
Gaucher: A Systematic Review on Oral and Radiological Aspects
 , ,
, ,  , ,
, ,  and
and 
Abstract
:1. Introduction
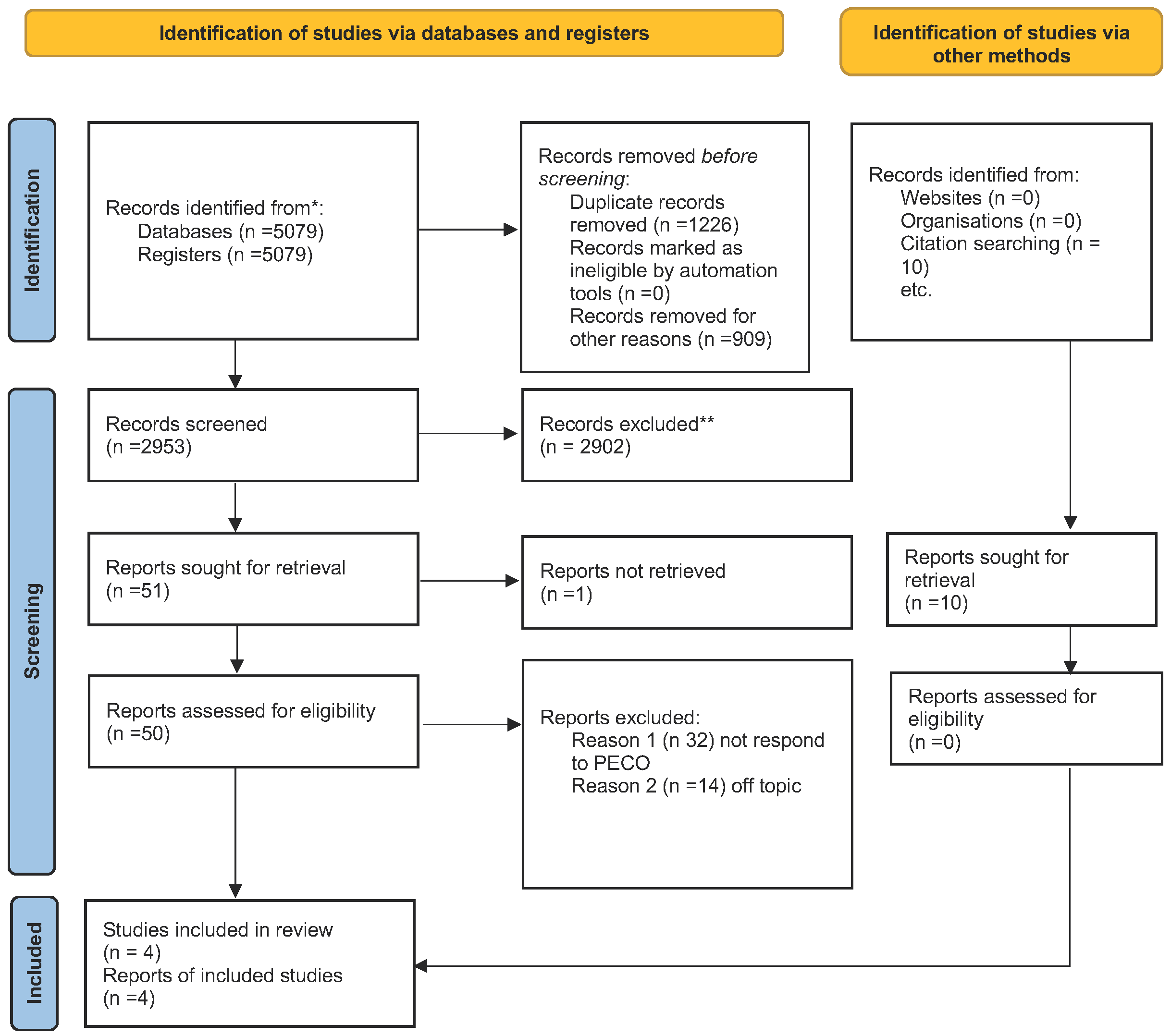
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Strategy
2.3. Data Extraction
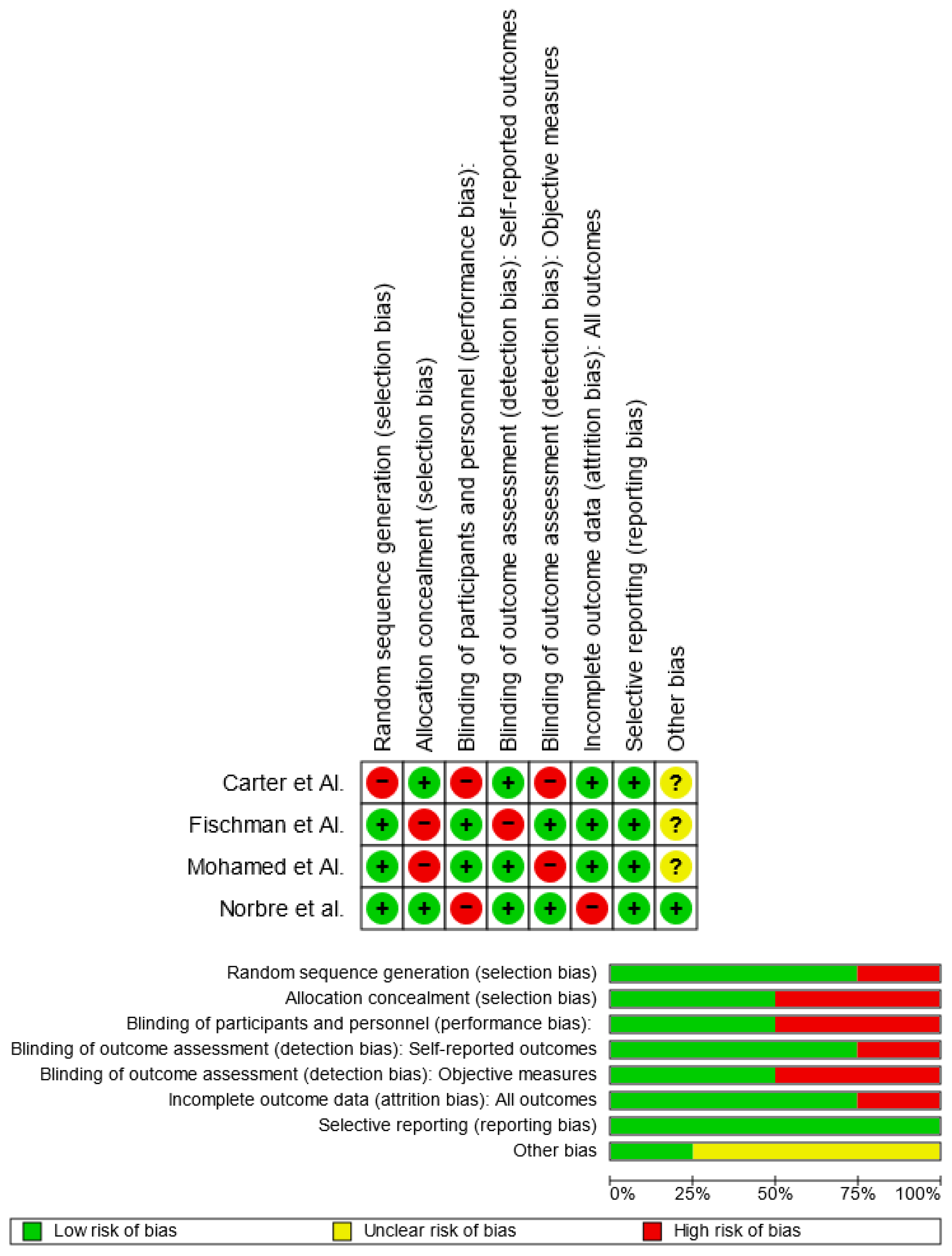
2.4. Quality Assessment
3. Results
3.1. Study Characteristics
3.2. Main Findings
3.3. Quality Assessment and Risk of Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| GD | Gaucher disease |
| CNS | Central nervous system |
| ERT | Enzyme replacement therapy |
| PECO | Patients, Exposure, Comparison, Outcome |
| MeSH | Medical subjects headings |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| GI | Gingival index |
| DMFT | Decayed, missing and filled teeth |
| CBCT | Cone beam tc |
| TMJ | Temporomandibular joint |
| MS | Missing surface |
| DMFS | Decayed, missing and filled surface |
References
- Huang, W.J.; Zhang, X.; Chen, W.W. Gaucher disease: A lysosomal neurodegenerative disorder. Eur. Rev. Med. Pharm. Sci. 2015, 19, 1219–1226. [Google Scholar]
- Stirnemann, J.; Belmatoug, N.; Camou, F.; Serratrice, C.; Froissart, R.; Caillaud, C.; Levade, T.; Astudillo, L.; Serratrice, J.; Brassier, A.; et al. A Review of Gaucher Disease Pathophysiology, Clinical Presentation and Treatments. Int. J. Mol. Sci. 2017, 18, 441. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikosch, P.; Hughes, D. An overview on bone manifestations in Gaucher disease. Wien. Med. Wochenschr. 1946 2010, 160, 609–624. [Google Scholar] [CrossRef] [PubMed]
- Adar, T.; Ilan, Y.; Elstein, D.; Zimran, A. Liver involvement in Gaucher disease—Review and clinical approach. Blood Cells Mol. Dis. 2018, 68, 66–73. [Google Scholar] [CrossRef]
- Moch, W.S. Gaucher’s disease with mandibular bone lesions. Oral Surg. Oral Med. Oral Pathol. 1953, 6, 1250–1254. [Google Scholar] [CrossRef] [PubMed]
- Kumar, N.S.; John, R.R.; Rethish, E. Relatively rare entity of avascular necrosis of maxillary bone caused by Gaucher’s disease—A case report. J. Oral Maxillofac. Surg. 2012, 70, 2590–2595. [Google Scholar] [CrossRef] [PubMed]
- Bender, I.B.; Bender, A.L. Dental observations in Gaucher’s disease: Review of the literature and two case reports with 13-and 60-year follow-ups. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1996, 82, 650–659. [Google Scholar] [CrossRef]
