


Association of Different Risk Scores and 30-Day Mortality in Kidney Transplant Recipients with COVID-19


Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical and Institutional Considerations
2.2. Study Design and Patients
2.3. Data Source and Patient Assessment
2.4. Risk Scores of Interests
2.5. Outcomes
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A
References
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- Gao, Y.-D.; Ding, M.; Dong, X.; Zhang, J.-J.; Azkur, A.K.; Azkur, D.; Gan, H.; Sun, Y.-L.; Fu, W.; Li, W.; et al. Risk factors for severe and critically ill COVID-19 patients: A review. Allergy 2021, 76, 428–455. [Google Scholar] [CrossRef]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef]
- Raja, M.A.; Mendoza, M.A.; Villavicencio, A.; Anjan, S.; Reynolds, J.M.; Kittipibul, V.; Fernandez, A.; Guerra, G.; Camargo, J.F.; Simkins, J.; et al. COVID-19 in solid organ transplant recipients: A systematic review and meta-analysis of current literature. Transplant. Rev. 2021, 35, 100588. [Google Scholar] [CrossRef]
- Jager, K.J.; Kramer, A.; Chesnaye, N.C.; Couchoud, C.; Sánchez-Álvarez, J.E.; Garneata, L.; Collart, F.; Hemmelder, M.H.; Ambühl, P.; Kerschbaum, J.; et al. Results from the ERA-EDTA Registry indicate a high mortality due to COVID-19 in dialysis patients and kidney transplant recipients across Europe. Kidney Int. 2020, 98, 1540–1548. [Google Scholar] [CrossRef]
- Loupy, A.; Aubert, O.; Reese, P.P.; Bastien, O.; Bayer, F.; Jacquelinet, C. Organ procurement and transplantation during the COVID-19 pandemic. Lancet 2020, 395, e95–e96. [Google Scholar] [CrossRef]
- Caillard, S.; Chavarot, N.; Francois, H.; Matignon, M.; Greze, C.; Kamar, N.; Gatault, P.; Thaunat, O.; Legris, T.; Frimat, L.; et al. Is COVID-19 infection more severe in kidney transplant recipients? Am. J. Transplant. 2021, 21, 1295–1303. [Google Scholar] [CrossRef]
- Mahalingasivam, V.; Craik, A.; Tomlinson, L.A.; Ge, L.; Hou, L.; Wang, Q.; Yang, K.; Fogarty, D.G.; Keenan, C. A Systematic Review of COVID-19 and Kidney Transplantation. Kidney Int. Rep. 2021, 6, 24–45. [Google Scholar] [CrossRef]
- Pereira, M.R.; Mohan, S.; Cohen, D.J.; Husain, S.A.; Dube, G.K.; Ratner, L.E.; Arcasoy, S.; Aversa, M.M.; Benvenuto, L.J.; Dadhania, D.M.; et al. COVID-19 in solid organ transplant recipients: Initial report from the US epicenter. Am. J. Transplant. 2020, 20, 1800–1808. Available online: https://onlinelibrary.wiley.com/doi/10.1111/ajt.15941 (accessed on 10 May 2022). [CrossRef]
- Demir, E.; Ucar, Z.A.; Dheir, H.; Danis, R.; Yelken, B.; Uyar, M.; Parmaksiz, E.; Artan, A.S.; Sinangil, A.; Merhametsiz, O.; et al. COVID-19 in Kidney Transplant Recipients: A Multicenter Experience from the First Two Waves of Pandemic. BMC Nephrol. 2022, 23, 183. [Google Scholar] [CrossRef]
