
A Comprehensive Review on Bariatric Endoscopy: Where We Are Now and Where We Are Going
 , , ,
, , ,
Abstract
:1. Introduction
2. Primary Bariatric Endoscopic Therapies
2.1. Restrictive Gastric Procedures
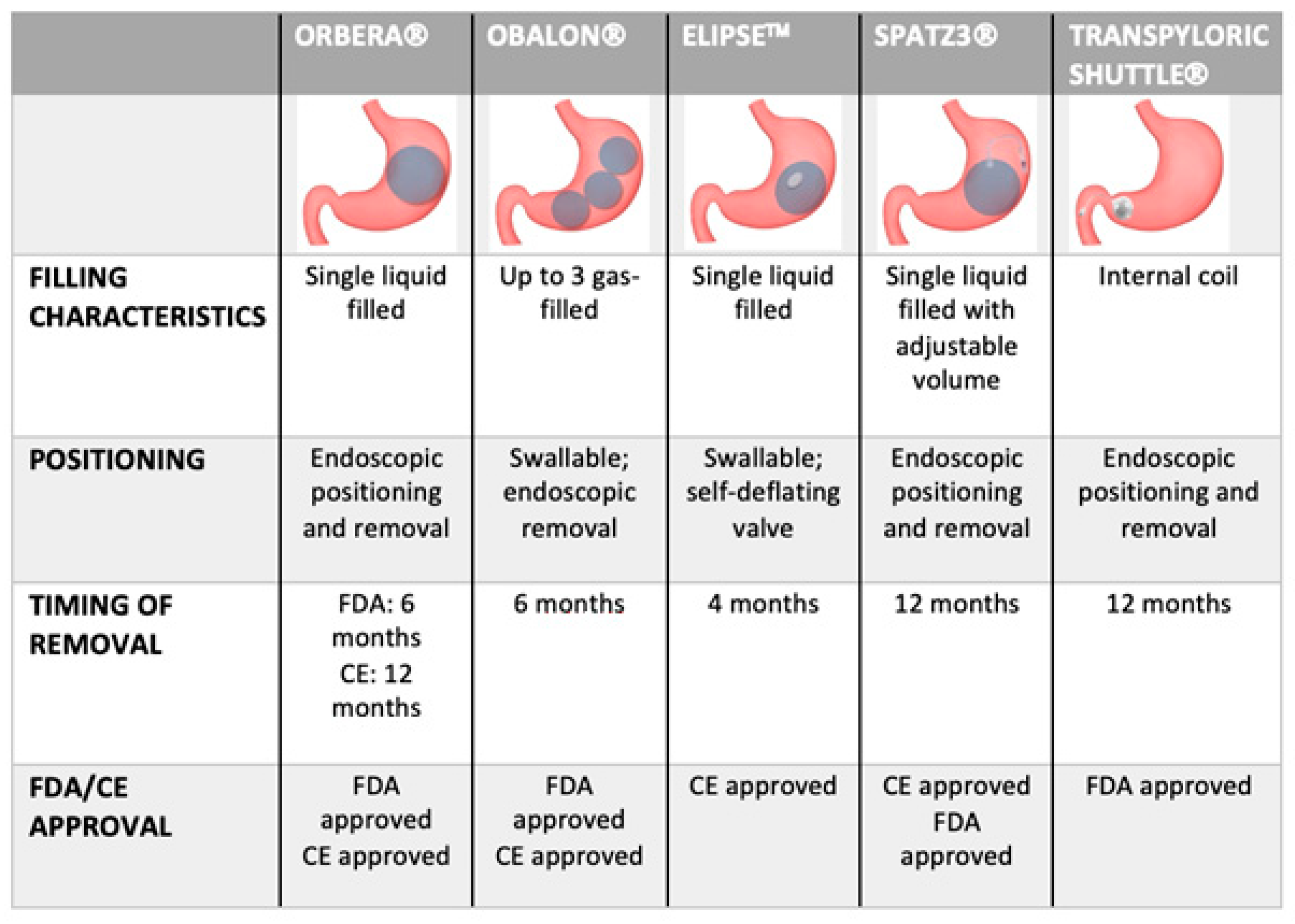
2.1.1. Intragastric Balloons
2.1.2. Transpyloric Shuttle
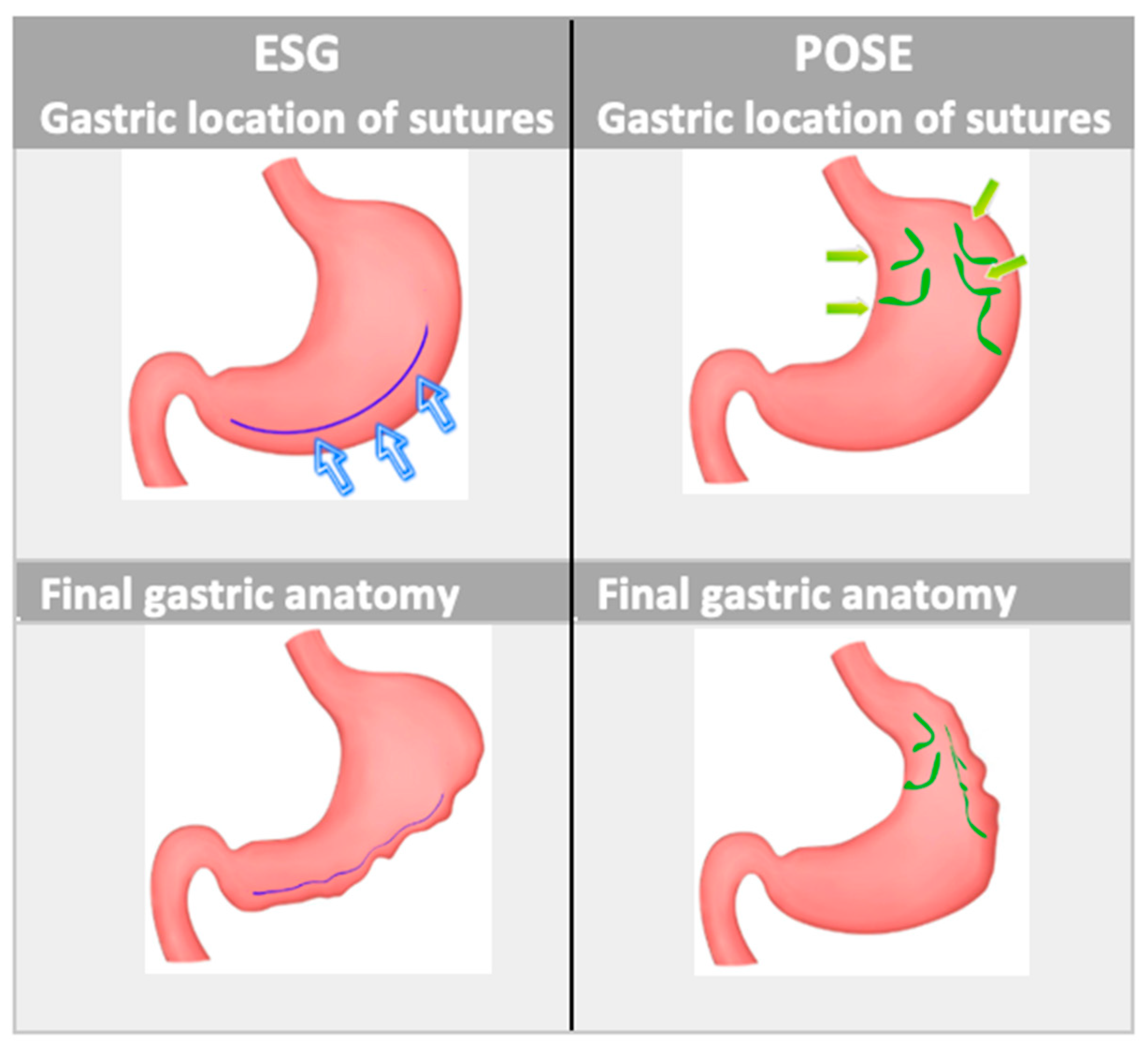
2.1.3. Endoscopic Gastroplasties
2.2. Aspiration Therapy
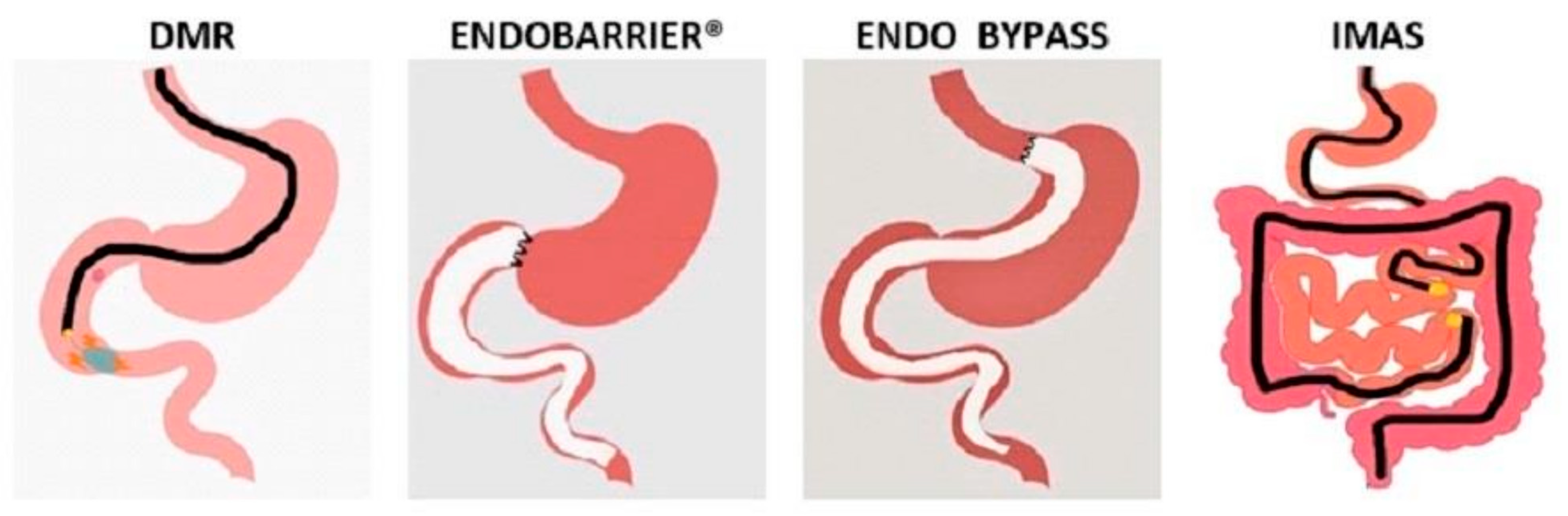
3. Endoscopic Malabsorptive Interventions
3.1. Duodenal Mucosal Resurfacing
3.2. Duodenal-Jejunal Bypass
3.3. Gastroduodenojejunal Bypass
3.4. The Incisionless Magnetic Anastomotic System
4. Revisional Endoscopy after Bariatric Surgery
4.1. Endoscopic Revision after Roux-en-Y Gastric Bypass
4.2. Endoscopic Revision after Sleeve Gastrectomy
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Obesity and Overweight. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 22 November 2022).
- Sturm, R.; Hattori, A. Morbid obesity rates continue to rise rapidly in the United States. Int. J. Obes. 2013, 37, 889–891. [Google Scholar] [CrossRef] [Green Version]
- Heymsfield, S.B.; Wadden, T.A. Mechanisms, Pathophysiology, and Management of Obesity. N. Engl. J. Med. 2017, 376, 1492. [Google Scholar] [CrossRef]
- Berkowitz, R.I.; Fabricatore, A.N. Obesity, psychiatric status, and psychiatric medications. Psychiatr. Clin. N. Am. 2011, 34, 747–764. [Google Scholar] [CrossRef] [PubMed]
- Executive Summary: Guidelines (2013) for the Management of Overweight and Obesity in Adults, a Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Obesity Society Published by the Obesity Society and American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Based on a systematic review from the The Obesity Expert Panel, 2013. Obesity 2014, 22 (Suppl. 2), S5–S39.
