

A Systematic Review of Clinical Pharmacokinetics of Inhaled Antiviral

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Identification of the Research Question
2.2. Literature Search
2.3. Inclusion and Exclusion Criteria
2.4. Study Selection
2.5. Data Extraction
2.6. Quality Assessment
2.7. Data Synthesis and Reporting
3. Results
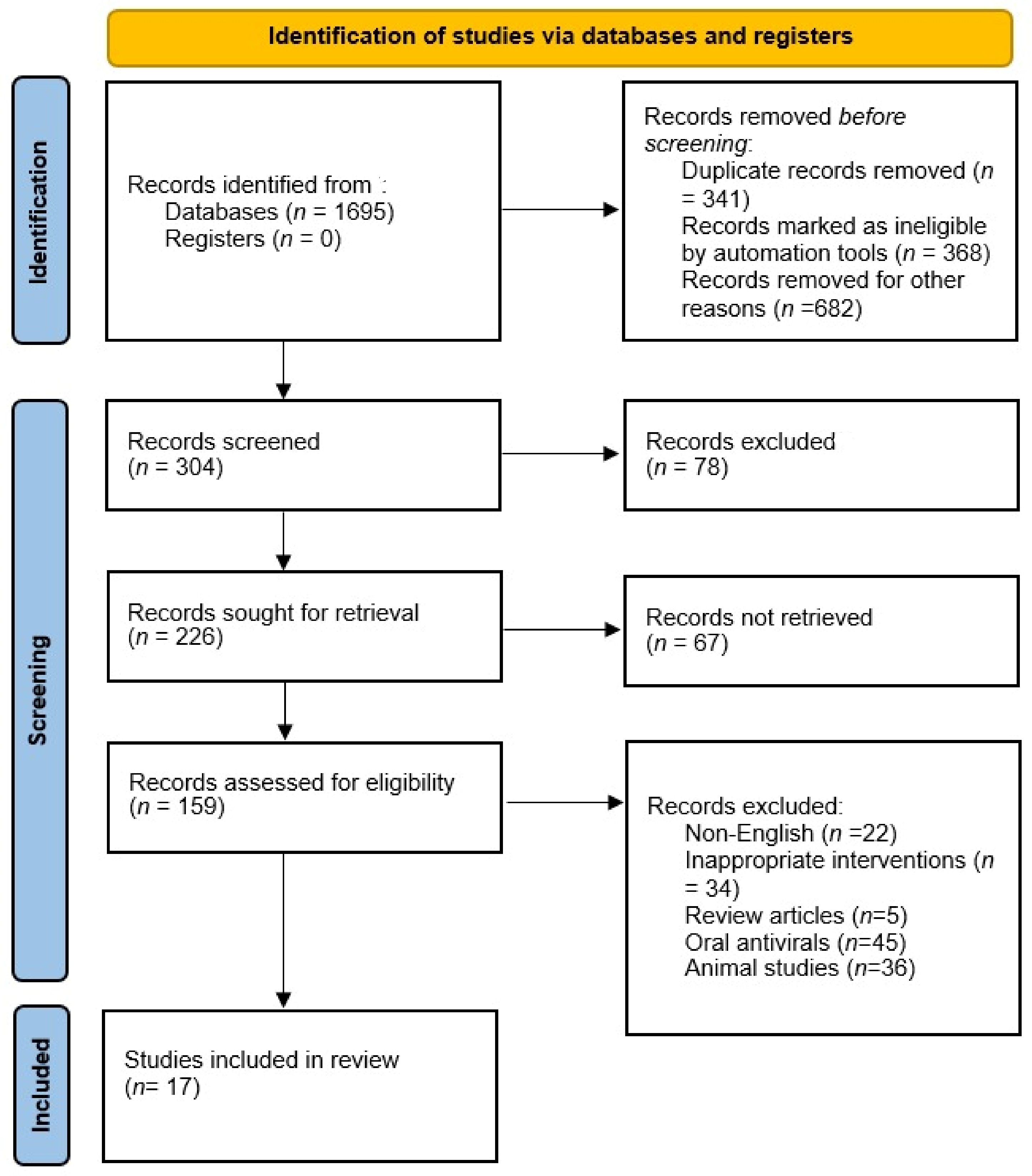
3.1. Literature Search
3.2. Characteristics of Studies
3.3. Quality Assessment of the Studies
3.4. Zanamivir
3.5. Laninamivir
3.6. Ribavirin
3.7. Rimantadine
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Stockmann, C.; Roberts, J.K.; Yellepeddi, V.K.; Sherwin, C.M.T. Clinical Pharmacokinetics of Inhaled Antimicrobials. Clin. Pharmacokinet. 2015, 54, 473–492. [Google Scholar] [CrossRef]
- Dolovich, M.B.; Dhand, R. Aerosol drug delivery: Developments in device design and clinical use. Lancet 2011, 377, 1032–1045. [Google Scholar] [CrossRef]
- Hickey, A.J. Emerging trends in inhaled drug delivery. Adv. Drug Deliv. Rev. 2020, 157, 63–70. [Google Scholar] [CrossRef]
- Anderson, S.; Atkins, P.; Bäckman, P.; Cipolla, D.; Clark, A.; Daviskas, E.; Disse, B.; Entcheva-Dimitrov, P.; Fuller, R.; Gonda, I.; et al. Inhaled Medicines: Past, Present, and Future. Pharmacol. Rev. 2022, 74, 48–118. [Google Scholar] [CrossRef]
- Newman, S.P. Drug delivery to the lungs: Challenges and opportunities. Ther. Deliv. 2017, 8, 647–661. [Google Scholar] [CrossRef]
- Ibrahim, M.; Verma, R.; Garcia-Contreras, L. Inhalation drug delivery devices: Technology update. Med. Devices 2015, 8, 131–139. [Google Scholar]
- Heyder, J. Deposition of inhaled particles in the human respiratory tract and consequences for regional targeting in respiratory drug delivery. Proc. Am. Thorac. Soc. 2004, 1, 315–320. [Google Scholar] [CrossRef]
- Peng, A.W.; Hussey, E.K.; Moore, K.H.P.; Peng, A.W. A Population Pharmacokinetic Analysis of Zanamivir in Subjects with Experimental and Naturally Occurring Influenza: Effects of Formulation and Route of Administration. J. Clin. Pharmacol. 2000, 40, 242–249. [Google Scholar] [CrossRef]
- Groneberg, D.; Witt, C.; Wagner, U.; Chung, K.; Fischer, A. Fundamentals of pulmonary drug delivery. Respir. Med. 2003, 97, 382–387. [Google Scholar] [CrossRef] [Green Version]
- Ishizuka, H.; Toyama, K.; Yoshiba, S.; Okabe, H.; Furuie, H. Intrapulmonary Distribution and Pharmacokinetics of Laninamivir, a Neuraminidase Inhibitor, after a Single Inhaled Administration of Its Prodrug, Laninamivir Octanoate, in Healthy Volunteers. Antimicrob. Agents Chemother. 2012, 56, 3873–3878. [Google Scholar] [CrossRef] [Green Version]
- Labiris, N.R.; Dolovich, M.B. Pulmonary drug delivery. Part II: The role of inhalant delivery devices and drug formulations in therapeutic effectiveness of aerosolized medications. Br. J. Clin. Pharmacol. 2003, 56, 600–612. [Google Scholar] [CrossRef] [Green Version]
- Ibrahim, M.; Garcia-Contreras, L. Mechanisms of absorption and elimination of drugs administered by inhalation. Ther. Deliv. 2013, 4, 1027–1045. [Google Scholar] [CrossRef] [PubMed]
