
Bone Marrow Aspirate Concentrate versus Human Umbilical Cord Blood-Derived Mesenchymal Stem Cells for Combined Cartilage Regeneration Procedure in Patients Undergoing High Tibial Osteotomy: A Systematic Review and Meta-Analysis

Abstract
:1. Introduction
2. Materials and Methods
2.1. Meta-Analyses Principles
2.2. Search Strategy
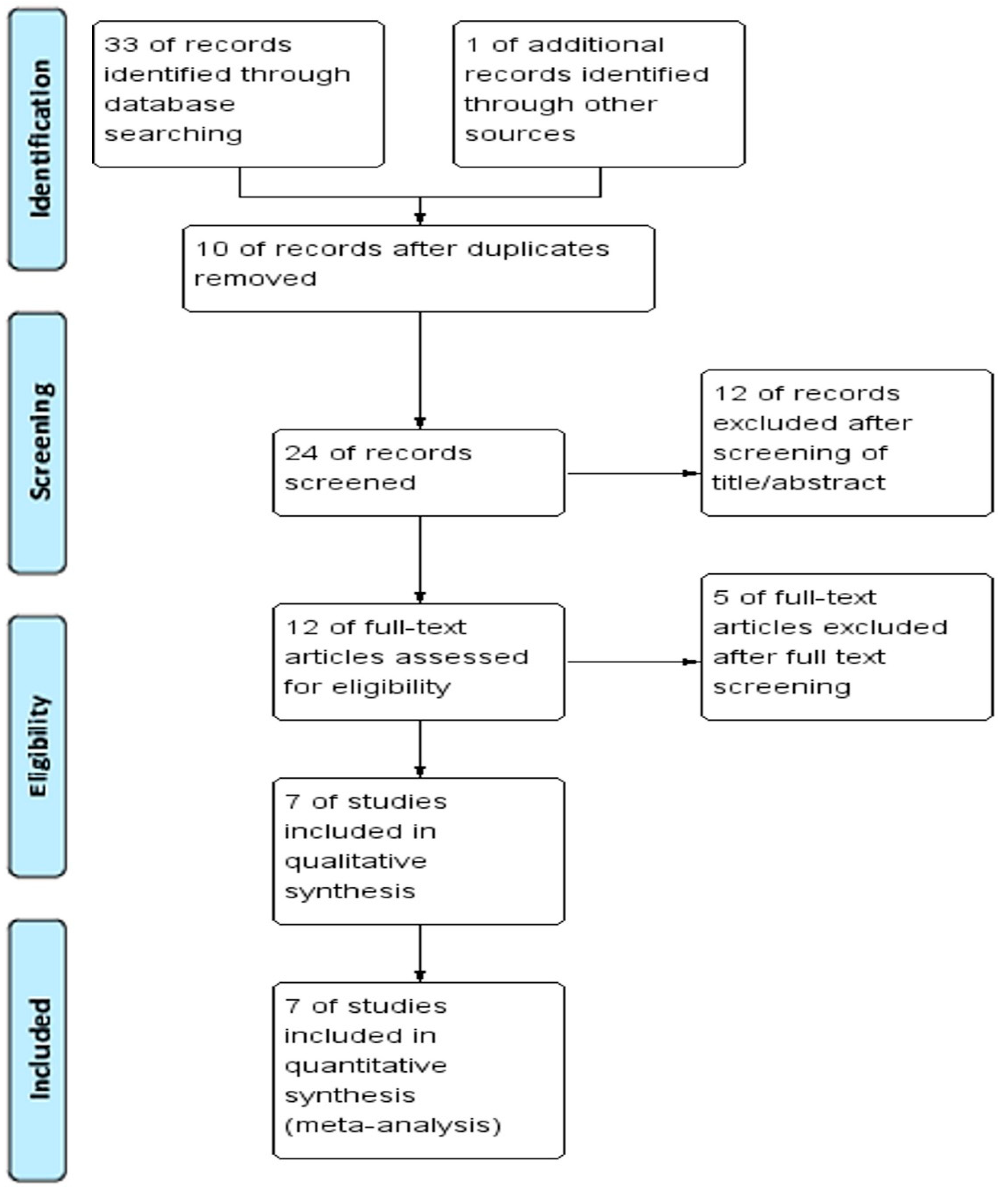
2.3. Study Criteria and Screening Process
2.4. Data Extraction and Quality Control
2.5. Statistical Analyses
3. Results
3.1. Study Characteristics
3.2. Methodological Quality

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Level of Evidence | Design | Type of Osteotomy | Intervention | Gender (M, F) | Age (Years) | BMI (kg/m2) | Number of Patients in Intervention Group |
|---|---|---|---|---|---|---|---|---|
| Cavallo, 2018 [35] | IV | retrospective case series study | HTO (medial opening-wedge) | bone marrow-derived cells + PRF | BMAC (15, 9) | 47.9 ± 12.3 | Not reported | 24 |
| Song, 2020 [36] | IV | retrospective case series study | HTO | hUCB-MSC + multiple holes | hUCB-MSC (2, 23) | 64.9 ± 4.4 | 24.9 ± 3.1 | 25 |
| Song, 2020 [37] | IV | retrospective case series study | HTO (uniplanar osteotomy) | hUCB-MSC + multiple holes | hUCB-MSC (30, 95) | 58.3 ± 6.8 | 25.6 ± 2.7 | 125 |
| Jin, 2021 [34] | III | retrospective comparative study | HTO (biplanar opening wedge osteotomy) | BMAC + MFx vs. MFx | BMAC (11, 37) | 56.9 ± 6.1 | 25.8 ± 3.1 (range, 18.1–33.2) | 48 |
| Chung, 2021 [38] | IV | retrospective case series study | HTO (biplanar opening wedge osteotomy) | hUCB-MSC + multiple drill holes | Not reported | 56.6 (range, 43–65) | 25.8 (range, 20.9–33.2) | 93 |
| Lee, 2021 [24] | III | retrospective comparative study | HTO (biplanar opening wedge osteotomy) | BMAC + MFx vs. hUCB-MSC + MFx | BMAC (6, 36); hUCB-MSC (6, 26) | BMAC, 60.7 ± 4.1; hUCB-MSC, 58.1 ± 3.6 | BMAC, 26.1 ± 2.8; hUCB-MSC, 26.6 ± 3 | BMAC (42), hUCB-MSC (32) |
| Yang, 2022 [23] | III | retrospective cohort study | HTO (biplanar opening wedge osteotomy) | BMAC + MFx vs. hUCB-MSC + MFx | BMAC (17, 38); hUCB-MSC (13, 42) | BMAC, 55.0 ± 7.3; hUCB-MSC, 56.4 ± 5.3 | BMAC, 27.2 ± 3.9 hUCB-MSC, 26.8 ± 3.2 | BMAC (55), hUCB-MSC (55) |
| Study | Pre-OP K-L Grade | Pre-OP ICRS Grade | Defect Size (MFC, cm2) | Mean Follow-Up (Months) | HKA Angle (Pre-OP vs. Post-OP) | Clinical Assessment | Number of Patients Undergoing 2nd-Look Arthroscopy | Post-OP ICRS-CRA Grade | Post-OP Koshino Staging |
|---|---|---|---|---|---|---|---|---|---|
| Cavallo, 2018 [35] | IV or less | Not reported | Not reported | 44.4 ± 17.7 | Pre-OP, varus 1–15°; Post-OP, Not reported | IKDC, KOOS, VAS, Tegner | NA | Not reported | Not reported |
| Song,2020 [36] | Not reported | Not reported | 7.2 ± 1.9 | 26.7 ± 1.8 | Pre-OP, ≥3°; Post-OP, Not reported | IKDC, VAS, WOMAC | 14 | I (6), II (8), III (0), IV (0) | Not reported |
