


The Recurrence of Ptosis after Correction Surgery Is Associated with Refractive Error
Abstract
:1. Introduction
2. Methods
2.1. Inclusion and Exclusion Criteria
2.2. Ophthalmologic Examination
2.3. Surgical Technique
2.4. Evaluation of Recurrence
2.5. Statistical Analysis
3. Results
3.1. Demographic and Clinical Data
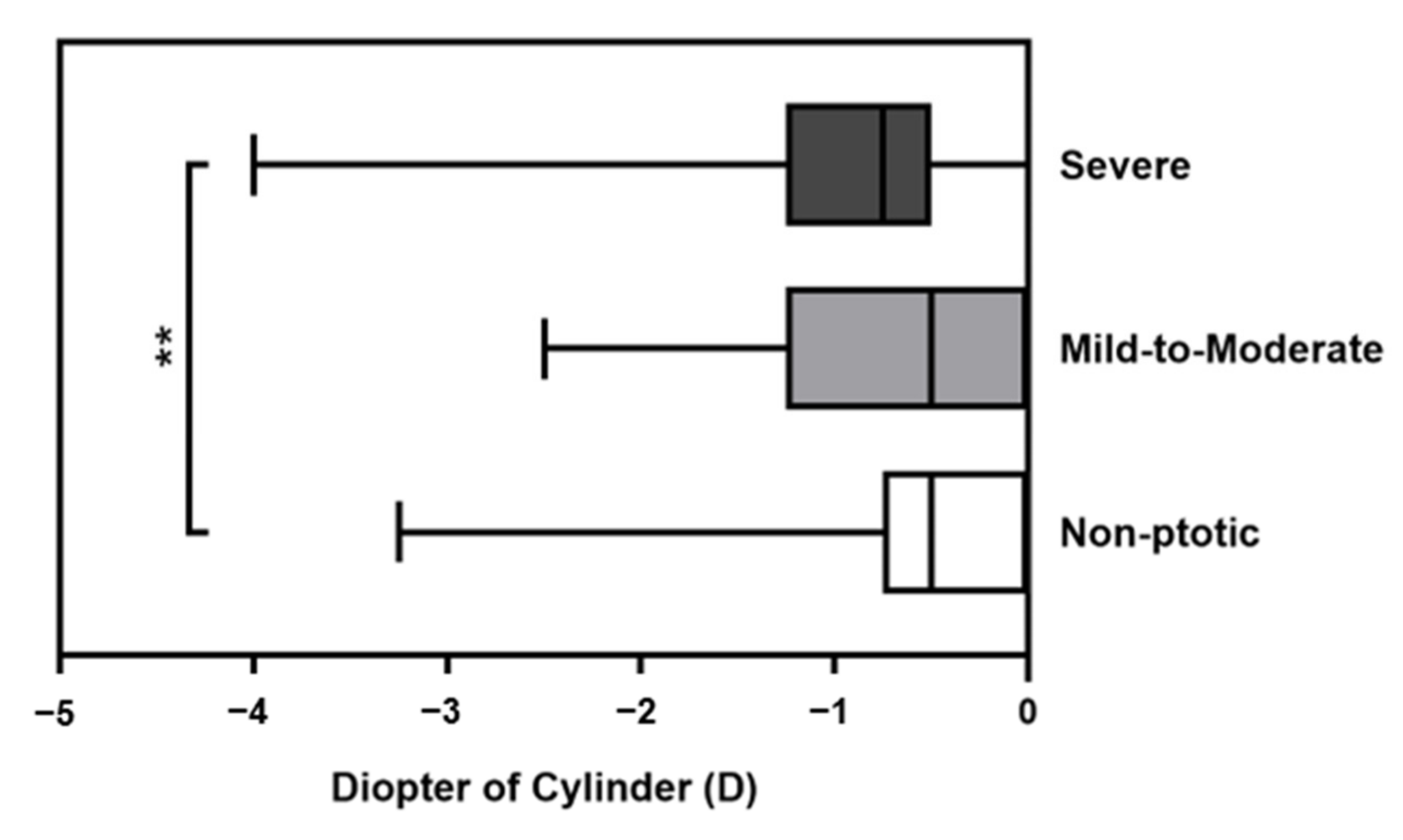
3.2. Comparison of Cylindrical Power between Different Severity Groups
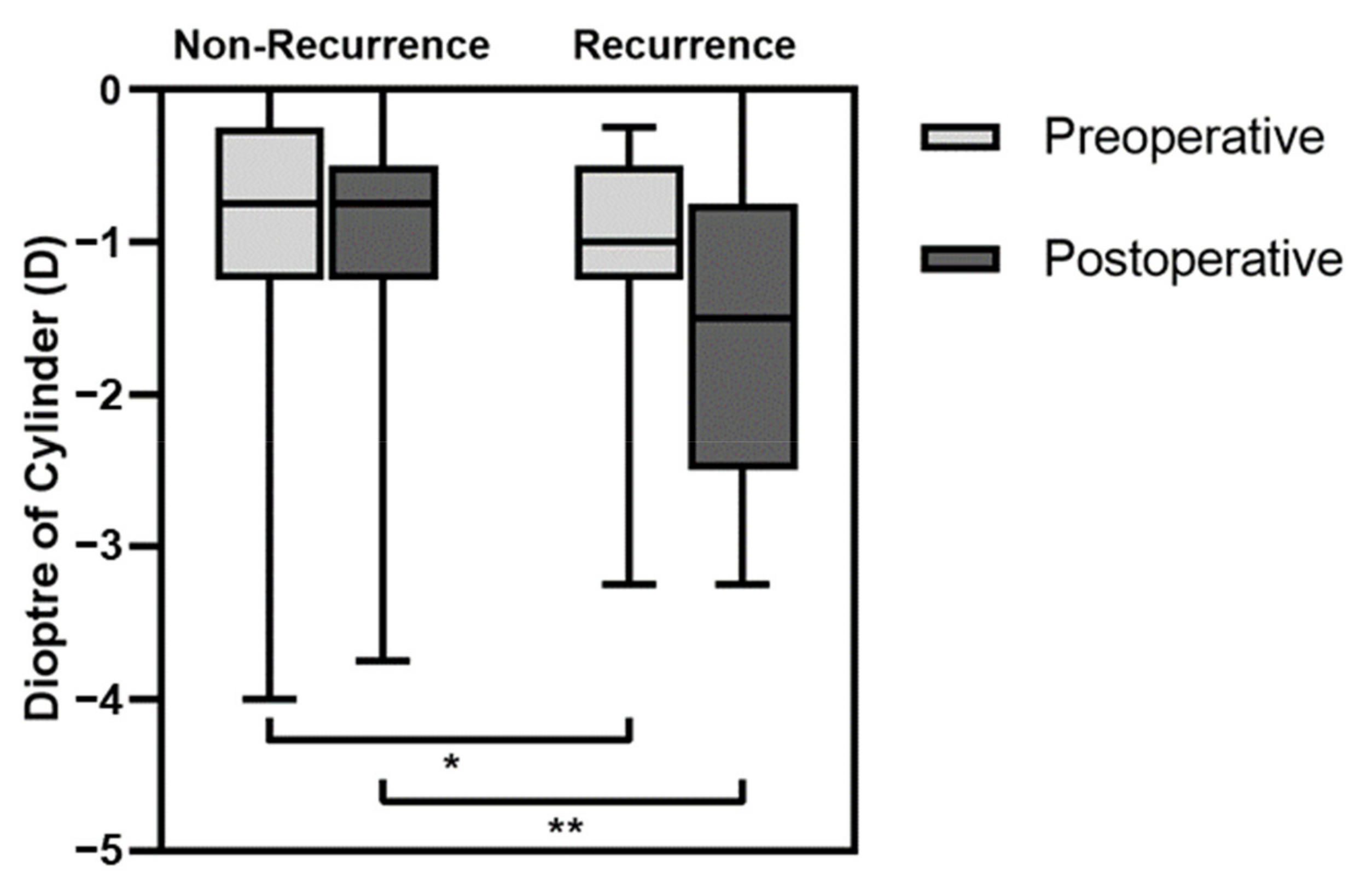
3.3. Comparison of Clinical Data between the Recurrence and Non-Recurrence Groups
3.4. Association between Recurrence and Clinical Data
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Griepentrog, G.J.; Diehl, N.N.; Mohney, B.G. Incidence and demographics of childhood ptosis. Ophthalmology 2011, 118, 1180–1183. [Google Scholar] [CrossRef] [Green Version]
- Wang, Y.; Xu, Y.; Liu, X.; Lou, L.; Ye, J. Amblyopia, Strabismus and Refractive Errors in Congenital Ptosis: A systematic review and meta-analysis. Sci. Rep. 2018, 8, 8320. [Google Scholar] [CrossRef] [Green Version]
- Zeng, X.Y.; Wang, J.X.; Qi, X.L.; Li, X.; Zhao, S.Z.; Li, X.L.; Qian, X.H.; Wei, N. Effects of congenital ptosis on the refractive development of eye and vision in children. Int. J. Ophthalmol. 2020, 13, 1788–1793. [Google Scholar] [CrossRef]
- Kim, Y.; Lee, J.H. Association of blepharoptosis with refractive error in the Korean general population. Eye 2021, 35, 3141–3146. [Google Scholar] [CrossRef] [PubMed]
- Hsia, N.Y.; Wen, L.Y.; Chou, C.Y.; Lin, C.L.; Wan, L.; Lin, H.J. Increased Risk of Refractive Errors and Amblyopia among Children with Ptosis: A Nationwide Population-Based Study. J. Clin. Med. 2022, 11, 2334. [Google Scholar] [CrossRef] [PubMed]
- Mongkolareepong, N.; Mekhasingharak, N.; Pimpha, O. Factors associated with corneal astigmatism change after ptosis surgery. Int. J. Ophthalmol. 2022, 15, 576–580. [Google Scholar] [CrossRef]
- Hoyt, C.S.; Stone, R.D.; Fromer, C.; Billson, F.A. Monocular axial myopia associated with neonatal eyelid closure in human infants. Am. J. Ophthalmol. 1981, 91, 197–200. [Google Scholar] [CrossRef]
