
Investigation of Radiochromic Film Use for Source Position Verification through a LINAC On-Board Imager (OBI)
 ,
,  and
and
Abstract
:1. Introduction
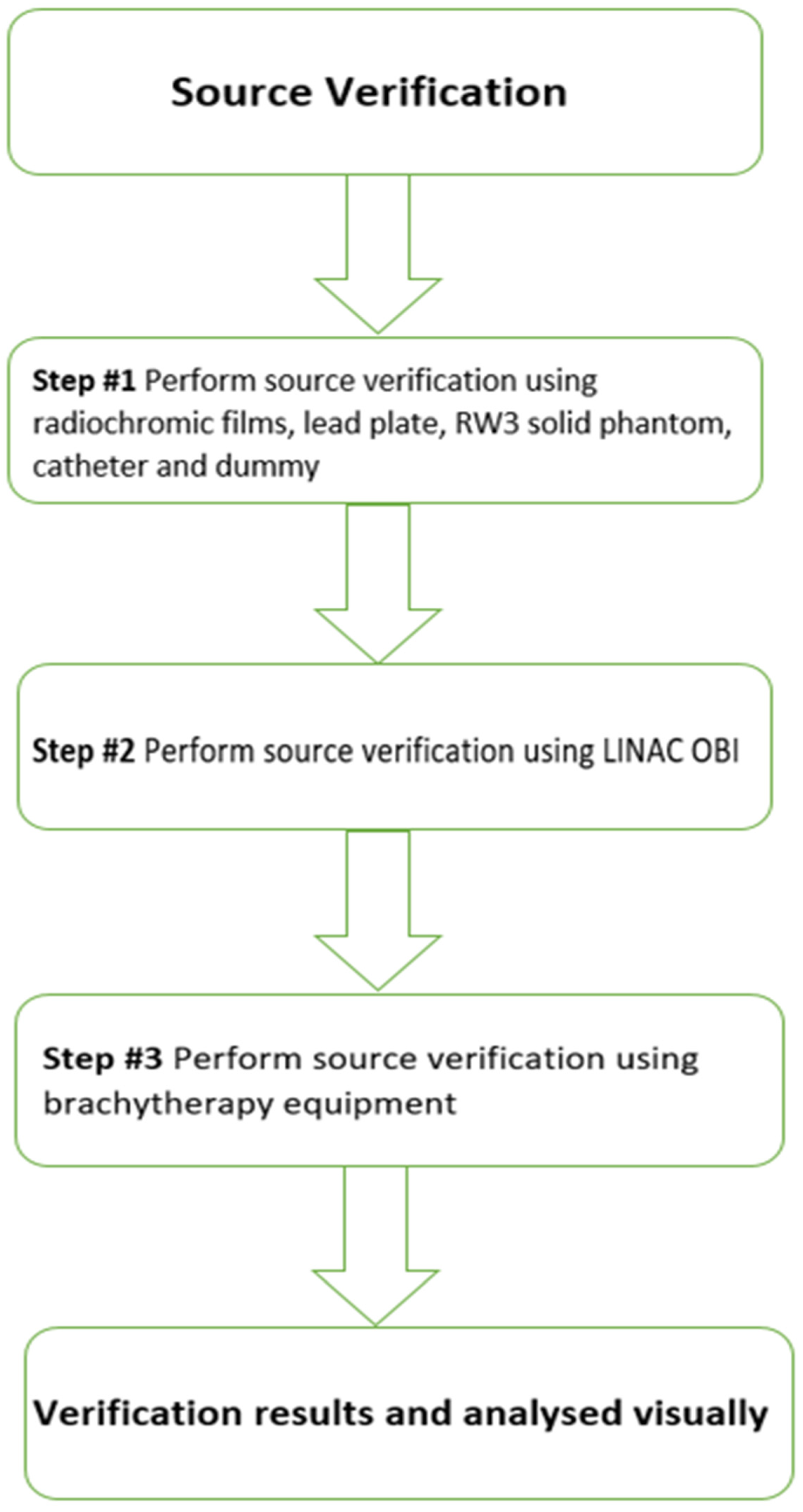
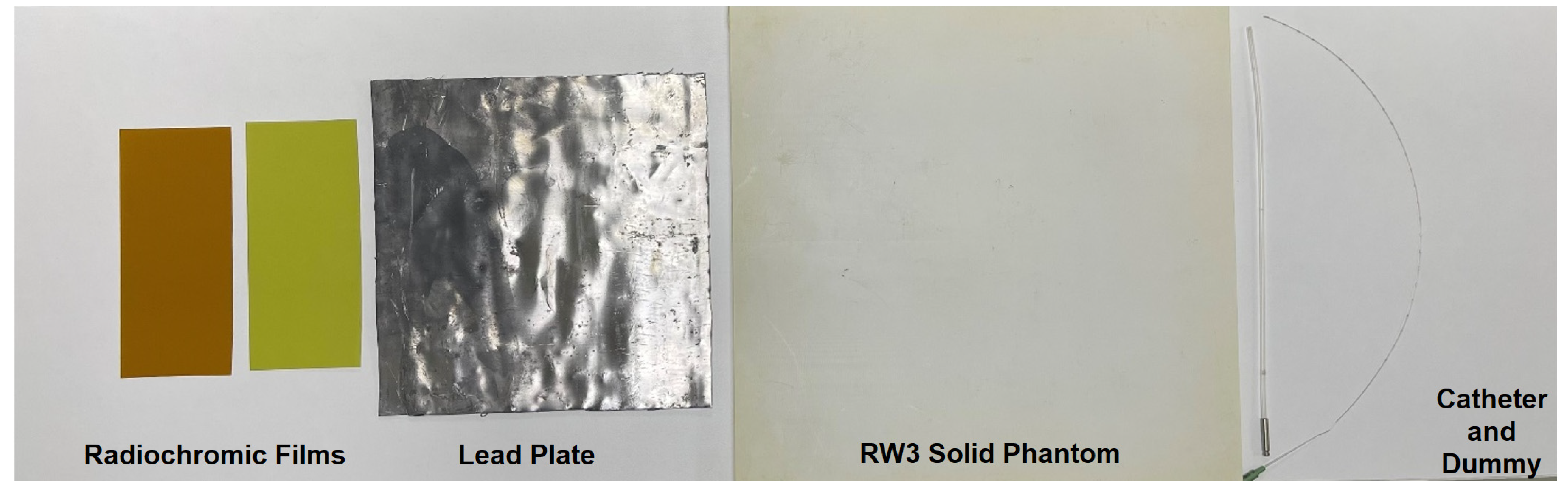
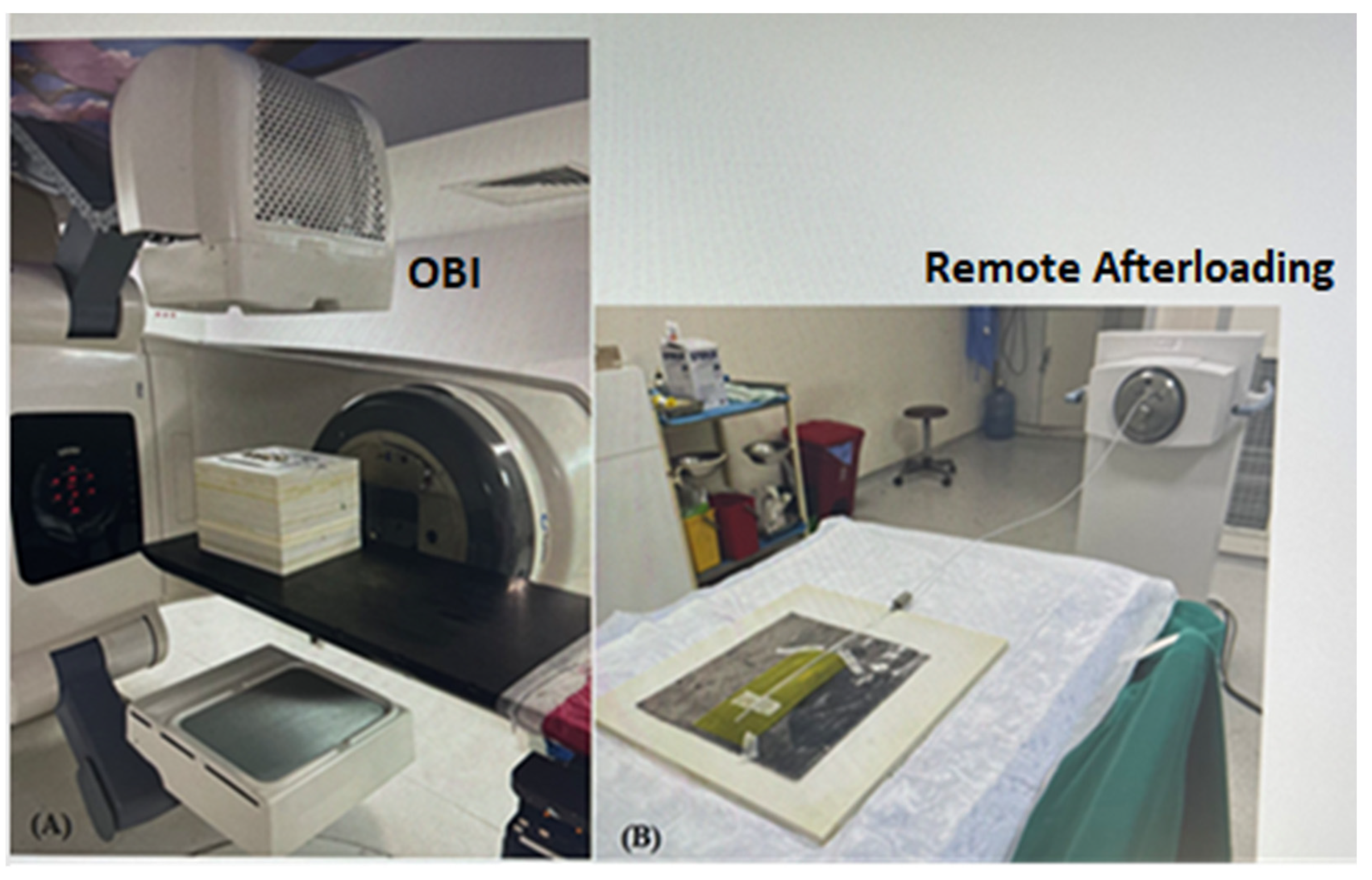
2. Materials and Methods
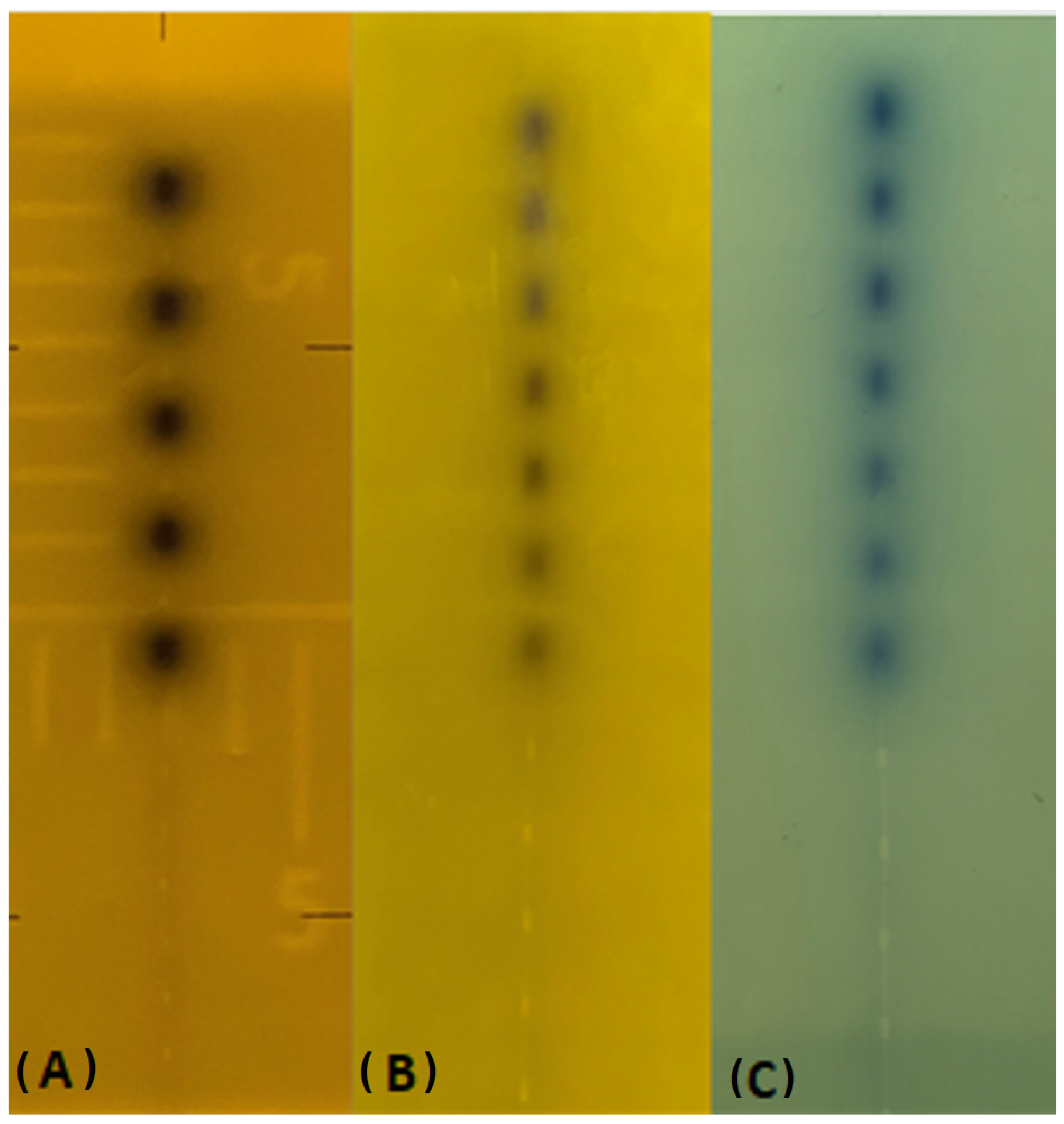
3. Results and Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chargari, C.; Deutsch, E.; Blanchard, P.; Gouy, S.; Martelli, H.; Guérin, F.; Dumas, I.; Bossi, A.; Morice, P.; Viswanathan, A.N.; et al. Brachytherapy: An Overview for Clinicians. CA Cancer J. Clin. 2019, 69, 386–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Skowronek, J. Current status of brachytherapy in cancer treatment—Short overview. J. Contemp. Brachyther. 2017, 9, 581–589. [Google Scholar] [CrossRef] [PubMed]
- Fulkerson, R.K.; Perez-Calatayud, J.; Ballester, F.; Buzurovic, I.; Kim, Y.; Niatsetski, Y.; Ouhib, Z.; Pai, S.; Rivard, M.J.; Rong, Y.; et al. Surface brachytherapy: Joint report of the AAPM and the GEC-ESTRO Task Group No. 253. Med. Phys. 2020, 47, e951–e987. [Google Scholar] [CrossRef] [PubMed]