| Song, 2020 [37] | III or less | IV (125) | 6.9 ± 2.0 | Not reported | Pre-OP, 7.6 ± 2.4; Post-OP, Not reported | IKDC, WOMAC, VAS | 125 | I (73), II (37), III (15), IV (0) | Not reported |
| Jin, 2021 [34] | III (36), IV (12) | III (41), IV (7) | 2.3 ± 0.9 | 33.6 ± 6.6 | 7.5 ± 3.4 vs. −2.9 ± 2.5 | IKDC, WOMAC, KSS-pain, KSS-function | 33 | I (1), II (18), III (11), IV (3) | A (2), B (15), C (16) |
| Chung, 2021 [38] | III | III or IV | 6.5 (range, 2.0–12.8) | 20.4 (range, 12–42) | Pre-OP, >3°; Post-OP, Not reported | IKDC, WOMAC, KSS-pain, KSS-function, HSS | 49 | I (4), II (34), III (11), IV (0) | A (0), B (12), C (37) |
| Lee, 2021 [24] | Not reported | BMAC, MFC 3.9 ± 0.3, MTC 3.9 ± 0.3; hUCB-MSC, MFC 3.9 ± 0.3, MTC 3.9 ± 0.3 | BMAC, 6.5 ± 2.9; hUCB-MSC, 7 ± 1.9 | BMAC, 20.7 ± 6.1; hUCB-MSC, 15.6 ± 2.8 | BMAC, 8.6 ± 3.1 vs. −2.8 ± 3.2; hUCB-MSC, 7.4 ± 2.6 vs. −2.9 ± 1.6 | HSS, WOMAC, KSS-pain, KSS-function | BMAC (42), hUCB-MSC (32) | BMAC (42), I (1), II (18), III (12), IV (11); hUCB-MSC (32), I (6), II (20), III (6), IV (0) | Not reported |
| Yang, 2022 [23] | III | BMAC (55), III (5), IV (50); hUCB-MSC (55), III (3), IV (52) | BMAC, 6.4 ± 3.1; hUCB-MSC, 6.2 ± 2.4 | BMAC, 34.2 ± 8.4; hUCB-MSC, 31.0 ± 6.0 | BMAC, 7.6 ± 2.9 vs. −1.5 ± 2.3; hUCB-MSC, 7.5 ± 2.7 vs. −1.6 ± 2.2 | IKDC, KOOS, SF-36, Tegner | BMAC (37), hUCB-MSC (44) | BMAC (37), I (1), II (20), III (11), IV (5); hUCB-MSC (44), I (4), II (30), III (10), IV (0) | BMAC (37), A (4), B (12), C (21); hUCB-MSC (44), A (0), B (12), C (32) |
| Study | Pre-OP BMAC or hUCB-MSC Preservation | Rehabilitation | Complication | Number of Patients in Control Group |
|---|---|---|---|---|
| Cavallo, 2018 [35] | 60 mL of bone marrow from the posterior iliac crest, 15 min centrifugation cycles, a collagen scaffold | Partial weight-bearing was after six weeks; full weight-bearing at eight weeks after evaluation of bone consolidation | Knee swelling due to hemarthrosis in three cases; two cases of infrapatellar nerve injury; one case of delayed union of the osteotomy | NA |
| Song, 2020 [36] | hUCB-MSCs were used as a stem cell drug (CARTISTEM, MEDIPost-OP), mixed with sodium hyaluronate, therapeutic dosage 500 μL/cm2 of the defect area with a cell concentration of 0.5 × 107 cells/mL | Non-weight-bearing for eight weeks, full weight-bearing after twelve weeks | Not reported | NA |
| Song, 2020 [37] | CARTISTEM® (MediPost-OP, Seongnam-si, Gyeonggi-do, Republic of Korea), 1.5 mL hUCB-MSCs (7.5 × 106 cells/vial) and 4% hyaluronic acid (HA) hydrogel, therapeutic dose 500 mL/cm2 | Partial weight-bearing after four weeks; full weight-bearing at six weeks | Not reported | NA |
| Jin, 2021 [34] | contralateral anterior superior iliac spine, at least 40 mL of bone marrow, centrifuged for 4 min at 2500 rpm | Non-weight-bearing to partial weight-bearing after six weeks; full weight-bearing after twelve weeks considering bone healing | Not reported | MFx (43) |
