

A Retrospective Comparative Study of Endoscopic Treatment of Gastrocnemius Contracture using the Modified Soft Tissue Release Kit
 , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Sample Size and Study Design
2.2. Inclusion and Exclusion Criteria
2.3. Modified Soft Tissue Release Kit
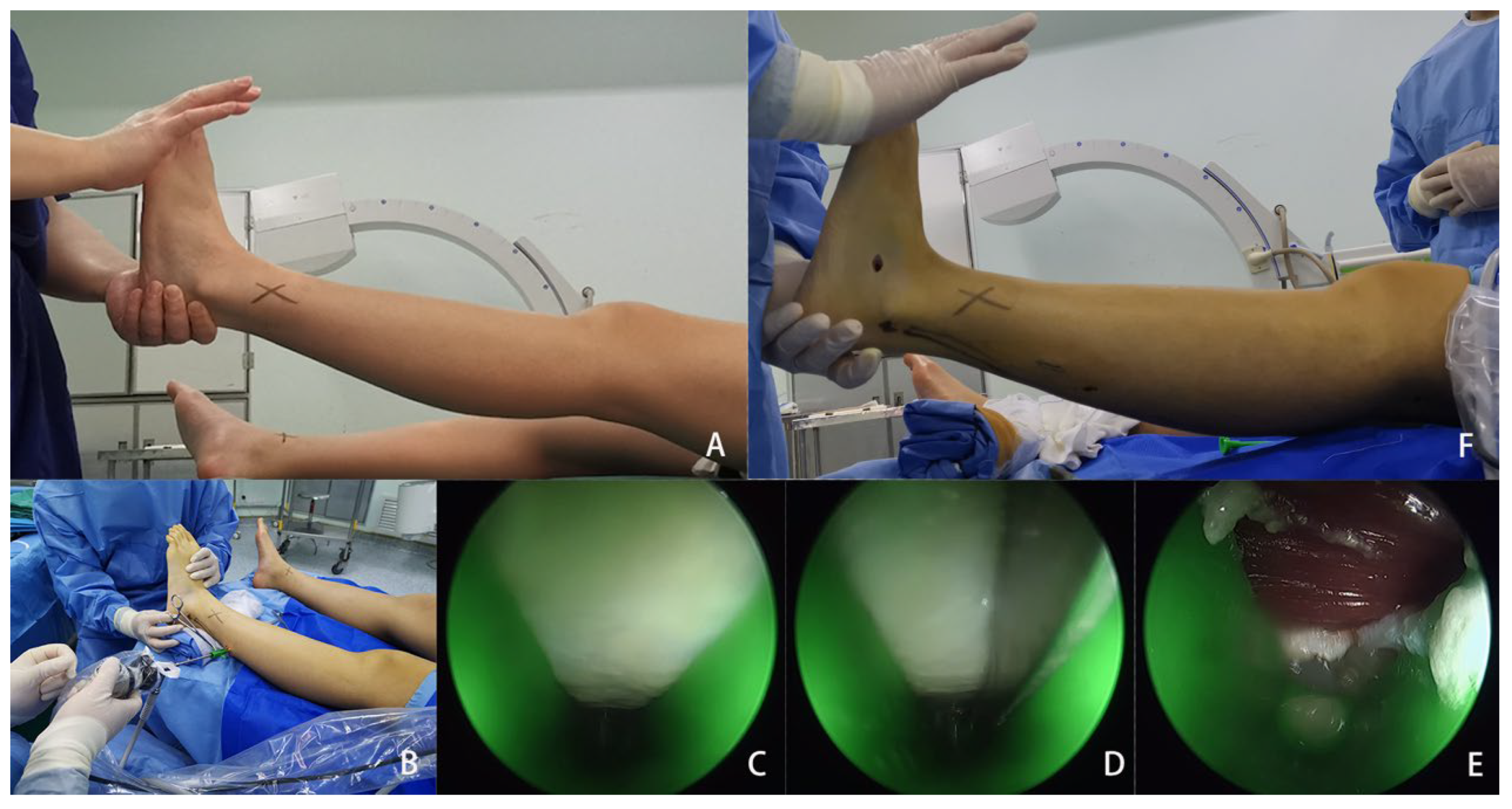
2.4. Surgical Procedure
2.5. Outcome Measures
2.5.1. American Orthopedic Foot and Ankle Society (AOFAS) Ankle-Hindfoot Score
2.5.2. Maximum Ankle Dorsiflexion Angle
2.5.3. Patient Satisfaction
2.5.4. Complications
2.6. Statistical Analysis
3. Results
3.1. General Results
3.2. Clinical Outcomes
3.3. Complications
4. Discussion
4.1. Levels of Gastrocnemius Recession
4.2. Current Status of Endoscopic Gastrocnemius Recession
4.3. Advantages of Endoscopic Gastrocnemius Recession Using the Modified Soft Tissue Release Kit
4.4. Experience in Applying the New Technique
4.5. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- DiGiovanni, C.W.; Kuo, R.; Tejwani, N.; Price, R.; Hansen, S.T., Jr.; Cziernecki, J.; Sangeorzan, B. Isolated gastrocnemius tightness. J. Bone Joint Surg. Am. 2002, 84, 962–970. [Google Scholar] [CrossRef] [PubMed]
- Cazeau, C.; Stiglitz, Y. Effects of gastrocnemius tightness on forefoot during gait. Foot Ankle Clin. 2014, 19, 649–657. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, M.; Ross, T.D. Bony Procedures for Correction of the Flexible Pediatric Flatfoot Deformity. Foot Ankle Clin. 2021, 26, 915–939. [Google Scholar] [CrossRef] [PubMed]
- Ueki, Y.; Sakuma, E.; Wada, I. Pathology and management of flexible flat foot in children. J. Orthop. Sci. 2019, 24, 9–13. [Google Scholar] [CrossRef] [PubMed]
- Campbell, J.T.; Jeng, C.L. Painful Accessory Navicular and Spring Ligament Injuries in Athletes. Clin. Sports Med. 2020, 39, 859–876. [Google Scholar] [CrossRef]
- Jastifer, J.R.; Marston, J. Gastrocnemius Contracture in Patients with and Without Foot Pathology. Foot Ankle Int. 2016, 37, 1165–1170. [Google Scholar] [CrossRef]
- Abbasian, A. Isolated contracture and gastrocnemius recession. Foot Ankle Int. 2013, 34, 307–308. [Google Scholar] [CrossRef]
- Cychosz, C.C.; Phisitkul, P.; Belatti, D.A.; Glazebrook, M.A.; DiGiovanni, C.W. Gastrocnemius recession for foot and ankle conditions in adults: Evidence-based recommendations. Foot Ankle Surg. 2015, 21, 77–85. [Google Scholar] [CrossRef]
- Anderson, J.G.; Bohay, D.R.; Eller, E.B.; Witt, B.L. Gastrocnemius recession. Foot Ankle Clin. 2014, 19, 767–786. [Google Scholar] [CrossRef]