- Huo, L.; Cui, D.; Yang, X.; Wan, W.; Liao, R.; Trier, K.; Zeng, J. A retrospective study: Form-deprivation myopia in unilateral congenital ptosis. Clin. Exp. Optom. 2012, 95, 404–409. [Google Scholar] [CrossRef]
- Srinagesh, V.; Simon, J.W.; Meyer, D.R.; Zobal-Ratner, J. The association of refractive error, strabismus, and amblyopia with congenital ptosis. J. AAPOS 2011, 15, 541–544. [Google Scholar] [CrossRef]
- Uğurbaş, S.H.; Zilelioğlu, G. Corneal topography in patients with congenital ptosis. Eye 1999, 13 Pt 4, 550–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, Y.K.; In, J.H.; Jang, S.Y. Changes in Corneal Curvature After Upper Eyelid Surgery Measured by Corneal Topography. J. Craniofac. Surg. 2016, 27, e235–e238. [Google Scholar] [CrossRef]
- Savino, G.; Battendieri, R.; Riso, M.; Traina, S.; Poscia, A.; D’Amico, G.; Caporossi, A. Corneal Topographic Changes After Eyelid Ptosis Surgery. Cornea 2016, 35, 501–505. [Google Scholar] [CrossRef]
- Gingold, M.P.; Ehlers, W.H.; Rodgers, I.R.; Hornblass, A. Changes in refraction and keratometry after surgery for acquired ptosis. Ophthalmic Plast. Reconstr. Surg. 1994, 10, 241–246. [Google Scholar] [CrossRef]
- Klimek, D.L.; Summers, C.G.; Letson, R.D.; Davitt, B.V. Change in refractive error after unilateral levator resection for congenital ptosis. J. AAPOS 2001, 5, 297–300. [Google Scholar] [CrossRef]
- Bee, Y.S.; Tsai, P.J.; Lin, M.C.; Chu, M.Y. Factors related to amblyopia in congenital ptosis after frontalis sling surgery. BMC Ophthalmol. 2018, 18, 302. [Google Scholar] [CrossRef]
- Ho, Y.F.; Wu, S.Y.; Tsai, Y.J. Factors Associated With Surgical Outcomes in Congenital Ptosis: A 10-Year Study of 319 Cases. Am. J. Ophthalmol. 2017, 175, 173–182. [Google Scholar] [CrossRef]
- Ben Simon, G.J.; Macedo, A.A.; Schwarcz, R.M.; Wang, D.Y.; McCann, J.D.; Goldberg, R.A. Frontalis suspension for upper eyelid ptosis: Evaluation of different surgical designs and suture material. Am. J. Ophthalmol. 2005, 140, 877–885. [Google Scholar] [CrossRef]
