


Different Designs of Deep Marginal Elevation and Its Influence on Fracture Resistance of Teeth with Monolith Zirconia Full-Contour Crowns
 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sample Collection
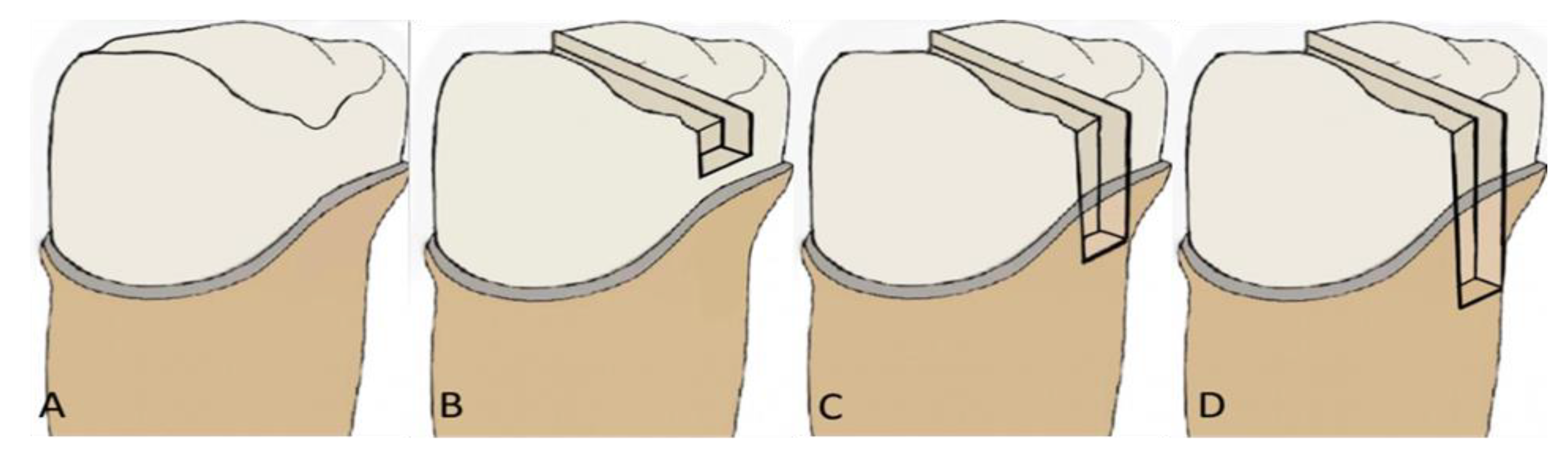
2.3. Description of the Experimental Groups
2.4. Tooth Preparation
2.5. Fabrication of Crowns
2.6. Cementation
2.7. Aging
2.8. Fracture Test
2.9. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Serin Kalay, T.; Yildirim, T.; Ulker, M. Effects of different cusp coverage restorations on the fracture resistance of endodontically treated maxillary premolars. J. Prosthet. Dent. 2016, 116, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Dablanca-Blanco, A.B.; Blanco-Carrión, J.; Martín-Biedma, B.; Varela-Patiño, P.; Bello-Castro, A.; Castelo-Baz, P. Management of large class II lesions in molars: How to restore and when to perform surgical crown lengthening. Restor. Dent. Endod. 2017, 42, 240–252. [Google Scholar] [CrossRef] [PubMed]
- Veneziani, M. Adhesive restorations in the posterior area with subgingival cervical margins: New classification and differentiated treatment approach. Eur. J. Esthet. Dent. 2010, 5, 50–76. [Google Scholar]
- Magne, P.; Spreafico, R.C. Deep margin elevation: A paradigm shift. Am. J. Esthet. Dent. 2012, 2, 86–96. [Google Scholar]
- Ferrari, M.; Koken, S.; Grandini, S.; Ferrari Cagidiaco, E.; Joda, T.; Discepoli, N. Influence of cervical margin relocation (CMR) on periodontal health: 12-month results of a controlled trial. J. Dent. 2018, 69, 70–76. [Google Scholar] [CrossRef]
- Dietschi, D.; Spreafico, R. Current clinical concepts for adhesive cementation of tooth-colored posterior restorations. Pract. Periodontics Aesthet. Dent. 1998, 10, 47–56. [Google Scholar] [PubMed]
- Juloski, J.; Köken, S.; Ferrari, M. Cervical margin relocation in indirect adhesive restorations: A literature review. J. Prosthodont. Res. 2018, 62, 273–280. [Google Scholar] [CrossRef]