- Becquemont, L. Type 1 Gaucher disease (CYP2D6-eliglustat). Therapies 2017, 72, 323–326. [Google Scholar] [CrossRef]
- Lehrer, S.; Montazem, A.; Ramanathan, L.; Pessin-Minsley, M.; Pfail, J.; Stock, R.G.; Kogan, R. Bisphosphonate-induced osteonecrosis of the jaws, bone markers, and a hypothesised candidate gene. J. Oral Maxillofac. Surg. 2009, 67, 159–161. [Google Scholar] [CrossRef]
- Komada, N.; Fujiwara, T.; Yoshizumi, H.; Ida, H.; Shimoda, K.A. Japanese Patient with Gaucher Disease Treated with the Oral Drug Eliglustat as Substrate Reducing Therapy. Case Rep. Gastroenterol. 2021, 15, 838–845. [Google Scholar] [CrossRef]
- Mitsui, J.; Matsukawa, T.; Sasaki, H.; Yabe, I.; Matsushima, M.; Dürr, A.; Brice, A.; Takashima, H.; Kikuchi, A.; Aoki, M.; et al. Variants associated with Gaucher disease in multiple system atrophy. Ann. Clin. Transl. Neurol. 2015, 2, 417–426. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poll, L.W.; Koch, J.A.; Vom Dahl, S.; Loxtermann, E.; Sarbia, M.; Niederau, C.; Häussinger, D.; Mödder, U. Extraosseous manifestation of Gaucher’s disease type I: MR and histological appearance. Eur. Radiol. 2000, 10, 1660–1663. [Google Scholar] [CrossRef] [PubMed]
- Saccomanno, S.; Quinzi, V.; D’andrea, N.; Albani, A.; Paskay, L.C.; Marzo, G. Traumatic events and eagle syndrome: Is there any correlation? A systematic review. Healthcare 2021, 9, 825. [Google Scholar] [CrossRef]
- Peterschmitt, M.J.; Freisens, S.; Underhill, L.H.; Foster, M.C.; Lewis, G.; Gaemers, S.J.M. Long-term adverse event profile from four completed trials of oral eliglustat in adults with Gaucher disease type 1. Orphanet J. Rare Dis. 2019, 14, 128. [Google Scholar] [CrossRef] [Green Version]
- Nobre, R.M.; Ribeiro, A.L.R.; Alves-Junior, S.M.; Tuji, F.M.; Rodrigues Pinheiro, M.D.G.; Pinheiro, L.R.; Pinheiro, J.J.V. Dentomaxillofacial manifestations of Gaucher’s disease: Preliminary clinical and radiographic findings. Dentomaxillofac. Radiol. 2012, 41, 541–547. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mistry, P.K.; Cappellini, M.D.; Lukina, E.; Özsan, H.; Pascual, S.M.; Rosenbaum, H.; Solano, M.H.; Spigelman, Z.; Villarrubia, J.; Watman, N.P.; et al. Consensus Conference: A reappraisal of Gaucher disease-diagnosis and disease management algorithms. Am. J. Hematol. 2011, 86, 110–115. [Google Scholar] [CrossRef]