| Chung, 2021 [38] | Cartistem, 1.5 mL of cord blood-derived MSCs (7.5 × 106) and 4% HA, 500 mL/cm2 of defect with a cell concentration of 0.5 × 107 cells/mL | Non-weight-bearing to partial weight-bearing walking after six weeks; full weight-bearing after twelve weeks based on the level of bone healing | Some patients, knee swelling for up to one month | NA |
| Lee, 2021 [24] | BMAC, contralateral anterior superior iliac spine, at least 40 mL of bone marrow, centrifuge for 4 min at 2500 rpm; Cartistem, hUCB-MSCs-HA hydrogel composites | Non-weight-bearing to partial weight-bearing after six weeks; full weight-bearing after twelve weeks depending on the level of bone healing | Not reported | NA |
| Yang, 2022 [23] | BMAC, contralateral anterior superior iliac spine, at least 40 mL of bone marrow, centrifuged for 4 min at 2500 rpm; Cartistem, 1.5 mL of cord blood-derived MSCs (7.5 × 106) and 4% HA, 500 mL/cm2 of defect with a cell concentration of 0.5 × 107 cells/mL | Partial weight-bearing after six weeks; full weight-bearing after twelve weeks. | BMAC: one patient complained of postoperative stiffness | NA |
3.3. Meta-Analysis Results
3.3.1. Clinical Outcomes
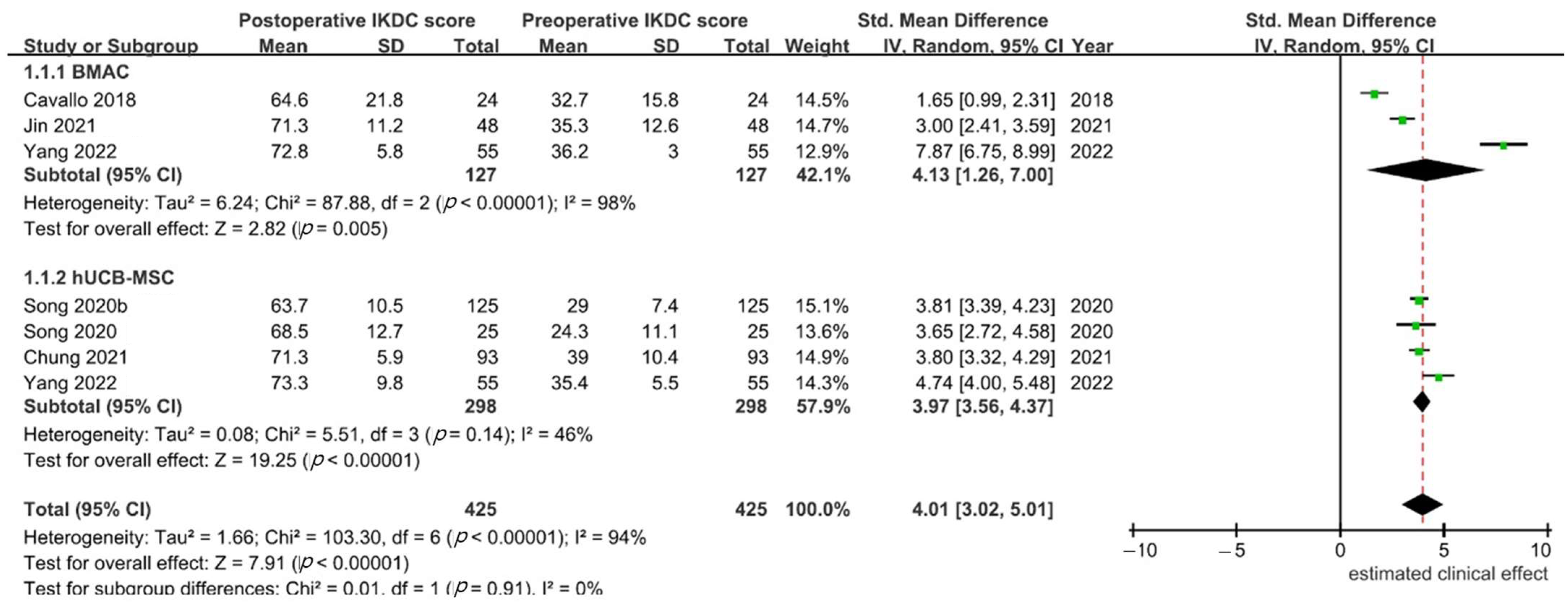
- IKDC: In six [23,34,35,36,37,38] of the seven studies, the IKDC score used to evaluate the clinical effects of BMAC or hUCB-MSCs with HTO in patients with varus knee OA was reported. The IKDC subgroup consisted of 127 patients treated using BMAC, and 298 patients treated using hUCB-MSCs. Significant heterogeneity was found (p < 0.001, I2 = 94%), and the random effects model was used. Patients treated with BMAC had significantly improved IKDC scores (SMD, 4.13; 95% CI, 1.23–7.00), as did those in the hUCB-MSC group (SMD, 3.92; 95% CI, 3.65–4.20). However, based on IKDC score, the clinical effects of BMAC vs. hUCB-MSCs for combined cartilage regeneration in patients undergoing HTO were equivalent (p = 0.91; Figure 2).
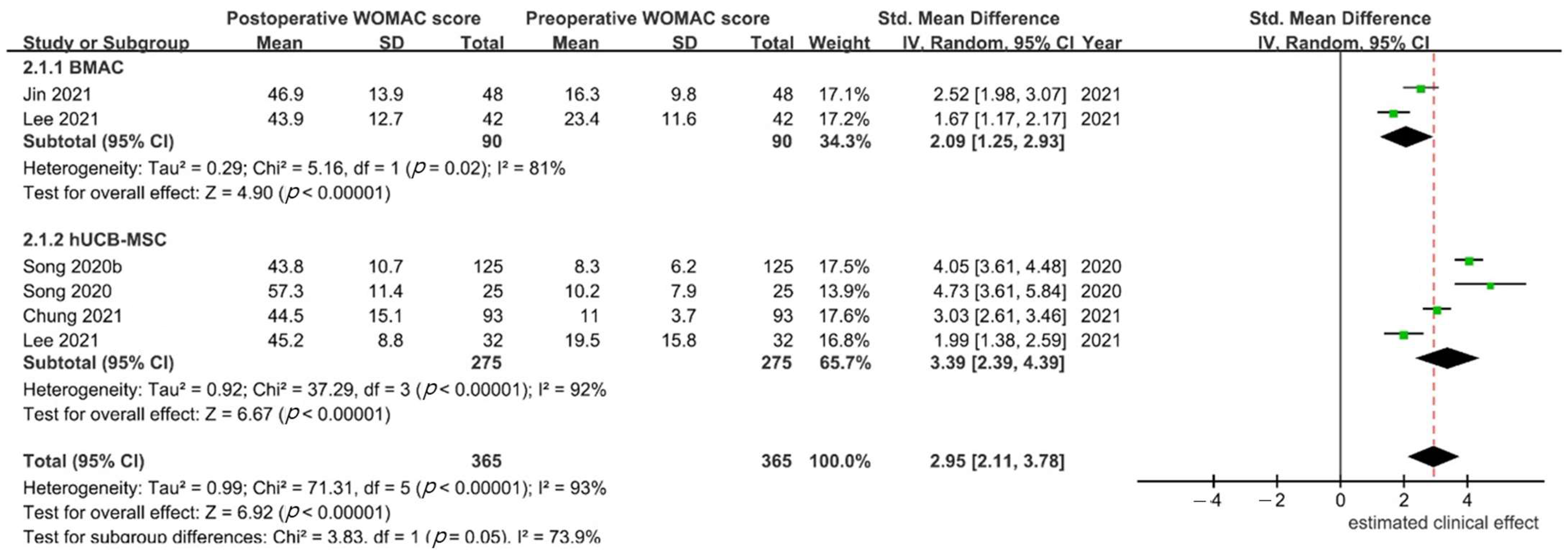
- WOMAC: In 5 studies [24,34,36,37,38], the WOMAC score was reported, and 90 and 275 participants were included in the BMAC and hUCB-MSC groups, respectively. Since only one [38] of five studies reported WOMAC subscales, while the other four reported only a total WOMAC score, and only the total WOMAC score was compared. Significant heterogeneity was found (p < 0.001; I2 = 93%), and a random effects model was used. Based on the WOMAC index, both BMAC and hUCB-MSCs had a significant clinical effect compared with the preoperative status (SMD 2.09, 95% CI, 1.25–2.93 for BMAC and 3.39, 95% CI, 2.39–4.397 for hUCB-MSCs). However, the difference between groups did not reach statistical significance (p = 0.05; Figure 3).