- Lee, M.J.; Oh, J.Y.; Choung, H.K.; Kim, N.J.; Sung, M.S.; Khwarg, S.I. Frontalis sling operation using silicone rod compared with preserved fascia lata for congenital ptosis a three-year follow-up study. Ophthalmology 2009, 116, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Chow, K.; Deva, N.; Ng, S.G. Prolene frontalis suspension in paediatric ptosis. Eye 2011, 25, 735–739. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayashi, K.; Katori, N.; Kasai, K.; Kamisasanuki, T.; Kokubo, K.; Ohno-Matsui, K. Comparison of nylon monofilament suture and polytetrafluoroethylene sheet for frontalis suspension surgery in eyes with congenital ptosis. Am. J. Ophthalmol. 2013, 155, 654–663.e651. [Google Scholar] [CrossRef] [PubMed]
- Woo, K.I.; Kim, Y.D.; Kim, Y.H. Surgical treatment of severe congenital ptosis in patients younger than two years of age using preserved fascia lata. Am. J. Ophthalmol. 2014, 157, 1221–1226.e1221. [Google Scholar] [CrossRef]
- Wagner, R.S.; Mauriello, J.A.; Nelson, L.B.; Calhoun, J.H.; Flanagan, J.C.; Harley, R.D. Treatment of Congenital Ptosis with Frontalis Suspension. Ophthalmology 1984, 91, 245–248. [Google Scholar] [CrossRef]
- Manners, R.M.; Tyers, A.G.; Morris, R.J. The use of Prolene as a temporary suspensory material for brow suspension in young children. Eye 1994, 8, 346–348. [Google Scholar] [CrossRef] [Green Version]
- Carter, S.R.; Meecham, W.J.; Seiff, S.R. Silicone Frontalis Slings for the Correction of Blepharoptosis. Ophthalmology 1996, 103, 623–630. [Google Scholar] [CrossRef]
- Kook, K.H.; Lew, H.; Chang, J.H.; Kim, H.Y.; Ye, J.; Lee, S.Y. Scanning electron microscopic studies of Supramid Extra from the patients displaying recurrent ptosis after frontalis suspension. Am. J. Ophthalmol. 2004, 138, 756–763. [Google Scholar] [CrossRef] [PubMed]
- Skaat, A.; Fabian, D.; Spierer, A.; Rosen, N.; Rosner, M.; Ben Simon, G.J. Congenital ptosis repair-surgical, cosmetic, and functional outcome: A report of 162 cases. Can. J. Ophthalmol. 2013, 48, 93–98. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.Y.; Son, B.J.; Son, J.; Hong, J.; Lee, S.Y. Analysis of the causes of recurrence after frontalis suspension using silicone rods for congenital ptosis. PLoS ONE 2017, 12, e0171769. [Google Scholar] [CrossRef] [PubMed]