- Carter, L.C.; Fischman, S.L.; Mann, J.; Elstein, D.; Stabholz, A.; Zimran, A. The nature and extent of jaw involvement in Gaucher disease: Observations in a series of 28 patients. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 1998, 85, 233–239. [Google Scholar] [CrossRef] [PubMed]
- Fischman, S.L.; Elstein, D.; Sgan-Cohen, H.; Mann, J.; Zimran, A. Dental profile of patients with Gaucher disease. BMC Oral Health 2003, 3, 4. [Google Scholar] [CrossRef] [Green Version]
- Femiano, F.; Femiano, R.; Femiano, L.; Nucci, L.; Minervini, G.; Antonelli, A.; Bennardo, F.; Barone, S.; Scotti, N.; Sorice, V.; et al. A New Combined Protocol to Treat the Dentin Hypersensitivity Associated with Non-Carious Cervical Lesions: A Randomized Controlled Trial. Appl. Sci. 2020, 11, 187. [Google Scholar] [CrossRef]
- Minervini, G.; Franco, R.; Marrapodi, M.M.; Mehta, V.; Fiorillo, L.; Badnjević, A.; Cervino, D.; Cicciu, M. The Association between COVID-19 Related Anxiety, Stress, Depression, Temporomandibular Disorders, and Headaches from Childhood to Adulthood: A Systematic Review. Brain Sci. 2023, 13, 481. [Google Scholar] [CrossRef]
- Mohamed, Y.S.A.; Zayet, M.K.; Omar, O.M.; El-Beshlawy, A.M. Jaw bones’ involvement and dental features of type I and type III Gaucher disease: A radiographic study of 42 paediatric patients. Eur. Arch. Paediatr. Dent. 2020, 21, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Fiorillo, L.; De Stefano, R.; Cervino, G.; Crimi, S.; Bianchi, A.; Herford, A.S.; Laino, L.; Cicciù, M.; Campagna, P. Oral and psychological alterations in haemophiliac patients. Biomedicines 2019, 7, 33. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spagnuolo, G.; Sorrentino, R. The Role of Digital Devices in Dentistry: Clinical Trends and Scientific Evidences. J. Clin. Med. 2020, 9, 1692. [Google Scholar] [CrossRef]
- Chakraborty, T.; Jamal, R.F.; Battineni, G.; Teja, K.V.; Marto, C.M.; Spagnuolo, G. A review of prolonged post-covid-19 symptoms and their implications on dental management. Int. J. Environ. Res. Public Health 2021, 18, 5131. [Google Scholar] [CrossRef]