- Yanovski, S.Z.; Yanovski, J.A. Long-term drug treatment for obesity, a systematic and clinical review. JAMA 2014, 311, 74–86. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sjöström, L.; Narbro, K.; Sjöström, C.D.; Karason, K.; Larsson, B.; Wedel, H.; Lystig, T.; Sullivan, M.; Bouchard, C.; Carlsson, B.; et al. Effects of bariatric surgery on mortality in Swedish obese subjects. N. Engl. J. Med. 2007, 357, 741–752. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schauer, P.R.; Mingrone, G.; Ikramuddin, S.; Wolfe, B. Clinical Outcomes of Metabolic Surgery, Efficacy of Glycemic Control, Weight Loss, and Remission of Diabetes. Diabetes Care 2016, 39, 902–911. [Google Scholar] [CrossRef] [Green Version]
- O’Brien, P.E.; Hindle, A.; Brennan, L.; Skinner, S.; Burton, P.; Smith, A.; Crosthwaite, G.; Brown, W. Long-Term Outcomes After Bariatric Surgery, a Systematic Review and Meta-analysis of Weight Loss at 10 or More Years for All Bariatric Procedures and a Single-Centre Review of 20-Year Outcomes After Adjustable Gastric Banding. Obes. Surg. 2019, 29, 3–14. [Google Scholar] [CrossRef] [Green Version]
- Arterburn, D.E.; Telem, D.A.; Kushner, R.F.; Courcoulas, A.P. Benefits and Risks of Bariatric Surgery in Adults: A Review. JAMA 2020, 324, 879–887. [Google Scholar] [CrossRef]
- Flum, D.R.; Belle, S.H.; King, W.C.; Wahed, A.S.; Berk, P.; Chapman, W.; Pories, W.; Courcoulas, A.; McCloskey, C.; Mitchell, J.; et al. Perioperative safety in the longitudinal assessment of bariatric surgery. N. Engl. J. Med. 2009, 361, 445–454. [Google Scholar]
- Chang, S.H.; Freeman, N.L.B.; Lee, J.A.; Stoll, C.R.T.; Calhoun, A.J.; Eagon, J.C.; Colditz, G.A. Early major complications after bariatric surgery in the USA, 2003–2014, a systematic review and meta-analysis. Obes. Rev. 2018, 19, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Mechanick, J.I.; Apovian, C.; Brethauer, S.; Garvey, W.T.; Joffe, A.M.; Kim, J.; Kushner, R.F.; Lindquist, R.; Pessah-Pollack, R.; Seger, J.; et al. Clinical practice guidelines for the perioperative nutrition, metabolic, and nonsurgical support of patients undergoing bariatric procedures—2019 update, cosponsored by american association of clinical endocrinologists/american college of endocrinology, the obesity society, american society for metabolic & bariatric surgery, obesity medicine association, and american society of anesthesiologists—Executive summary. Endocr. Pract. 2019, 25, 1346–1359. [Google Scholar]
- Sullivan, S.; Edmundowicz, S.A.; Thompson, C.C. Endoscopic Bariatric and Metabolic Therapies, New and Emerging Technologies. Gastroenterology 2017, 152, 1791–1801. [Google Scholar] [CrossRef] [PubMed]
- Bulajic, M.; Vadalà di Prampero, S.F.; Boškoski, I.; Costamagna, G. Endoscopic therapy of weight regain after bariatric surgery. World J. Gastrointest. Surg. 2021, 13, 1584–1596. [Google Scholar] [CrossRef]
- Kumbhari, V.; le Roux, C.W.; Cohen, R.V. Endoscopic Evaluation and Management of Late Complications After Bariatric Surgery, a Narrative Review. Obes. Surg. 2021, 31, 4624–4633. [Google Scholar] [CrossRef] [PubMed]
- Karlas, T.; Petroff, D.; Feisthammel, J.; Beer, S.; Blüher, M.; Schütz, T.; Lichtinghagen, R.; Hoffmeister, A.; Wiegand, J. Endoscopic Bariatric Treatment with Duodenal-Jejunal Bypass Liner Improves Non-invasive Markers of Non-alcoholic Steatohepatitis. Obes. Surg. 2022, 32, 2495–2503. [Google Scholar] [CrossRef]
- Na, H.K.; De Moura, D.T.H. Various Novel and Emerging Technologies in Endoscopic Bariatric and Metabolic Treatments. Clin. Endosc. 2021, 54, 25–31. [Google Scholar] [CrossRef]
- van Baar, A.C.G.; Meiring, S.; Smeele, P.; Vriend, T.; Holleman, F.; Barlag, M.; Mostafavi, N.; Tijssen, J.G.P.; Soeters, M.R.; Nieuwdorp, M.; et al. Duodenal mucosal resurfacing combined with glucagon-like peptide-1 receptor agonism to discontinue insulin in type 2 diabetes, a feasibility study. Gastrointest. Endosc. 2021, 94, 111–120.e3. [Google Scholar] [CrossRef]
- Buchwald, H.; Estok, R.; Fahrbach, K.; Banel, D.; Sledge, I. Trends in mortality in bariatric surgery, a systematic review and meta-analysis. Surgery 2007, 142, 621–632; discussion 32–35. [Google Scholar] [CrossRef]
- Nieben, O.G.; Harboe, H. Intragastric balloon as an artificial bezoar for treatment of obesity. Lancet 1982, 1, 198–199. [Google Scholar] [CrossRef]
- Neto, M.G.; Silva, L.B.; Grecco, E.; de Quadros, L.G.; Teixeira, A.; Souza, T.; Scarparo, J.; Parada, A.A.; Dib, R.; Moon, R.; et al. Brazilian Intragastric Balloon Consensus Statement (BIBC), practical guidelines based on experience of over 40,000 cases. Surg. Obes. Relat. Dis. 2018, 14, 151–159. [Google Scholar] [CrossRef] [Green Version]