- Trevino, S.; Gibbs, M.; Panchbhavi, V. Evaluation of results of endoscopic gastrocnemius recession. Foot Ankle Int. 2005, 26, 359–364. [Google Scholar] [CrossRef]
- Tashjian, R.Z.; Appel, A.J.; Banerjee, R.; DiGiovanni, C.W. Endoscopic gastrocnemius recession: Evaluation in a cadaver model. Foot Ankle Int. 2003, 24, 607–613. [Google Scholar] [CrossRef] [PubMed]
- Harris, R.C., 3rd; Strannigan, K.L.; Piraino, J. Comparison of the Complication Incidence in Open Versus Endoscopic Gastrocnemius Recession: A Retrospective Medical Record Review. J. Foot Ankle Surg. 2018, 57, 747–752. [Google Scholar] [CrossRef] [PubMed]
- Pinney, S.J.; Hansen, S.T., Jr.; Sangeorzan, B.J. The effect on ankle dorsiflexion of gastrocnemius recession. Foot Ankle Int. 2002, 23, 26–29. [Google Scholar] [CrossRef]
- Phisitkul, P.; Rungprai, C.; Femino, J.E.; Arunakul, M.; Amendola, A. Endoscopic Gastrocnemius Recession for the Treatment of Isolated Gastrocnemius Contracture: A Prospective Study on 320 Consecutive Patients. Foot Ankle Int. 2014, 35, 747–756. [Google Scholar] [CrossRef]
- Barouk, P. Technique, indications, and results of proximal medial gastrocnemius lengthening. Foot Ankle Clin. 2014, 19, 795–806. [Google Scholar] [CrossRef]
- Herzenberg, J.E.; Lamm, B.M.; Corwin, C.; Sekel, J. Isolated recession of the gastrocnemius muscle: The Baumann procedure. Foot Ankle Int. 2007, 28, 1154–1159. [Google Scholar] [CrossRef] [PubMed]
- Duthon, V.B.; Lübbeke, A.; Duc, S.R.; Stern, R.; Assal, M. Noninsertional Achilles tendinopathy treated with gastrocnemius lengthening. Foot Ankle Int. 2011, 32, 375–379. [Google Scholar] [CrossRef]
- Maskill, J.D.; Bohay, D.R.; Anderson, J.G. Gastrocnemius recession to treat isolated foot pain. Foot Ankle Int. 2010, 31, 19–23. [Google Scholar] [CrossRef]
- Saxena, A.; Gollwitzer, H.; Widtfeldt, A.; DiDomenico, L.A. Endoscopic gastrocnemius recession as therapy for gastrocnemius equinus. Z. Orthop. Unfall. 2007, 145, 499–504. [Google Scholar] [CrossRef]
- Saxena, A.; Widtfeldt, A. Endoscopic gastrocnemius recession: Preliminary report on 18 cases. J. Foot Ankle Surg. 2004, 43, 302–306. [Google Scholar] [CrossRef]
- Sammarco, G.J.; Bagwe, M.R.; Sammarco, V.J.; Magur, E.G. The effects of unilateral gastrocsoleus recession. Foot Ankle Int. 2006, 27, 508–511. [Google Scholar] [CrossRef] [PubMed]