- Cicciù, M.; Herford, A.S.; Cervino, G.; Troiano, G.; Lauritano, F.; Laino, L. Tissue fluorescence imaging (VELscope) for quick non-invasive diagnosis in oral pathology. J. Craniofacial Surg. 2017, 28, e112–e115. [Google Scholar] [CrossRef] [PubMed]
- Spagnuolo, G. Cone-Beam Computed Tomography and the Related Scientific Evidence. Appl. Sci. 2022, 12, 7140. [Google Scholar] [CrossRef]
- Weinreb, N.J. Encore! Oral therapy for type 1 Gaucher disease. Blood J. Am. Soc. Hematol. 2017, 129, 2337–2338. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cervino, G.; Fiorillo, L.; Arzukanyan, A.V.; Spagnuolo, G.; Campagna, P.; Cicciù, M. Application of bioengineering devices for stress evaluation in dentistry: The last 10 years FEM parametric analysis of outcomes and current trends. Minerva Stomatol. 2020, 69, 9. [Google Scholar] [CrossRef]
- Chis, B.A.; Chis, A.F.; Dumitrascu, D.L. Gaucher disease—Therapeutic aspects in Romania. Med. Pharm. Rep. 2021, 94 (Suppl. 1), S51–S53. [Google Scholar]
- Givol, N.; Goldstein, G.; Peleg, O.; Shenkman, B.; Zimran, A.; Elstein, D.; Kenet, G. Thrombocytopenia and bleeding in dental procedures of patients with Gaucher disease. Haemophilia 2012, 18, 117–121. [Google Scholar] [CrossRef]
- Mehta, V.; Sarode, G.S.; Obulareddy, V.T.; Sharma, T.; Kokane, S.; Cicciù, M.; Minervini, G. Clinicopathologic Profile, Management and Outcome of Sinonasal Ameloblastoma—A Systematic Review. J. Clin. Med. 2023, 12, 381. [Google Scholar] [CrossRef] [PubMed]
- Minervini, G.; Mariani, P.; Fiorillo, L.; Cervino, G.; Cicciù, M.; Laino, L. Prevalence of temporomandibular disorders in people with multiple sclerosis: A systematic review and meta-analysis. CRANIO® 2022, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Quinzi, V.; Paskay, L.C.; Manenti, R.J.; Giancaspro, S.; Marzo, G.; Saccomanno, S. Telemedicine for a multidisciplinary assessment of orofacial pain in a patient affected by eagle’s syndrome: A clinical case report. Open Dent. J. 2021, 15, 102–110. [Google Scholar] [CrossRef]
- D’Amore, S.; Kumar, N.; Ramaswami, U. Jaw involvement in Gaucher disease: A not-so-uncommon feature of a rare disease. BMJ Case Rep. 2021, 14, e244298. [Google Scholar] [CrossRef]
