial Granulomatosis and Crohn’s Disease? Inflamm. Bowel Dis. 2019, 25, 1367–1374. [Google Scholar] [CrossRef] [Green Version]
- Patton, D.W.; Ferguson, M.M.; Forsyth, A.; James, J. Oro-facial granulomatosis: A possible allergic basis. Br. J. Oral Maxillofac. Surg. 1985, 23, 235–242. [Google Scholar] [CrossRef]
- Rees, T.D. Orofacial granulomatosis and related conditions. Periodontology 2000 1999, 21, 145–157. [Google Scholar] [CrossRef]
- Ravindran, R.; Karunakaran, A. Idiopathic Orofacial Granulomatosis with Varied Clinical Presentation. Case Rep. Dent. 2013, 2013, 701749. [Google Scholar] [CrossRef] [Green Version]
- Tilakaratne, W.M.; Freysdottir, J.; Fortune, F. Orofacial granulomatosis: Review on aetiology and pathogenesis. J. Oral Pathol. Med. 2007, 37, 191. [Google Scholar] [CrossRef] [PubMed]
- Wei, M.; Xie, C.; Liu, Y.; Wang, Y.; Wang, Y.; Wang, X.; Liu, Y. Characterizing disease manifestations and treatment outcomes among patients with orofacial granulomatosis in China. JAAD Int. 2020, 1, 126–134. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Wang, J.; Yu, X.; Wang, W. Orofacial granulomatosis. Medicine 2017, 96, e8102. [Google Scholar] [CrossRef]
- Guttman-Yassky, E.; Weltfriend, S.; Bergman, R. Resolution of orofacial granulomatosis with amalgam removal. J. Eur. Acad. Dermatol. Venereol. JEADV 2003, 17, 344–347. [Google Scholar] [CrossRef] [PubMed]
- Lazarov, A.; Kidron, D.; Tulchinsky, Z.; Minkow, B. Contact orofacial granulomatosis caused by delayed hypersensitivity to gold and mercury. J. Am. Acad. Dermatol. 2003, 49, 1117–1120. [Google Scholar] [CrossRef] [PubMed]
- Tomka, M.; Machovcová, A.; Pelclová, D.; Petanová, J.; Arenbergerová, M.; Procházková, J. Orofacial granulomatosis associated with hypersensitivity to dental amalgam. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2003, 112, 335–341. [Google Scholar] [CrossRef]
- King, S.; Chow, C.K.; Eberhard, J. Oral health and cardiometabolic disease: Understanding the relationship. Intern. Med. J. 2022, 52, 198–205. [Google Scholar] [CrossRef]
- Matsudate, Y.; Yamashita, M.; Fujii, Y.; Urano, Y. Contact granulomatous hypersensitivity to indium in a patient with orofacial granulomatosis. Contact Dermat. 2019, 81, 293–294. [Google Scholar] [CrossRef]
- White, A.; Nunes, C.; Escudier, M.; Lomer, M.C.E.; Barnard, K.; Shirlaw, P.; Challacombe, S.J.; Sanderson, J.D. Improvement in orofacial granulomatosis on a cinnamon- and benzoate-free diet. Inflamm. Bowel Dis. 2006, 12, 508–514. [Google Scholar] [CrossRef] [Green Version]
- Campbell, H.E.; Escudier, M.P.; Patel, P.; Challacombe, S.J.; Sanderson, J.D.; Lomer, M.C.E. Review article: Cinnamon- and benzoate-free diet as a primary treatment for orofacial granulomatosis. Aliment. Pharmacol. Ther. 2011, 34, 687–701. [Google Scholar] [CrossRef]
- Merigo, E.; Fornaini, C.; Manfredi, M.; Meleti, M.; Alberici, F.; Corcione, L.; Buzio, C.; Rocca, J.P.; Ferri, T.; Vescovi, P. Orofacial granulomatosis treated with low-level laser therapy: A case report. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2012, 113, e25–e29. [Google Scholar] [CrossRef] [PubMed]
- Silva, A.M.B.; Costa, A.A.S.D.; Dias, J.D.P.R.; Cruz, A.F.; Mesquita, R.A.D.; Resende, R.G.; Lacerda, J.C.T. Orofacial Granulomatosis Treated with Corticosteroid and Laser-Therapy: Report of a Case. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2018, 126, e123. [Google Scholar] [CrossRef]