- Cravedi, P.; Mothi, S.S.; Azzi, Y.; Haverly, M.; Farouk, S.S.; Pérez-Sáez, M.J.; Redondo-Pachón, M.D.; Murphy, B.; Florman, S.; Cyrino, L.G.; et al. COVID-19 and kidney transplantation: Results from the TANGO International Transplant Consortium. Am. J. Transplant. 2020, 20, 3140–3148. [Google Scholar] [CrossRef]
- Blanco-Melo, D.; Nilsson-Payant, B.E.; Liu, W.-C.; Uhl, S.; Hoagland, D.; Møller, R.; Jordan, T.X.; Oishi, K.; Panis, M.; Sachs, D.; et al. Imbalanced Host Response to SARS-CoV-2 Drives Development of COVID-19. Cell 2020, 181, 1036–1045.e9. [Google Scholar] [CrossRef]
- Molnar, M.Z.; Bhalla, A.; Azhar, A.; Tsujita, M.; Talwar, M.; Balaraman, V.; Sodhi, A.; Kadaria, D.; Eason, J.D.; Hayek, S.S.; et al. Outcomes of critically ill solid organ transplant patients with COVID-19 in the United States. Am. J. Transplant. 2020, 20, 3061–3071. [Google Scholar] [CrossRef]
- Chavarot, N.; Gueguen, J.; Bonnet, G.; Jdidou, M.; Trimaille, A.; Burger, C.; Amrouche, L.; Weizman, O.; Pommier, T.; Aubert, O.; et al. COVID-19 severity in kidney transplant recipients is similar to nontransplant patients with similar comorbidities. Am. J. Transplant. 2020, 21, 1285–1294. [Google Scholar] [CrossRef]
- King, J.T., Jr.; Yoon, J.S.; Rentsch, C.T.; Tate, J.P.; Park, L.S.; Kidwai-Khan, F.; Skanderson, M.; Hauser, R.G.; Jacobson, D.A.; Erdos, J.; et al. Development and validation of a 30-day mortality index based on pre-existing medical administrative data from 13,323 COVID-19 patients: The Veterans Health Administration COVID-19 (VACO) Index. PLoS ONE 2020, 15, e0241825. [Google Scholar] [CrossRef]
- Knight, S.R.; Ho, A.; Pius, R.; Buchan, I.; Carson, G.; Drake, T.M.; Dunning, J.; Fairfield, C.J.; Gamble, C.; Green, C.A.; et al. Risk stratification of patients admitted to hospital with covid-19 using the ISARIC WHO Clinical Characterisation Protocol: Development and validation of the 4C Mortality Score. BMJ 2020, 370, m3339. [Google Scholar] [CrossRef]
- Subbe, C.P.; Kruger, M.; Rutherford, P.; Gemmel, L. Validation of a modified Early Warning Score in medical admissions. QJM 2001, 94, 521–526. [Google Scholar] [CrossRef] [Green Version]
- Aygun, H.; Eraybar, S. The role of emergency department triage early warning score (TREWS) and modified early warning score (MEWS) to predict in-hospital mortality in COVID-19 patients. Ir. J. Med. Sci. 2021, 191, 997–1003. [Google Scholar] [CrossRef]
- Haimovich, A.D.; Ravindra, N.G.; Stoytchev, S.; Young, H.P.; Wilson, F.P.; van Dijk, D.; Schulz, W.L.; Taylor, R.A. Development and Validation of the Quick COVID-19 Severity Index: A Prognostic Tool for Early Clinical Decompensation. Ann. Emerg. Med. 2020, 76, 442–453. [Google Scholar] [CrossRef]