- Nahidh, M.; Al-Khawaja, N.F.K.; Jasim, H.M.; Cervino, G.; Cicciù, M.; Minervini, G. The Role of Social Media in Communication and Learning at the Time of COVID-19 Lockdown—An Online Survey. Dent. J. 2023, 11, 48. [Google Scholar] [CrossRef]
- Minervini, G.; Del Mondo, D.; Russo, D.; Cervino, G.; D’Amico, C.; Fiorillo, L. Stem Cells in Temporomandibular Joint Engineering: State of Art and Future Persectives. J. Craniofacial Surg. 2022, 33, 2181–2187. [Google Scholar] [CrossRef]
- Minervini, G.; Basili, M.; Franco, R.; Bollero, P.; Mancini, M.; Gozzo, L.; Romano, G.L.; Marrapodi, M.M.; Gorassini, F.; D’Amico, C. Periodontal Disease and Pregnancy: Correlation with Underweight Birth. Eur. J. Dent. 2022. [Google Scholar] [CrossRef]
- Temelci, A.; Yılmaz, H.G.; Ünsal, G.; Uyanik, L.O.; Yazman, D.; Ayali, A.; Minervini, G. Investigation of the Wetting Properties of Thalassemia Patients’ Blood Samples on Grade 5 Titanium Implant Surfaces: A Pilot Study. Biomimetics 2023, 8, 25. [Google Scholar] [CrossRef]
- Rathi, S.; Chaturvedi, S.; Abdullah, S.; Rajput, G.; Alqahtani, N.M.; Chaturvedi, M.; Gurumurthy, V.; Saini, R.; Bavabeedu, S.; Minervini, G. Clinical Trial to Assess Physiology and Activity of Masticatory Muscles of Complete Denture Wearer Following Vitamin D Intervention. Medicina 2023, 59, 410. [Google Scholar] [CrossRef]
- Vu, L.; Cox, G.F.; Ibrahim, J.; Peterschmitt, M.J.; Ross, L.; Thibault, N.; Turpault, S. Effects of paroxetine, ketoconazole, and rifampin on the metabolism of eliglustat, an oral substrate reduction therapy for Gaucher disease type 1. Mol. Genet. Metab. Rep. 2020, 22, 100552. [Google Scholar] [CrossRef]
- Elstein, D.; Itzchaki, M.; Mankin, H.J. Skeletal involvement in Gaucher’s disease. Baillière’s Clin. Haematol. 1997, 10, 793–816. [Google Scholar] [CrossRef]
- Morgan, R.L.; Whaley, P.; Thayer, K.A.; Schünemann, H.J. Identifying the PECO: A framework for formulating good questions to explore the association of environmental and other exposures with health outcomes. Environ. Int. 2018, 121, 1027–1031. [Google Scholar] [CrossRef] [PubMed]