- Podder, T.K.; Beaulieu, L.; Caldwell, B.; Cormack, R.A.; Crass, J.B.; Dicker, A.P.; Fenster, A.; Fichtinger, G.; Meltsner, M.A.; Moerland, M.A.; et al. American Association of Physicists in Medicine Brachytherapy Subcommittee and Therapy Physics Committee; Groupe Européen de Curiethérapie-European Society for Radiotherapy & Oncology BRAPHYQS Subcommittee. AAPM and GEC-ESTRO guidelines for image-guided robotic brachytherapy: Report of Task Group 192. Med. Phys. 2014, 41, 101501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lim, Y.K.; Kim, D. Brachytherapy: A Comprehensive Review. Prog. Med. Phys. 2021, 32, 25–39. [Google Scholar] [CrossRef]
- Thomadsen, B.R.; Erickson, B.A.; Eifel, P.J.; Hsu, I.-C.; Patel, R.R.; Petereit, D.G.; Fraass, B.A.; Rivard, M.J. A review of safety, quality management, and practice guidelines for high-dose-rate brachytherapy: Executive summary. Pract. Radiat. Oncol. 2014, 4, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Kutcher, G.J.; Coia, L.; Gillin, M.; Hanson, W.F.; Leibel, S.; Morton, R.J.; Palta, J.R.; Purdy, J.A.; Reinstein, L.E.; Svensson, G.K.; et al. Comprehensive QA for Radiation Oncology: Report of AAPM Radiation Therapy Committee Task Group 40. Med. Phys. 1994, 21, 581–618. [Google Scholar] [CrossRef] [PubMed]