- Martins, T.M.; Bosco, A.F.; Nóbrega, F.J.; Nagata, M.J.; Garcia, V.G.; Fucini, S.E. Periodontal tissue response to coverage of root cavities restored with resin materials: A histomorphometric study in dogs. J. Periodontol. 2007, 78, 1075–1082. [Google Scholar] [CrossRef]
- Shahmoradi, M.; Wan, B.; Zhang, Z.; Swain, M.; Li, Q. Mechanical failure of posterior teeth due to caries and occlusal wear- A modelling study. J. Mech. Behav. Biomed. Mater. 2022, 125, 104942. [Google Scholar] [CrossRef]
- Abu-Awwad, M. Dentists’ decisions regarding the need for cuspal coverage for endodontically treated and vital posterior teeth. Clin. Exp. Dent. Res. 2019, 5, 326–335. [Google Scholar] [CrossRef]
- Irusa, K.; Al-Rawi, B.; Donovan, T.; Alraheam, I.A. Survival of cast gold and ceramic onlays placed in a school of Dentistry: A Retrospective Study. J. Prosthodont. 2020, 29, 693–698. [Google Scholar] [CrossRef]
- Miyazaki, T.; Nakamura, T.; Matsumura, H.; Ban, S.; Kobayashi, T. Current status of zirconia restoration. J. Prosthodont. Res. 2013, 57, 236–261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skjold, A.; Schriwer, C.; Olio, M. Effect of margin design on fracture load of zirconia crowns. Eur. J. Oral Sci. 2019, 127, 89–96. [Google Scholar] [CrossRef]
- Kim, S.-H.; Yeo, M.-Y.; Choi, S.-Y.; Park, E.-J. Fracture resistance of monolith zirconia crowns depending on different marginal thicknesses. Materials 2022, 15, 4861. [Google Scholar] [CrossRef]
- Sadeqi, H.A.; Baig, M.R.; Al-Shammari, M. Evaluation of marginal/internal fit and fracture load of monolithic zirconia and zirconia lithium silicate (ZLS) CAD/CAM crown systems. Materials 2021, 14, 6346. [Google Scholar] [CrossRef] [PubMed]
- Raszewski, Z.; Brzakalski, D.; Derpenski, L.; Jalbrzykowski, M.; Przekop, R.E. Aspects and principles of material connections in Restorative dentistry—A comprehensive review. Materials 2022, 15, 7131. [Google Scholar] [CrossRef] [PubMed]
- Thammajaruk, P.; Inokoshi, M.; Chong, S.; Guazzato, M. Bonding of composite cements to zirconia: A systematic review and meta-analysis of in vitro studies. J. Mech. Behav. Biomed. Mater. 2018, 80, 258–268. [Google Scholar] [CrossRef] [PubMed]