- Weller, S.; Jones, L.S.; Lou, Y.; Piscitelli, S.; Peppercorn, A.; Ng-Cashin, J. Safety, Tolerability and Pharmacokinetics of Orally Inhaled Zanamivir: A Randomized Study Comparing Rotacap/Rotahaler and Rotadisk/Diskhaler in Healthy Adults; SAGE Publications: London, UK, 2013. [Google Scholar]
- Sahin, G.; Akbal-Dagistan, O.; Culha, M.; Erturk, A.; Basarir, N.S.; Sancar, S.; Yildiz-Pekoz, A. Antivirals and the Potential Benefits of Orally Inhaled Drug Administration in COVID-19 Treatment. J. Pharm. Sci. 2022, 111, 2652–2661. [Google Scholar] [CrossRef]
- Bodier-Montagutelli, E.; Mayor, A.; Vecellio, L.; Respaud, R.; Heuzé-Vourc’h, N. Designing inhaled protein therapeutics for topical lung delivery: What are the next steps? Expert Opin. Drug Deliv. 2018, 15, 729–736. [Google Scholar] [CrossRef] [PubMed]
- Liao, Q.; Yuan, S.; Cao, J.; Tang, K.; Qiu, Y.; Seow, H.C.; Man, R.C.H.; Shao, Z.; Huang, Y.; Liang, R.; et al. Inhaled Dry Powder Formulation of Tamibarotene, a Broad-Spectrum Antiviral against Respiratory Viruses Including SARS-CoV-2 and Influenza Virus. Adv. Ther. 2021, 4, 2100059. [Google Scholar] [CrossRef]
- Abdellatif, A.A.; Tawfeek, H.M.; Abdelfattah, A.; Batiha, G.E.-S.; Hetta, H.F. Recent updates in COVID-19 with emphasis on inhalation therapeutics: Nanostructured and targeting systems. J. Drug Deliv. Sci. Technol. 2021, 63, 102435. [Google Scholar] [CrossRef] [PubMed]
- Cass, L.M.; Efthymiopoulos, C.; Bye, A. Pharmacokinetics of zanamivir after intravenous, oral, inhaled or intranasal administration to healthy volunteers. Clin. Pharmacokinet. 1999, 36, 1–11. [Google Scholar] [CrossRef]
- Cass, L.M.R.; Brown, J.; Pickford, M.; Fayinka, S.; Newman, S.P.; Johansson, C.J.; Bye, A. Pharmacoscintigraphic Evaluation of Lung Deposition of Inhaled Zanamivir in Healthy Volunteers. Clin. Pharmacokinet. 1999, 36, 21–31. [Google Scholar] [CrossRef]
- Ishizuka, H.; Yoshiba, S.; Yoshihara, K.; Okabe, H. Assessment of the Effects of Renal Impairment on the Pharmacokinetic Profile of Laninamivir, a Novel Neuraminidase Inhibitor, After a Single Inhaled Dose of Its Prodrug, CS-8958. J. Clin. Pharmacol. 2011, 51, 243–251. [Google Scholar] [CrossRef]
- Ishizuka, H.; Yoshiba, S.; Okabe, H.; Yoshihara, K. Clinical Pharmacokinetics of Laninamivir, a Novel Long-Acting Neuraminidase Inhibitor, After Single and Multiple Inhaled Doses of Its Prodrug, CS-8958, in Healthy Male Volunteers. J. Clin. Pharmacol. 2010, 50, 1319–1329. [Google Scholar] [CrossRef]
- Yoshiba, S.; Okabe, H.; Ishizuka, H. Pharmacokinetics of laninamivir after a single administration of its prodrug, laninamivir octanoate, a long-acting neuraminidase inhibitor, using an easy-to-use inhaler in healthy volunteers. J. Bioequiv. Availab. 2011, 3, 001–004. [Google Scholar] [CrossRef] [Green Version]
- Yoshihara, K.; Ishizuka, H.; Kubo, Y. Population Pharmacokinetics of Laninamivir and Its Prodrug Laninamivir Octanoate in Healthy Subjects and in Adult and Pediatric Patients with Influenza Virus Infection. Drug Metab. Pharmacokinet. 2013, 28, 416–426. [Google Scholar] [CrossRef]
- Couroux, P.; Brkovic, A.; Vittitow, J.L.; Israel, R.J.; Pamidi, C.; Patel, J.; Barakat, M. A randomized, placebo-controlled study to evaluate safety and pharmacokinetics of inhaled ribavirin. Clin. Transl. Sci. 2022, 15, 2159–2171. [Google Scholar] [CrossRef] [PubMed]