- Espinet Coll, E.; Del Pozo García, A.J.; Turró Arau, R.; Nebreda Durán, J.; Cortés Rizo, X.; Serrano Jiménez, A.; Escartí Usó, M.; Muñoz Tornero, M.; Carral Martínez, D.; Bernabéu López, J.; et al. Spanish Intragastric Balloon Consensus Statement (SIBC), practical guidelines based on experience of over 20 000 cases. Rev. Esp. Enferm. Dig. 2023, 115, 22–34. [Google Scholar]
- Ribeiro, I.B.; Kotinda, A.; Sánchez-Luna, S.A.; de Moura, D.T.H.; Mancini, F.C.; de Souza, T.F.; Matuguma, S.E.; Sakai, C.M.; Rocha, R.S.P.; Luz, G.O.; et al. Adverse Events and Complications with Intragastric Balloons, a Narrative Review (with Video). Obes. Surg. 2021, 31, 2743–2752. [Google Scholar] [CrossRef] [PubMed]
- Trang, J.; Lee, S.S.; Miller, A.; Cruz Pico, C.X.; Postoev, A.; Ibikunle, I.; Ibikunle, C.A. Incidence of nausea and vomiting after intragastric balloon placement in bariatric patients—A systematic review and meta-analysis. Int. J. Surg. 2018, 57, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Moura, D.; Oliveira, J.; De Moura, E.G.; Bernardo, W.; Galvão Neto, M.; Campos, J.; Popov, V.B.; Thompson, C. Effectiveness of intragastric balloon for obesity, A systematic review and meta-analysis based on randomized control trials. Surg. Obes. Relat. Dis. 2016, 12, 420–429. [Google Scholar] [CrossRef]
- Singh, S.; de Moura, D.T.H.; Khan, A.; Bilal, M.; Chowdhry, M.; Ryan, M.B.; Bazarbashi, A.N.; Thompson, C.C. Intragastric Balloon Versus Endoscopic Sleeve Gastroplasty for the Treatment of Obesity, a Systematic Review and Meta-analysis. Obes. Surg. 2020, 30, 3010–3029. [Google Scholar] [CrossRef] [PubMed]
- Fittipaldi-Fernandez, R.J.; Zotarelli-Filho, I.J.; Diestel, C.F.; Klein, M.; de Santana, M.F.; de Lima, J.H.F.; Bastos, F.S.S.; Dos Santos, N.T. Intragastric Balloon, a Retrospective Evaluation of 5874 Patients on Tolerance, Complications, and Efficacy in Different Degrees of Overweight. Obes. Surg. 2020, 30, 4892–4898. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, M.L.; Drew, R.L.; Chazin-Caldie, M. Factors determining conversion from laparoscopic to open Roux-en-Y gastric bypass. Obes. Surg. 2004, 14, 1193–1197. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.A.; Grinberg, R.; Johnson, S.; Afthinos, J.N.; Gibbs, K.E. Perioperative risk factors for 30-day mortality after bariatric surgery, is functional status important? Surg. Endosc. 2013, 27, 1772–1777. [Google Scholar] [CrossRef]
- Loo, J.H.; Lim, Y.H.; Seah, H.L.; Chong, A.Z.Q.; Tay, K.V. Intragastric Balloon as Bridging Therapy Prior to Bariatric Surgery for Patients with Severe Obesity (BMI ≥ 50 kg/m(2)), a Systematic Review and Meta-analysis. Obes. Surg. 2022, 32, 489–502. [Google Scholar] [CrossRef]
- Schapiro, M.; Benjamin, S.; Blackburn, G.; Frank, B.; Heber, D.; Kozarek, R.; Randall, S.; Stern, W. Obesity and the gastric balloon, a comprehensive workshop. Gastrointest. Endosc. 1987, 33, 323–327. [Google Scholar] [CrossRef] [PubMed]
- Stavrou, G.; Shrewsbury, A.; Kotzampassi, K. Six intragastric balloons, Which to choose? World J. Gastrointest. Endosc. 2021, 13, 238–259. [Google Scholar] [CrossRef] [PubMed]
- Wahlen, C.H.; Bastens, B.; Herve, J.; Malmendier, C.; Dallemagne, B.; Jehaes, C.; Markiewicz, S.; Monami, B.; Weerts, J. The BioEnterics Intragastric Balloon (BIB), how to use it. Obes. Surg. 2001, 11, 524–527. [Google Scholar] [CrossRef] [PubMed]
- Abu Dayyeh, B.K.; Kumar, N.; Edmundowicz, S.A.; Jonnalagadda, S.; Larsen, M.; Sullivan, S.; Thompson, C.C.; Banerjee, S. ASGE Bariatric Endoscopy Task Force systematic review and meta-analysis assessing the ASGE PIVI thresholds for adopting endoscopic bariatric therapies. Gastrointest. Endosc. 2015, 82, 425–438.e5. [Google Scholar] [CrossRef]
- Kumar, N.; Bazerbachi, F.; Rustagi, T.; McCarty, T.R.; Thompson, C.C.; Galvao Neto, M.P.; Zundel, N.; Wilson, E.B.; Gostout, C.J.; Abu Dayyeh, B.K. The Influence of the Orbera Intragastric Balloon Filling Volumes on Weight Loss, Tolerability, and Adverse Events, a Systematic Review and Meta-Analysis. Obes. Surg. 2017, 27, 2272–2278. [Google Scholar] [CrossRef]
- Mion, F.; Ibrahim, M.; Marjoux, S.; Ponchon, T.; Dugardeyn, S.; Roman, S.; Deviere, J. Swallowable Obalon® gastric balloons as an aid for weight loss, a pilot feasibility study. Obes. Surg. 2013, 23, 730–733. [Google Scholar] [CrossRef]
- Král, J.; Machytka, E.; Horká, V.; Selucká, J.; Doleček, F.; Špičák, J.; Kovářová, V.; Haluzík, M.; Bužga, M. Endoscopic Treatment of Obesity and Nutritional Aspects of Bariatric Endoscopy. Nutrients 2021, 13, 4268. [Google Scholar] [CrossRef]