- Rodriguez-Nava, G.; Yanez-Bello, M.A.; Trelles-Garcia, D.P.; Chung, C.W.; Friedman, H.J.; Hines, D.W. Performance of the quick COVID-19 severity index and the Brescia-COVID respiratory severity scale in hospitalized patients with COVID-19 in a community hospital setting. Int. J. Infect. Dis. 2020, 102, 571–576. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Tuty Kuswardhani, R.A.; Henrina, J.; Pranata, R.; Anthonius Lim, M.; Lawrensia, S.; Suastika, K. Charlson comorbidity index and a composite of poor outcomes in COVID-19 patients: A systematic review and meta-analysis. Diabetes Metab. Syndr. 2020, 14, 2103–2109. [Google Scholar] [CrossRef]
- Fine, M.J.; Auble, T.E.; Yealy, D.M.; Hanusa, B.H.; Weissfeld, L.A.; Singer, D.E.; Coley, C.M.; Marrie, T.J.; Kapoor, W.N. A prediction rule to identify low-risk patients with community-acquired pneumonia. N. Engl. J. Med. 1997, 336, 243–250. [Google Scholar] [CrossRef]
- Guo, L.; Wei, D.; Zhang, X.; Wu, Y.; Li, Q.; Zhou, M.; Qu, J. Clinical Features Predicting Mortality Risk in Patients With Viral Pneumonia: The MuLBSTA Score. Front. Microbiol. 2019, 10, 2752. [Google Scholar] [CrossRef] [Green Version]
- Iijima, Y.; Okamoto, T.; Shirai, T.; Mitsumura, T.; Sakakibara, R.; Honda, T.; Ishizuka, M.; Tateishi, T.; Tamaoka, M.; Aiboshi, J.; et al. MuLBSTA score is a useful tool for predicting COVID-19 disease behavior. J. Infect. Chemother. 2020, 27, 284–290. [Google Scholar] [CrossRef]
- Ma, B.; Gong, J.; Yang, Y.; Yao, X.; Deng, X.; Chen, X. Applicability of MuLBSTA scoring system as diagnostic and prognostic role in early warning of severe COVID-19. Microb. Pathog. 2020, 150, 104706. [Google Scholar] [CrossRef]
- Taylor, F.B.; Toh, C.H.; Hoots, W.K.; Wada, H.; Levi, M.; Scientific Subcommittee on Disseminated Intravascular Coagulation (DIC) of the International Society on Thrombosis and Haemostasis (ISTH). Towards definition, clinical and laboratory criteria, and a scoring system for disseminated intravascular coagulation. Thromb. Haemost. 2001, 86, 1327–1330. [Google Scholar] [CrossRef] [Green Version]
- Anwar, N.; Tashfeen, S.; Akhtar, F.; Noor, A.; Khan, S.A.; Omair, A. Can disseminated intravascular coagulation scores predict mortality in COVID-19 patients? J. Taibah Univ. Med. Sci. 2021, 16, 596–604. [Google Scholar] [CrossRef]
- Liang, W.; Liang, H.; Ou, L.; Chen, B.; Chen, A.; Li, C.; Li, Y.; Guan, W.; Sang, L.; Lu, J.; et al. Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients With COVID-19. JAMA Intern. Med. 2020, 180, 1081–1089. [Google Scholar] [CrossRef]