- Dumont, E.F.; Oliver, A.J.; Ioannou, C.; Billiard, J.; Dennison, J.; Van Den Berg, F.; Yang, S.; Chandrasekaran, V.; Young, G.C.; Lahiry, A.; et al. A Novel Inhaled Dry-Powder Formulation of Ribavirin Allows for Efficient Lung Delivery in Healthy Participants and Those with Chronic Obstructive Pulmonary Disease in a Phase 1 Study. Antimicrob. Agents Chemother. 2020, 64, e02267-19. [Google Scholar] [CrossRef] [Green Version]
- Atmar, R.L.; Greenberg, S.B.; Quarles, J.M.; Wilson, S.Z.; Tyler, B.; Feldman, S.; Couch, R.B. Safety and pharmacokinetics of rimantadine small-particle aerosol. Antimicrob. Agents Chemother. 1990, 34, 2228–2233. [Google Scholar] [CrossRef] [Green Version]
- Englund, J.A.; Piedra, P.A.; Jefferson, L.S.; Wilson, S.Z.; Taber, L.H.; Gilbert, B.E. High-dose, short-duration ribavirin aerosol therapy in children with suspected respiratory syncytial virus infection. J. Pediatr. 1990, 117, 313–320. [Google Scholar] [CrossRef]
- Linn, W.S.; Gong, H.; Anderson, K.R.; Clark, K.W.; Shamoo, D.A. Exposures of Health-Care Workers to Ribavirin Aerosol: A Pharmacokinetic Study. Arch. Environ. Health Int. J. 1995, 50, 445–451. [Google Scholar] [CrossRef]
- Toyama, K.; Furuie, H.; Ishizuka, H. Safety and Pharmacokinetics of Nebulized Laninamivir Octanoate, A Long Acting Neuraminidase Inhibitor, In Healthy Subjects. Clin. Ther. 2017, 39, e25–e26. [Google Scholar] [CrossRef] [Green Version]
- Peng, A.W.; Hussey, E.K.; Rosolowski, B.; Blumer, J.L. Pharmacokinetics and tolerability of a single inhaled dose of zanamivir in children. Curr. Ther. Res. 2000, 61, 36–46. [Google Scholar] [CrossRef]
- Shelton, M.J.; Lovern, M.; Ng-Cashin, J.; Jones, L.; Gould, E.; Gauvin, J.; Rodvold, K.A. Zanamivir Pharmacokinetics and Pulmonary Penetration into Epithelial Lining Fluid following Intravenous or Oral Inhaled Administration to Healthy Adult Subjects. Antimicrob. Agents Chemother. 2011, 55, 5178–5184. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yu, R.-H.; Cao, Y.-X. A method to determine pharmacokinetic parameters based on andante constant-rate intravenous infusion. Sci. Rep. 2017, 7, 13279. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berkenfeld, K.; Lamprecht, A.; McConville, J.T. Devices for Dry Powder Drug Delivery to the Lung. AAPS PharmSciTech 2015, 16, 479–490. [Google Scholar] [CrossRef] [PubMed]
- Bradley, B.T.; Bryan, A. Emerging respiratory infections: The infectious disease pathology of SARS, MERS, pandemic influenza, and Legionella. Semin. Diagn. Pathol. 2019, 36, 152–159. [Google Scholar] [CrossRef] [PubMed]
- Bloom, D.E.; Cadarette, D. Infectious Disease Threats in the Twenty-First Century: Strengthening the Global Response. Front. Immunol. 2019, 10, 549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Clayville, L.R. Influenza update: A review of currently available vaccines. P T A Peer-Rev. J. Formul. Manag. 2011, 36, 659–684. [Google Scholar]
- Wang, K.; Shun-Shin, M.; Gill, P.; Perera, R.; Harnden, A. Neuraminidase inhibitors for preventing and treating influenza in children (published trials only). Cochrane Database Syst. Rev. 2012, 2012, CD002744. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mifsud, E.J.; Hayden, F.G.; Hurt, A.C. Antivirals targeting the polymerase complex of influenza viruses. Antivir. Res. 2019, 169, 104545. [Google Scholar] [CrossRef]