- Sullivan, S.; Swain, J.; Woodman, G.; Edmundowicz, S.; Hassanein, T.; Shayani, V.; Fang, J.C.; Noar, M.; Eid, G.; English, W.J.; et al. Randomized sham-controlled trial of the 6-month swallowable gas-filled intragastric balloon system for weight loss. Surg. Obes. Relat. Dis. 2018, 14, 1876–1889. [Google Scholar] [CrossRef]
- Machytka, E.; Gaur, S.; Chuttani, R.; Bojkova, M.; Kupka, T.; Buzga, M.; Giannakou, A.; Ioannis, K.; Mathus-Vliegen, E.; Levy, S.; et al. Elipse, the first procedureless gastric balloon for weight loss, a prospective, observational, open-label, multicenter study. Endoscopy 2017, 49, 154–160. [Google Scholar] [CrossRef]
- Jamal, M.H.; Almutairi, R.; Elabd, R.; AlSabah, S.K.; Alqattan, H.; Altaweel, T. The Safety and Efficacy of Procedureless Gastric Balloon, a Study Examining the Effect of Elipse Intragastric Balloon Safety, Short and Medium Term Effects on Weight Loss with 1-Year Follow-Up Post-removal. Obes. Surg. 2019, 29, 1236–1241. [Google Scholar] [CrossRef]
- Machytka, E.; Klvana, P.; Kornbluth, A.; Peikin, S.; Mathus-Vliegen, L.E.; Gostout, C.; Lopez-Nava, G.; Shikora, S.; Brooks, J. Adjustable intragastric balloons, a 12-month pilot trial in endoscopic weight loss management. Obes. Surg. 2011, 21, 1499–1507. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fittipaldi-Fernandez, R.J.; Zotarelli-Filho, I.J.; Diestel, C.F.; Klein, M.; de Santana, M.F.; de Lima, J.H.F.; Bastos, F.S.S.; Dos Santos, N.T. Randomized Prospective Clinical Study of Spatz3® Adjustable Intragastric Balloon Treatment with a Control Group, a Large-Scale Brazilian Experiment. Obes. Surg. 2021, 31, 787–796. [Google Scholar] [CrossRef]
- Abu Dayyeh, B.K.; Maselli, D.B.; Rapaka, B.; Lavin, T.; Noar, M.; Hussan, H.; Chapman, C.G.; Popov, V.; Jirapinyo, P.; Acosta, A.; et al. Adjustable intragastric balloon for treatment of obesity, a multicentre, open-label, randomised clinical trial. Lancet 2021, 398, 1965–1973. [Google Scholar] [CrossRef]
- Ponce, J.; Quebbemann, B.B.; Patterson, E.J. Prospective, randomized, multicenter study evaluating safety and efficacy of intragastric dual-balloon in obesity. Surg. Obes. Relat. Dis. 2013, 9, 290–295. [Google Scholar] [CrossRef] [PubMed]
- Marinos, G.; Eliades, C.; Raman Muthusamy, V.; Greenway, F. Weight loss and improved quality of life with a nonsurgical endoscopic treatment for obesity, clinical results from a 3- and 6-month study. Surg. Obes. Relat. Dis. 2014, 10, 929–934. [Google Scholar] [CrossRef]
- Rothstein, R.; Woodman, G.; Swain, J. Weight Reduction in Patients with Obesity Using the Transpyloric Shuttle®, ENDObesity® II Study. In Proceedings of the Obesity Week 2018, Nashville, TN, USA, 11–15 November 2018. [Google Scholar]
- Abu Dayyeh, B.K.; Rajan, E.; Gostout, C.J. Endoscopic sleeve gastroplasty, a potential endoscopic alternative to surgical sleeve gastrectomy for treatment of obesity. Gastrointest. Endosc. 2013, 78, 530–535. [Google Scholar] [CrossRef]
- Lopez-Nava, G.; Galvão, M.P.; Bautista-Castaño, I.; Jimenez-Baños, A.; Fernandez-Corbelle, J.P. Endoscopic Sleeve Gastroplasty, How I Do It? Obes. Surg. 2015, 25, 1534–1538. [Google Scholar] [CrossRef] [PubMed]
- Espinós, J.C.; Turró, R.; Mata, A.; Cruz, M.; da Costa, M.; Villa, V.; Buchwald, J.N.; Turró, J. Early experience with the Incisionless Operating Platform™ (IOP) for the treatment of obesity, the Primary Obesity Surgery Endolumenal (POSE) procedure. Obes. Surg. 2013, 23, 1375–1383. [Google Scholar] [CrossRef]
- Telese, A.; Sehgal, V.; Magee, C.G.; Naik, S.; Alqahtani, S.A.; Lovat, L.B.; Haidry, R.J. Bariatric and Metabolic Endoscopy, A New Paradigm. Clin. Transl. Gastroenterol. 2021, 12, e00364. [Google Scholar] [CrossRef]
- Gys, B.; Plaeke, P.; Lamme, B.; Lafullarde, T.; Komen, N.; Beunis, A.; Hubens, G. Endoscopic Gastric Plication for Morbid Obesity, a Systematic Review and Meta-analysis of Published Data over Time. Obes. Surg. 2019, 29, 3021–3029. [Google Scholar] [CrossRef]
- Mohan, B.P.; Asokkumar, R.; Khan, S.R.; Kotagiri, R.; Sridharan, G.K.; Chandan, S.; Ravikumar, N.P.; Ponnada, S.; Jayaraj, M.; Adler, D.G. Outcomes of endoscopic sleeve gastroplasty, how does it compare to laparoscopic sleeve gastrectomy? A systematic review and meta-analysis. Endosc. Int. Open 2020, 8, E558–E565. [Google Scholar] [CrossRef] [Green Version]
- Hedjoudje, A.; Abu Dayyeh, B.K.; Cheskin, L.J.; Adam, A.; Neto, M.G.; Badurdeen, D.; Morales, J.G.; Sartoretto, A.; Nava, G.L.; Vargas, E.; et al. Efficacy and Safety of Endoscopic Sleeve Gastroplasty, A Systematic Review and Meta-Analysis. Clin. Gastroenterol. Hepatol. 2020, 18, 1043–1053.e4. [Google Scholar] [CrossRef] [PubMed]