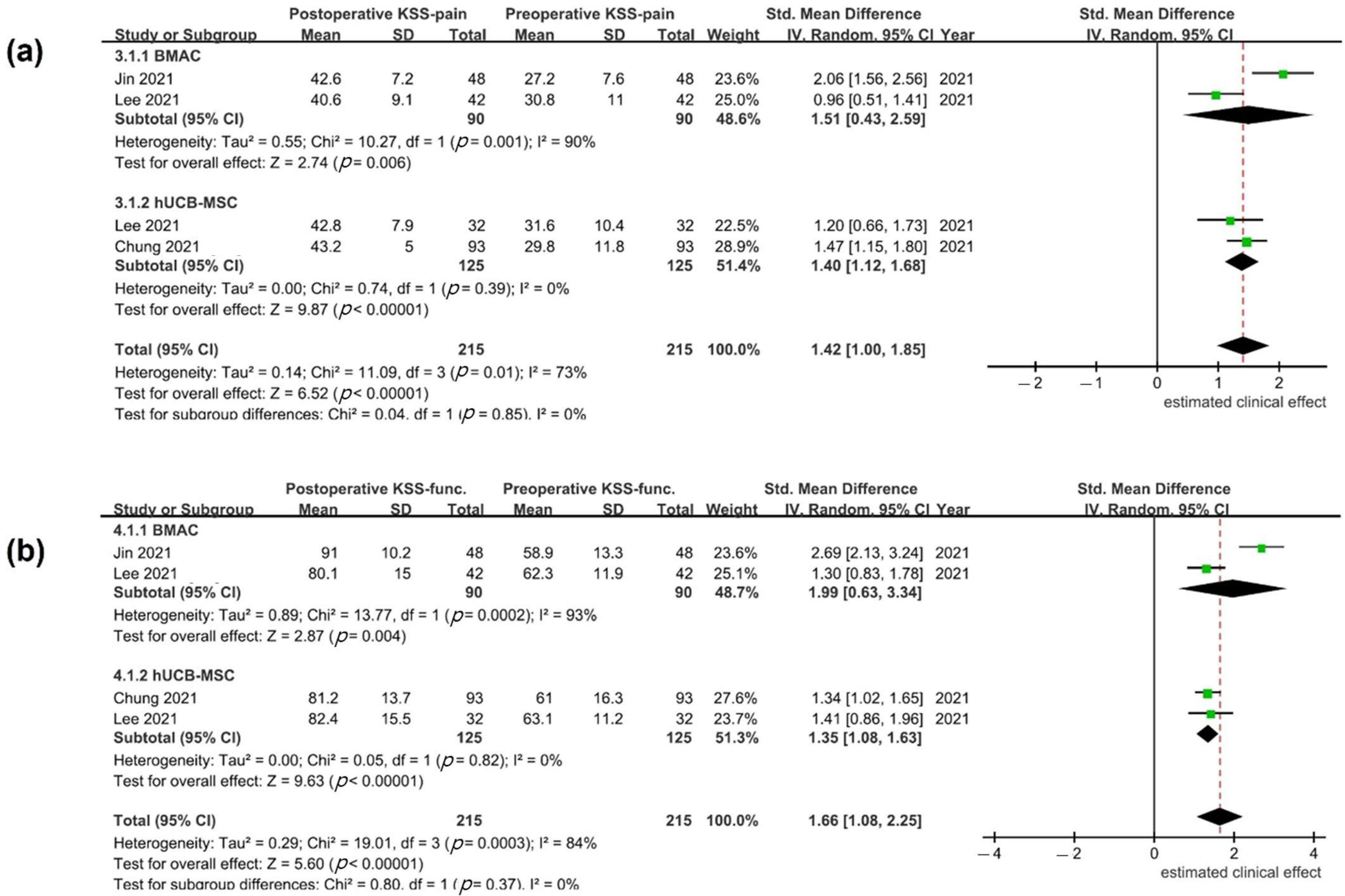
- Other reported clinical outcomes: Other reported outcomes were KSS score (three studies), VAS (three studies), KOOS (two studies), HSS (two studies), SF-36 (one study), and Tegner activity score (two studies). The mean preoperative and postoperative values for the outcome scales are shown in Table 4. KSS was the only measure used in more than one study to evaluate BMAC and hUCB-MSCs; it was used in three studies [24,34,38]. Mean KSS subscale (pain and function) values were reported in all studies; statistically significant heterogeneity was detected (KSS pain, p = 0.01, I2 = 73%; KSS function, p < 0.001, I2 = 84%). In a random effects model, patients treated with BMAC or hUCB-MSCs showed improved clinical outcome after surgery (KSS pain SMD, 1.51, 95% CI, 0.43–2.59 for BMAC and 1.40; 95% CI, 1.12–1.68 for hUCB-MSCs; KSS function SMD, 1.99, 95% CI, 0.63–3.34 for BMAC and 1.35; 95% CI, 1.08–1.63 for hUCB-MSCs). However, differences in KSS pain and function scores were not found between the two treatment groups (p = 0.85 and p = 0.37, respectively; Figure 4).