- Świerczyńska, M.; Mirowska-Guzel, D.M.; Pindelska, E. Antiviral Drugs in Influenza. Int. J. Environ. Res. Public Health 2022, 19, 3018. [Google Scholar] [CrossRef]
- Chairat, K.; Tarning, J.; White, N.J.; Lindegardh, N. Pharmacokinetic Properties ofAnti-Influenza Neuraminidase Inhibitors. J. Clin. Pharmacol. 2013, 53, 119–139. [Google Scholar] [CrossRef]
- Feng, E.; Ye, D.; Li, J.; Zhang, D.; Wang, J.; Zhao, F.; Hilgenfeld, R.; Zheng, M.; Jiang, H.; Liu, H. Recent Advances in Neuraminidase Inhibitor Development as Anti-influenza Drugs. Chemmedchem 2012, 7, 1527–1536. [Google Scholar] [CrossRef]
- Yamashita, M. Laninamivir and its Prodrug, CS-8958: Long-Acting Neuraminidase Inhibitors for the Treatment of Influenza. Antivir. Chem. Chemother. 2010, 21, 71–84. [Google Scholar] [CrossRef] [PubMed]
- Sriwilaijaroen, N.; Vavricka, C.J.; Kiyota, H.; Suzuki, Y. Influenza A Virus Neuraminidase Inhibitors. In Glycovirology: Methods and Protocols; Springer: Berlin/Heidelberg, Germany, 2022; pp. 321–353. [Google Scholar]
- Hussain, M.; Galvin, H.D.; Haw, T.Y.; Nutsford, A.N.; Husain, M. Drug resistance in influenza A virus: The epidemiology and management. Infect. Drug Resist. 2017, 10, 121–134. [Google Scholar] [CrossRef] [Green Version]
- Zaraket, H.; Saito, R. Japanese Surveillance Systems and Treatment for Influenza. Curr. Treat. Options Infect. Dis. 2016, 8, 311–328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pavia, A.T. Viral Infections of the Lower Respiratory Tract: Old Viruses, New Viruses, and the Role of Diagnosis. Clin. Infect. Dis. 2011, 52 (Suppl. S4), S284–S289. [Google Scholar] [CrossRef] [PubMed]
- Azzari, C.; Baraldi, E.; Bonanni, P.; Bozzola, E.; Coscia, A.; Lanari, M.; Manzoni, P.; Mazzone, T.; Sandri, F.; Lisi, G.C.; et al. Epidemiology and prevention of respiratory syncytial virus infections in children in Italy. Ital. J. Pediatr. 2021, 47, 198. [Google Scholar] [CrossRef] [PubMed]
- Turner, T.L.; Kopp, B.T.; Paul, G.; Landgrave, L.C.; Hayes, N.; Thompson, R. Respiratory syncytial virus: Current and emerging treatment options. Clin. Outcomes Res. 2014, 6, 217–225. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, W.J.; Hall, C.B.; Welliver, R.; Simoes, E.A.; Ryan, M.E.; Stutman, H.; Johnson, G.; Van Dyke, R.; Groothuis, J.R.; Arrobio, J.; et al. Efficacy and safety of aerosolized ribavirin in young children hospitalized with influenza: A double-blind, multicenter, placebo-controlled trial. J. Pediatr. 1994, 125, 129–135. [Google Scholar] [CrossRef]
- Englund, J.A. Antiviral therapy of influenza. Semin. Pediatr. Infect. Dis. 2002, 13, 120–128. [Google Scholar] [CrossRef]
- Venisse, N.; Peytavin, G.; Bouchet, S.; Gagnieu, M.C.; Garraffo, R.; Guilhaumou, R.; Solas, C.; Monitoring, S.T.D. ANRS-AC43 Clinical Pharmacology Committee Concerns about pharmacokinetic (PK) and pharmacokinetic-pharmacodynamic (PK-PD) studies in the new therapeutic area of COVID-19 infection. Antivir. Res. 2020, 181, 104866. [Google Scholar] [CrossRef]