- Godden, T.J. Physical Aspects of Brachytherapy. Medical Physics Handbooks; CRC Press: Boca Raton, FL, USA, 1988. [Google Scholar]
- Evans, M.D.C.; Devic, S.; Podgorsak, E.B. High Dose-Rate Brachytherapy Source Position Quality Assurance Using Radiochromic Film. Med. Dosim. 2007, 32, 13–15. [Google Scholar] [CrossRef] [PubMed]
- Küçücük, H.; Şenkesen, Ö.; Göksel, E.O. Quality Assurance in Brachytherapy. Turk. J. Oncol. 2019, 34 (Suppl. 1), 29–37. [Google Scholar] [CrossRef]
- Nath, R.; Anderson, L.L.; Meli, J.A. Code of practice for brachytherapy physics: Report of the AAPM Radiation Therapy Committee Task Group No. 56. American Association of Physicists in Medicine. Med. Phys. 1997, 24, 1557–1598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kohr, P.; Siebert, F.A. Quality assurance of brachytherapy afterloaders using a multi-slit phantom. Phys. Med. Biol. 2007, 52, N387–N391. [Google Scholar] [CrossRef] [PubMed]
- Palmer, A.L.; Lee, C.; Ratcliffe, A.J.; Bradley, D.; Nisbet, A. Design and implementation of a film dosimetry audit tool for comparison of planned and delivered dose distributions in high dose rate (HDR) brachytherapy. Phys. Med. Biol. 2013, 58, 6623–6640. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, H.; Iijima, K.; Chiba, T. Technical note: Analysis of brachytherapy source movement by high-speed camera. Med. Phys. 2022, 49, 4804–4811. [Google Scholar] [CrossRef] [PubMed]
- Awunor, O.; Berger, D.; Kirisits, C. A multicenter study to quantify systematic variations and associated uncertainties in source positioning with commonly used HDR afterloaders and ring applicators for the treatment of cervical carcinomas. Med. Phys. 2015, 42, 4472–4483. [Google Scholar] [CrossRef] [PubMed]
- Stern, R.; Liu, T. Dwell position inaccuracy in the Varian GammaMed HDR ring applicator. J. Appl. Clin. Med. Phys. 2010, 11, 291–296. [Google Scholar] [CrossRef] [PubMed]
- Demsey, C.; Smith, R.; Nyathi, T.; Ceylan, A.; Howard, L.; Patel, V.; Das, R.; Haworth, A. Acpsem brachytherapy working group recommendations for quality assurance in the brachytherapy. Phys. Eng. Sci. Med. 2013, 36, 387–396. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Film | SSD (cm) | kV | mA | ms |