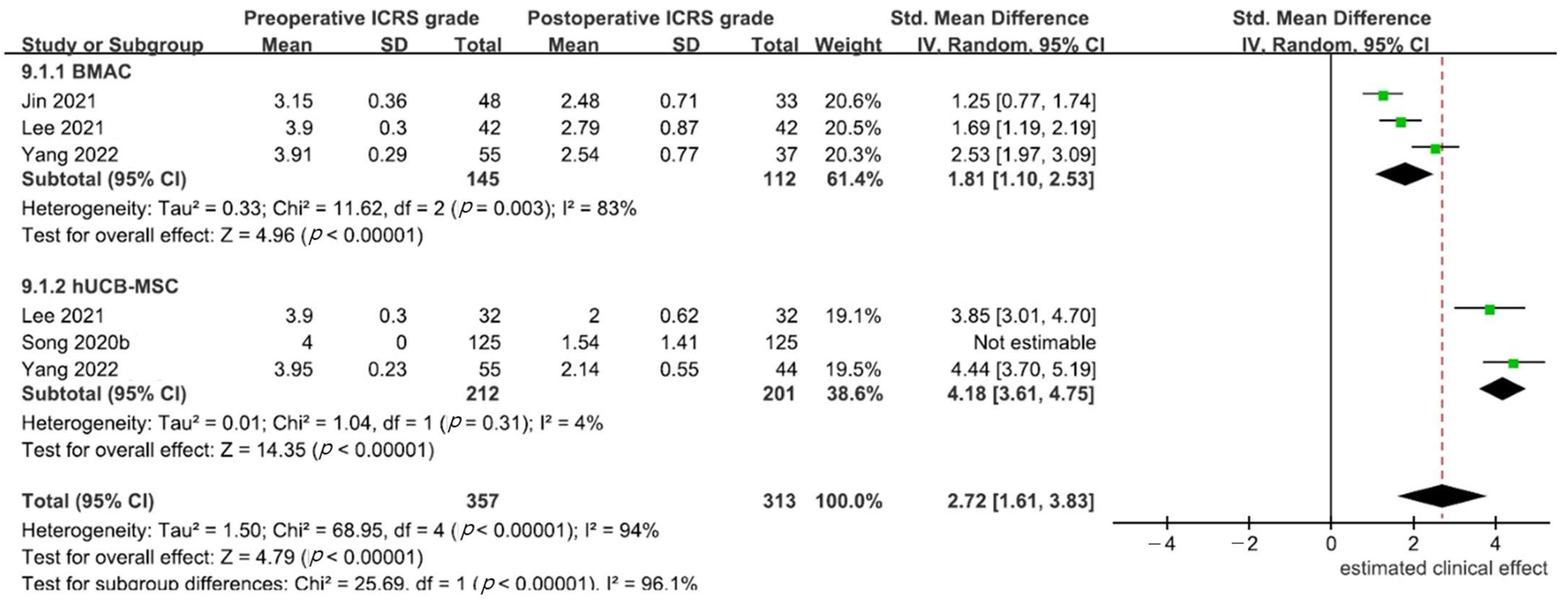
3.3.2. Second-Look Arthroscopic Findings
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Biant, L.C.; McNicholas, M.J.; Sprowson, A.P.; Spalding, T. The surgical management of symptomatic articular cartilage defects of the knee: Consensus statements from United Kingdom knee surgeons. Knee 2015, 22, 446–449. [Google Scholar] [CrossRef] [PubMed]
- Akizuki, S.; Shibakawa, A.; Takizawa, T.; Yamazaki, I.; Horiuchi, H. The long-term outcome of high tibial osteotomy: A ten- to 20-year follow-up. J. Bone Joint. Surg. Br. 2008, 90, 592–596. [Google Scholar] [CrossRef] [PubMed]
- Amendola, A.; Bonasia, D.E. Results of high tibial osteotomy: Review of the literature. Int. Orthop. 2010, 34, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Matsunaga, D.; Akizuki, S.; Takizawa, T.; Yamazaki, I.; Kuraishi, J. Repair of articular cartilage and clinical outcome after osteotomy with microfracture or abrasion arthroplasty for medial gonarthrosis. Knee 2007, 14, 465–471. [Google Scholar] [CrossRef] [PubMed]
- Kanamiya, T.; Naito, M.; Hara, M.; Yoshimura, I. The influences of biomechanical factors on cartilage regeneration after high tibial osteotomy for knees with medial compartment osteoarthritis: Clinical and arthroscopic observations. Arthroscopy 2002, 18, 725–729. [Google Scholar] [CrossRef] [PubMed]
- Niemeyer, P.; Stöhr, A.; Köhne, M.; Hochrein, A. Medial opening wedge high tibial osteotomy. Oper. Orthop. Traumatol. 2017, 29, 294–305. [Google Scholar] [CrossRef] [PubMed]
- Jung, W.-H.; Takeuchi, R.; Chun, C.-W.; Lee, J.-S.; Ha, J.-H.; Kim, J.-H.; Jeong, J.-H. Second-look arthroscopic assessment of cartilage regeneration after medial opening-wedge high tibial osteotomy. Arthroscopy 2014, 30, 72–79. [Google Scholar] [CrossRef] [PubMed]
- Hui, C.; Salmon, L.J.; Kok, A.; Williams, H.A.; Hockers, N.; van der Tempel, W.M.; Chana, R.; Pinczewski, L.A. Long-term survival of high tibial osteotomy for medial compartment osteoarthritis of the knee. Am. J. Sports Med. 2011, 39, 64–70. [Google Scholar] [CrossRef]
- Wu, L.-D.; Hahne, H.J.; Hassenpflug, T. A long-term follow-up study of high tibial osteotomy for medial compartment osteoarthrosis. Chin. J. Traumatol. 2004, 7, 348–353. [Google Scholar]
- Lee, O.-S.; Ahn, S.; Ahn, J.H.; Teo, S.H.; Lee, Y.S. Effectiveness of concurrent procedures during high tibial osteotomy for medial compartment osteoarthritis: A systematic review and meta-analysis. Arch. Orthop. Trauma Surg. 2018, 138, 227–236. [Google Scholar] [CrossRef]
- Ha, C.-W.; Park, Y.-B.; Kim, S.H.; Lee, H.-J. Intra-articular Mesenchymal Stem Cells in Osteoarthritis of the Knee: A Systematic Review of Clinical Outcomes and Evidence of Cartilage Repair. Arthroscopy 2019, 35, 277–288.e2. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Djaja, Y.P.; Park, Y.-B.; Park, J.-G.; Ko, Y.-B.; Ha, C.-W. Intra-articular Injection of Culture-Expanded Mesenchymal Stem Cells Without Adjuvant Surgery in Knee Osteoarthritis: A Systematic Review and Meta-analysis. Am. J. Sports Med. 2020, 48, 2839–2849. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.S.; Koh, Y.G. Comparative Matched-Pair Analysis of Open-Wedge High Tibial Osteotomy With Versus Without an Injection of Adipose-Derived Mesenchymal Stem Cells for Varus Knee Osteoarthritis: Clinical and Second-Look Arthroscopic Results. Am. J. Sports Med. 2018, 46, 2669–2677. [Google Scholar] [CrossRef] [PubMed]
- Koh, Y.-G.; Kwon, O.-R.; Kim, Y.-S.; Choi, Y.-J. Comparative outcomes of open-wedge high tibial osteotomy with platelet-rich plasma alone or in combination with mesenchymal stem cell treatment: A prospective study. Arthroscopy 2014, 30, 1453–1460. [Google Scholar] [CrossRef] [PubMed]
- Wong, K.L.; Lee, K.B.; Tai, B.C.; Law, P.; Lee, E.H.; Hui, J.H. Injectable cultured bone marrow-derived mesenchymal stem cells in varus knees with cartilage defects undergoing high tibial osteotomy: A prospective, randomized controlled clinical trial with 2 years’ follow-up. Arthroscopy 2013, 29, 2020–2028. [Google Scholar] [CrossRef]