- Nyström, K.; Waldenström, J.; Tang, K.-W.; Lagging, M. Ribavirin: Pharmacology, multiple modes of action and possible future perspectives. Future Virol. 2019, 14, 153–160. [Google Scholar] [CrossRef] [Green Version]
- Glue, P.; Schenker, S.; Gupta, S.; Clement, R.P.; Zambas, D.; Salfi, M. The single dose pharmacokinetics of ribavirin in subjects with chronic liver disease. Br. J. Clin. Pharmacol. 2000, 49, 417–421. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nainwal, N. Treatment of respiratory viral infections through inhalation therapeutics: Challenges and opportunities. Pulm. Pharmacol. Ther. 2022, 77, 102170. [Google Scholar] [CrossRef] [PubMed]
- Restrepo, M.I.; Keyt, H.; Reyes, L.F. Aerosolized Antibiotics. Respir. Care 2015, 60, 762–773. [Google Scholar] [CrossRef] [Green Version]
- Hayden, F.G.; Zylidnikov, D.; Iljenko, V.; Padolka, Y. Comparative therapeutic effect of aerosolized and oral rimantadine HC1 in experimental human influenza A virus infection. Antivir. Res. 1982, 2, 147–153. [Google Scholar] [CrossRef]
- Hayden, F.G.; Minocha, A.; A Spyker, D.; E Hoffman, H. Comparative single-dose pharmacokinetics of amantadine hydrochloride and rimantadine hydrochloride in young and elderly adults. Antimicrob. Agents Chemother. 1985, 28, 216–221. [Google Scholar] [CrossRef] [Green Version]
- Velkov, T.; Abdul Rahim, N.; Zhou, Q.T.; Chan, H.K.; Li, J. Inhaled anti-infective chemotherapy for respiratory tract infections: Successes, challenges and the road ahead. Adv. Drug Deliv. Rev. 2014, 85, 65–82. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Pharmacokinetics | Antivirals | Characteristics of Patient | Type of Population |
|---|---|---|---|
| MeSH terms | MeSH terms | MeSH terms | MeSH terms |
| Clinical pharmacokinetics (MeSH) Clinical pharmacokinetics (subheading) Drug monitoring (subheading) Pharmacokinetic analysis (subheading) | Antiviral agents (MeSH) Antimicrobial agents (MeSH) Inhaled antiviral agents (MeSH) | Healthy volunteers Patients with viral infection Critically ill | Pediatric patients (MeSH) Adolescents (MeSH) Adults (MeSH) |
| Title/Abstract | Title/Abstract | Title/Abstract | Title/Abstract |
| Pharmacokinetic, pharmacodynamic, target attainment, area under curve, maximum plasma concentration, drug monitoring, drug deposition | See electronic and supplementary file | Influenza, healthy, subjects, volunteers, renal impairment, critically ill, ICU patients, PICU | Children, workers, youth, males, females, elderly, adults, babies |
| Study | Research Objectives | Study Design | Outcome Measures | Sample Size | Spray Device | Model Structure |
|---|---|---|---|---|---|---|
| Zenamivir | ||||||
| Cass et al., 1999 [18] | To assess the clinical PKs and safety of Zanamivir. | RCT | Cmax, AUC, t1/2, Cl, Vd | 104 | Nebulizer/dry powder inhaler | Non-compartmental models |
| Weller et al., 2013 [13] | To evaluate preliminary PKs and safety data to support the use of Zanamivir via Rotahaler/Rotacap. | RCT | Cmax, AUC, Tmax, t1/2 | 18 | Rotadisk/Diskhaler | Mixed-effect models |
| Cass et al., 1999 [19] | To determine the sites of Zanamivir deposition in the respiratory tract and the PKs of Zanamivir via Diskhaler device and a prototype device. | RCT | Cmax, AUC, t1/2, Cl | 13 | Diskhaler/prototype device | Non-compartmental models |