- Byard, S.D.; Sood, V.; Jones, C.A. Long-term refractive changes in children following ptosis surgery: A case series and a review of the literature. Int. Ophthalmol. 2014, 34, 1303–1307. [Google Scholar] [CrossRef]
- Paik, J.S.; Kim, S.A.; Park, S.H.; Yang, S.W. Refractive error characteristics in patients with congenital blepharoptosis before and after ptosis repair surgery. BMC Ophthalmol. 2016, 16, 177. [Google Scholar] [CrossRef] [Green Version]
- Gusek-Schneider, G.C. Congenital ptosis: Amblyogenic refractive errors, amblyopia, manifest strabismus and stereopsis related to the types of ptosis. Data on 77 patients and review of the literature. Klin. Monbl. Augenheilkd. 2002, 219, 340–348. [Google Scholar] [CrossRef] [PubMed]
- Heisel, C.J.; Heider, A.; Stewart, K.J.; Andrews, C.A.; Kahana, A. Orbital Septum Fibrosis in Congenital Ptosis Correlates With Eyelid Function: A Clinicopathologic Study. Ophthalmic Plast. Reconstr. Surg. 2019, 35, 469–473. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, Y.; Kang, H.; Kakizaki, H. Axial Globe Length in Congenital Ptosis. J. Pediatr. Ophthalmol. Strabismus 2015, 52, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Wallman, J.; Winawer, J. Homeostasis of eye growth and the question of myopia. Neuron 2004, 43, 447–468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nalci Baytaroglu, H.; Kaya, B.; Korkusuz, P.; Hosal, M.B. A Study of Histopathologic Evaluation and Clinical Correlation for Isolated Congenital Myogenic Ptosis and Aponeurotic Ptosis. Ophthalmic Plast. Reconstr. Surg. 2020, 36, 380–384. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Unilateral (n = 59, 69.4%) | Bilateral (n = 26, 30.6%) | p | |
|---|---|---|---|
| Sex, n (%) | 0.099 | ||
| Male | 37 (62.7%) | 21 (80.8%) | |
| Female | 22 (37.3%) | 5 (19.2%) | |
| Age, n (%) | 0.943 | ||
| <5 years | 30 (50.8%) | 13 (50.0%) | |
| ≥5 years | 29 (49.2%) | 13 (50.0%) | |
| Age, mean ± SD a | |||
| Total: 6.11 ± 3.99 | 5.37 ± 3.12 | 6.96 ± 4.72 | 0.198 |
| Follow-up time (days, IQR) | 287 (155 to 384) | 208.5 (101.5 to 376.75) | 0.108 |
| Severity, n (%) | 0.798 | ||
| Mild-to-moderate | 8 (13.6%) | 3 (11.5%) | |