- Grassi, E.D.A.; de Andrade, G.S.; Tribst, J.P.M.; Machry, R.V.; Valandro, L.F.; Ramos, N.D.C.; Bresciani, E.; Saavedra, G.D.S.F.A. Fatigue behavior and stress distribution of molars restored with MOD inlays with and without deep margin elevation. Clin. Oral. Investig. 2021, 26, 2513–2526. [Google Scholar] [CrossRef]
- Reeh, E.S.; Messer, H.H.; Douglas, W.H. Reduction in tooth stiffness as a result of endodontic and restorative procedures. J. Endod. 1989, 15, 512–516. [Google Scholar] [CrossRef]
- Wang, B.; Fan, J.; Wang, L.; Xu, B.; Wang, L.; Chai, L. Onlays/partial crowns versus full crowns in restoring posterior teeth: A systematic review and meta-analysis. Head Face Med. 2022, 18, 36. [Google Scholar] [CrossRef]
- Ilgenstein, I.; Zitzmann, N.; Bühler, J.; Wegehaupt, F.; Attin, T.; Weiger, R.; Krastl, G. Influence of proximal box elevation on the marginal quality and fracture behavior of root-filled molars restored with CAD/CAM ceramic or composite onlays. Clin. Oral Investig. 2014, 19, 1021–1028. [Google Scholar] [CrossRef] [Green Version]
- Bresser, R.; van de Geer, L.; Gerdolle, D.; Schepke, U.; Cune, M.; Gresnigt, M. Influence of deep margin elevation and preparation design on the fracture strength of indirectly restored molars. J. Mech. Behav. Biomed. Mater. 2020, 110, 103950. [Google Scholar] [CrossRef] [PubMed]
- Roggendorf, M.J.; Krämer, N.; Dippold, C.; Vosen, V.E.; Naumann, M.; Jablonski-Momeni, A.; Frankenberger, R. Effect of proximal box elevation with resin composite on marginal quality of resin composite inlays in vitro. J. Dent. 2012, 40, 1068–1073. [Google Scholar] [CrossRef]
- Mugri, M.H.; Sayed, M.E.; Nedumgottil, B.M.; Bhandi, S.; Raj, A.T.; Testarelli, L.; Khurshid, Z.; Jain, S.; Patil, S. Treatment Prognosis of Restored Teeth with Crown Lengthening vs. Deep Margin Elevation: A Systematic Review. Materials 2021, 14, 6733. [Google Scholar] [CrossRef] [PubMed]
- Bertoldi, C.; Monari, E.; Cortellini, P.; Generali, L.; Lucchi, A.; Spinato, S.; Zaffe, D. Clinical and Histological Reaction of Periodontal Tissues to Subgingival Resin Composite Restorations. Clin. Oral Investig. 2019, 24, 1001–1011. [Google Scholar] [CrossRef]