- Park, Y.-B.; Ha, C.-W.; Rhim, J.H.; Lee, H.-J. Stem Cell Therapy for Articular Cartilage Repair: Review of the Entity of Cell Populations Used and the Result of the Clinical Application of Each Entity. Am. J. Sports Med. 2018, 46, 2540–2552. [Google Scholar] [CrossRef]
- Scharstuhl, A.; Schewe, B.; Benz, K.; Gaissmaier, C.; Bühring, H.-J.; Stoop, R. Chondrogenic potential of human adult mesenchymal stem cells is independent of age or osteoarthritis etiology. Stem Cells 2007, 25, 3244–3251. [Google Scholar] [CrossRef]
- Ando, W.; Tateishi, K.; Katakai, D.; Hart, D.A.; Higuchi, C.; Nakata, K.; Hashimoto, J.; Fujie, H.; Shino, K.; Yoshikawa, H.; et al. In vitro generation of a scaffold-free tissue-engineered construct (TEC) derived from human synovial mesenchymal stem cells: Biological and mechanical properties and further chondrogenic potential. Tissue Eng. Part A 2008, 14, 2041–2049. [Google Scholar] [CrossRef]
- Kern, S.; Eichler, H.; Stoeve, J.; Klüter, H.; Bieback, K. Comparative analysis of mesenchymal stem cells from bone marrow, umbilical cord blood, or adipose tissue. Stem Cells 2006, 24, 1294–1301. [Google Scholar] [CrossRef]
- Flynn, A.; Barry, F.; O’Brien, T. UC blood-derived mesenchymal stromal cells: An overview. Cytotherapy 2007, 9, 717–726. [Google Scholar] [CrossRef]
- Kahlenberg, C.A.; Nwachukwu, B.U.; Hamid, K.S.; Steinhaus, M.E.; Williams, R.J., 3rd. Analysis of Outcomes for High Tibial Osteotomies Performed With Cartilage Restoration Techniques. Arthroscopy 2017, 33, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Wen, H.-J.; Yuan, L.-B.; Tan, H.-B.; Xu, Y.-Q. Microfracture versus Enhanced Microfracture Techniques in Knee Cartilage Restoration: A Systematic Review and Meta-Analysis. J. Knee Surg. 2022, 35, 707–717. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.-Y.; Song, E.-K.; Kang, S.-J.; Kwak, W.-K.; Kang, J.-K.; Seon, J.-K. Allogenic umbilical cord blood-derived mesenchymal stromal cell implantation was superior to bone marrow aspirate concentrate augmentation for cartilage regeneration despite similar clinical outcomes. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 208–218. [Google Scholar] [CrossRef] [PubMed]
- Lee, N.-H.; Na, S.-M.; Ahn, H.-W.; Kang, J.-K.; Seon, J.-K.; Song, E.-K. Allogenic Human Umbilical Cord Blood-Derived Mesenchymal Stem Cells Are More Effective Than Bone Marrow Aspiration Concentrate for Cartilage Regeneration After High Tibial Osteotomy in Medial Unicompartmental Osteoarthritis of Knee. Arthroscopy 2021, 37, 2521–2530. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed]
- Kohn, M.D.; Sassoon, A.A.; Fernando, N.D. Classifications in Brief: Kellgren-Lawrence Classification of Osteoarthritis. Clin. Orthop. Relat. Res. 2016, 474, 1886–1893. [Google Scholar] [CrossRef] [PubMed]
- van den Borne, M.P.; Raijmakers, N.J.; Vanlauwe, J.; Victor, J.; de Jong, S.N.; Bellemans, J.; Saris, D.B. International Cartilage Repair Society (ICRS) and Oswestry macroscopic cartilage evaluation scores validated for use in Autologous Chondrocyte Implantation (ACI) and microfracture. Osteoarthr. Cartil. 2007, 15, 1397–1402. [Google Scholar] [CrossRef]
- Sumida, Y.; Nakamura, K.; Feil, S.; Siebold, M.; Kirsch, J.; Siebold, R. Good healing potential of patellar chondral defects after all-arthroscopic autologous chondrocyte implantation with spheroids: A second-look arthroscopic assessment. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 1535–1542. [Google Scholar] [CrossRef] [PubMed]
- Koshino, T.; Wada, S.; Ara, Y.; Saito, T. Regeneration of degenerated articular cartilage after high tibial valgus osteotomy for medial compartmental osteoarthritis of the knee. Knee 2003, 10, 229–236. [Google Scholar] [CrossRef]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Weir, C.J.; Butcher, I.; Assi, V.; Lewis, S.C.; Murray, G.D.; Langhorne, P.; Brady, M.C. Dealing with missing standard deviation and mean values in meta-analysis of continuous outcomes: A systematic review. BMC Med Res. Methodol. 2018, 18, 25. [Google Scholar] [CrossRef]
- Higgins, L.D.; Taylor, M.K.; Park, D.; Ghodadra, N.; Marchant, M.; Pietrobon, R.; Cook, C. Reliability and validity of the International Knee Documentation Committee (IKDC) Subjective Knee Form. Jt. Bone Spine 2007, 74, 594–599. [Google Scholar] [CrossRef] [PubMed]