- Riley, J.M.; Moeller, P.J.; Crawford, A.G.; Schaefer, J.W.; Cheney-Peters, D.R.; Venkataraman, C.M.; Li, C.J.; Smaltz, C.M.; Bradley, C.G.; Lee, C.Y.; et al. External validation of the COVID-19 4C mortality score in an urban United States cohort. Am. J. Med. Sci. 2022, 364, 409–413. [Google Scholar] [CrossRef]
- Akilli, I.K.; Bilge, M.; Guz, A.U.; Korkusuz, R.; Unlu, E.C.; Yasar, K.K. Comparison of Pneumonia Severity Indices, qCSI, 4C-Mortality Score and qSOFA in Predicting Mortality in Hospitalized Patients with COVID-19 Pneumonia. J. Pers. Med. 2022, 12, 801. [Google Scholar] [CrossRef]
- Hanley, J.A.; McNeil, B.J. A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology 1983, 148, 839–843. [Google Scholar] [CrossRef] [Green Version]
- King, J.T., Jr.; Yoon, J.S.; Bredl, Z.M.; Habboushe, J.P.; Walker, G.A.; Rentsch, C.T.; Tate, J.P.; Kashyap, N.M.; Hintz, R.C.; Chopra, A.P. Accuracy of the Veterans Health Administration COVID-19 (VACO) Index for predicting short-term mortality among 1307 Yale New Haven Hospital inpatients and 427,224 Medicare patients. J. Epidemiol. Community Health 2021, 76, 254–260. [Google Scholar] [CrossRef]
- Zheng, Z.; Peng, F.; Xu, B.; Zhao, J.; Liu, H.; Peng, J.; Li, Q.; Jiang, C.; Zhou, Y.; Liu, S.; et al. Risk factors of critical & mortal COVID-19 cases: A systematic literature review and meta-analysis. J. Infect. 2020, 81, e16–e25. [Google Scholar] [CrossRef]
- Parohan, M.; Yaghoubi, S.; Seraji, A.; Javanbakht, M.H.; Sarraf, P.; Djalali, M. Risk factors for mortality in patients with Coronavirus disease 2019 (COVID-19) infection: A systematic review and meta-analysis of observational studies. Aging Male 2020, 23, 1416–1424. [Google Scholar] [CrossRef]
- Udomkarnjananun, S.; Kerr, S.J.; Townamchai, N.; Susantitaphong, P.; Tulvatana, W.; Praditpornsilpa, K.; Eiam-Ong, S.; Avihingsanon, Y. Mortality risk factors of COVID-19 infection in kidney transplantation recipients: A systematic review and meta-analysis of cohorts and clinical registries. Sci. Rep. 2021, 11, 20073. [Google Scholar] [CrossRef]
- Park, M.; Hur, M.; Kim, H.; Lee, C.H.; Lee, J.H.; Kim, H.W.; Nam, M. Prognostic Utility of Procalcitonin, Presepsin, and the VACO Index for Predicting 30-day Mortality in Hospitalized COVID-19 Patients. Ann. Lab. Med. 2022, 42, 406–414. [Google Scholar] [CrossRef]
- Andrianto; Al-Farabi, M.J.; Nugraha, R.A.; Marsudi, B.A.; Azmi, Y. Biomarkers of endothelial dysfunction and outcomes in coronavirus disease 2019 (COVID-19) patients: A systematic review and meta-analysis. Microvasc. Res. 2021, 138, 104224. [Google Scholar] [CrossRef]
- Kefale, B.; Tegegne, G.T.; Degu, A.; Tadege, M.; Tesfa, D. Prevalence and Risk Factors of Thromboembolism among Patients With Coronavirus Disease-19: A Systematic Review and Meta-Analysis. Clin. Appl. Thromb./Haemost. 2020, 26, 1–13. [Google Scholar] [CrossRef]