- Ghezzi, C.; Brambilla, G.; Conti, A.; Dosoli, R.; Ceroni, F.; Ferrantino, L. Cervical margin relocation: Case series and new classifica-tion system. Int. J. Esthet. Dent. 2019, 14, 272–284. [Google Scholar] [PubMed]
- Zhang, H.; Li, H.; Cong, Q.; Zhang, Z.; Du, A.; Wang, Y. Effect of proximal box elevation on fracture resistance and microleakage of premolars restored with ceramic endocrowns. PLoS ONE 2021, 16, e0252269. [Google Scholar] [CrossRef]
- Grubbs, T.D.; Vargas, M.; Kolker, J.; Teixeira, E.C. Efficacy of direct restorative materials in proximal box elevation on the margin quality and fracture resistance of molars restored with CAD/CAM onlays. Oper. Dent. 2020, 45, 52–61. [Google Scholar] [CrossRef] [Green Version]
- Scotti, N.; Baldi, A.; A Vergano, E.; Tempesta, R.M.; Alovisi, M.; Pasqualini, D.; Carpegna, G.C.; Comba, A. Tridimensional evaluation of the interfacial gap in deep cervical margin restorations: A micro-CT study. Oper. Dent. 2020, 45, E227–E236. [Google Scholar] [CrossRef]
- Christensen, G.J. The case for onlays versus tooth-colored crowns. J. Am. Dent. Assoc. 2012, 143, 1141–1144. [Google Scholar] [CrossRef]
- Al-Haj Husain, N.; Özcan, M.; Molinero-Mourelle, P.; Joda, T. Clinical performance of partial and full-coverage fixed dental restorations fabricated from hybrid polymer and ceramic CAD/CAM materials: A systematic review and meta-analysis. J. Clin. Med. 2020, 9, 2107. [Google Scholar] [CrossRef] [PubMed]
- Larsson, C.; Wennerberg, A. The clinical success of zirconia-based crowns: A systematic review. Int. J. Prosthodont. 2014, 27, 33–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sulaiman, T.A.; Abdulmajeed, A.A.; Delgado, A.; Donovan, T.E. Fracture rate of 188695 lithium disilicate and zirconia ceramic restorations after up to 7.5 years of clinical service: A dental laboratory survey. J. Prosthet. Dent. 2020, 123, 807–810. [Google Scholar] [CrossRef]