- Abu Dayyeh, B.K.; Bazerbachi, F.; Vargas, E.J.; Sharaiha, R.Z.; Thompson, C.C.; Thaemert, B.C.; Teixeira, A.F.; Chapman, C.G.; Kumbhari, V.; Ujiki, M.B.; et al. Endoscopic sleeve gastroplasty for treatment of class 1 and 2 obesity (MERIT), a prospective, multicentre, randomised trial. Lancet 2022, 400, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Veltzke-Schlieker, W.; Adler, A.; Specht, M.; Eskander, W.; Ismail, M.; Badakhshi, H.; Galvao, M.P.; Zorron, R. Endoscopic Sleeve Gastroplasty (ESG) for High-Risk Patients, High Body Mass Index (> 50 kg/m(2)) Patients, and Contraindication to Abdominal Surgery. Obes. Surg. 2021, 31, 3400–3409. [Google Scholar] [CrossRef] [PubMed]
- Zorron, R.; Veltzke-Schlieker, W.; Adler, A.; Denecke, C.; Dziodzio, T.; Pratschke, J.; Benzing, C. Endoscopic sleeve gastroplasty using Apollo Overstitch as a bridging procedure for superobese and high risk patients. Endoscopy 2018, 50, 81–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopez-Nava, G.; Asokkumar, R.; Turró Arau, R.; Neto, M.G.; Dayyeh, B.A. Modified primary obesity surgery endoluminal (POSE-2) procedure for the treatment of obesity. VideoGIE 2020, 5, 91–93. [Google Scholar] [CrossRef] [Green Version]
- Jirapinyo, P.; Thompson, C.C. Endoscopic gastric body plication for the treatment of obesity, technical success and safety of a novel technique (with video). Gastrointest. Endosc. 2020, 91, 1388–1394. [Google Scholar] [CrossRef]
- Graus Morales, J.; Crespo Pérez, L.; Marques, A.; Marín Arribas, B.; Bravo Arribas, R.; Ramo, E.; Escalada, C.; Arribas, C.; Himpens, J. Modified endoscopic gastroplasty for the treatment of obesity. Surg. Endosc. 2018, 32, 3936–3942. [Google Scholar] [CrossRef]
- Fayad, L.; Adam, A.; Schweitzer, M.; Cheskin, L.J.; Ajayi, T.; Dunlap, M.; Badurdeen, D.S.; Hill, C.; Paranji, N.; Lalezari, S.; et al. Endoscopic sleeve gastroplasty versus laparoscopic sleeve gastrectomy, a case-matched study. Gastrointest. Endosc. 2019, 89, 782–788. [Google Scholar] [CrossRef]
- Sharaiha, R.Z.; Kumta, N.A.; Saumoy, M.; Desai, A.P.; Sarkisian, A.M.; Benevenuto, A.; Tyberg, A.; Kumar, R.; Igel, L.; Verna, E.C.; et al. Endoscopic Sleeve Gastroplasty Significantly Reduces Body Mass Index and Metabolic Complications in Obese Patients. Clin. Gastroenterol. Hepatol. 2017, 15, 504–510. [Google Scholar] [CrossRef]
- Thompson, C.C.; Abu Dayyeh, B.K.; Kushner, R.; Sullivan, S.; Schorr, A.B.; Amaro, A.; Apovian, C.M.; Fullum, T.; Zarrinpar, A.; Jensen, M.D.; et al. Percutaneous Gastrostomy Device for the Treatment of Class II and Class III Obesity, Results of a Randomized Controlled Trial. Am. J. Gastroenterol. 2017, 112, 447–457. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crothall, K. 2022. Available online: https://www.aspirebariatrics.com/ (accessed on 25 November 2022).
- Rajagopalan, H.; Cherrington, A.D.; Thompson, C.C.; Kaplan, L.M.; Rubino, F.; Mingrone, G.; Becerra, P.; Rodriguez, P.; Vignolo, P.; Caplan, J.; et al. Endoscopic Duodenal Mucosal Resurfacing for the Treatment of Type 2 Diabetes, 6-Month Interim Analysis From the First-in-Human Proof-of-Concept Study. Diabetes Care 2016, 39, 2254–2261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mingrone, G.; van Baar, A.C.; Devière, J.; Hopkins, D.; Moura, E.; Cercato, C.; Rajagopalan, H.; Lopez-Talavera, J.C.; White, K.; Bhambhani, V.; et al. Safety and efficacy of hydrothermal duodenal mucosal resurfacing in patients with type 2 diabetes, the randomised, double-blind, sham-controlled, multicentre REVITA-2 feasibility trial. Gut 2022, 71, 254–264. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Grunert, L.; Galvao Neto, M.P.; Alamo, M.; Ramos, A.C.; Baez, P.B.; Tarnoff, M. First human experience with endoscopically delivered and retrieved duodenal-jejunal bypass sleeve. Surg. Obes. Relat. Dis. 2008, 4, 55–59. [Google Scholar] [CrossRef]
- Rohde, U.; Hedbäck, N.; Gluud, L.L.; Vilsbøll, T.; Knop, F.K. Effect of the EndoBarrier Gastrointestinal Liner on obesity and type 2 diabetes, a systematic review and meta-analysis. Diabetes Obes. Metab. 2016, 18, 300–305. [Google Scholar] [CrossRef] [PubMed]
- Jirapinyo, P.; Haas, A.V.; Thompson, C.C. Effect of the Duodenal-Jejunal Bypass Liner on Glycemic Control in Patients With Type 2 Diabetes With Obesity, A Meta-analysis With Secondary Analysis on Weight Loss and Hormonal Changes. Diabetes Care 2018, 41, 1106–1115. [Google Scholar] [CrossRef] [Green Version]
- Caiazzo, R.; Branche, J.; Raverdy, V.; Czernichow, S.; Carette, C.; Robert, M.; Disse, E.; Barthet, M.; Cariou, B.; Msika, S.; et al. Efficacy and Safety of the Duodeno-Jejunal Bypass Liner in Patients With Metabolic Syndrome, A Multicenter Randomized Controlled Trial (ENDOMETAB). Ann. Surg. 2020, 272, 696–702. [Google Scholar] [CrossRef]
- ClinicalTrials. Available online: https://clinicaltrials.gov/ct2/show/NCT04101669 (accessed on 1 March 2023).