- Thumboo, J.; Chew, L.H.; Soh, C.H. Validation of the Western Ontario and Mcmaster University osteoarthritis index in Asians with osteoarthritis in Singapore. Osteoarthr. Cartil. 2001, 9, 440–446. [Google Scholar] [CrossRef] [PubMed]
- Jin, Q.-H.; Chung, Y.-W.; Na, S.-M.; Ahn, H.-W.; Jung, D.-M.; Seon, J.-K. Bone marrow aspirate concentration provided better results in cartilage regeneration to microfracture in knee of osteoarthritic patients. Knee Surg. Sports Traumatol. Arthrosc. 2021, 29, 1090–1097. [Google Scholar] [CrossRef] [PubMed]
- Cavallo, M.; Sayyed-Hosseinian, S.-H.; Parma, A.; Buda, R.; Mosca, M.; Giannini, S. Combination of High Tibial Osteotomy and Autologous Bone Marrow Derived Cell Implantation in Early Osteoarthritis of Knee: A Preliminary Study. Arch. Bone Jt. Surg. 2018, 6, 112–118. [Google Scholar] [PubMed]
- Song, J.-S.; Hong, K.-T.; Kim, N.-M.; Park, H.-S.; Choi, N.-H. Human umbilical cord blood-derived mesenchymal stem cell implantation for osteoarthritis of the knee. Arch. Orthop. Trauma Surg. 2020, 140, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Song, J.-S.; Hong, K.-T.; Kong, C.-G.; Kim, N.-M.; Jung, J.-Y.; Park, H.-S.; Kim, Y.J.; Chang, K.B.; Kim, S.J. High tibial osteotomy with human umbilical cord blood-derived mesenchymal stem cells implantation for knee cartilage regeneration. World J. Stem Cells 2020, 12, 514–526. [Google Scholar] [CrossRef]
- Chung, Y.-W.; Yang, H.-Y.; Kang, S.-J.; Song, E.-K.; Seon, J.-K. Allogeneic umbilical cord blood-derived mesenchymal stem cells combined with high tibial osteotomy: A retrospective study on safety and early results. Int. Orthop. 2021, 45, 481–488. [Google Scholar] [CrossRef]
- Sterett, W.I.; Steadman, J.R.; Huang, M.J.; Matheny, L.M.; Briggs, K.K. Chondral resurfacing and high tibial osteotomy in the varus knee: Survivorship analysis. Am. J. Sports Med. 2010, 38, 1420–1424. [Google Scholar] [CrossRef]
- Betzler, B.K.; Chew, A.H.B.M.R.; Razak, H.R.B.A. Intra-articular injection of orthobiologics in patients undergoing high tibial osteotomy for knee osteoarthritis is safe and effective—A systematic review. J. Exp. Orthop. 2021, 8, 83. [Google Scholar] [CrossRef]
- Turner, L.G. Federal Regulatory Oversight of US Clinics Marketing Adipose-Derived Autologous Stem Cell Interventions: Insights From 3 New FDA Draft Guidance Documents. Mayo Clin. Proc. 2015, 90, 567–571. [Google Scholar] [CrossRef] [PubMed]
- Jäger, M.; Hernigou, P.; Zilkens, C.; Herten, M.; Li, X.; Fischer, J.; Krauspe, R. Cell therapy in bone healing disorders. Orthop. Rev. 2010, 2, e20. [Google Scholar]
- Cavallo, C.; Boffa, A.; de Girolamo, L.; Merli, G.; Kon, E.; Cattini, L.; Santo, E.; Grigolo, B.; Filardo, G. Bone marrow aspirate concentrate quality is affected by age and harvest site. Knee Surg. Sports Traumatol. Arthrosc. 2022. [Google Scholar] [CrossRef] [PubMed]
- Chahla, J.; Mannava, S.; Cinque, M.E.; Geeslin, A.G.; Codina, D.; LaPrade, R.F. Bone Marrow Aspirate Concentrate Harvesting and Processing Technique. Arthrosc. Tech. 2017, 6, e441–e445. [Google Scholar] [CrossRef] [PubMed]
- Steinert, A.F.; Rackwitz, L.; Gilbert, F.; Nöth, U.; Tuan, R.S. Concise review: The clinical application of mesenchymal stem cells for musculoskeletal regeneration: Current status and perspectives. Stem. Cells Transl. Med. 2012, 1, 237–247. [Google Scholar] [CrossRef]
- Madry, H.; Gao, L.; Eichler, H.; Orth, P.; Cucchiarini, M. Bone Marrow Aspirate Concentrate-Enhanced Marrow Stimulation of Chondral Defects. Stem Cells Int. 2017, 2017, 1609685. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.-B.; Ha, C.-W.; Lee, C.-H.; Yoon, Y.C.; Park, Y. Cartilage Regeneration in Osteoarthritic Patients by a Composite of Allogeneic Umbilical Cord Blood-Derived Mesenchymal Stem Cells and Hyaluronate Hydrogel: Results from a Clinical Trial for Safety and Proof-of-Concept with 7 Years of Extended Follow-Up. Stem Cells Transl. Med. 2017, 6, 613–621. [Google Scholar] [CrossRef] [PubMed]