- Sola-Ruiz, M.F.; Baixauli-Lopez, M.; Roig-Vanaclocha, A.; Amengual-Lorenzo, J.; Agustin-Panadero, R. Prospective study of monolith zirconia crowns: Clinical behavior and survival rate at a 5-year follow-up. J. Prosthodont. Res. 2021, 65, 284–290. [Google Scholar] [CrossRef]
- Göktürk, H.; Karaarslan, E.Ş.; Tekin, E.; Hologlu, B.; Sarıkaya, I. The effect of the different restorations on fracture resistance of root-filled premolars. BMC Oral Health 2018, 18, 196. [Google Scholar] [CrossRef] [PubMed]
- Rekow, E.D.; Harsono, M.; Janal, M.; Thompson, V.P.; Zhang, G. Factorial analysis of variables influencing stress in all-ceramic crowns. Dent. Mater. 2006, 22, 125–132. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, K.; Harada, A.; Inagaki, R.; Kanno, T.; Niwano, Y.; Milleding, P.; Örtengren, U. Fracture resistance of monolithic zirconia molar crowns with reduced thickness. Acta. Odontol. Scand. 2015, 73, 602–608. [Google Scholar] [CrossRef] [Green Version]
- Jassim, Z.M.; Majeed, M.A. Comparative evaluation of the fracture strength of monolithic crowns fabricated from different all-ceramic CAD/CAM materials (an in vitro study). Biomed. Pharmacol. J. 2018, 11, 1689–1697. [Google Scholar] [CrossRef]
- Chen, Y.C.; Lin, C.L.; Hou, C.H. Investigating inlay designs of class II cavity with deep margin elevation using finite element method. BMC Oral Health 2021, 21, 264. [Google Scholar] [CrossRef]
- Zhang, H. Fracture resistance of endodontically treated premolar with deep class II: In vitro evaluation of different restorative procedures. Investig. Clin. 2019, 60, 154–161. [Google Scholar]
- Alahmari, N.M.; Adawi, H.A.; Moaleem, M.M.A.; Alqahtani, F.M.; Alshahrani, F.T.; Aldhelai, T.A. Effects of the cervical marginal relocation technique on the marginal adaptation of lithium disilicate CAD/CAM ceramic crowns on premolars. J. Contemp. Dent. Pract. 2021, 22, 900–906. [Google Scholar] [CrossRef] [PubMed]
- Sorrentino, R.; Nagasawa, Y.; Infelise, M.; Bonadeo, G.; Ferrari, M. In vitro analysis of the fracture resistance of CAD-CAM monolithic lithium disilicate molar crowns with different occlusal thickness. J. Osseointegr. 2018, 10, 50–56. [Google Scholar] [CrossRef]