| Peng et al., 2000 [8] | To assess the population PKs of Zenamivir in participants with experimental and naturally occurring influenza. | RCT | Cl, Vd | 201 | Intranasal and inhaled powder | Mixed-effect models |
| Peng et al., 2000 [30] | To examine the PKs, safety, and tolerability of Zanamivir in pediatric patients. | Prospective study | Cmax, AUC, Tmax, t1/2, Vd | 18 | Nebulizer and Diskhaler | Non-compartment model |
| Shelton et al., 2011 [31] | To evaluate serum as well as pulmonary PKs following IV and oral inhaled administration. | Non-randomized study | Cmax, AUC, Tmax, t1/2, Cl, Vd | 42 | Diskhaler and Rotahaler | Non-compartmental model |
| Laninamivir | ||||||
| Ishizuka et al., 2011 [20] | To assess the safety and PKs of Laninamivir after administration of its prodrug, CS-8958. | RCT | Cmax, AUC, Tmax, t1/2, Vd | 20 | Flowcaps dry powder inhaler | Non-compartment model |
| Ishizuka et al., 2010 [21] | To evaluate its safety, tolerability, and PKs after inhaled administration of its prodrug, CS-8958. | RCT | Cmax, AUC, Tmax, t1/2, Cl, Vd | 76 | Flowcaps dry powder inhaler | Non-compartmental model |
| Yoshiba et al., 2011 [22] | To measure the PK parameters of Laninamivir using a new easy-to-use inhaler. | RCT | Cmax, AUC, Tmax, t1/2, Cl, Vd | 16 | Flow powder inhaler | Non-compartmental model |
| Ishizuka et al., 2012 [10] | To determine the intrapulmonary PKs of LO and Laninamivir. | Open-label study | Cmax, AUC, T max, T1/2 | 36 | Dry powder inhaler | Non-compartmental model |
| Toyama et al., 2017 [29] | To evaluate the safety and PKs of Nebulized Laninamivir Octanoate. | Open-label study | T1/2 | 40 | Reusable nebulizer | Non-compartmental model |
| Yoshihara et al., 2013 [23] | To study the population PKs of LO and Laninamivir in healthy subjects, and adult and pediatric patients with influenza virus infection from eight clinical studies, and to evaluate covariate effects on PKs. | RCT | Cmax, AUC, T1/2, Cl | 175 | Prototype and commercial | One- and two-compartmental models |
| Ribavirin | ||||||
| Couroux et al., 2022 [24] | To assess the safety and PKs of four, single-dose regimens of Ribavirin aerosol. | RCT | Cmax, AUC, t1/2, | 32 | Air-jet nebulizer | Non-compartmental model |
| Englund et al., 1990 [27] | To evaluate the safety of high-dose, short-duration Ribavirin aerosol therapy in pediatric patients with suspected RSV infection. To evaluate the drug concentrations in blood and respiratory secretions and antiviral effects. | Preliminary study | Cmax, t1/2 | 9 | Aerosol nebulizer | Not stated |
| Linn et al., 1995 [28] | To evaluate exposure variables including aerosol concentration, duration of exposure, aerosol size range, and exposed participants’ ventilation rates. | Preliminary study | Cmax, t1/2 | 14 | Aerosol nebulizer | Not stated |
| Dumont et al., 2020 [25] | To assess the efficient delivery of Ribavirin using the particle replication in non-wetting templates (PRINT) technology. | RCT | Cmax, AUC, Tmax | 60 | Rotahaler | Non-compartmental model |
| Rimantadine | ||||||