- Song, J.-S.; Hong, K.-T.; Kim, N.-M.; Jung, J.-Y.; Park, H.-S.; Lee, S.H.; Cho, Y.J.; Kim, S.J. Implantation of allogenic umbilical cord blood-derived mesenchymal stem cells improves knee osteoarthritis outcomes: Two-year follow-up. Regen. Ther. 2020, 14, 32–39. [Google Scholar] [CrossRef]
- Yang, S.-E.; Ha, C.-W.; Jung, M.; Jin, H.-J.; Lee, M.; Song, H.; Choi, S.; Oh, W.; Yang, Y.-S. Mesenchymal stem/progenitor cells developed in cultures from UC blood. Cytotherapy 2004, 6, 476–486. [Google Scholar] [CrossRef]
- Agneskirchner, J.D.; Hurschler, C.; Wrann, C.D.; Lobenhoffer, P. The effects of valgus medial opening wedge high tibial osteotomy on articular cartilage pressure of the knee: A biomechanical study. Arthroscopy 2007, 23, 852–861. [Google Scholar] [CrossRef]
- Bagno, L.; Hatzistergos, K.E.; Balkan, W.; Hare, J.M. Mesenchymal Stem Cell-Based Therapy for Cardiovascular Disease: Progress and Challenges. Mol. Ther. 2018, 26, 1610–1623. [Google Scholar] [CrossRef] [PubMed]
- Galipeau, J.; Sensébé, L. Mesenchymal Stromal Cells: Clinical Challenges and Therapeutic Opportunities. Cell Stem Cell 2018, 22, 824–833. [Google Scholar] [CrossRef] [PubMed]





| Study | Reported Outcomes | IKDC | WOMAC | KSS-Pain | KSS-Function | KOOS | VAS | HSS | SF-36 | Tegner |
|---|---|---|---|---|---|---|---|---|---|---|
| Cavallo, 2018 [35] | IKDC, KOOS, VAS, Tegner | BMAC, 32.7 ± 15.8 vs. 64.6 ± 21.8 | - | - | - | BMAC, 30.46 ± 11.67 vs. 72.38 ± 20.1 | BMAC, 7.50 ± 1.24 vs. 3.00 ± 2.08 | - | - | BMAC, 1.21 ± 1.02 vs. 2.12 ± 1.39 |
| Song, 2020 [36] | IKDC, VAS, WOMAC | hUCB-MSC, 24.3 ± 11.1 vs. 68.5 ± 12.7 | hUCB-MSC, 57.3 ± 11.4 vs. 10.2 ± 7.9 | - | - | - | hUCB-MSC, 76.4 ± 16.6 vs. 12.8 ± 11.7 | - | - | - |
| Song, 2020 [37] | IKDC, WOMAC, VAS | hUCB-MSC, 29 ± 7.4 vs. 63.7 ± 10.5 | hUCB-MSC, 43.8 ± 10.7 vs. 8.3 ± 6.2 | - | - | - | hUCB-MSC, 7.6 ± 1.36 vs. 1.7 ± 1.4 | - | - | - |
| Jin, 2021 [34] | IKDC, WOMAC, KSS-pain, KSS-function | BMAC, 35.3 ± 12.6 vs. 71.3 ± 11.2 | BMAC, 46.9 ± 13.9 vs. 16.3 ± 9.8 | BMAC, 27.2 ± 7.6 vs. 42.6 ± 7.2 | BMAC, 58.9 ± 13.3 vs. 91.0 ± 10.2 | - | - | - | - | - |
| Chung, 2021 [38] | IKDC, WOMAC, KSS-pain, KSS-function, HSS | hUCB-MSC, 39.0 ± 10.4 vs. 71.3 ± 5.9 | hUCB-MSC, 44.5 ± 15.1 vs. 11.0 ± 3.7 | hUCB-MSC, 29.8 ± 11.8 vs. 43.2 ± 5.0 | hUCB-MSC, 61.0 ± 16.3 vs. 81.2 ± 13.7 | - | - | hUCB-MSC, 61.6 ± 12.9 vs. 82.7 ± 13.5 | - | - |
| Lee, 2021 [24] | HSS, WOMAC, KSS-pain, KSS-function | - | BMAC, 43.9 ± 12.7 vs. 23.4 ± 11.6; hUCB-MSC, 45.2 ± 8.8 vs. 19.5 ± 15.8 | BMAC, 30.8 ± 11.0 vs. 40.6 ± 6.1; hUCB-MSC, 31.6 ± 10.4 vs. 42.8 ± 7.9 | BMAC, 62.3 ± 11.9 vs. 80.1 ± 15.0; hUCB-MSC, 63.1 ± 11.2 vs. 82.4 ± 15.5 | - | - | BMAC, 57.9 ± 12.9 vs. 79.2 ± 11.5; hUCB-MSC, 56.1 ± 10.6 vs. 84.6 ± 15.5 | - | - |
| Yang, 2022 [23] | IKDC, KOOS, SF-36, Tegner | BMAC, 43.9 ± 12.7 vs. 23.4 ± 11.6; hUCB-MSC, 45.2 ± 8.8 vs. 19.5 ± 15.8 | - | - | - | BMAC, 37.7 ± 2.7 vs. 78.2 ± 7.9; hUCB-MSC, 36.8 ± 7.1 vs. 78.4 ± 8.6 | - | - | BMAC, 43.6 ± 10.4 vs. 64.0 ± 11.6; hUCB-MSC, 45.8 ± 12.3 vs. 64.5 ± 11.9 | BMAC, 2.3 ± 0.9 vs. 4.0 ± 0.5; hUCB-MSC, 2.2 ± 0.8 vs. 4.1 ± 0.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, D.; Choi, Y.H.; Kang, S.H.; Koh, H.S.; In, Y. Bone Marrow Aspirate Concentrate versus Human Umbilical Cord Blood-Derived Mesenchymal Stem Cells for Combined Cartilage Regeneration Procedure in Patients Undergoing High Tibial Osteotomy: A Systematic Review and Meta-Analysis. Medicina 2023, 59, 634. https://doi.org/10.3390/medicina59030634
Park D, Choi YH, Kang SH, Koh HS, In Y. Bone Marrow Aspirate Concentrate versus Human Umbilical Cord Blood-Derived Mesenchymal Stem Cells for Combined Cartilage Regeneration Procedure in Patients Undergoing High Tibial Osteotomy: A Systematic Review and Meta-Analysis. Medicina. 2023; 59(3):634. https://doi.org/10.3390/medicina59030634
Chicago/Turabian StylePark, Dojoon, Youn Ho Choi, Se Hyun Kang, Hae Seok Koh, and Yong In. 2023. "Bone Marrow Aspirate Concentrate versus Human Umbilical Cord Blood-Derived Mesenchymal Stem Cells for Combined Cartilage Regeneration Procedure in Patients Undergoing High Tibial Osteotomy: A Systematic Review and Meta-Analysis" Medicina 59, no. 3: 634. https://doi.org/10.3390/medicina59030634