- Yildiz, C.; Vanlioğlu, B.A.; Evren, B.; Uludamar, A.; Ozkan, Y.K. Marginal-internal adaptation and fracture resistance of CAD/CAM crown restorations. Dent. Mater. J. 2013, 32, 42–47. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sorrentino, R.; Triulzio, C.; Tricarico, M.G.; Bonadeo, G.; Gherlone, E.F.; Ferrari, M. In vitro analysis of the fracture resistance of CAD-CAM monolithic zirconia molar crowns with different occlusal thickness. J. Mech. Behav. Biomed. Mater. 2016, 61, 328–333. [Google Scholar] [CrossRef]
- Zhang, Y.; Mai, Z.; Barani, A.; Bush, M.; Lawn, B. Fracture-resistant monolithic dental crowns. Dent. Mater. 2016, 32, 442–449. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample | Control | Mesio-Occluso-Distal (MOD) Tooth Preparation | ||||||
|---|---|---|---|---|---|---|---|---|
| A | B | C | D | |||||
| Maximum Load (N) | FR (MPa) | Maximum Load (N) | FR (MPa) | Maximum Load (N) | FR (MPa) | Maximum Load (N) | FR (MPa) | |
| 1 | 3436.55 | 72.65 | 2040.66 | 56.06 | 1460.13 | 34.97 | 1368.39 | 30.23 |
| 2 | 3586.65 | 75.82 | 2072.61 | 45.22 | 2012.64 | 42.62 | 2285.31 | 40.88 |
| 3 | 3479.02 | 73.55 | 1801.64 | 49.57 | 2253.41 | 51.77 | 2168.52 | 45.84 |
| 4 | 3219.50 | 68.06 | 2222.84 | 48.38 | 2704.48 | 57.17 | 2103.77 | 41.80 |
| 5 | 3357.72 | 70.98 | 2959.94 | 62.57 | 2173.11 | 45.94 | 2180.15 | 43.61 |
| 6 | 3485.54 | 73.69 | 3170.40 | 67.02 | 2452.58 | 51.85 | 1358.02 | 32.16 |
| 7 | 3411.18 | 72.11 | 2737.58 | 57.87 | 1582.64 | 47.36 | 1883.83 | 48.56 |
| 8 | 3393.20 | 71.73 | 2654.50 | 56.12 | 2014.36 | 42.58 | 1979.91 | 45.99 |
| 9 | 3436.22 | 72.64 | 2773.51 | 58.63 | 2597.09 | 54.90 | 1854.38 | 41.00 |
| 10 | 3350.55 | 70.83 | 2507.50 | 53.01 | 1832.15 | 49.87 | 1737.28 | 36.72 |
| Units | Groups | n | Mean | Std. Deviation | 95% Confidence Interval | p-Value | |
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
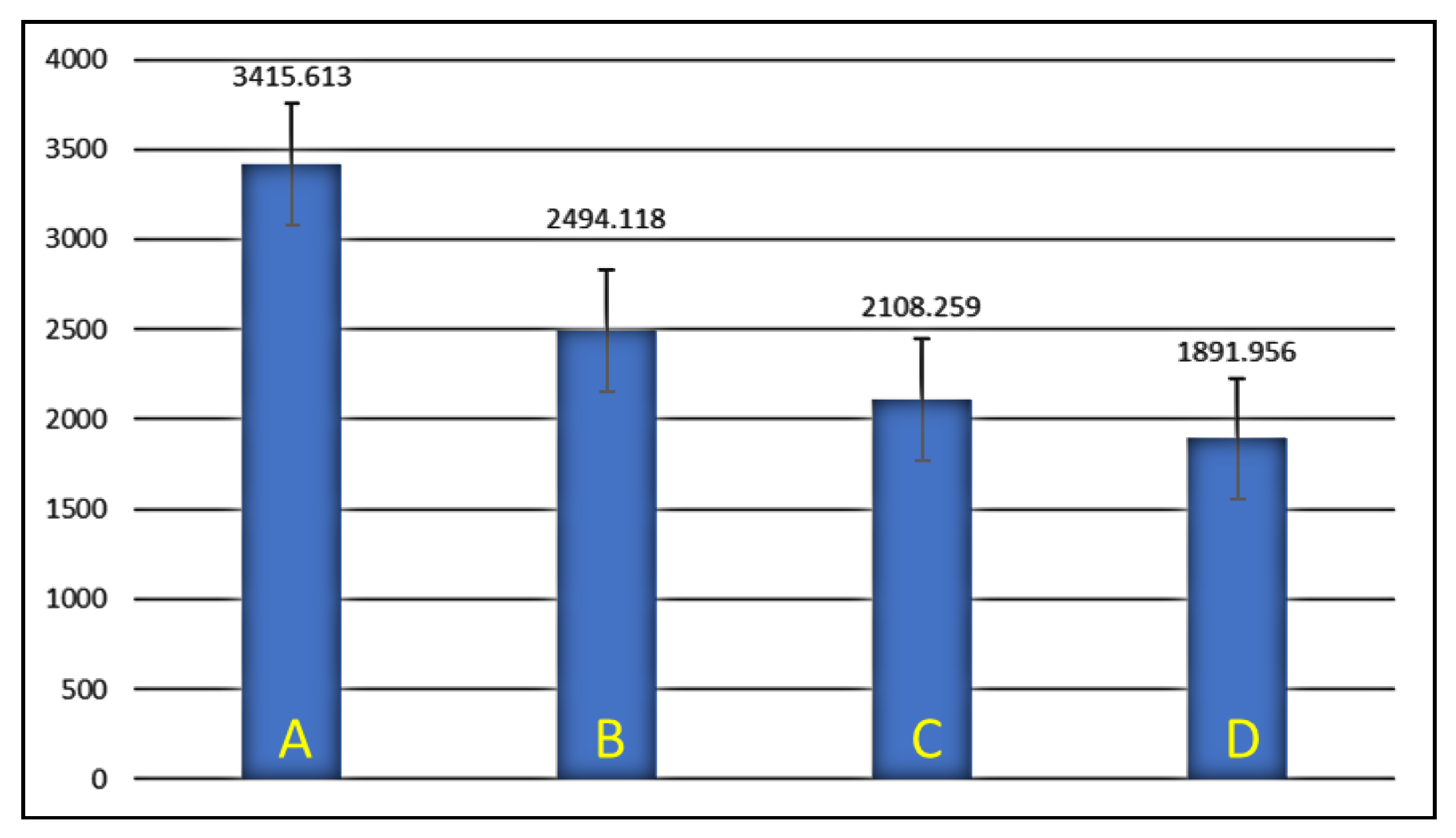
| Max load(N) | A | 10 | 3415.61 | 97.52 | 3345.8503 | 3485.3757 | <0.00001 *** |
| B | 10 | 2494.11 | 443.97 | 2176.5202 | 2811.7158 | ||
| C | 10 | 2108.25 | 412.15 | 1813.4246 | 2403.0934 | ||