- Campbell, H.; Escudier, M.P.; Brostoff, J.; Patel, P.; Milligan, P.; Challacombe, S.J.; Sanderson, J.D.; Lomer, M.C.E. Dietary intervention for oral allergy syndrome as a treatment in orofacial granulomatosis: A new approach? J. Oral Pathol. Med. Off. Publ. Int. Assoc. Oral Pathol. Am. Acad. Oral Pathol. 2013, 42, 517–522. [Google Scholar] [CrossRef]
- Hoekman, D.R.; Roelofs, J.J.T.H.; van Schuppen, J.; Schonenberg-Meinema, D.; D’Haens, G.R.; Benninga, M.A. Case report of cheilitis granulomatosa and joint complaints as presentation of Crohn’s disease. Clin. J. Gastroenterol. 2016, 9, 73–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sachdeva, S.; Raina, A.; Sardana, K.; Malhotra, P. A case of orofacial granulomatosis evolving into Melkersson Rosenthal syndrome in a child treated with a steroid free regimen of Clofazimine and Minocycline. Dermatol. Ther. 2021, 34. [Google Scholar] [CrossRef]
- Galdiero, M.R.; Maio, F.; Arcoleo, F.; Boni, E.; Bonzano, L.; Brussino, L.; Cancian, M.; Cremonte, L.; Del Giacco, S.R.; De Paulis, A.; et al. Orofacial granulomatosis: Clinical and therapeutic features in an Italian cohort and review of the literature. Allergy 2021, 76, 2189–2200. [Google Scholar] [CrossRef] [PubMed]
- Al-Abeedi, F.; Aldahish, Y.; Almotawa, Z.; Kujan, O. The Differential Diagnosis of Desquamative Gingivitis: Review of the Literature and Clinical Guide for Dental Undergraduates. J. Int. Oral Heal. JIOH 2015, 7, 88–92. [Google Scholar]
- Lazzerini, M.; Martelossi, S.; Cont, G.; Bersanini, C.; Ventura, G.; Fontana, M.; Zuin, G.; Ventura, A.; Taddio, A. Orofacial granulomatosis in children: Think about Crohn’s disease. Dig. Liver Dis. 2015, 47, 338–341. [Google Scholar] [CrossRef]
- Simonsen, A.B.; Deleuran, M. Orofacial Granulomatosis in Children can be the Initial Manifestation of Systemic Disease: A Presentation of Two Cases. Dermatol. Rep. 2014, 6, 5039. [Google Scholar] [CrossRef] [Green Version]
- Marcoval, J.; Penín, R. Histopathological Features of Orofacial Granulomatosis. Am. J. Dermatopathol. 2016, 38, 194–200. [Google Scholar] [CrossRef]
- Mehta, A.; Dalziel, K.; David, G. Gold allergy as a cause of orofacial granulomatosis. J. Am. Acad. Dermatol. 2005, 52, 78. [Google Scholar]
- Ulhaq, A.; Tidbury, K. Orofacial Granulomatosis in an Orthodontic Patient: A Case Report. Orthod. Update 2019, 12, 25–28. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cecchin-Albertoni, C.; Pieruccioni, L.; Canceill, T.; Benetah, R.; Chaumont, J.; Guissard, C.; Monsarrat, P.; Kémoun, P.; Marty, M. Gingival Orofacial Granulomatosis Clinical and 2D/3D Microscopy Features after Orthodontic Therapy: A Pediatric Case Report. Medicina 2023, 59, 673. https://doi.org/10.3390/medicina59040673
Cecchin-Albertoni C, Pieruccioni L, Canceill T, Benetah R, Chaumont J, Guissard C, Monsarrat P, Kémoun P, Marty M. Gingival Orofacial Granulomatosis Clinical and 2D/3D Microscopy Features after Orthodontic Therapy: A Pediatric Case Report. Medicina. 2023; 59(4):673. https://doi.org/10.3390/medicina59040673
Chicago/Turabian StyleCecchin-Albertoni, Chiara, Laetitia Pieruccioni, Thibault Canceill, Robin Benetah, Jade Chaumont, Christophe Guissard, Paul Monsarrat, Philippe Kémoun, and Mathieu Marty. 2023. "Gingival Orofacial Granulomatosis Clinical and 2D/3D Microscopy Features after Orthodontic Therapy: A Pediatric Case Report" Medicina 59, no. 4: 673. https://doi.org/10.3390/medicina59040673