- Jin, S.; Jin, Y.; Xu, B.; Hong, J.; Yang, X. Prevalence and Impact of Coagulation Dysfunction in COVID-19 in China: A Meta-Analysis. Thromb. Haemost. 2020, 120, 1524–1535. [Google Scholar] [CrossRef]
- Elec, F.I.; Bolboacă, S.D.; Muntean, A.; Elec, A.D.; Cismaru, C.; Lupşe, M.; Oltean, M. Comparing the First and Second Wave of COVID-19 in Kidney Transplant Recipients: An East-European Perspective. Eur. Surg. Res. 2022, 63, 25–32. [Google Scholar] [CrossRef]
- Azzi, Y.; Parides, M.; Alani, O.; Loarte-Campos, P.; Bartash, R.; Forest, S.; Colovai, A.; Ajaimy, M.; Liriano-Ward, L.; Pynadath, C.; et al. COVID-19 infection in kidney transplant recipients at the epicenter of pandemics. Kidney Int. 2020, 98, 1559–1567. [Google Scholar] [CrossRef]
- Villanego, F.; Mazuecos, A.; Pérez-Flores, I.M.; Moreso, F.; Andrés, A.; Jiménez-Martín, C.; Molina, M.; Canal, C.; Sánchez-Cámara, L.A.; Zárraga, S.; et al. Predictors of severe COVID-19 in kidney transplant recipients in the different epidemic waves: Analysis of the Spanish Registry. Am. J. Transplant. 2021, 21, 2573–2582. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Variables | Study Sample (N = 65) |
|---|---|
| Age (years) | 57 (45–66) |
| Female sex | 43 (66.2%) |
| Systolic blood pressure (mmHg) | 130 (126–140) |
| Diastolic blood pressure (mmHg) | 78 (75–89) |
| Heart rate (/min) | 80 (76–93) |
| SpO2 (%) | 96 (95–96) |
| Transplant duration (years) | 8 (2–11) |
| Single-dose Pfizer-BioNTech COVID-19 vaccination | 3 (4.6%) |
| Double-dose Pfizer-BioNTech COVID-19 vaccination | 11 (16.9%) |
| Symptom duration upon hospital admission (days) | 7 (3–11) |
| Follow-up (days) | 38 (35–42) |
| Comorbidities | |
| Arterial hypertension | 53 (81.5%) |
| Diabetes mellitus | 18 (27.7%) |
| Chronic heart failure | 5 (7.7%) |
| Active smoking | 5 (7.7%) |
| Atrial fibrillation | 7 (10.8%) |
| Prior AMI | 7 (10.8%) |
| Prior CVI | 6 (9.2%) |
| PAD | 10 (15.4%) |
| COPD/asthma | 4 (6.2%) |
| Laboratory parameters | |
| WBC (×109/L) | 6.5 (5.3–8.9) |
| RBC (×1012/L) | 4.7 (4.4–4.8) |
| Hgb (g/L) | 128.5 (125.0–134.3) |
| Platelets (×103/L) | 240.1 (198.0–262.3) |
| CRP (mmol/L; maximal values) | 72.6 (34.8–121.8) |
| BUN (mmol/L) | 9.8 (8.0–15.3) |
| Creatinine (μmol/L) | 128.5 (111.5–215.0) |
| eGFR (ml/min/1.73 m2) | 44.5 (24.8–63.8) |
| D-dimers (mmol/L) | 0.8 (0.6–1.7) |
| Chronic immunosuppressive therapy | |
| Mycophenolate Mofetil | 58 (89.2%) |
| Azathioprine | 1 (1.5%) |
| Cyclosporine | 20 (30.8%) |
| Tacrolimus | 36 (55.4%) |
| Everolimus | 8 (12.3%) |
| Sirolimus | 3 (4.6%) |
| Prednisone | 65 (100.0%) |
| COVID-19-related therapy | |
| Reconvalescent plasma | 6 (9.2%) |
| Casirivimab/Imdevimab | 2 (3.1%) |
| Remdesivir | 44 (67.7%) |
| Oxygen therapy | 24 (36.9%) |