- La Torre, G.; Shivkumar, S.; Mehta, V.; Kumar Vaddamanu, S.; Shetty, U.A.; Hussain Alhamoudi, F.; Ali Alwadi, M.; Ibrahim Aldosari, L.; Ali Alshadidi, A.; Minervini, G. Surgical Protocols before and after COVID-19-A Narrative Review. Vaccines 2023, 11, 439. [Google Scholar] [CrossRef]
- Bollero, P.; Carmine, P.P.; D’Addona, A.; Pasquantonio, G.; Mancini, M.; Condò, R.; Cerroni, L. Oral management of adult patients undergoing hematopoietic stem cell transplantation. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 876–887. [Google Scholar] [PubMed]
- Saranjam, H.R.; Sidransky, E.; Levine, W.Z.; Zimran, A.; Elstein, D. Mandibular and dental manifestations of Gaucher disease. Oral Dis. 2012, 18, 421–429. [Google Scholar] [CrossRef] [Green Version]
- Michanowicz, A.E.; Michanowicz, J.P.; Stein, G.M. Gaucher’s disease: Report of a case. Oral Surg. Oral Med. Oral Pathol. 1967, 23, 36–42. [Google Scholar] [CrossRef]
- Aşantoğrol, F.; Dursun, H.; Canger, E.M.; Bayram, F. Clinical and radiological evaluation of dentomaxillofacial involvement in Type I Gaucher disease. Oral Radiol. 2022, 38, 210–223. [Google Scholar] [CrossRef]
- Gurbeta, L.; Alic, B.; Dzemic, Z.; Badnjevic, A. Testing of infusion pumps in healthcare institutions in Bosnia and herzegovina. In Proceedings of the Joint Conference of the European Medical and Biological Engineering Conference (EMBEC) and the Nordic-Baltic Conference on Biomedical Engineering and Medical Physics (NBC), Tampere, Finland, 11–15 June 2017; pp. 390–393. [Google Scholar]
- Badnjevic, A.; Koruga, D.; Cifrek, M.; Smith, H.J.; Bego, T. Interpretation of pulmonary function test results in relation to asthma classification using integrated software suite. In Proceedings of the 36th International Convention on Information and Communication Technology, Electronics and Microelectronics (MIPRO 2013), Opatija, Croatia, 20–24 May 2013; pp. 140–144. [Google Scholar]
- Granulo, E.; Bećar, L.; Gurbeta, L.; Badnjević, A. Telemetry system for diagnosis of asthma and chronical obstructive pulmonary disease (COPD). In Lecture Notes of the Institute for Computer Sciences, Social-Informatics and Telecommunications Engineering, Proceedings of the Third International Conference, HealthyIoT 2016, Västerås, Sweden, 18–19 October 2016; Springer: Cham, Switzerland, 2016; Volume LNICST 187, pp. 113–118. [Google Scholar]