| Severe | 51 (86.4%) | 23 (88.5%) | |
| Preoperative MRD1 (IQR) a | −1 (−1 to 0) | 0 (−1 to 0.88) | 0.014 |
| Preoperative DS (IQR) a | 2.00 (1.50 to 3.00) | 1.75 (0.56 to 2.44) | 0.039 |
| Preoperative DC (IQR) a | −0.75 (−1.50 to −0.50) | −0.75 (−1.25 to −0.25) | 0.438 |
| Preoperative SE (IQR) a | 1.63 (0.75 to 2.38) | 1.31 (0.28 to 2.00) | 0.068 |
| Postoperative MRD1 (IQR) a | 2 (1.5 to 3) | 2 (0 to 2.88) | 0.087 |
| Postoperative DS (IQR) a | 2.25 (1.50 to 3.00) | 1.50 (0.50 to 2.25) | 0.013 |
| Postoperative DC (IQR) a | −0.75 (−1.75 to −0.50) | −1.00 (−1.50 to −0.50) | 0.915 |
| Postoperative SE (IQR) a | 1.63 (0.88 to 2.50) | 1.00 (−0.25 to 2.09) | 0.014 |
| Mild-to-Moderate Group (n = 11, 12.9%) | Severe Group (n = 74, 87.1%) | p | |
|---|---|---|---|
| Age (IQR) a | 6.52 (4.63 to 7.36) | 4.70 (3.62 to 6.44) | 0.050 |
| <5 years/≥5 years b | 3/8 | 40/34 | 0.097 |
| Male/female b | 6/5 | 52/22 | 0.296 |
| Follow-up time (IQR) a | 246 (155 to 386) | 243.5 (139.75 to 379.75) | 0.455 |
| Unilateral/bilateral b | 3/8 | 23/51 | 0.798 |
| Preoperative DS (IQR) a | 1.50 (0.50 to 2.06) | 2.00 (1.13 to 2.86) | 0.038 |
| Preoperative DC (IQR) a | −0.63 (−1.25 0.00) | −0.75 (−1.25 to −0.50) | 0.303 |
| Preoperative SE (IQR) a | 1.25 (0.00 to 1.66) | 1.50 (0.56 to 2.31) | 0.051 |
| Postoperative MRD1 (IQR) a | 2.00 (1.75 to 3.00) | 2.00 (1.00 to 3.00) | 0.113 |
| Postoperative DS (IQR) a | 1.50 (0.25 to 2.25) | 2.00 (1.00 to 2.86) | 0.144 |
| Postoperative DC (IQR) a | −0.75 (−1.44 to −0.50) | −1.00 (−1.63 to −0.50) | 0.832 |
| Postoperative SE (IQR) a | 1.06 (−0.34 to 1.94) | 1.50 (0.50 to 2.25) | 0.102 |
| Recurrence Group (n = 16, 19.8%) | Non-Recurrence Group (n = 69, 81.2%) | p | |
|---|---|---|---|
| Age (IQR) a | 4.86 (3.52 to 7.62) | 4.96 (3.81 to 6.62) | 0.982 |
| <5 years/≥5 years b | 8/8 | 35/34 | 0.985 |
| Male/female b | 11/5 | 47/22 | 0.961 |
| Follow-up time (IQR) a | 217 (103 to 379) | 240 (143 to 381) | 0.867 |
| Unilateral/bilateral b | 7/9 | 52/17 | 0.032 |
| Preoperative MRD1 (IQR) a | −1 (−2 to 0) | 0 (−1 to 0) | 0.067 |
| Preoperative DS (IQR) a | 2.25 (1.25 to 3.50) | 1.75 (0.81 to 2.50) | 0.115 |