| Transplant-related therapy | |
| Mycophenolate + Tacrolimus + Prednison | 34 (52.3%) |
| Mycophenolate + Cyclosporine + Prednison | 18 (27.7%) |
| Mycophenolate + Everolimus + Prednison | 4 (6.3%) |
| Mycophenolate + Sirolimus + Prednison | 3 (4.6%) |
| Tacrolimus + Everolimus + Prednison | 3 (4.6%) |
| Cyclosporine + Everolimus + Prednison | 1 (1.5%) |
| Azathioprine + Prednison | 1 (1.5%) |
| Cyclosporine + Prednison | 1 (1.5%) |
| Transplant-related therapy in the setting of COVID-19 | |
| Corticosteroid dose increase | 65 (100.0%) |
| Calcineurin dose modification | |
| No dose modification | 38 (58.5%) |
| Dose reduction | 24 (36.9%) |
| Drug removal | 3 (4.6%) |
| Antimetabolite dose modification | |
| No dose modification | 6 (9.2%) |
| Dose reduction | 24 (36.9%) |
| Drug removal | 35 (53.8%) |
| Variables | Survival Group (N = 53) | Mortality Group (N = 12) | p-Value |
|---|---|---|---|
| Age (years) | 61 (51–68) | 73 (62–75) | 0.063 |
| Female sex | 18 (34.0%) | 4 (33.3%) | 0.967 |
| Systolic blood pressure (mmHg) | 135 (130–150) | 120 (117–126) | 0.012 |
| Diastolic blood pressure (mmHg) | 80 (75–90) | 73 (70–80) | 0.173 |
| Heart rate (/min) | 80 (75–90) | 89 (70–107) | 0.022 |
| SpO2 (%) | 96 (95–96) | 88 (86–96) | <0.001 |
| Transplant duration (years) | 6 (2–10) | 10 (2–22) | 0.157 |
| Symptom duration upon hospital admission (days) | 5 (3–10) | 3 (1–8) | 0.195 |
| Acute kidney injury during follow-up | 2 (3.8%) | 6 (50.0%) | <0.001 |
| Follow-up (days) | 40 (37–43) | 20 (14–35) | <0.001 |
| Comorbidities | |||
| Arterial hypertension | 45 (84.9%) | 8 (66.7%) | 0.141 |
| Diabetes mellitus | 13 (24.5%) | 5 (41.7%) | 0.231 |
| Chronic heart failure | 2 (3.8%) | 3 (25.0%) | 0.013 |
| Active smoking | 5 (9.4%) | 0 (0.0%) | 0.268 |
| Atrial fibrillation | 6 (11.3%) | 1 (8.3%) | 0.763 |
| Prior AMI | 6 (11.3%) | 1 (8.3%) | 0.763 |
| Prior CVI | 4 (7.5%) | 2 (16.7%) | 0.324 |
| PAD | 7 (13.2%) | 3 (25.0%) | 0.307 |
| COPD/asthma | 4 (7.5%) | 0 (0.0%) | 0.326 |
| Laboratory parameters | |||
| WBC (×109/L) | 6.6 (5.2–8.1) | 7.9 (3.9–9.9) | 0.279 |
| RBC (×1012/L) | 4.7 (4.3–5.0) | 4.3 (3.8–4.7) | 0.089 |
| Hgb (g/L) | 133.0 (124.0–151.1) | 127.5 (109.3–139.0) | 0.059 |
| Platelets (×103/L) | 213.0 (175.0–251.0) | 204.5 (168.8–246.3) | 0.618 |
| CRP (mmol/L; maximal values) | 72.6 (22.2–75.5) | 102.8 (34.0–265.8) | 0.003 |
| BUN (mmol/L) | 8.6 (6.6–12.7) | 9.9 (6.0–17.0) | 0.076 |
| Creatinine (μmol/L) | 134.5 (108.0–178.0) | 147.0 (103.5–228.8) | 0.187 |
| eGFR (mL/min/1.73 m2) | 42.5 (32.8–66.7) | 37.5 (26.2–59.4) | 0.264 |
| D-dimers (mmol/L) | 0.8 (0.5–1.1) | 0.8 (0.7–1.5) | 0.474 |
| Risk Scores | 30-Day Post-Discharge Mortality | |||
|---|---|---|---|---|