- Stokes, K.; Castaldo, R.; Franzese, M.; Salvatore, M.; Fico, G.; Pokvic, L.G.; Badnjevic, A.; Pecchia, L. A machine learning model for supporting symptom-based referral and diagnosis of bronchitis and pneumonia in limited resource settings. Biocybern. Biomed. Eng. 2021, 41, 1288–1302. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| PubMed (gaucher disease) AND ((bone) OR (oral health)) |
| Web of Science TITLE-ABS-KEY (gaucher disease) AND ((bone) OR (oral health)) |
| Lilacs (gaucher disease) AND ((bone) OR (oral health)) |
| Scopus TITLE-ABS-KEY (((gaucher AND disease) AND ((bone) OR (oral AND health)))) |
| Authors | Year | Sample | Age | Radiographic Signs | Evaluation of Oral Health | Nationality |
|---|---|---|---|---|---|---|
| Norbre et al. | 2012 | 10 with GD compared with 20 healthy | 23.2 years | Generalized rarefaction and enlarged narrow space | No difference | Brazil |
| Mohamed et al. | 2020 | 42 with GD compared with 84 healthy | 11.37 years | Generalized rarefaction, pseudocysts radiolucent lesion, anodontia | No difference | Egypt |
| Fischman et al. | 2003 | 350 with GD and 31 control | 30.7 years | Bone involvement is frequent. The finding in the ortho-panoramic is always frequent | No statistical significance between DMFT, Gingival Index | Israel |
| Carter et al. | 1998 | 28 with GD | 32.4 years | The most common findings are enlargement of medullary spaces | No dental findings in oral health | Israel |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Minervini, G.; Franco, R.; Marrapodi, M.M.; Mehta, V.; Fiorillo, L.; Badnjević, A.; Cervino, G.; Cicciù, M. Gaucher: A Systematic Review on Oral and Radiological Aspects. Medicina 2023, 59, 670. https://doi.org/10.3390/medicina59040670
Minervini G, Franco R, Marrapodi MM, Mehta V, Fiorillo L, Badnjević A, Cervino G, Cicciù M. Gaucher: A Systematic Review on Oral and Radiological Aspects. Medicina. 2023; 59(4):670. https://doi.org/10.3390/medicina59040670
Chicago/Turabian StyleMinervini, Giuseppe, Rocco Franco, Maria Maddalena Marrapodi, Vini Mehta, Luca Fiorillo, Almir Badnjević, Gabriele Cervino, and Marco Cicciù. 2023. "Gaucher: A Systematic Review on Oral and Radiological Aspects" Medicina 59, no. 4: 670. https://doi.org/10.3390/medicina59040670