|---|---|---|---|---|
| RTQA2 film | 70 | 80 | 250 | 1000 |
| EBT 3 film | 70 | 80 | 250 | 5000 |
| Film | Dwell Time (s) | Dwell Position Interval (cm) | Total Dwell Time (s) |
|---|---|---|---|
| RTQA2 film | 0.5 | 1.0 | 3.5 |
| EBT 3 film | 0.8 | 1.0 | 5.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Karaçam, S.Ç.; Tunçman, D.; ALMisned, G.; Ene, A.; Tekin, H.O. Investigation of Radiochromic Film Use for Source Position Verification through a LINAC On-Board Imager (OBI). Medicina 2023, 59, 628. https://doi.org/10.3390/medicina59030628
Karaçam SÇ, Tunçman D, ALMisned G, Ene A, Tekin HO. Investigation of Radiochromic Film Use for Source Position Verification through a LINAC On-Board Imager (OBI). Medicina. 2023; 59(3):628. https://doi.org/10.3390/medicina59030628
Chicago/Turabian StyleKaraçam, Songül Çavdar, Duygu Tunçman, Ghada ALMisned, Antoaneta Ene, and Huseyin Ozan Tekin. 2023. "Investigation of Radiochromic Film Use for Source Position Verification through a LINAC On-Board Imager (OBI)" Medicina 59, no. 3: 628. https://doi.org/10.3390/medicina59030628