| Atmar et al., 1990 [26] | To assess the safety and PKs of rimantadine in healthy adults and adults with acute influenza virus infection. | RCT | AUC, t1/2, Cl, V | 27 | Collison nebulizer | Non-compartmental model |
| Drug/Study | Dosing Practice | Pharmacokinetic Parameters | ||||
|---|---|---|---|---|---|---|
| Cmax | T1/2 | AUC | Vd | Cl | ||
| Zenamivir | ||||||
| Cass et al., 1999 [18] | Single and multiple doses of 8 and 16 mg six times daily for 5 days | Nebulizer: 63–139 µg/L Dry powder inhaler: Cmax: 39–54 µg/L | Nebulizer: 2.21 h Dry powder inhaler: 3.56 h | Nebulizer 425 µg.h/L Dry powder inhaler 160 µg.h/L | Not stated | Not stated |
| Weller et al., 2013 [13] | A dose of 10 mg via oral inhalation every 12 h for 5 days using Rotadisk/Diskhaler A dose of 10 mg via oral inhalation every 12 h for 5 days using Rotacap/Rotahaler | Diskhaler: 32 ng/mL Rotahaler: 37 ng/mL | Diskhaler: 3 h Rotahaler: 3.2 h | Diskhaler: 133 ng.h/mL Rotahaler: 157 ng.h/mL | Not stated | Diskhaler: 54 L/h Rotahaler: 49 L/h |
| Cass et al., 1999 [19] | A dose of 10 mg using Diskhaler A dose of 10 mg using prototype device | Diskhaler: 34 µg/L Prototype device: 30 µg/L | Diskhaler: 2.5 h Prototype device: 3.0 h | Diskhaler 184 µg.h/L Rotahaler 190 µg.h/L | Not stated | Diskhaler 54.3 L/h Rotahaler 52.6 L/h |
| Peng et al., 2000 [8] | Placebo/Zanamivir twice daily for 5 days either intranasally (10 mg) or orally inhaled (6.4 mg) | Not stated | Not stated | Not stated | Intranasal: 296 L Inhaled powder: 161 L | Intranasal: Cl: 74.1 L/h Inhaled powder: Cl: 40 L/h |
| Peng et al., 2000 [30] | A dose of 10 mg inhaled by nebulizer A dose of 10 mg inhaled by Diskhaler | Nebulizer: 47 µg/L Diskhaler: 40–47 µg/L | Nebulizer: 1.9 h Diskhaler: 2 h | Nebulizer: 184 µg. h/L Diskhaler: 167–192 µg.h/L | Nebulizer: 16.9 L Diskhaler: 3.5–6.9 L | Nebulizer: 54.3 L/h Diskhaler: 52.1–60 L/h |
| Shelton et al., 2011 [31] | 10 mg q12h for two doses | 21.2 ng/mL | 1.75 h | 175 ng.h/mL | Not stated | Not stated |
| Laninamivir | ||||||
| Ishizuka et al., 2011 [20] | A single inhaled dose of 20 mg | CS-8958: 57.4–74.3 ng/mL Laninamivir: 14.5–29.9 ng/mL | CS-8958: 2.3–5.3 h Laninamivir: 53.2–57 h | CS-8958: 291–401 Laninamivir: 426–2223 ng.h/mL | CS-8958: 6.5–26 mL/min Laninamivir: 12.7–65 mL/min | Not stated |
| Ishizuka et al., 2010 [21] | Doses of CS-8958 of 5 mg–120 mg | CS-8958: 12.8–433 ng/mL Laninamivir: 2.6–66 ng/mL | CS-8958: 1.7–10.7 h Laninamivir: 5.7–80.8 h | CS-8958: 45.3–1567 Laninamivir: 19.9–2059 | CS-8958: 193–956 L Laninamivir: Not stated | CS-8958: 35–61 mL/min Laninamivir: 90–576 mL/min |
| Yoshiba et al., 2011 [22] | Doses of 20 mg and 40 mg | Laninamivir: 19–38.3 ng/mL LO: 145–336 ng/mL | Laninamivir: 66.6–74.4 h LO: 1.79–2.70 h | Laninamivir: 558–1080 ng.h/mL LO: 440–1018 ng.h/mL | Laninamivir: Not stated LO: 121–160 L | Laninamivir: 84.9–106.9 mL/min LO: 34.3–35.9 mL/min |
| Ishizuka et al., 2012 [10] | A single inhaled dose of 40 mg of LO | Laninamivir: 0.025–152.3 µg/mL LO: 0.162–2085 µg/mL | Laninamivir: 45.7 h LO: 2.6–89.9 h | Laninamivir: 0.826–17,271 µg/mL LO: 0.705–31942 | Not stated | Not stated |