- Rush, S.M.; Ford, L.A.; Hamilton, G.A. Morbidity associated with high gastrocnemius recession: Retrospective review of 126 cases. J. Foot Ankle Surg. 2006, 45, 156–160. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Baseline Characteristics | Endoscopic Group | Open Group | p Value |
|---|---|---|---|
| Sex | 0.768 | ||
| Male | 12 (54.5%) | 10 (50%) | |
| Female | 10 (45.5%) | 10 (50%) | |
| Age (years) | 19.9 ± 12.6 (8–53) | 32.4 ± 22.8 (6–74) | 0.117 |
| Follow-up time (month) | 19.1 ± 8.6 (7–32) | 13.9 ± 5.9 (7–26) | 0.056 |
| Foot | 0.638 | ||
| Left | 15 (44.1%) | 15 (50%) | |
| Right | 19 (55.9%) | 15 (50%) | |
| Flatfoot correction procedure | 0.537 | ||
| Subtalar arthroereisis | 24 (70.6%) | 19 (63.3%) | |
| Evans osteotomy | 10 (29.4%) | 11 (36.7%) |
| Indicators | Preoperative | Last Follow-Up | p Value |
|---|---|---|---|
| AOFAS score (points) | 50 (18) | 90 (13) | <0.001 |
| Maximum ankle dorsiflexion angle (degrees) | −7.7 (2.8) | 10.6 (3.6) | <0.001 |
| Indicators | Preoperative | Last Follow-Up | p Value |
|---|---|---|---|
| AOFAS score (points) | 47 (15) | 90 (18) | <0.001 |
| Maximum ankle dorsiflexion angle (degrees) | −7.6 (4.0) | 10.7 (3.3) | <0.001 |
| Indicators | Endoscopic Group | Open Group | p Value |
|---|---|---|---|
| Change values of the AOFAS score (points) | 39 (15) | 40.5 (11) | 0.322 |
| Change values of the maximum ankle dorsiflexion angle (degrees) | 19.5 (4.3) | 19.1 (4.9) | 0.856 |
| Levels | Endoscopic Group | Open Group | p Value |
|---|---|---|---|
| Very satisfied—5-point | 18 | 13 | 0.497 |
| Satisfied—4-point | 2 | 4 | |
| Fair—3-point | 2 | 2 | |
| Dissatisfied—2-point | 0 | 1 | |
| Very dissatisfied—1-point | 0 | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, Y.; Wang, Z.; Gan, Y.; Jiao, X.; Xu, C.; Zhao, J.; Dai, K. A Retrospective Comparative Study of Endoscopic Treatment of Gastrocnemius Contracture using the Modified Soft Tissue Release Kit. Medicina 2023, 59, 635. https://doi.org/10.3390/medicina59030635
Li Y, Wang Z, Gan Y, Jiao X, Xu C, Zhao J, Dai K. A Retrospective Comparative Study of Endoscopic Treatment of Gastrocnemius Contracture using the Modified Soft Tissue Release Kit. Medicina. 2023; 59(3):635. https://doi.org/10.3390/medicina59030635
Chicago/Turabian StyleLi, Yiming, Zengguang Wang, Yaokai Gan, Xin Jiao, Chen Xu, Jie Zhao, and Kerong Dai. 2023. "A Retrospective Comparative Study of Endoscopic Treatment of Gastrocnemius Contracture using the Modified Soft Tissue Release Kit" Medicina 59, no. 3: 635. https://doi.org/10.3390/medicina59030635