| HR (95% CI) | p-Value * | Harrell’s C Concordance Index | Somers’ D | |
| MEWS risk score | 1.65 (1.21–2.25) | 0.002 | 0.694 | 0.388 |
| qCSI risk score | 1.32 (1.15–1.52) | <0.001 | 0.809 | 0.618 |
| VACO risk score | 1.00 (0.94–1.06) | 0.904 | 0.427 | −0.146 |
| PSI/PORT risk score | 1.04 (1.02–1.07) | 0.001 | 0.833 | 0.665 |
| CCI risk score | 1.79 (1.13–2.83) | 0.013 | 0.785 | 0.570 |
| MuLBSTA risk score | 1.31 (1.05–1.64) | 0.017 | 0.678 | 0.356 |
| ISTH-DIC risk score | 1.72 (0.94–3.13) | 0.077 | 0.645 | 0.289 |
| COVID-GRAM risk score | 1.03 (1.01–1.06) | 0.004 | 0.748 | 0.496 |
| 4C Mortality risk score | 1.79 (1.40–2.31) | <0.001 | 0.914 | 0.829 |
| Risk Scores | 30-Day Post-Discharge Mortality | |
|---|---|---|
| aHR (95% CI) | p-Value * | |
| MEWS risk score | 1.56 (0.98–2.49) | 0.059 |
| qCSI risk score | 1.33 (1.11–1.59) | 0.002 |
| VACO risk score | 1.00 (0.99–1.01) | 0.542 |
| PSI/PORT risk score | 1.04 (1.01–1.07) | 0.012 |
| CCI risk score | 1.64 (0.94–2.84) | 0.080 |
| MuLBSTA risk score | 1.36 (1.01–1.85) | 0.046 |
| ISTH-DIC risk score | 1.40 (0.67–2.94) | 0.376 |
| COVID-GRAM risk score | 1.03 (1.00–1.07) | 0.095 |
| 4C Mortality risk score | 1.93 (1.45–2.57) | <0.001 |
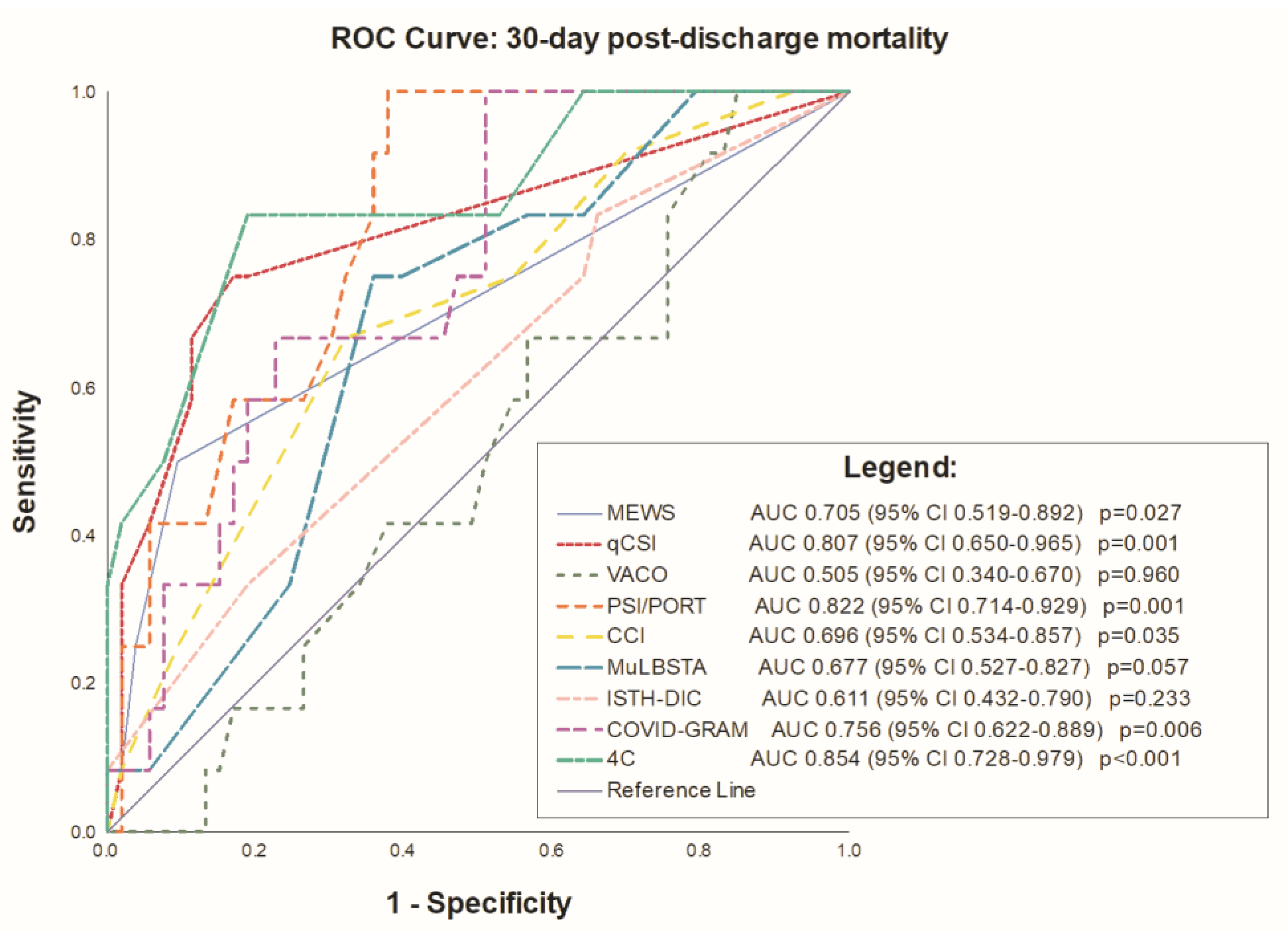
| Risk Scores | C-Statistic (95% CI) | p-Value | Sensitivity/Specificity | Youden’s Index |
|---|---|---|---|---|
| MEWS risk score | 0.705 (0.519–0.892) | 0.027 | 50.0/90.6 | >1 |
| qCSI risk score | 0.807 (0.650–0.965) | 0.001 | 75.0/83.0 | >2 |
| VACO risk score | 0.505 (0.340–0.670) | 0.960 | 100.0/15.1 | >3.6 |
| PSI/PORT risk score | 0.822 (0.714–0.929) | 0.001 | 100.0/62.3 | >82 |
| CCI risk score | 0.696 (0.534–0.857) | 0.035 | 66.7/67.9 | >5 |
| MuLBSTA risk score | 0.677 (0.527–0.827) | 0.057 | 75.0/64.2 | >10 |
| ISTH-DIC risk score | 0.611 (0.432–0.790) | 0.233 | 83.3/34.0 | >1 |
| COVID-GRAM risk score | 0.756 (0.622–0.889) | 0.006 | 100.0/49.1 | >125 |
| 4C Mortality risk score | 0.854 (0.728–0.979) | <0.001 | 83.3/81.1 | >10 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Domjanović, J.; Domjanović Škopinić, T.; Matetic, A. Association of Different Risk Scores and 30-Day Mortality in Kidney Transplant Recipients with COVID-19. Medicina 2023, 59, 657. https://doi.org/10.3390/medicina59040657
Domjanović J, Domjanović Škopinić T, Matetic A. Association of Different Risk Scores and 30-Day Mortality in Kidney Transplant Recipients with COVID-19. Medicina. 2023; 59(4):657. https://doi.org/10.3390/medicina59040657
Chicago/Turabian StyleDomjanović, Josipa, Tea Domjanović Škopinić, and Andrija Matetic. 2023. "Association of Different Risk Scores and 30-Day Mortality in Kidney Transplant Recipients with COVID-19" Medicina 59, no. 4: 657. https://doi.org/10.3390/medicina59040657