- Ruban, A.; Miras, A.D.; Glaysher, M.A.; Goldstone, A.P.; Prechtl, C.G.; Johnson, N.; Chhina, N.; Al-Najim, W.; Aldhwayan, M.; Klimowska-Nassar, N.; et al. Duodenal-Jejunal Bypass Liner for the management of Type 2 Diabetes Mellitus and Obesity, A Multicenter Randomized Controlled Trial. Ann. Surg. 2022, 275, 440–447. [Google Scholar] [CrossRef]
- Yvamoto, E.Y.; de Moura, D.T.H.; Proença, I.M.; do Monte Junior, E.S.; Ribeiro, I.B.; Ribas, P.; Hemerly, M.C.; de Oliveira, V.L.; Sánchez-Luna, S.A.; Bernardo, W.M.; et al. The Effectiveness and Safety of the Duodenal-Jejunal Bypass Liner (DJBL) for the Management of Obesity and Glycaemic Control, a Systematic Review and Meta-Analysis of Randomized Controlled Trials. Obes. Surg. 2023, 33, 585–599. [Google Scholar] [CrossRef]
- Sandler, B.J.; Rumbaut, R.; Swain, C.P.; Torres, G.; Morales, L.; Gonzales, L.; Schultz, S.; Talamini, M.A.; Jacobsen, G.R.; Horgan, S. One-year human experience with a novel endoluminal, endoscopic gastric bypass sleeve for morbid obesity. Surg. Endosc. 2015, 29, 3298–3303. [Google Scholar] [CrossRef]
- Machytka, E.; Bužga, M.; Zonca, P.; Lautz, D.B.; Ryou, M.; Simonson, D.C.; Thompson, C.C. Partial jejunal diversion using an incisionless magnetic anastomosis system, 1-year interim results in patients with obesity and diabetes. Gastrointest. Endosc. 2017, 86, 904–912. [Google Scholar] [CrossRef]
- De Moura, D.T.H.; Barrichello, S., Jr.; de Moura, E.G.H.; de Souza, T.F.; Dos Passos Galvão Neto, M.; Grecco, E.; Sander, B.; Hoff, A.C.; Matz, F.; Ramos, F.; et al. Endoscopic sleeve gastroplasty in the management of weight regain after sleeve gastrectomy. Endoscopy 2020, 52, 202–210. [Google Scholar]
- Cambi, M.P.C.; Baretta, G.A.P.; Magro, D.O.; Boguszewski, C.L.; Ribeiro, I.B.; Jirapinyo, P.; de Moura, D.T.H. Multidisciplinary Approach for Weight Regain-how to Manage this Challenging Condition, an Expert Review. Obes. Surg. 2021, 31, 1290–1303. [Google Scholar] [CrossRef]
- Brunaldi, V.O.; Jirapinyo, P.; de Moura, D.T.H.; Okazaki, O.; Bernardo, W.M.; Galvão Neto, M.; Campos, J.M.; Santo, M.A.; de Moura, E.G.H. Endoscopic Treatment of Weight Regain Following Roux-en-Y Gastric Bypass, a Systematic Review and Meta-analysis. Obes. Surg. 2018, 28, 266–276. [Google Scholar] [CrossRef] [PubMed]
- Fayad, L.; Trindade, A.J.; Benias, P.C.; Simsek, C.; Raad, M.; Badurdeen, D.; Hill, C.; Brewer Gutierrez, O.I.; Fayad, G.; Dunlap, M.; et al. Cryoballoon ablation for gastric pouch and/or outlet reduction in patients with weight regain post Roux-en-Y gastric bypass. Endoscopy 2020, 52, 227–230. [Google Scholar] [CrossRef]
- Jirapinyo, P.; de Moura, D.T.H.; Dong, W.Y.; Farias, G.; Thompson, C.C. Dose response for argon plasma coagulation in the treatment of weight regain after Roux-en-Y gastric bypass. Gastrointest. Endosc. 2020, 91, 1078–1084. [Google Scholar] [CrossRef]
- de Quadros, L.G.; Neto, M.G.; Marchesini, J.C.; Teixeira, A.; Grecco, E.; Junior, R.L.K.; Zundel, N.; Filho, I.J.Z.; de Souza, T.F.; Filho, A.C.; et al. Endoscopic Argon Plasma Coagulation vs. Multidisciplinary Evaluation in the Management of Weight Regain After Gastric Bypass Surgery, a Randomized Controlled Trial with SHAM Group. Obes. Surg. 2020, 30, 1904–1916. [Google Scholar] [CrossRef] [PubMed]
- Dhindsa, B.S.; Saghir, S.M.; Naga, Y.; Dhaliwal, A.; Ramai, D.; Cross, C.; Singh, S.; Bhat, I.; Adler, D.G. Efficacy of transoral outlet reduction in Roux-en-Y gastric bypass patients to promote weight loss, a systematic review and meta-analysis. Endosc. Int. Open 2020, 8, E1332–E1340. [Google Scholar] [CrossRef] [PubMed]
- Jaruvongvanich, V.; Vantanasiri, K.; Laoveeravat, P.; Matar, R.H.; Vargas, E.J.; Maselli, D.B.; Alkhatry, M.; Fayad, L.; Kumbhari, V.; Fittipaldi-Fernandez, R.J. Endoscopic full-thickness suturing plus argon plasma mucosal coagulation versus argon plasma mucosal coagulation alone for weight regain after gastric bypass, a systematic review and meta-analysis. Gastrointest. Endosc. 2020, 92, 1164–1175.e6. [Google Scholar] [CrossRef]
- Jirapinyo, P.; Dayyeh, B.K.; Thompson, C.C. Gastrojejunal anastomotic reduction for weight regain in roux-en-y gastric bypass patients, physiological, behavioral, and anatomical effects of endoscopic suturing and sclerotherapy. Surg. Obes. Relat. Dis. 2016, 12, 1810–1816. [Google Scholar] [CrossRef] [Green Version]
- Heylen, A.M.; Jacobs, A.; Lybeer, M.; Prosst, R.L. The OTSC®-clip in revisional endoscopy against weight gain after bariatric gastric bypass surgery. Obes. Surg. 2011, 21, 1629–1633. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.; Ellenbogen, Y.; Doumouras, A.G.; Gmora, S.; Anvari, M.; Hong, D. Single- or double-anastomosis duodenal switch versus Roux-en-Y gastric bypass as a revisional procedure for sleeve gastrectomy, A systematic review and meta-analysis. Surg. Obes. Relat. Dis. 2019, 15, 556–566. [Google Scholar] [CrossRef]
- Eid, G. Sleeve gastrectomy revision by endoluminal sleeve plication gastroplasty, a small pilot case series. Surg. Endosc. 2017, 31, 4252–4255. [Google Scholar] [CrossRef]