| Toyama et al., 2017 [29] | A single dose of 40~320 mg of LO was inhaled | Not stated | Laninamivir: 58.3–165.8 h LO: 1.8–55.1 h | Not stated | Not stated | Not stated |
| Yoshihara et al., 2013 [23] | Group 1: 5, 10, 20, 40 mg (single dose) Group 2: 20, 40 mg (BID, 3 days) Group 3: 40 mg (single dose: young and elderly); 20 mg (QID, 2 days: elderly only) Group 4: 20 mg (single dose) Group 5: 80, 120 mg (single dose) Group 6 40 mg (single dose) Group 7: 20, 40 mg (single dose); 20 mg (QID, 2 days) Group 8: 40 mg (single dose) | Not stated | Laninamivir: 4 h LO: 2 h | Not stated | Not stated | Laninamivir: 5.21 h/L LO: 64.8 h/L |
| Ribavirin | ||||||
| Couroux et al., 2022 [24] | Cohort 1: 50 mg/mL Ribavirin/placebo (10 mL total volume) Cohort 2: 50 mg/mL Ribavirin/placebo (20 mL total volume) Cohort 3: 100 mg/mL Ribavirin/placebo (10 mL total volume) Cohort 4: 100 mg/mL Ribavirin/placebo (20 mL total volume) | Cohort 1: 0.63 µg/mL Cohort 2: 1.07 µg/mL Cohort 3: 0.95 µg/mL Cohort 4: 1.64 µg/mL | Cohort 1: 1 h Cohort 2: 1.75 h Cohort 3: 1.5 h Cohort 4: 2.0 h | Cohort 1: 4.90 µg/mL Cohort 2: 10.55 µg/mL Cohort 3: 9.27 µg/mL Cohort 4: 15.55 µg/mL | Not stated | Not stated |
| Englund et al., 1990 [27] | A dose of 60 mg/mL for 2 h periods TID for up to 5 days | 1725–2179 pmol/L | 1.9 h | Not stated | Not stated | Not stated |
| Linn et al., 1995 [28] | High exposure group A dose of 30 mg QID for 4 days Low exposure group A dose of 3 mg QID for 4 days | 0.89 pmol/L | 37–39 h | Not stated | Not stated | Not stated |
| Dumont et al., 2020 [25] | Cohort A Single dose of 60 mg and 120 mg followed by 30 mg BID for 14 days Cohort B 60 mg BID for 14 consecutive days | Cohort A: 143–508 ng/mL Cohort B: 189–285 ng/mL | Cohort A: 0.5–0.625 h Cohort B: 0.5–0.633 h | Cohort A: 578–1490 ng.h/mL Cohort B: 565–2060 ng.h/mL | Not stated | Not stated |
| Rimantidine | ||||||
| Atmar et al., 1990 [26] | Rimantadine in water 40 µg/L of air every 15 min to 4 h Rimantadine in PBS 40 µg/L of air after every 4 h Rimantadine in water 20 µg/L of air every 4 h to 12 h | Not stated | Oral: 25.2 h SPA: 24.1 h | Oral: 8193 ng.h/mL SPA: 1208 ng.h/mL | Oral: 904 L SPA: 906 L | Oral: 25.3 SPA: 29.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshammari, M.K.; Almutairi, M.S.; Althobaiti, M.D.; Alsawyan, W.A.; Alomair, S.A.; Alwattban, R.R.; Al Khozam, Z.H.; Alanazi, T.J.; Alhuqyal, A.S.; Darwish, H.S.A.; et al. A Systematic Review of Clinical Pharmacokinetics of Inhaled Antiviral. Medicina 2023, 59, 642. https://doi.org/10.3390/medicina59040642
Alshammari MK, Almutairi MS, Althobaiti MD, Alsawyan WA, Alomair SA, Alwattban RR, Al Khozam ZH, Alanazi TJ, Alhuqyal AS, Darwish HSA, et al. A Systematic Review of Clinical Pharmacokinetics of Inhaled Antiviral. Medicina. 2023; 59(4):642. https://doi.org/10.3390/medicina59040642
Chicago/Turabian StyleAlshammari, Mohammed Kanan, Mohammed Salem Almutairi, Mohammed Dakhilallah Althobaiti, Watin Ahmed Alsawyan, Samar Abdulrahman Alomair, Raghad Rsheed Alwattban, Zahra Hassan Al Khozam, Taif Jundi Alanazi, Abdullah S. Alhuqyal, Hassan Saud Al Darwish, and et al. 2023. "A Systematic Review of Clinical Pharmacokinetics of Inhaled Antiviral" Medicina 59, no. 4: 642. https://doi.org/10.3390/medicina59040642