| D | 10 | 1891.95 | 325.14 | 1659.3600 | 2124.5520 | ||
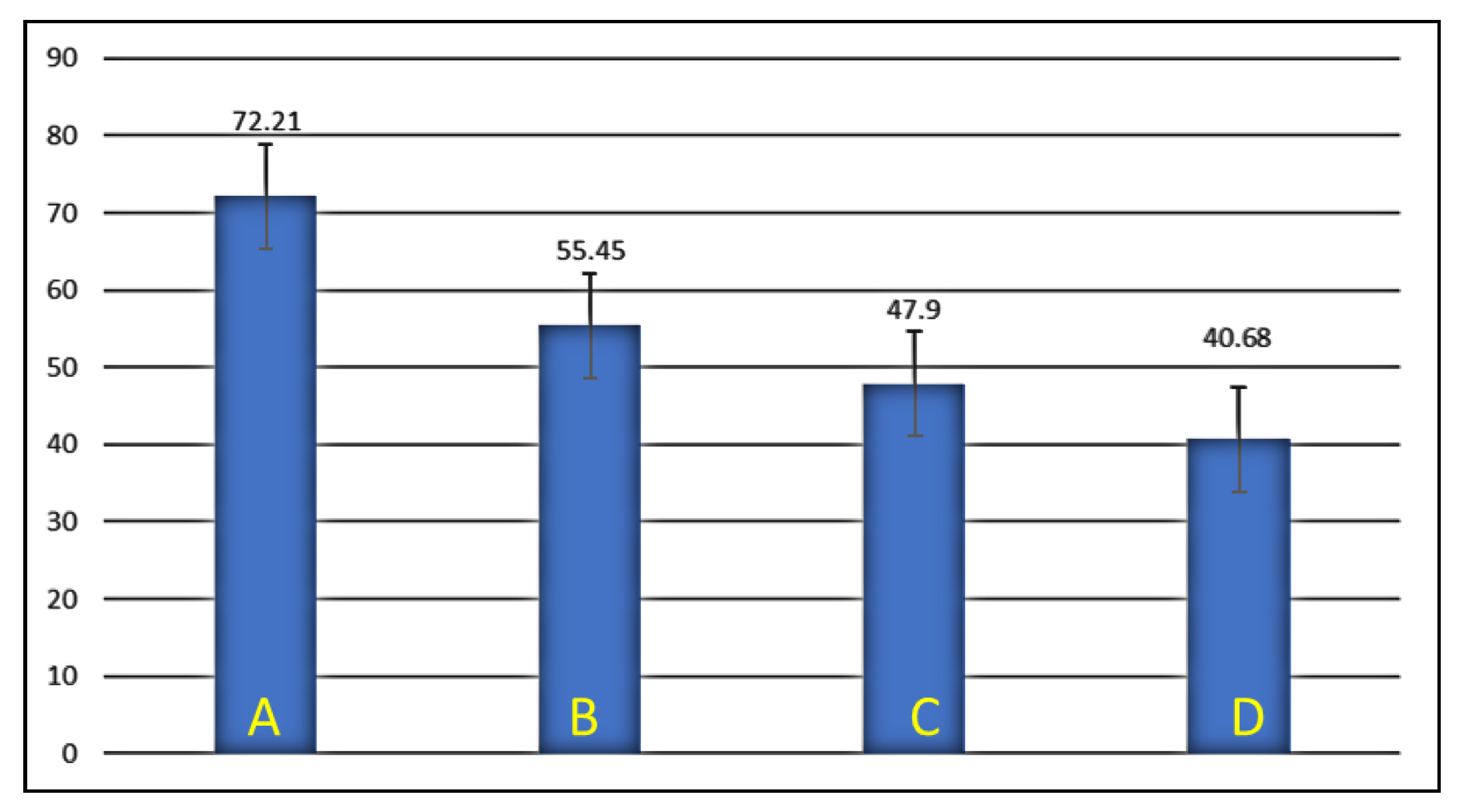
| FR (MPa) | A | 10 | 72.21 | 2.06 | 70.737 | 73.687 | <0.00001 *** |
| B | 10 | 55.45 | 6.63 | 50.701 | 60.199 | ||
| C | 10 | 47.90 | 6.64 | 43.157 | 52.659 | ||
| D | 10 | 40.68 | 6.00 | 36.391 | 44.979 | ||
| Groups | Comparative Groups | Mean Difference | p | 95% Confidence Interval | |
|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||
| A | Group B | 921.49500 | <0.001 *** | 465.0409 | 1377.9491 |
| Group C | 1307.35400 | <0.001 *** | 850.8999 | 1763.8081 | |
| Group D | 1523.65700 | <0.001 *** | 1067.2029 | 1980.1111 | |
| B | Group C | 385.85900 | 0.133 | −70.5951 | 842.3131 |
| Group D | 602.16200 | 0.004 ** | 145.7079 | 1058.6161 | |
| C | Group D | 216.30300 | 0.664 | −240.1511 | 672.7571 |
| Groups | n | R (%) | U (%) |
|---|---|---|---|
| A | 10 | 1 (10) | 9 (90) |
| B | 10 | 1 (10) | 9 (90) |
| C | 10 | 1 (10) | 9 (90) |
| D | 10 | 2 (20) | 8 (80) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Robaian, A.; Alqahtani, A.; Alanazi, K.; Alanazi, A.; Almalki, M.; Aljarad, A.; Albaijan, R.; Maawadh, A.; Sufyan, A.; Mirza, M.B. Different Designs of Deep Marginal Elevation and Its Influence on Fracture Resistance of Teeth with Monolith Zirconia Full-Contour Crowns. Medicina 2023, 59, 661. https://doi.org/10.3390/medicina59040661
Robaian A, Alqahtani A, Alanazi K, Alanazi A, Almalki M, Aljarad A, Albaijan R, Maawadh A, Sufyan A, Mirza MB. Different Designs of Deep Marginal Elevation and Its Influence on Fracture Resistance of Teeth with Monolith Zirconia Full-Contour Crowns. Medicina. 2023; 59(4):661. https://doi.org/10.3390/medicina59040661
Chicago/Turabian StyleRobaian, Ali, Abdullah Alqahtani, Khalid Alanazi, Abdulrhman Alanazi, Meshal Almalki, Anas Aljarad, Refal Albaijan, Ahmed Maawadh, Aref Sufyan, and Mubashir Baig Mirza. 2023. "Different Designs of Deep Marginal Elevation and Its Influence on Fracture Resistance of Teeth with Monolith Zirconia Full-Contour Crowns" Medicina 59, no. 4: 661. https://doi.org/10.3390/medicina59040661