- Maselli, D.B.; Alqahtani, A.R.; Abu Dayyeh, B.K.; Elahmedi, M.; Storm, A.C.; Matar, R.; Nieto, J.; Teixeira, A.; Al Khatry, M.; Neto, M.G. Revisional endoscopic sleeve gastroplasty of laparoscopic sleeve gastrectomy, an international, multicenter study. Gastrointest. Endosc. 2021, 93, 122–130. [Google Scholar] [CrossRef] [PubMed]
- Kushner, R.F.; Ryan, D.H. Assessment and lifestyle management of patients with obesity, clinical recommendations from systematic reviews. JAMA 2014, 312, 943–952. [Google Scholar] [CrossRef] [PubMed]
- Acosta, A.; Streett, S.; Kroh, M.D.; Cheskin, L.J.; Saunders, K.H.; Kurian, M.; Schofield, M.; Barlow, S.E.; Aronne, L. White Paper AGA, POWER—Practice Guide on Obesity and Weight Management, Education, and Resources. Clin. Gastroenterol. Hepatol. 2017, 15, 631–649.e10. [Google Scholar] [CrossRef] [PubMed]
- Lopez Nava, G.; Arau, R.T.; Asokkumar, R.; Maselli, D.B.; Rapaka, B.; Matar, R.; Bautista, I.; Espinos Perez, J.C.; Bilbao, A.M.; Jaruvongvanich, V.; et al. Prospective Multicenter Study of the Primary Obesity Surgery Endoluminal (POSE 2.0) Procedure for Treatment of Obesity. Clin. Gastroenterol. Hepatol. 2023, 21, 81–89.e4. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type of Study | Number of Patients | Comparator Group | Weight Loss Outcome | AEs Outcome | |||
|---|---|---|---|---|---|---|---|
| Primary endoscopic therapies | Space occupying devices | Orbera® | Meta-analysis [35] | 1638 (17 studies) | None | EWL 25.44 (95% CI, 21.47–29.4) at 1 year | 33.7% pain and nausea 1.4% migration 0.1% gastric perforation |
| Obalon® | Double-blind RCT with sham group [39] | 387 | Lifestyle therapy | TBWL 7.1 ± 5.3 vs. 3.6 ± 5.1 kg | 0.4% SAEs (one bleeding and one balloon deflation | ||
| Elipse™ | Prospective observational [41] | 112 | None | TBWL 7.9% at 1 year | 51% nausea and vomiting 0% SAEs [25] * | ||
| Spatz3® | RCT [44] | 288 | Lifestyle therapy | TBWL 15.0% vs. 3.3% 32 weeks at 32 wks (p < 0.0001) | Seven SAEs (7%). No deaths | ||
| Transpyloric Shuttle® | Observational [46] | 20 | None | EWL 41% at 6 months | 10% early removal for gastric ulceration | ||
| Endoscopic gastroplasties | ESG | Meta-analysis [53] | 1815 (8 studies on ESG) 2179 (7 studies on LSG) | Laparoscopic sleeve gastrectomy | TBWL 17.1% vs. 30.5% (ESG vs. LSG) at 1 year | Overall AEs 2.9% (95% CI 1.8–4.4) vs. 11.8% (95% CI 8.4–16.4) | |
| POSE | Meta-analysis [52] | 465 (5 studies on POSE) and 1717 (8 studies on ESG) | ESG | EWL 44.9 ± 2.1% vs. 68.3 ± 3.8% (POSE vs. ESG) at 1 year | 4 SAEs for POSE (3 bleeding and 1 hepatic abscess) | ||
| Endoscopic malabsoptive procedures | DMR | RCT [66] | 108 | Sham procedure | HbA1c reduction from 8.5 ± 0.7% to 7.5 ± 0.8% | None | |
| EndoBarrier® | RCT [70] | 80 | Conventional medical therapy | TBWL 9.7% vs. 2.1% at 1 year | 19 (39%) SAEs (11 re-intervention) | ||
| Endo Bypass System | Prospective observational [74] | 13 | None | EWL was 35.9% at 1 year | None | ||
| IMAS | Prospective observational [75] | 10 | None | TBWL was 14.6%; EWL% 40.2% at 1 year | Diarrhea | ||
| Revisional Endoscopic therapies | APC | RCT with sham group [81] | 42 | Diet | −9.73 kg vs. + 1.38 kg at 6 months | None in 1 year follow-up period | |
| Cryoablation | Retrospective series [79] | 22 | None | TBWL 8.1% at 8 weeks | 13.6% (one stenosis and 2 bleeding) | ||
| TORe | Meta-analysis [82] | 850 (13 studies) | None | TBWL 8.55% at 1 year | Total 11.4% ± 10.11 Severe 0.57% ± 1.35 | ||
| TORe + APC | Meta-analysis [83] | 1625 (16 studies) | TORe | TBWL at 12 months 9.5% vs. 5.8% | Strictures in 4.8% of patients | ||
| Sodium morrhuate | Prospective comparative [84] | 43 | TORe | TBWL 2.7% ±5.5 vs. 10.4% ± 2.2 | N/A | ||
| OTSC | Observational [85] | 94 | None | BMI drop from 32.8 (±1.9) to 27.4 (±3.8) at 1 year | Two stenoses requiring endoscopic dilation | ||
| R-Endosleeve | Prospective [88] | 82 | None | TBWL 15.7% (±7.6%) at 1 year | One moderate adverse event | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mauro, A.; Lusetti, F.; Scalvini, D.; Bardone, M.; De Grazia, F.; Mazza, S.; Pozzi, L.; Ravetta, V.; Rovedatti, L.; Sgarlata, C.; et al. A Comprehensive Review on Bariatric Endoscopy: Where We Are Now and Where We Are Going. Medicina 2023, 59, 636. https://doi.org/10.3390/medicina59030636
Mauro A, Lusetti F, Scalvini D, Bardone M, De Grazia F, Mazza S, Pozzi L, Ravetta V, Rovedatti L, Sgarlata C, et al. A Comprehensive Review on Bariatric Endoscopy: Where We Are Now and Where We Are Going. Medicina. 2023; 59(3):636. https://doi.org/10.3390/medicina59030636
Chicago/Turabian StyleMauro, Aurelio, Francesca Lusetti, Davide Scalvini, Marco Bardone, Federico De Grazia, Stefano Mazza, Lodovica Pozzi, Valentina Ravetta, Laura Rovedatti, Carmelo Sgarlata, and et al. 2023. "A Comprehensive Review on Bariatric Endoscopy: Where We Are Now and Where We Are Going" Medicina 59, no. 3: 636. https://doi.org/10.3390/medicina59030636