| Preoperative DC (IQR) a | −1.00 (−1.25 to −0.50) | −0.75 (−1.25 to −0.25) | 0.042 |
| Preoperative SE (IQR) a | 1.63 (0.50 to 2.50) | 1.50 (0.50 to 2.09) | 0.299 |
| Postoperative MRD1 (IQR) a | 0 (0 to 0) | 2 (2 to 3) | <0.001 |
| Postoperative DS (IQR) a | 2.25 (0.75 to 3.75) | 1.75 (1.00 to 250) | 0.329 |
| Postoperative DC (IQR) a | −1.50 (−2.50 to −0.75) | −0.75 (−1.25 to −0.50) | 0.009 |
| Postoperative SE (IQR) a | 1.50 (−0.13 to 3.00) | 1.43(0.50 to 2.13) | 0.757 |
| Single Regression | Multiple Regression | ||||
|---|---|---|---|---|---|
| OR (95% CI) | p | Adjusted OR (95% CI) | p | ||
| Sex a (male as reference) | 0.842 (0.298 to 2.375) | 0.745 | 0.664 | ||
| Age a | 1.040 (0.941 to 1.150) | 0.441 | 0.972 | ||
| Preoperative SE (IQR) a | 1.180 (0.898 to 1.553) | 0.235 | |||
| Preoperative DS (IQR) a | 1.235 (0.943 to 1.617) | 0.125 | |||
| Preoperative DC (IQR) a | 0.662 (0.399 to 1.098) | 0.110 | |||
| Laterality a (bilateral as reference) | 0.303 (0.113 to 0.811) | 0.017 | 0.202 (0.064 to 0.638) | 0.006 | |
| Preoperative MRD1 (IQR) a | 0.723 (0.508 to 1.029) | 0.072 | 0.617 (0.412 to 0.924) | 0.019 | |
| Follow-up time a | 1.000 (0.998 to 1.002) | 0.857 | |||
| Postoperative SE (IQR) a | 1.099 (0.861 to 1.404) | 0.448 | |||
| Postoperative DS (IQR) a | 1.171 (0.921 to 1.489) | 0.198 | |||
| Postoperative DC (IQR) a | 0.512 (0.311 to 0.842) | 0.008 | 0.432 (0.241 to 0.776) | 0.005 | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ke, Y.; Meng, J.; Zhou, M.; Wu, P.; Zhang, F.; Hei, X.; Huang, D. The Recurrence of Ptosis after Correction Surgery Is Associated with Refractive Error. Medicina 2023, 59, 630. https://doi.org/10.3390/medicina59030630
Ke Y, Meng J, Zhou M, Wu P, Zhang F, Hei X, Huang D. The Recurrence of Ptosis after Correction Surgery Is Associated with Refractive Error. Medicina. 2023; 59(3):630. https://doi.org/10.3390/medicina59030630
Chicago/Turabian StyleKe, Yu, Jie Meng, Min Zhou, Pengsen Wu, Fan Zhang, Xiangqing Hei, and Danping Huang. 2023. "The Recurrence of Ptosis after Correction Surgery Is Associated with Refractive Error" Medicina 59, no. 3: 630. https://doi.org/10.3390/medicina59030630